
Abstract
With the rapid aging of the world population, the number of older adults aged 65 years and over is expected to double to 2.1 billion by 2050 worldwide (Naja et al., 2017). The decreased fertility rate and increased life expectancy largely due to advancements in medical science and technology have led to the increase in the aging of the global population (Kaplan & Inguanzo, 2017). Cognitive decline is a growing health concern among older adults with impaired memory, executive dysfunction, delayed processing speed and reasoning which are often affected leading to adverse outcomes (Deary et al., 2009; Park et al., 2003). Other health conditions associated with aging accelerate the rate of functional and structural changes in the brain, thereby leading to a faster cognitive decline (Falck et al., 2018; Murman, 2015). Some of these age-related health conditions include pain, diabetes, hypertension, arthritis, osteoarthritis, osteoporosis, depression, cardiovascular disease, and cancer (Denton & Spencer, 2010; Orfila et al., 2006). Thus, older adults experience cognitive decline with varying degrees of severity, which is associated with an increased risk of mortality, functional disability, and poor health-related quality of life (Zaninotto et al., 2018).
Total hemoglobin (Hgb), a protein in red blood cells, delivers oxygen to the tissues and ensures adequate tissue oxygenation which is essential to maintain physical needs and cognitive function (Billett, 1990; Otto et al., 2017). According to the diagnostic criteria by the World Health Organization, the normal range of Hgb is 12–16 g/dL for male adults and 11–15 g/dL for female adults (Qin et al., 2019). When the Hgb level is lower than 12 g/dL for male adults and 11 g/dL for female adults, this is referred to as anemia, where there is low Hgb in the red blood cell, resulting in poor tissue oxygen saturation (Qin et al., 2019). This inadequate cerebral oxygenation from anemia leads to impaired cerebral perfusion and function (e.g., vascular mechanisms). In response, vasodilation occurs with resultant increases in cerebral flow to compensate for the low Hgb level. However, this compensation eventually fails and leads to impaired cerebral function and ischemia, both of which can adversely affect cognition (Schneider et al., 2016). In contrast, an abnormally high Hgb level of 16 g/dL or above for male adults and 15 g/dL for female adults is considered as hyperhemoglobinemia, which can cause blood thickness and impaired blood circulation to the brain (Qin et al., 2019). Among older adults, the level of Hgb has been prospectively associated with cognitive decline (Yang et al., 2022). For example, there was a significant association between anemia (<13 g/dL for males and <12 g/dL for females) and global cognitive function and episodic memory among Chinese middle-aged and older adults (Qin et al., 2019). In addition, both anemia (<12 g/dL for males and <11 g/dL for females) and hyperhemoglobinemia (>16 g/dL for males and >15 g/dL for females) have been strongly associated with poor global cognitive function (Yang et al., 2022).
Despite their clinical importance, there is no established guidelines to classify low, normal, and high Hgb level in older adults (Goodnough & Schrier, 2014; Stauder & Thein, 2014). Most studies have used the Hgb guideline for general adults aged 18 years and over, while Hgb level is presumed to decrease with aging (Stauder & Thein, 2014). Stauder & Thein (2014) points out that the main challenge of defining a normal Hgb range in older adults is finding a “healthy” cohort who often suffer from multiple comorbidities (Stauder & Thein, 2014). Thus, it is vital to understand the relationship between Hgb and cognition in healthy older adults without any cognitive impairment and to find a critical Hgb level that is associated with cognitive improvement or decline in this population.
To date, there are mixed findings on the relationship between Hgb and cognition, with some studies reporting both low and high levels of Hgb to be associated with cognitive decline.
These mixed findings may indicate that the relationship between Hgb and cognition is highly likely to be non-linear (Qin et al., 2019; Shah et al., 2009; Yang et al., 2022). Some explanations regarding non-linearity could include threshold effect below and above a certain level of Hgb (Zakai et al., 2013), inverted U-shaped curve in the relationship between Hgb and cognition (Shah et al., 2009), differential effects of Hgb in different brain regions (Ward et al., 2020), and theories related to low and high Hgb and their effect on brain structure (Gattas et al., 2020; Shah et al., 2011). First, the threshold effect may exist where cognition may not improve above a certain level of Hgb, thus increasing Hgb level beyond this point may not have any additional benefits (Zakai et al., 2013). Similarly, below a certain level of Hgb, the negative effects of anemia on cognitive function may become more pronounced (Zakai et al., 2013). In addition, the best fitting model to describe the relationship between Hgb and cognition may follow an inverted U-shaped curve (Shah et al., 2009). In other words, low and high Hgb levels are associated with worse cognitive function, whereas moderate Hgb level is associated with better cognitive function (Shah et al., 2009). Hgb may have differential effects on cognitive function based on which brain regions are affected, with low and high level of Hgb associated with worse performance on semantic memory and perceptual speed but no effect on other cognitive domains among older adults (Deal et al., 2009; Qin et al., 2019; Shah et al., 2009). Another study found that low Hgb level was associated with only executive dysfunction (Deal et al., 2009). Other relevant theories explain that low Hgb level may be a marker for ischemia associated with cerebrovascular disease and lead to oxidative stress-associated changes in heme regulation (Shah et al., 2011). Anemia may hint a potential vascular cause which is the main reason why low Hgb level is associated with cognitive decline in most cognitive domains except episodic memory (Shah et al., 2011). In contrast, high hemoglobin level may be associated with cognitive decline through potential ischemic and hypoxic mechanisms as polycythemia vera has been associated with an increased risk of cerebral thrombosis (Shah et al., 2011). All of these explanations suggest that the use of statistical methodology suitable for examining the potential underlying non-linear relationship is needed (Qin et al., 2019; Shah et al., 2009; Yang et al., 2022).
In addition, it is worthwhile to examine the differences in the relationship between Hgb and cognition by gender, as gender differences exist in the level of Hgb in defining anemia and hyperhemoglobinemia (Qin et al., 2019; Shah et al., 2009). This is supported by previous studies where gender differences existed in the relationship between Hgb and cognitive function. For example, a study of older adults found that the risk of cognitive impairment increased significantly for men with anemia, but not for women (Trevisan et al., 2016). Contrastingly, another study showed that women with anemia showed significantly worse performance on global cognitive functioning based on the Telephone Interview of Cognitive Status (Qin et al., 2019). Through examining gender differences in the relationship between Hgb and cognition, we can further understand the underlying mechanisms involved and thus develop more targeted interventions to improve cognitive function and outcomes in both men and women. This emphasizes the importance of considering intersectionality and how different social identities may interact to affect health outcomes. To date, a commonly used statistical model in previous studies was the generalized linear model (GLM), which is a parametric model that aims to understand the relationship among variables of interest. GLM assumes a linear relationship among these variables in terms of the link function and allows the magnitude of variance to be a function of its predicted value (Zhao, 2013). While a non-linear relationship can also be estimated in GLM with a quadratic term, this may lead to multiple problems of multicollinearity and the non-linear effects estimated this way are global when in some cases the non-linearity is a local phenomenon (Tanskanen et al., 2016). In other words, this means that the non-linearity might exist only throughout a specific range of the scale (e.g., only at the bottom of the scale or at the top of the scale (Tanskanen et al., 2016). In our current work, we believe that the non-linearity could be a local phenomenon at a low Hgb and high Hgb level and thus believe GLM might not be able to capture this local non-linearity. GLM also estimates interaction effects which are usually forced into a linear form for simplification purpose which is one of its limitations. Rather, generalized additive model (GAM) estimates simple nonparametric smoothers which can be interpreted as interactions with possible non-linearity (Tanskanen et al., 2016). Given the potential non-linear relationship between Hgb and cognition, it may be statistically naïve to use a parametric model by assuming a linear relationship as the functional form. Instead, the use of a nonparametric model which does not make any particular assumptions about the form of mapping function may be appropriate in understanding the underlying relationship between Hgb and cognition (Hastie, 1992; Horowitz, 2001). Herein, the GAM offers greater flexibility and interpretation to examine the unknown functional form and uncover hidden patterns in the data (Hastie, 1992; Horowitz, 2001). Another advantage of GAM is regularization in which the smoothness of the predictor function is controlled to prevent overfitting of the model (Hastie, 1992; Horowitz, 2001). The use of GAM may help reveal a non-linear relationship between Hgb and cognition not captured in previous studies which can further explain their mixed findings. In addition, we will be able to compare the degree of non-linearity and identify critical inflection points where the slope changes significantly in both genders.
Thus, the purpose of this exploratory study was to identify the potential non-linear relationship between Hgb and cognition using GAM among cognitively normal older adults and how this relationship differs in terms of gender (male vs. female) in three GAM models, specifically: Model 1- not adjusting for covariates; Model 2- adjusted for sociodemographic factors; and Model 3- adjusted for sociodemographic, lifestyle, and clinical factors.
Methods
Study Design and Data Collection
This is a secondary data analysis using the cross-sectional data of Wave II (2010–2011) from the National Social Life, Health, and Aging Project (NSHAP). Among the available waves (Waves I–IV), Wave I did not measure cognition based on Montreal Cognitive Assessment (MOCA) and Wave IV is currently undergoing data collection. Thus, Wave II and Wave III were left for data analysis. Wave II was selected based on the larger sample size of older adults aged between 65 and 85 years.
Description of the Data Set
The NSHAP is a longitudinal, population-based study to understand the well-being of older, community-dwelling adults aged 57–85 years old in the United States at the time of recruitment. It examined physical, cognitive, and social domains of older adults specific to aging (e.g., cognitive function, sensory function, and frailty) through a collection of extensive surveys and biomarker data collection. Wave II was conducted in 2010–2011, and the same participants from Wave I were re-interviewed as well as their cohabiting spouse or partners (Ho et al., 2018; Olivieri-Mui et al., 2022).
Participants
Older adults aged between 65 and 85 years old with normal cognition as defined by MOCA score of 26 or above (Larner, 2012) were included in the data analysis (Bohannon & Magasi, 2015; Bugos et al., 2007). Participants with missing values on key study variables: Hgb and MOCA cognition score were excluded, leaving a total of 759 participants for this study.
Measures
Total Hemoglobin (Hgb)
Total hemoglobin (Hgb) was collected from the dried blood spot samples collected during the interview from the parent study (Williams & McDade, 2009). In the parent study, finger sticks and disposable lancets were used to collect whole blood and filter paper for transport and storage. It has been previously validated that the dried blood spot sample method has good sensitivity and precision compared to venous blood draws (Williams & McDade, 2009). The collected blood samples were analyzed using a standardized procedure in the Laboratory for Human Biology Research at Northwestern University. Hgb levels collected from the dried blood spot samples were converted to whole-blood equivalent Hgb (g/dL) (O’Doherty et al., 2014).
Cognition
The survey-adaptation of MoCA (Montreal Cognitive Assessment), MoCA-SA, was used to measure cognition among older adults which has shown good internal reliability (Cronbach’s a = 0.76), and successfully captured cognitive abilities in multiple domains across gender, racial/ethnic groups, and education. The MoCA-SA scores have been converted into MoCA scores (ranging from 0 to 30) using the high-fidelity prediction equation that yields identical scores with 99% cases, with higher scores denoting a better cognitive ability (Dale et al., 2018; Kotwal et al., 2016).
Sociodemographic, Lifestyle, and Clinical Characteristics
Sociodemographic, lifestyle, and clinical characteristics were included in the data analysis. These characteristics included age, race, gender, marital status, education level, annual household income, current employment status (no/yes), current smoking (no/yes), alcohol (no/yes), physical activity, rested sleep (no/yes), and the presence (no/yes) of diabetes, hypertension, stroke, arthritis, osteoporosis, cancer, congestive heart failure, heart attack, and lung disease (“Has a doctor ever told you that you have, for example, certain chronic condition?”). Other important age-related biomarkers such as complete blood count, lipids, and inflammatory biomarkers were not included due to their limited availability in the NSHAP.
Perceived social support was measured by asking a total of six questions on how often the participants could 1) rely on and 2) open up to their spouse/partner, family, or friends. Each question had a possible response on a 4-point Likert scale from 0 (“hardly ever or never”) to 3 (“often”). The total perceived social support that ranges from 0 to 18, with a higher score indicating more perceived social support. Social interaction was measured by asking a total of three questions on the frequency of 1) volunteering, 2) attending organizations, and 3) socializing with friends or relatives. Each question was on a 7-point Likert scale from 0 (“never”) to 6 (“several times a week),” with the total score ranging from 0 to 18. A higher score indicates more frequent social interaction (Santini et al., 2020; Stephens et al., 2011).
Depression was assessed using the 11-item Center for Epidemiological Studies Depression (CESD-11) scale, a shorter version of the original 20-item CESD (CESD-20) scale. CESD-11 has shown good internal reliability with Cronbach’s alpha of .80. In the CESD-11, participants were asked to rate the frequency of their feelings in the past week on a 4-point Likert scale from 0 (“rarely or none of the time”) to 3 (“most of the time”). The summed score ranged from 0 to 33, with a higher score indicating more severe depressive symptoms (Pun et al., 2017).
Anxiety was assessed using the 7-item Hospital Anxiety and Depression Scale (HADS), which has shown good reliability and validity in population-based studies. Participants were asked to rate the frequency of their feelings in the past week on a 4-point Likert scale from 0 (“rarely or none of the time”) to 3 (“most of the time”). The summed score ranged from 0 to 21, with a higher score indicating more severe anxiety (Pun et al., 2017).
Stress was assessed using the 4-item Perceived Stress Scale (PSS) with Cronbach’s alpha of 0.66 (Ezzati et al., 2014). Participants were asked to rate the frequency of stress on a 4-point Likert scale from 0 (“rarely or none of the time” to 3 (“most of the time),” with a total score ranging from 0 (lowest perceived stress) to 12 (highest perceived stress) (Shen & Liu, 2021). Loneliness was assessed using a 3-item shortened UCLA-loneliness scale that has shown good internal reliability with Cronbach’s alpha of 0.81 (Shiovitz-Ezra & Leitsch, 2010). Participants are asked to rate the frequency of loneliness on a 3-point Likert scale from 0 (“hardly ever”) to 2 (“often”), with a total score ranging from 0 (not lonely) to 6 (very lonely).
Ethical Considerations
The de-identified NSHAP study database, codebook, and survey questionnaires are currently available for public access from the Inter-university Consortium for Political and Social Research (ICPSR) website. All the materials were downloaded to a secure, encrypted server at Columbia University. Only the de-identified information was archived and analyzed. All datasets, corresponding codebooks, and statistical programs were stored on a secure, encrypted server at Columbia University. The current study received Columbia university institutional review board declaration of exemption [IRB-AAAU4294].
Data Analysis
The “mgcv” package v.1.8–31 in the R statistical software program (version 4.0.5) was used to fit three GAM models. GAM is a nonparametric regression model that supports non-Gaussian error distributions and captures the non-linear relationship between the predictors and outcome (López-Moreno & Nogués-Bravo, 2005). GAM has two main parts in its estimation method: the first part is the parametric estimation for covariates (e.g., sociodemographic, lifestyle, and clinical factors), and the second part is the nonparametric estimation for smoothing predictor (e.g., Hgb). Different from GLM, GAM can carry out the interaction between two or more predictors. A nonparametric smoother was applied to the predictor (e.g., Hgb) and the component response was additively calculated. Instead of using polynomial functions, GAM uses smoothing splines for functions. We used the thin-plate regression spline smooth available in the “mgcv” package to balance the data's fit with the model’s complexity, thus preventing model overfitting. Herein, we estimated the smoothing parameter based on a restricted maximum likelihood (REML) approach. The basis dimension for smoothing term (k) was set to 9 after using the “gam.check” function in the “mgcv” package with a k-index of 1.01 and p > .05. Furthermore, the outcome variable (e.g., cognition) in GAM could address different probability distributions using the link function (Yin & Wang, 2017). Thus, we used a Gaussian distribution with an identity link in our GAM model. As a result, three GAM models were built: Model 1: not adjusting for covariates, Model 2: adjusted for sociodemographic factors, and Model 3: adjusted for sociodemographic, lifestyle, and clinical factors. While Model 1 might be considered less precise and provide biased results, Model 1 was built to serve as a knowledge basis to closely understand how adjustment of covariates might affect the relationship between Hgb and cognition.
For each model, the predicted smooth functions and confidence intervals were plotted. The effective degree of freedom (EDF) was calculated, which quantifies the degree of the non-linearity of the curve. An EDF equal to 1 indicates a linear relationship, 1 < EDF ≤2 indicates a weak non-linear relationship (if EDF ≈1.5, then it will be regarded as moderate non-linear relation; if EDF ≈2, high-moderate non-linear relationship) and EDF >2 indicates a highly non-linear relationship (Hunsicker et al., 2016). When there was a non-linear relationship between Hgb and cognition, the recursive method automatically identified the inflection point using the maximum model likelihood. The threshold effect was examined using a two-piecewise linear regression model and multiple slope parameters separated by the inflection point were obtained. The inflection point identifies the specific point of Hgb level where the slope changed the direction significantly. Estimates of the slopes and inflection points were obtained using the “segmented” package (Muggeo, 2008).
Regarding the missing data for covariates, the Little test revealed that the data was not missing completely at random (p < .001) and was considered missing at random. Multivariate imputation by chained equations is a robust method of addressing missing at random data. During this procedure, several regression models are run where each variable with missing data is modeled conditional upon the other variables in the dataset. This iterative process continued until the convergence has met. Further details on the imputation procedures can be found elsewhere (Azur et al., 2011).
Results
Participant Characteristics
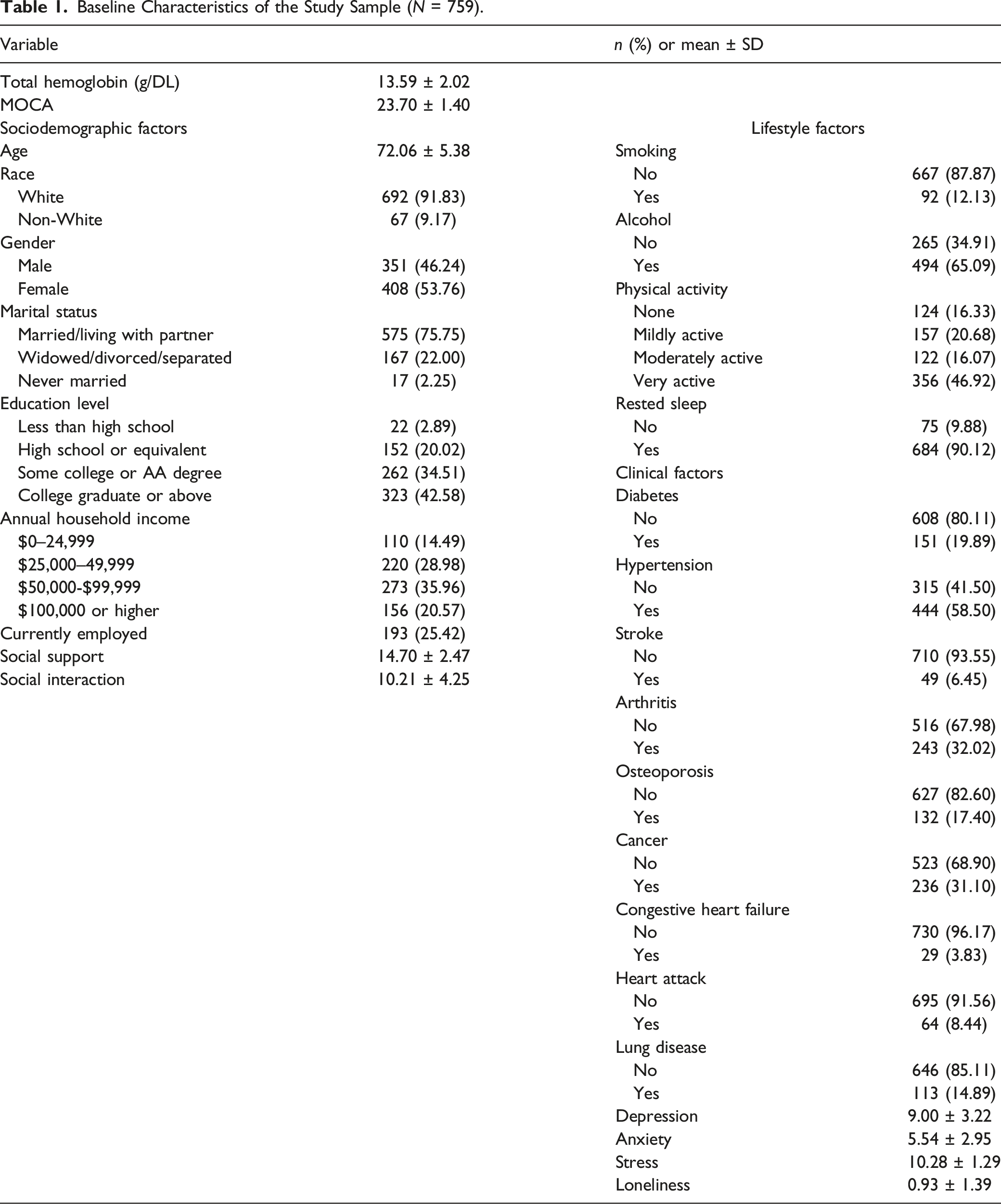
Baseline Characteristics of the Study Sample (N = 759).
Generalized Additive Models
Estimated Regression Coefficients From the Overall Additive Model With a Factor-Smooth Interaction.
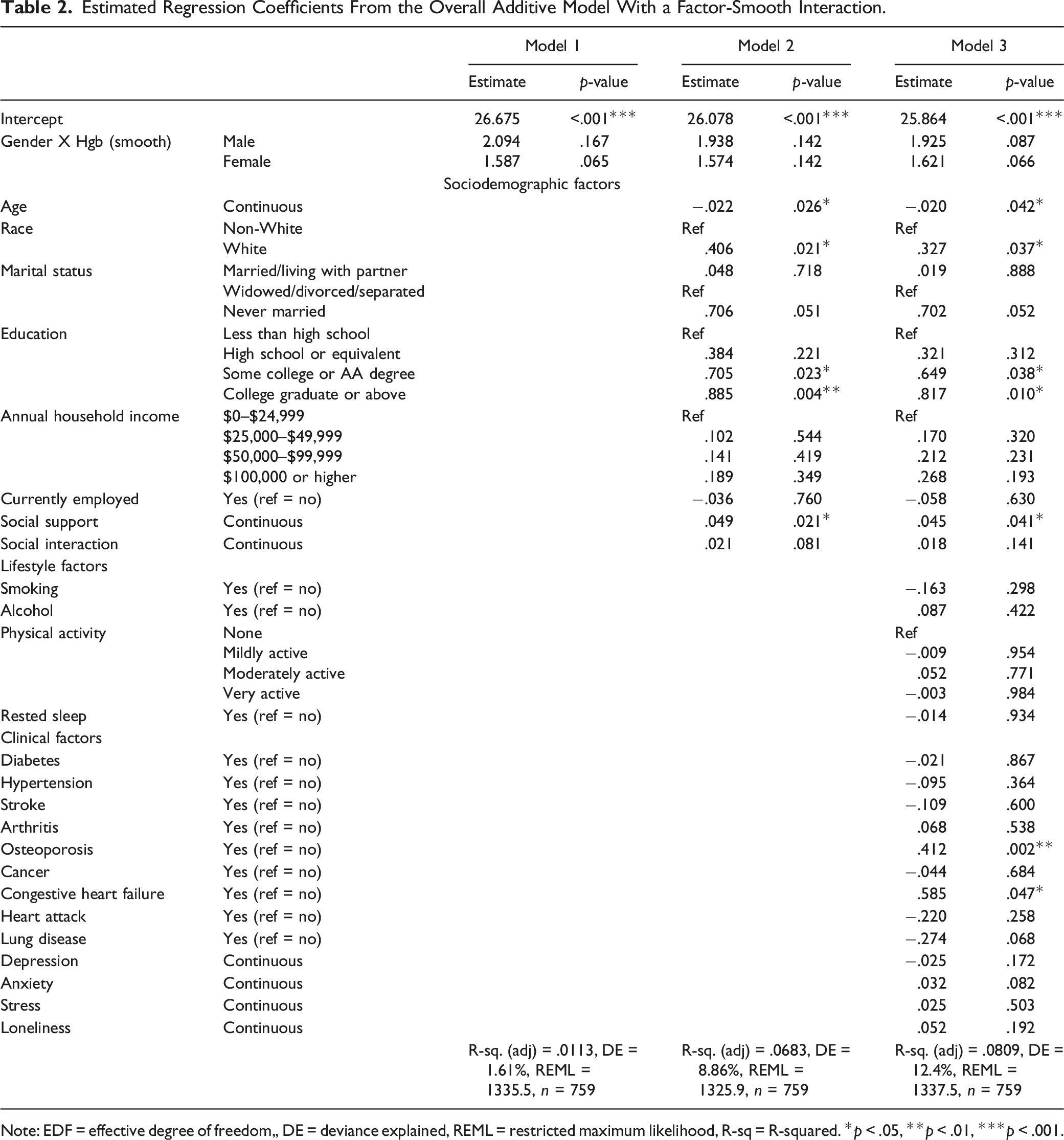
Note: EDF = effective degree of freedom,, DE = deviance explained, REML = restricted maximum likelihood, R-sq = R-squared. *p < .05, **p < .01, ***p < .001.
Model 1: Not Adjusting for Covariates
In Model 1, cognition was used as the outcome variable with a smoothing spline function of Hgb as a predictor variable in male and female older adults. In the male group, EDF was 2.094, indicating a highly non-linear relationship but it was not significant (p = 167). In the female group, EDF was 1.587, indicating a moderate non-linear relationship but it was also not significant (p = .065). Figure 1 shows the plots of estimated smoothing spline functions for Model 1. Plots of estimated smoothing spline functions (Model 1). Note. Left: male; right: female.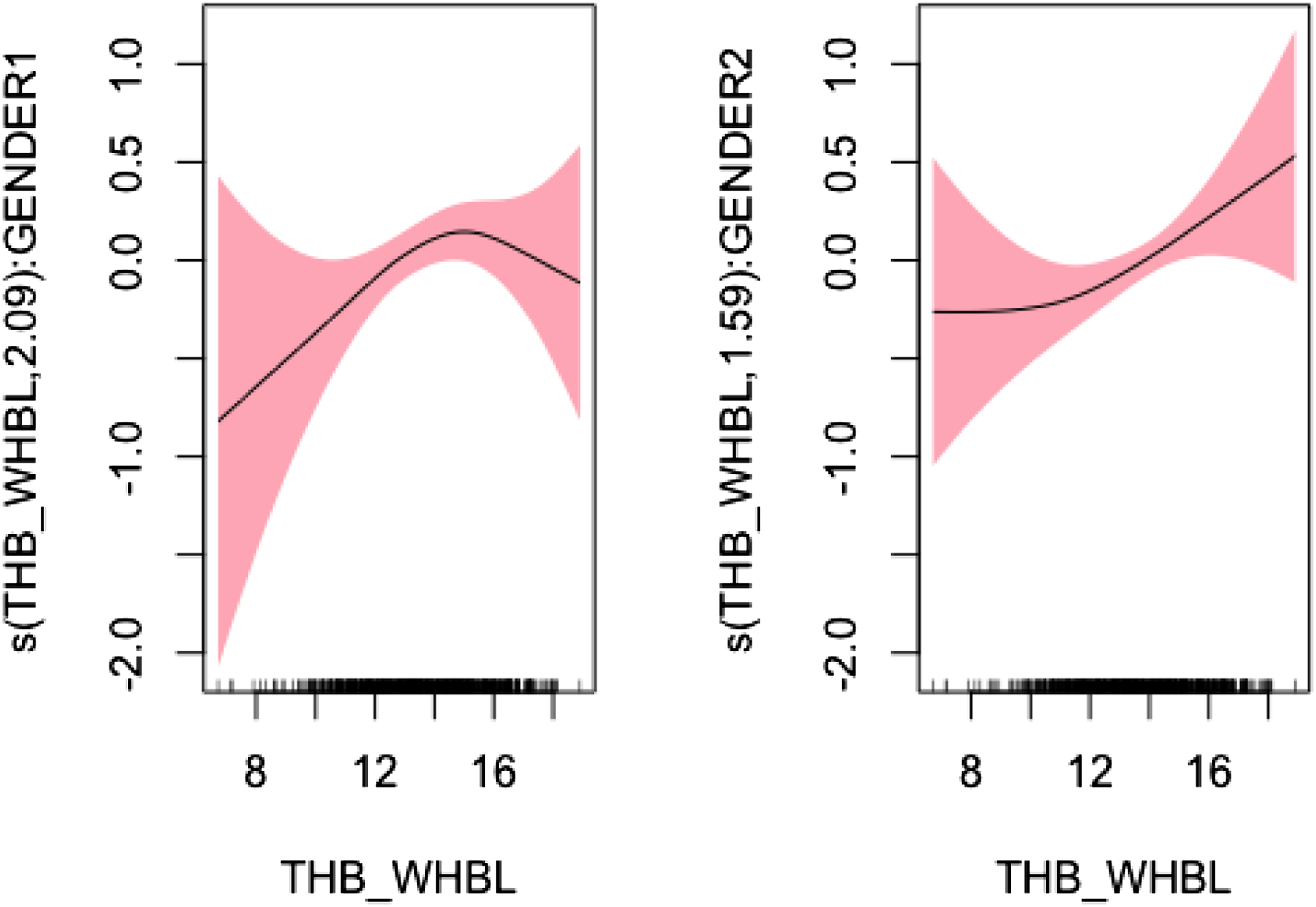
Model 2: Adjusted for Sociodemographic Factors
Model 2 was built upon Model 1 while adjusted for sociodemographic factors such as age, gender, marital status, education, annual household income, current employment, social support, and social interaction. There was a high-moderate non-linear relationship between Hgb and cognition in the male group (EDF = 1.938, p = .142) and a moderate non-linear relationship in the female group (EDF = 1.574, p = .142). However, both of these relationships were not significant. Figure 2 shows the plots of estimated smoothing spline functions for Model 2. Plots of estimated smoothing spline functions (Model 2). Note. Left: male; right: female.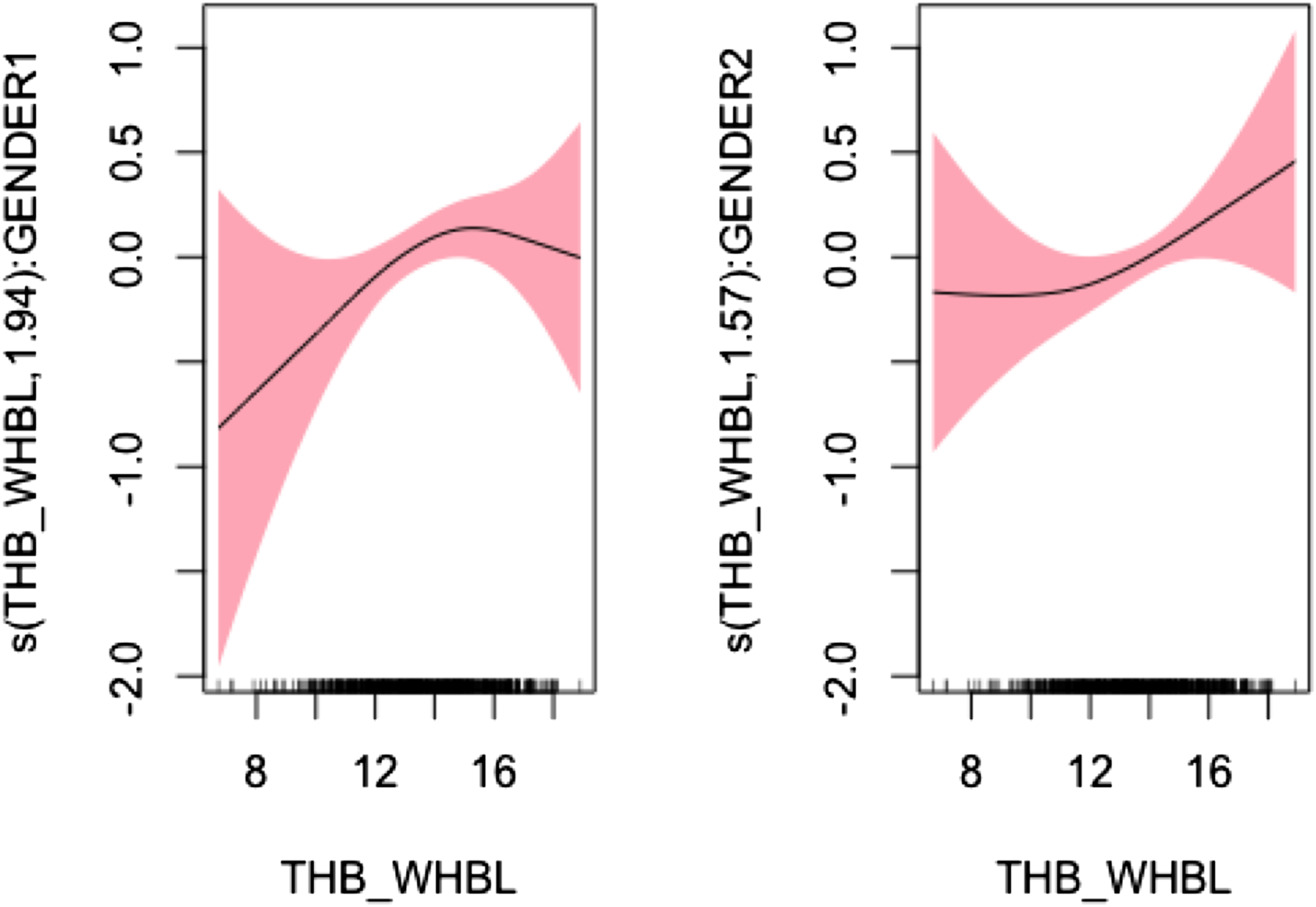
Model 3: Adjusted for Sociodemographic, Lifestyle, and Clinical Factors
Model 3 was built upon Model 2, and further adjusted for lifestyle and clinical factors. These lifestyle and clinical factors included smoking status, alcohol consumption, physical activity, rested sleep, presence of diabetes, hypertension, stroke, arthritis, osteoporosis, cancer, congestive heart failure, heart attack, lung disease, depression, anxiety, stress, and loneliness. Similarly, there was a high-moderate non-linear relationship between Hgb and cognition in the male group (EDF = 1.925, p = .087) and a moderate non-linear relationship in the female group (EDF = 1.574, p = .066), both of which were not significant. Figure 3 shows the plots of estimated smoothing spline functions for Model 3. Plots of estimated smoothing spline functions (Model 3). Note. Left: male; right: female.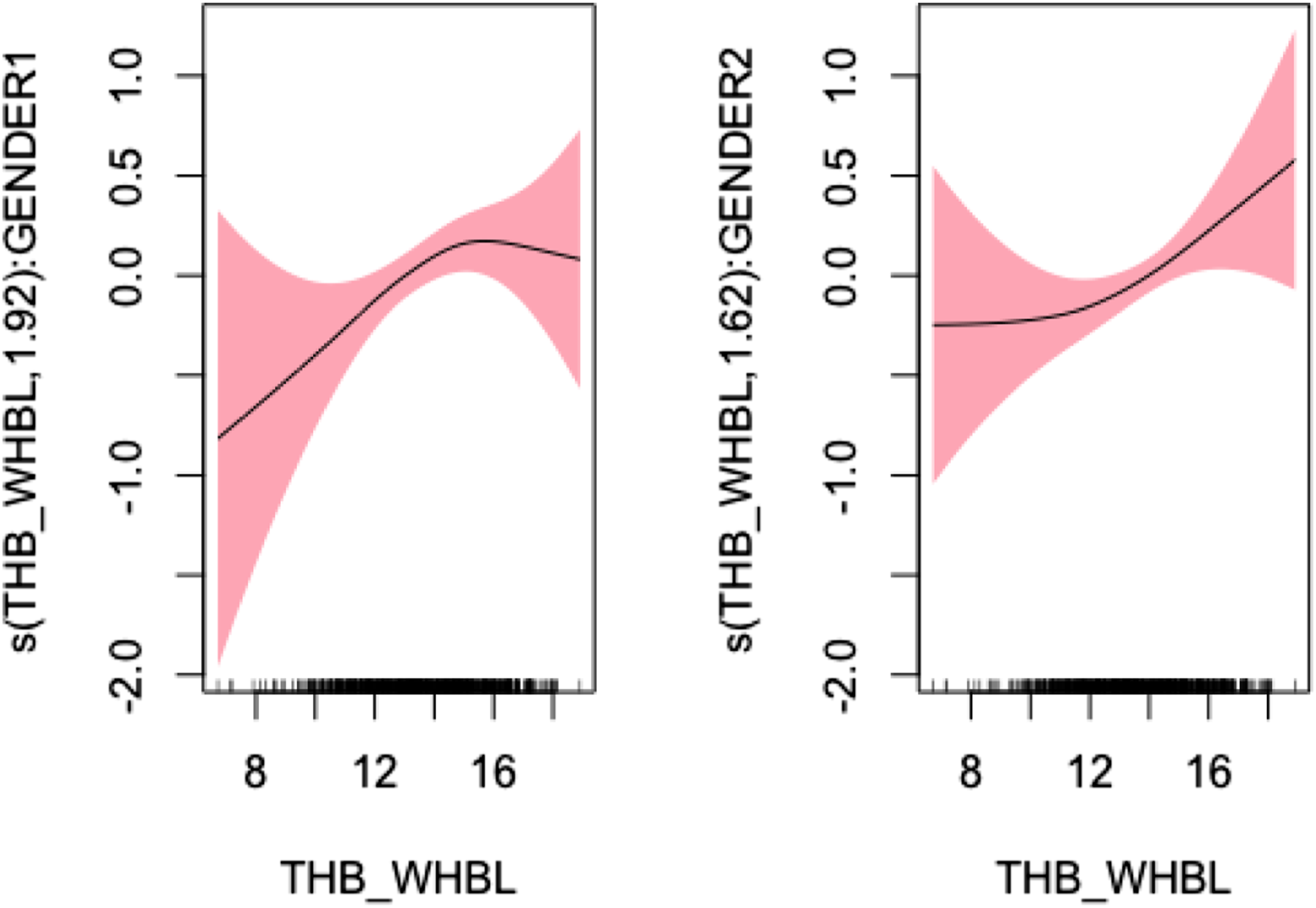
Relationship Between Hgb and Cognition in Male Older Adults
Adjusted Association Between Hgb and Cognition in Older Adults (Male) < or ≥ Optimum Threshold Level (15.10 g/DL With Standard Error of .76).
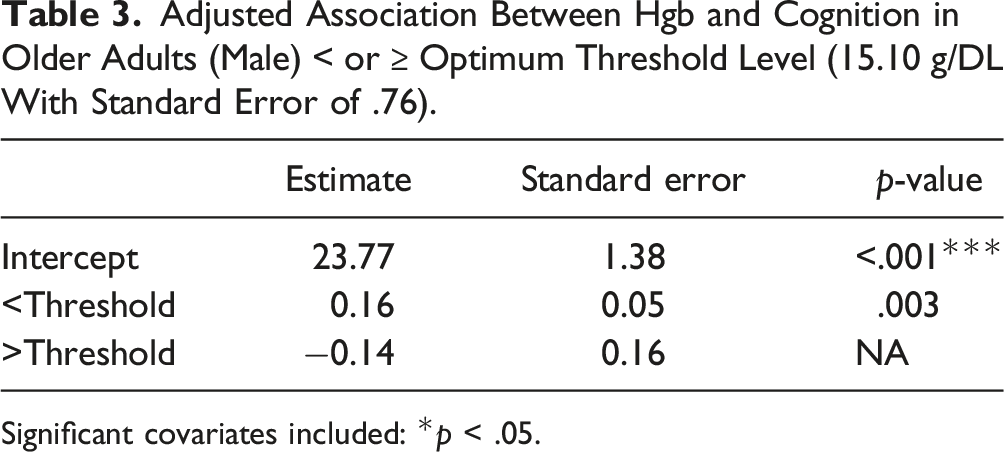
Significant covariates included: *p < .05.
Relationship Between Hgb and Cognition in Female Older Adults
Adjusted Association Between Hgb and Cognition in Older Adults (Female) < or ≥ Optimum Threshold Level (11.72 g/DL With Standard Error of 1.02).
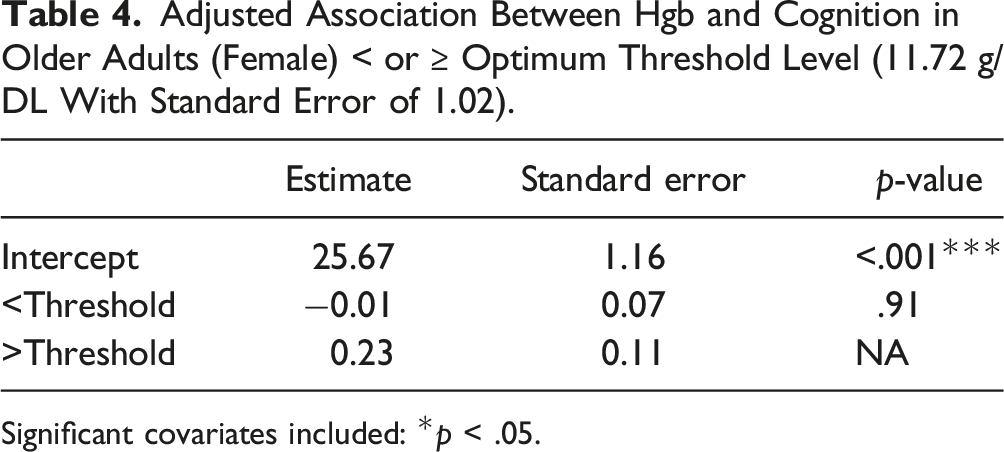
Significant covariates included: *p < .05.
Discussion
The current exploratory study used the GAM to understand the association between Hgb and cognition and to examine potential gender differences among older adults aged 65 years and above. While both genders had a non-linear association between Hgb and cognition, the degree of non-linearity was more pronounced in male older adults. The inflection point of 15.10 g/dL was obtained for male older adults where the level of cognition initially increased but decreased beyond the inflection point. In contrast, the level of cognition continuously increased beyond the inflection point of 11.72 g/dL for female older adults.
In both genders, there was a non-linear association between Hgb and cognition with different degrees of non-linearity in unadjusted and adjusted models. To date, there are mixed results on the association between the level of Hgb and cognition among cognitively healthy older adults (Chen et al., 2012; Deal et al., 2009; Kurella Tamura et al., 2010; Shah et al., 2009). For example, both anemia and hyperhemoglobinemia were associated with cognitive decline, particularly in the domains of semantic memory and perceptual speed among older adults (Shah et al., 2009). In contrast, another study reported that there was no significant association between Hgb and cognitive impairment after adjusting for covariates (Kurella Tamura et al., 2010). More specifically, anemia was not associated with cognitive performance, but with depression, in healthy male older adults without any severe physical or psychological comorbidities (Chen et al., 2012). In theory, cognition is highly likely to be adversely affected by poor tissue oxygen saturation with a low Hgb level and impaired blood circulation with a high Hgb level (Qin et al., 2019). Yet, such mixed findings may be due to the use of GLM, which may not be an appropriate statistical method when there is presumed to be a non-linear relationship (Chen et al., 2012; Deal et al., 2009; Kurella Tamura et al., 2010; Shah et al., 2009). Thus, our study adds to the current literature by using a relatively new method of GAM, which offers greater flexibility and interpretation to examine the potential non-linear relationship between variables of interest (Hastie, 1992; Horowitz, 2001). However, given the exploratory nature of our study, we focused on cognition as a whole domain. It is recommended that future research examine multiple cognitive domains and explore the relationship between Hgb and each cognitive domain in both genders using GAM, and how this relationship might differ by gender. This will allow us to understand which cognitive domain is the most or least affected by Hgb among older adults in respect to gender. Furthermore, clinicians need to understand the importance of Hgb on cognition and include routine blood work into care to carefully monitor their Hgb level especially for older adults with cognitive symptoms.
Our study also identified the critical inflection point for male (15.10 g/dL) and female (11.72 g/dL) older adults where the slope changed direction significantly. Among male older adults, the level of cognition increased until it reached the inflection point and decreased thereafter. Contrastingly, female older adults experienced an increasing level of cognition beyond the inflection point. An analysis of two large national databases (NHANES_III, SCRIPPS_Kaiser Data) found that the normal ranges for Hgb values remained unchanged for older adults, even when research shows that Hgb tends to decrease in this population (Beutler & Waalen, 2006). Typically, among older adults, there is an underlying etiology for lower Hgb level such as chronic disease, nutritional deficiency, or myelodysplastic syndromes (Goodnough & Schrier, 2014). As a result, the use of current guidelines to define low, normal, and high Hgb level among older adults may not be appropriate. Thus, the critical inflection point of 15.10 g/dL in males could be used as a standard to define high Hgb level among older adults, which is associated with cognitive decline. In female older adults, the inflection point did not significantly affect the association between Hgb and cognition. Findings from this study suggest that the inflection point of 11.72 g/dL could be used as an optimal Hgb level, which is slightly lower than the currently used optimal Hgb level of ≥12.6 g/dL in female older adults (Stauder et al., 2018). Our exploratory study might suggest that current standard guidelines for Hgb level may not be appropriate in older adults. Future confirmatory studies with a larger sample size should replicate the current study and identify the critical inflection points in both male and female older adults. In addition, future studies could further consider the similarities or differences in critical inflection points by different age groups: young-old (age 65–74), old-old (age 75–84), and oldest-old (age 85 and over) by gender (Min et al., 2023). Once the critical inflection points are identified through future research, they could be utilized as important Hgb guidelines for older adults in clinical practice.
Furthermore, our findings contribute to precision medicine by identifying the non-linear relationship between Hgb and cognition and the critical Hgb inflection point among older male and female adults. Precision medicine considers differences in individuals’ characteristics such as biomarkers, genetic, epigenetic, and other omics factors when providing care to patients (Fu et al., 2019). Herein, we focused on a specific type of biomarker (Hgb), and the role of biomarkers in precision medicine provides an innovative approach for technological developments to improve the health of individuals and reduce health-related costs (Slikker, 2018). Given the exploratory nature of our study, future studies should utilize Hgb when understanding cognition in male and female older adults and verify our results to further advance precision medicine. Such precision medicine-based approach should be incorporated in future clinical practice to carefully monitor Hgb level and cognition among older adults. As a result, clinicians could enhance precise diagnosis and assessment and deliver personalized interventions to those at risk for cognitive decline, especially among the male older adults (Fu et al., 2019).
There are several limitations to the study. First, we used cross-sectional data to examine the association between Hgb and cognition. Future studies should consider using longitudinal data to understand the temporal changes in the association between Hgb and cognition and identify critical time points where the level of cognition significantly decreases. Second, the study sample included older adults with normal cognition. There were two main reasons for sample selection: the majority of the participants with moderate and severe cognition had missing data on their cognition, and we followed the recommendation of previous research to conduct a study in a “healthy” cohort (Stauder & Thein, 2014). Future studies should include older adults with mild, moderate, and severe cognitive impairment and compare their association between Hgb-cognition. Third, we used objective measure to collect Hgb (dried blood spot sample) and to measure cognition (MOCA) among older adults. While these objective measures are deemed accurate, there is a potential for downward bias due to the differences in their measurement domains. Fourth, other important age-related covariates such as complete blood count, lipids, and inflammation biomarkers were not included in the current study due to limited data availability. Future studies should include these age-related biomarkers as covariates and examine the association between Hgb and hemoglobin. Herein, a larger sample size would be required to add more important covariates.
Conclusion
This exploratory study used GAM to identify the non-linear association between Hgb and cognition among older adults by gender. In addition, the critical inflection point of Hgb was identified for both male and female older adults. Particularly for men, the inflection point significantly affected the association pattern, where cognition increased up to the inflection point and decreased afterward. From a theoretical perspective, it might not be appropriate to consider the association between Hgb and cognition from standard parametric models. Future studies are needed to validate these results with a larger sample size and consider use of multiple cognitive domains, which can help develop precision medicine approaches and integrate our study findings into clinical practice. From a clinical perspective, clinicians can routinely assess and identify important Hgb level associated with cognitive decline and deliver personalized interventions to older adults at risk for cognitive decline with this new knowledge.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Se Hee Min is supported by the National Institute for Nursing Research training grant Reducing Health Disparities through Informatics (RHeaDI) (T32NR007969).