
Abstract
We aimed to assess the contribution of a- and presymptomatic residents and healthcare workers in transmission of SARS-CoV-2 in nursing homes. We conducted two serial point-prevalence surveys, including standardized symptom assessment and nasopharyngeal and oropharyngeal testing for SARS-CoV-2, among 297 residents and 542 healthcare workers of three Dutch nursing homes (NHs) with recent SARS-CoV-2 introduction. At the first point-prevalence survey, 15 residents tested positive of which one was presymptomatic and three remained asymptomatic. At the second point-prevalence survey one resident and one healthcare worker tested SARS-CoV-2 positive and both remained asymptomatic. Although a limited number of SARS-CoV-2 positive cases were identified, this study confirms a- and presymptomatic occurrence of Covid-19. We additionally describe factors that may contribute to the prevention of transmission. Taken together, our study complements the discussion on effective SARS-CoV-2 screening in NHs.
Introduction
Since the introduction of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), many nursing homes (NHs) worldwide have been hit by outbreaks of this new virus. In the Netherlands, at the time of conduction of the current study it was advised to perform SARS-CoV-2 testing in case of symptoms consistent with possible coronavirus disease 2019 (Covid-19). However, transmission of SARS-CoV-2 by a- and presymptomatic NH residents has been reported, which may warrant alternative screening policy in NHs (Arons et al., 2020; Goldberg et al., 2020). More evidence is needed to support adjustment of screening policy, thereby also including the role of healthcare workers in SARS-CoV-2 transmission. We therefore aimed to assess the contribution of a- and presymptomatic residents and healthcare workers in transmission of SARS-CoV-2 in three NHs in the Netherlands.
Methods
Setting and Study Population
The study was conducted in three NHs in the Netherlands with recent SARS-CoV-2 introduction (i.e., at least one SARS-CoV-2 positive resident): NH-A, NH-B, and NH-C, of which NH-B had a Covid-19 outbreak in the month preceding the study and recent newly identified cases. During the period of study conduction, the incidence of confirmed cases of COVID-19 varied from 0.6 to 2.1 cases per 100,000 inhabitants, and at study onset there were 628 NH locations with COVID-19 cases across the country (Dutch Ministry on Health, Welfare and Sport [VWS], 2020). It was national policy that all NHs were closed for visitors. Characteristics of participating NHs, including NH-specific Covid-19 policy at the time of study conduction, are presented in Table 1. All NHs implemented a policy of weekly testing of all residents and health care workers regardless of symptoms, while at the time of study conduction the national policy included testing in the occurrence of symptoms. All residents and health care workers were invited to participate.
Characteristics of the Participating NHs.

Note. NH = nursing home; PPE = personal protective equipment; Covid-19 = Coronavirus disease 2019.
With regard to healthcare workers, policy of the National Institute for Public Health and the Environment is followed, implying that all individuals with Covid-19 consistent symptoms stay home until they receive their SARS-CoV-2 test results. In case of a negative result, healthcare workers with mild symptoms are allowed to work, taking into account general hygiene precautions. Health care workers with a positive test stay home until minimal 7 days after symptom onset, and until they have been free of fever for at least 48 hours and free of symptoms for at least 24 hours. In exceptional situations, positive and symptomatic healthcare workers can work using PPE. In addition to the abovementioned policy, policy of the participating NHs in case of positive but asymptomatic healthcare workers was that these individuals stay home for 72 hours; national policy as stated above was followed if symptoms developed in the meantime, if no symptoms developed healthcare workers were allowed to work using PPE.
In general, Dutch NHs accommodate frail older adults who require complex and continuing care. Types of wards on which they can be accommodated include; somatic wards (i.e., for persons with mainly physical issues), psychogeriatric wards (i.e., for persons with cognitive disorders, mainly dementia), rehabilitation wards, and palliative care wards. Medical care is generally provided by elderly care physicians—a separate medical discipline in the Netherlands—who are employed by, and have their principal site of practice in the NH (Koopmans et al., 2017).
Serial Point Prevalence Survey
We conducted two serial point-prevalence surveys, including SARS-CoV-2 testing of all residents and healthcare workers, irrespective of whether they had been previously tested SARS-CoV-2 positive, and questionnaire completion. The first survey was performed in the week of May 4th, 2020, and was repeated 7 days later when tests were negative. SARS-CoV-2 positive individuals without symptoms or with atypical symptoms in the 14 days before their positive test were followed 14 days for development of symptoms.
Nasopharyngeal and oropharyngeal swabs were collected by trained healthcare workers and specialized swab teams from the Public Health Service, in accordance with national guidelines (Jacobi et al., 2020). Samples were transported to collaborating laboratories at the end of each test day, where they were tested for SARS-CoV-2 polymerase chain reaction (PCR) targets, see Supplemental Material.
Questionnaires were completed on the day of SARS-CoV-2 testing. Resident questionnaires were completed by healthcare workers, based on an interview with the resident and/or review of medical records; healthcare worker questionnaires were completed by the research team based on an interview with the healthcare worker, or online by healthcare workers themselves. The questionnaire included baseline characteristics (i.e., age and sex) and a standardized symptom-assessment form (for included signs and symptoms, see below). For residents, additionally documented were: ward name and type, comorbid conditions, previous Covid-19 disease, and recent admission or internal relocation. Healthcare workers were additionally asked for their type of profession (e.g., nurse assistant, nurse, physician), wards where they had worked the preceding 14 days, and personal protective equipment (PPE) use.
Analysis
A participant was classified symptomatic in case of at least one new/worsened typical or atypical symptom of Covid-19 in the 14 days before a positive SARS-CoV-2 test. Typical signs and symptoms included fever (measured according to local NH protocol), cough, and shortness of breath. Atypical symptoms included chills, malaise, fatigue, rhinorrhea, nasal congestion, sore throat, myalgia, headache, nausea or diarrhea, diminished food intake, and loss of smell or taste. For residents, (increased) confusion and decreased oxygen saturation (both measured according to local NH protocol) were also classified as atypical. A participant was classified presymptomatic if no symptoms were present the 14 days before a positive SARS-CoV-2 test, but typical or atypical symptoms developed during follow-up; when no symptoms developed during follow-up the participant was classified asymptomatic. Data were analyzed descriptively using Excel and SPSS version 26 (IBM, Armonk, NY).
Ethics
Residents, or their representatives in case of legal incapacity, were given the opportunity to opt-out for using their data in the study. Health care workers provided informed consent for using their data prior to questionnaire administration. The Medical Ethics Committee of Amsterdam University Medical Center, location VU University Medical Center, reviewed the study protocol and confirmed that the study does not fall under the scope of the Medical Research Involving Human Subjects Act.
Results
A total of 297 NH residents were included in the study (overall response: 86%; NH-A: 86%, NH-B: 90%, NH-C: 80%). 542 healthcare workers were included (overall response: 91%; NH-A: 94%, NH-B: 93%, NH-C: 87%). Demographic characteristics are presented in Tables 2 and 3.
Demographic Characteristics of Residents of Participating NHs.

In NH-B, data on care type was missing for 12 residents.
Demographic Characteristics of Healthcare Workers of Participating NHs.
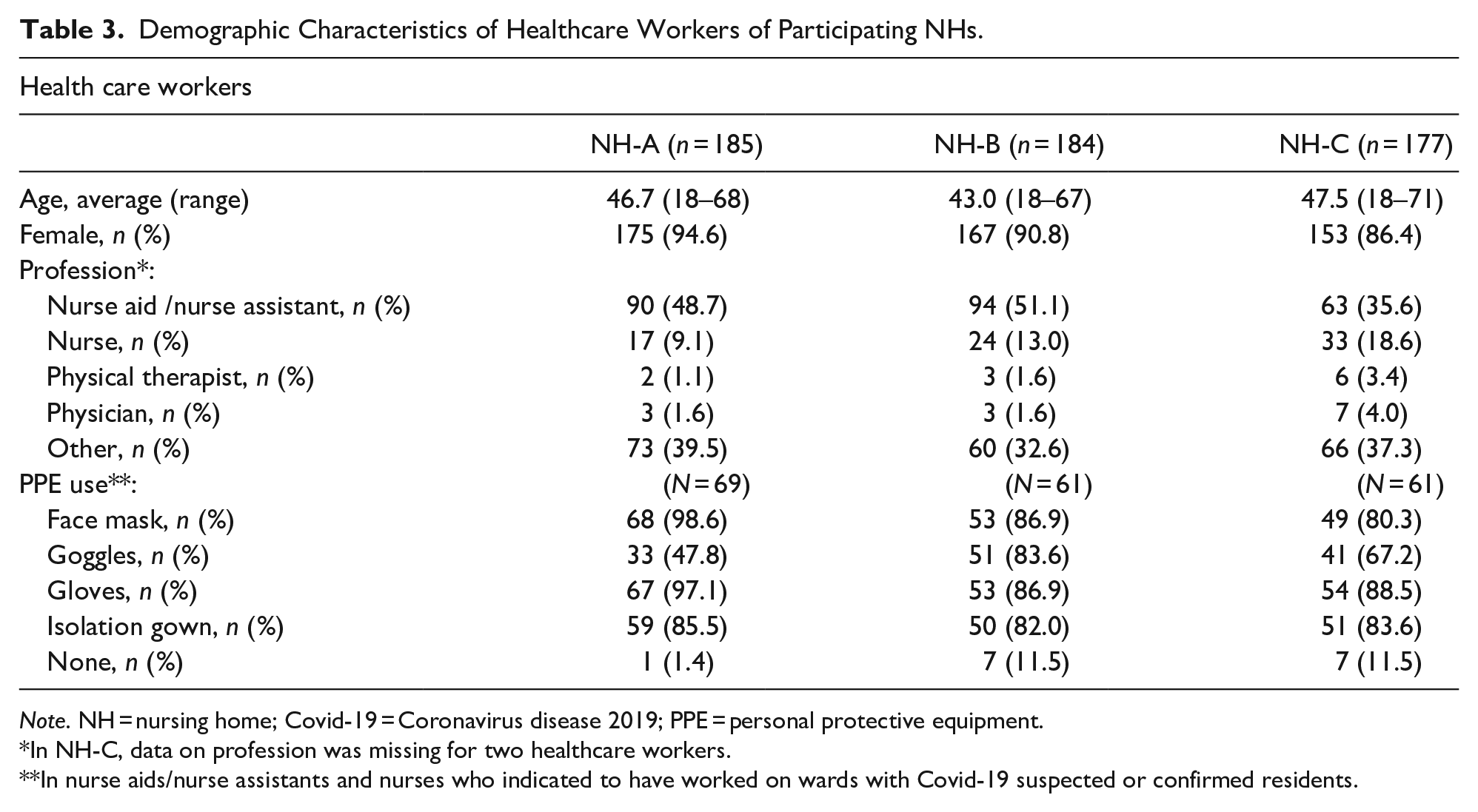
Note. NH = nursing home; Covid-19 = Coronavirus disease 2019; PPE = personal protective equipment.
In NH-C, data on profession was missing for two healthcare workers.
In nurse aids/nurse assistants and nurses who indicated to have worked on wards with Covid-19 suspected or confirmed residents.
At the first point-prevalence survey, 15 residents (5%) tested SARS-CoV-2 positive (NH-A: 1, NH-B: 11, NH-C: 3), of which nine (NH-B: 7, NH-C: 2) had a previous positive test result in the months preceding study onset. Of the six newly identified cases of SARS-CoV-2, two were symptomatic (both in NH-B; Cycle threshold (Ct) value 22 in both), one was presymptomatic (in NH-A; Ct value >35), and three remained asymptomatic during follow-up (two in NH-B and one in NH-C; Ct values 23, 30, and 32). A total of eight healthcare workers tested SARS-CoV-2 positive at the first point-prevalence survey (NH-B: 7, NH-C: 1). All had typical symptoms; five had not worked in the 2 weeks before the first point-prevalence survey. At the second point-prevalence survey, one resident and one healthcare worker in NH-A tested SARS-CoV-2 positive (Ct value >35 and 24, respectively). Both were asymptomatic on the day of testing.
Discussion
We aimed to study transmission of SARS-CoV-2 in three NHs with recent introduction of the virus, and to determine the role of a- and presymptomatic residents and healthcare workers herein. We identified three asymptomatic and one presymptomatic SARS-CoV-2 positive residents at the first point-prevalence survey. However, the number of cases identified in the follow-up survey was low (i.e., two in NH-A, none in NH-B and NH-C), which indicates very limited transmission and impeded the ability to answer the aforementioned research question. Nevertheless, we identified an asymptomatic resident and healthcare worker with Ct values below 25, suggesting that these cases have the potential to contribute to viral spread as previously suggested (Arons et al., 2020; Bullard et al., 2020; Goldberg et al., 2020).
Interestingly, the introduction of SARS-CoV-2 in two of the participating NHs (i.e., NH-A and NH-C) has not resulted in facility wide outbreaks during the study and the weeks thereafter. NH-B had an outbreak before the start of the study, and newly identified cases shortly before study onset. In response to the previous outbreak, this NH had taken measures such as increased hygiene precautions, the setup of cohorts of SARS-CoV-2 positive residents, and screening of healthcare workers for SARS-CoV-2, regardless of presence of symptoms (see also Table 1). The current study suggests that these measures were effective in this NH since no new transmission had occurred the weeks after the identification of new cases. This is supported by data where the implementation of repeated point prevalence surveys, including infection prevention consultations, resulted in mitigation of ongoing transmissions (Sanchez et al., 2020).
Other factors that may have contributed to the prevention of spread in the participating NHs include the decreased prevalence of Covid-19 in the Netherlands from mid-April until after study conclusion (National Institute for Public Health and the Environment [RIVM], 2020), reducing chances of new introductions of the virus in NHs. A high number of cases per capita have been identified as a predicting factor for outbreaks in NHs in previous studies (Gorges & Konetzka, 2020; Shi et al., 2020). In addition, whereas NHs were—due to scarcity of Covid-19 tests—previously advised to stop performing Covid-19 tests after two positive cases (and consider all symptomatic residents in that ward Covid-19 positive), the availability of Covid-19 tests had increased since April 10th. NHs had been able to perform low threshold testing ever since, facilitating early recognition of cases and, if appropriate measures are taken in response, decreasing chances of viral spread. Likewise, previously scarcely available PPE had become available on larger scale for NHs since April 13th. We indeed found high PPE use in the participating NHs (Table 3) and although we did not evaluate whether they were appropriately used, it is plausible that this contributed to the prevention of further spread. Finally, the constructional features of the NHs may have been beneficial in preventing transmission, for example, by the ability to physically separate wards, and an interior that facilitates quarantine and isolation measures. We did not collect data on the quality of the buildings’ ventilation systems; it may be interesting to include this in future studies, given previous calls to include building engineering controls as part of the infection control strategy (Morawska et al., 2020).
Our study contributes to the discussion on appropriate screening for SARS-CoV-2 in NHs. Similar to our study, Roxby et al. (2020) reported limited detection and transmission of SARS-CoV-2 in a NH with recent Covid-19 cases, upon screening of all residents and healthcare workers. There were asymptomatic residents among the identified cases, like in our study, which one may argue calls for policy beyond symptom-based screening. This is in line with recommendations of the European Center for Disease Prevention and Control (ECDC) to test all residents and healthcare workers once a confirmed case is detected (and in areas with ongoing community transmission, to test healthcare workers regularly even without any confirmed cases) (Danis et al., 2020). On the other hand, authors of a French study in which all healthcare workers of a NH were tested for SARS-CoV-2 after a first positive resident, argued that human and financial resources for systematic screening are disproportionate to its effectiveness (they identified only one asymptomatic individual) (Guery et al., 2020). The CDC advices initial testing of (asymptomatic) close contacts when testing capacity is limited: this could be a pragmatic alternative instead of facility wide testing at a first confirmed case (Center for Disease Prevention and Control [CDC], 2020).
Our study has several strengths. First, we were able to collect data on all possible contributors to transmission, that is, residents and healthcare workers, since visitors were not allowed in NHs at the time of study conduction. Second, response rates were high, which reduces chances of missing relevant numbers of Covid-19 cases in our study. A possible limitation is the limited amount of detail in the collected data (e.g., no registration of exact body temperature and oxygen saturation, no registration of previous Covid-19 in healthcare workers). We chose to keep the study questionnaire as short and simple as possible to reduce burden on healthcare workers, especially given their limited available time due to Covid-19 related understaffing. We anticipated that a lower questionnaire burden would contribute to the high responses required to study viral transmission.
Conclusion and Implications
Based on our findings, we argue that the necessity of large-scale screening in NHs may be dependent of the local situation regarding prevalence of cases in the surrounding community, infection control opportunities and testing capacity. If availability of equipment and constructional features facilitate rapid application of appropriate measures after a first identified case, this may suffice in preventing further transmission of SARS-CoV-2.
In conclusion; although we were not able to answer our predefined research question on the contribution of a- and presymptomatic cases in transmission of SARS-CoV-2, our study confirms a- and presymptomatic occurrence of Covid-19 among residents and healthcare workers. We described factors that may contribute to the prevention of SARS-CoV-2 transmission in NHs. Finally, our findings add to the discussion of effective Covid-19 screening policy in NHs.
Supplemental Material
sj-pdf-1-ggm-10.1177_2333721420982800 – Supplemental material for Asymptomatic Cases and Limited Transmission of SARS-CoV-2 in Residents and Healthcare Workers in Three Dutch Nursing Homes
Supplemental material, sj-pdf-1-ggm-10.1177_2333721420982800 for Asymptomatic Cases and Limited Transmission of SARS-CoV-2 in Residents and Healthcare Workers in Three Dutch Nursing Homes by Laura W. van Buul, Judith H. van den Besselaar, Fleur M. H. P. H. Koene, Bianca M. Buurman and Cees M. P. M. Hertogh in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
We thank all nurses and physician assistants of the participating NHs and Public Health Services for their contribution to and/or performance of SARS-CoV-2 testing. We thank the persons from Amsterdam UMC who assisted in questionnaire administration. We thank the NHs for their participation in the study in general, and in particular those individuals involved in logistic and/or administrative aspects of the study. We thank the laboratories of the Franciscus Gasthuis & Vlietland, Erasmus Medical Center, Public Health Service of Amsterdam, Wageningen Bioveterinary Research, and Microvida for the performance of SARS-CoV-2 tests.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Public Health and the Environment (Dutch: RIVM), Bilthoven, The Netherlands.
Ethical Approval
The Medical Ethics Committee of Amsterdam University Medical Center, location VU University Medical Center, reviewed the study protocol and confirmed that the study does not fall under the scope of the Medical Research Involving Human Subjects Act.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.