
Abstract
Introduction
Extensive progress has been made to reduce the United States’ cardiovascular disease (CVD) mortality rate; however, states such as Michigan continue to experience a disproportionate number of these deaths. According to the Michigan Department of Health and Human Services’ 2017 statistics, the age-adjusted heart disease mortality rate (per 1000,000) in Michigan is 1.18 times higher than the national rate (Michigan Department of Health and Human Services, 2019b). Additionally, Michigan’s heart disease rate has been substantially higher than the national rate since the early 2000s (Michigan Department of Health and Human Services, 2019a). A 2020 study by Dean and colleagues examined Michigan’s burden, which indicated that additional efforts are warranted to improve the cardiovascular health (CVH) of Michigan residents ≥50 years. The study’s outcomes showed that compared to Michigan residents <50, residents ≥50 years were more likely to have non-ideal levels for blood pressure and body mass index [BMI] (Dean et al., 2020). Moreover, a substantial percentage of Michigan residents ≥50 years have high blood cholesterol and are physically inactive (Dean et al., 2020).
Research shows that one’s CVH status may be, in part, attributable to their self-reported health-related quality of life (HRQL) (Odom, 2016). In 2016, Odom and colleagues conducted a cross-sectional study examining the association between U.S. adults’ CVH score and HRQL measures. This study’s results indicated that a lower CVH score was associated with reporting a fair/poor health status and experiencing ≥14 unhealthy physical and mental health, and limited activity days (Odom, 2016). This study highlights the significant association between HRQL and CVH status of U.S. adults.
Additionally, several studies have identified a significant relationship between CVH status and social determinants of health (SDOH) (Dean et al., 2020; Havranek et al., 2015). Specifically, Michiganders ≥50 years with an income of less than $15,000 had a mean CVH score of 2.85 out of 6.00 (Dean et al., 2020). This is substantially lower than their counterparts’ mean CVH score (3.60) with an income >$50,000 (Dean et al., 2020). Although the relationship between CVH and HRQL and CVH and SDOH have been examined, there is a gap in the literature on the relationship between CVH status, perceived HRQL, and SDOH among adults ≥50 years. With the known disease burden and complexity of middle-aged and older adults’ health needs, understanding the association between CVH status, HRQL, and SDOH can inform interventional efforts. In particular, interventions to improve the CVH of Michigan residents ≥50 years. Therefore, this study’s objective was to examine SDOH associated with Michigan residents ≥50 years HRQL measures and CVH status.
Methods
Participants
Michigan-level data was extracted from the 2017 Behavioral Risk Factor Surveillance System (BRFSS), a survey that examines residents’ health behaviors and risks (Behavioral Risk Factor Surveillance System, 2018). BRFSS is a state-based telephone survey conducted annually among U.S. adults ≥18 years who are living in a household (Behavioral Risk Factor Surveillance System, 2018). Additional details on questionnaire development and dissemination are available in the BRFSS overview (Behavioral Risk Factor Surveillance System, 2018). Michigan residents who self-reported being ≥50 years were included in the study because previous research indicates this population has a higher CVD risk (Dean et al., 2020).
Measures
Dependent
The dependent variables included “CVH and mental health status,” “CVH and physical health status,” “CVH and general health status,” and “CVH/HRQL score.” The following describes the derivation of these variables.
CVH status
Participants’ responses to BRFSS questions for six CVH metrics were dichotomized to (non-ideal vs. ideal) to reflect the American Heart Association’s recommendations for ideal CVH (Lloyd-Jones et al., 2010). This categorization has been mirrored in previous research (Odom, 2016). These questions included: “Have you EVER been told by a doctor, nurse or other health professional that you have high blood pressure?” (yes, yes, but female told only during pregnancy, no, or no, told pre-hypertensive) to (yes vs. no); “Have you EVER been told by a doctor, nurse or other health professional that your blood cholesterol is high?” (yes vs. no); and “Ever told you have diabetes?” (yes, yes, but female told only during pregnancy, no, or no, told pre-diabetic) to (yes vs. no).
Physical activity was developed from three questions, “During the past month, other than your regular job, did you participate in any physical activities or exercises such as running, calisthenics, golf, gardening, or walking for exercise?” (yes/no); “How many times per week or per month did you take part in this activity during the past month?” (in times per week and month); and “And when you took part in this activity, for how many minutes or hours did you usually keep at it?” (in hours and minutes) in which BRFSS calculated the number of minutes of physical activity (0–149 minutes—or vigorous equivalent minutes vs. 150 minutes—or vigorous equivalent minutes).
Smoking status was developed based on two questions, “Have you smoked at least 100 cigarettes in your entire life?” (yes/no), and “Do you now smoke cigarettes every day, some days, or not at all?” (every day, some days, or not at all). These questions were combined to non-ideal vs. ideal of “smoked at least 100 cigarettes in lifetime and now smoke every day” or “smoked at least 100 cigarettes” versus “smoked at least 100 cigarettes in lifetime and currently do not smoke” or “had not smoked at least 100 cigarettes in lifetime.”
The BMI variable [BMI = (kg/m2) weight/(height × height)] was calculated by BRFSS from the questions, “About how tall are you without shoes?” (in meters) and “About how much do you weigh without shoes?” (in kilograms). The calculated variable was recategorized to “≥25 kg/m2” versus “<25 kg/m2.”
The CVH score variable was created from the metrics above. The score of 0 to 4 indicated a non-ideal CVH status versus a score of 5 to 6 denoted having an ideal CVH status, coinciding with research showing a CVH score of ≥5 is associated with an 88% risk reduction in CVD-related mortality (Ford et al., 2012).
HRQL status
The HRQL-related BRFSS questions utilized in this study have been used to examine perceived HRQL in previous research (Odom, 2016). The questions’ response options were dichotomized to ideal versus non-ideal; “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?” recoded to <14 versus ≥14 days; “Now thinking about your physical health, which includes physical illness and injury, for how many days during the past 30 days was your physical health not good?” recoded to <14 versus ≥14 days; and “Would you say that in general your health is excellent, very good, good, fair, or poor?” recoded to “excellent, very good, and good” versus “fair/poor.”
The CVH status and HRQL measures were combined to create three of the four dependent variables: CVH and mental health status, CVH and physical health status, and CVH and general health status. Each variable’s responses ranged from 0 to 2, with “0” meaning a non-ideal status, “1” representing a moderate status, and “2” indicating an ideal status:
1. CVH and mental health status “0” representing non-ideal CVH and non-ideal general health, “1” indicating non-ideal CVH and ideal general health/ideal CVH and non-ideal general health, and “2” denoting ideal CVH and ideal general health.
2. CVH and physical health status “0” symbolizing non-ideal CVH and non-ideal physical health, “1” indicating non-ideal CVH and ideal physical health/ideal CVH and non-ideal physical health, and “2” denoting ideal CVH and ideal physical health.
3. CVH and general health status “0” denoting non-ideal CVH and non-ideal general health, “1” indicating non-ideal CVH and ideal general health/ideal CVH and non-ideal general health, and “2” denoting ideal CVH and ideal general health.
The aforementioned variables were combined to create the fourth dependent variable, CVH/HRQL score. This variable was dichotomized to higher CVH/HRQL score versus lower CVH/HRQL score with a lower CVH/HRQL score signifying non-ideal CVH and reporting ideal for ≤2 HRQL measures.
SDOH
Determinants incorporated were guided by the World Health Organization’s SDOH framework for structural and intermediary determinants (World Health Organization, 2010). Structural determinants included sex (male/female), and race/ethnicity, which was recoded from “White, Black, Hispanic, Asian, Multiracial, American Indian/Alaskan Native, Native Hawaiian/other Pacific Islander, or Other” to White, Black, Hispanic, or Other to address limited responses. Additional variables included were education level (less than high school, high school, some college, and graduate degree), income (<$15,000, $15,000–$24,999, $25,000–$34,999, $35,000–$49,000, and >$50,000) recoded to (<$25,000, $25,000–$50,000, >$50,000), and employment status (employed for wages, self-employed, out of work >1 year, out of work <1 year, homemaker, student, retired, and unable to work) recoded to “employed for wages, self-employed, out of work, retired, and other (homemaker, student, or unable to work).”
Intermediary variables included marital status (married, divorced, widowed, separated, never married, and member of an unmarried couple) with divorced, separated, and member of unmarried couple combined to address limited responses. Additionally, have health insurance (yes/no), unable to visit provider past 12 months due to medical cost (yes/no), metropolitan status (center of city, outside city center, inside suburban, and not in metropolitan status area), ever told depressed by provider (yes/no), last routine healthcare visit (past year, 2 years, 5 years, ≥5 years, and never), with 5 years, ≥5 years, and never combined to address limited responses. Household size was included and calculated from survey responses on the number of adults and children in household.
Statistical Analyses
Utilizing STATA MP14 (Stata, 2015), the data were weighted to extrapolate state-level estimates. Multinomial and binary logistic regression analyses identified SDOH associated with Michiganders ≥50 years CVH and HRQL status.
Results
The sample consisted of 10,889 participants. The multinomial and binary logistic regression models identified SDOH associated with residents’ CVH and HRQL status (Table 1). Male participants had 1.45 higher odds of having a lower CVH/HRQL score compared to female participants (95% CI: 1.11–1.90).
Relationship between CVH, General, Physical, and Mental Health Status, and Social Determinants of Health.
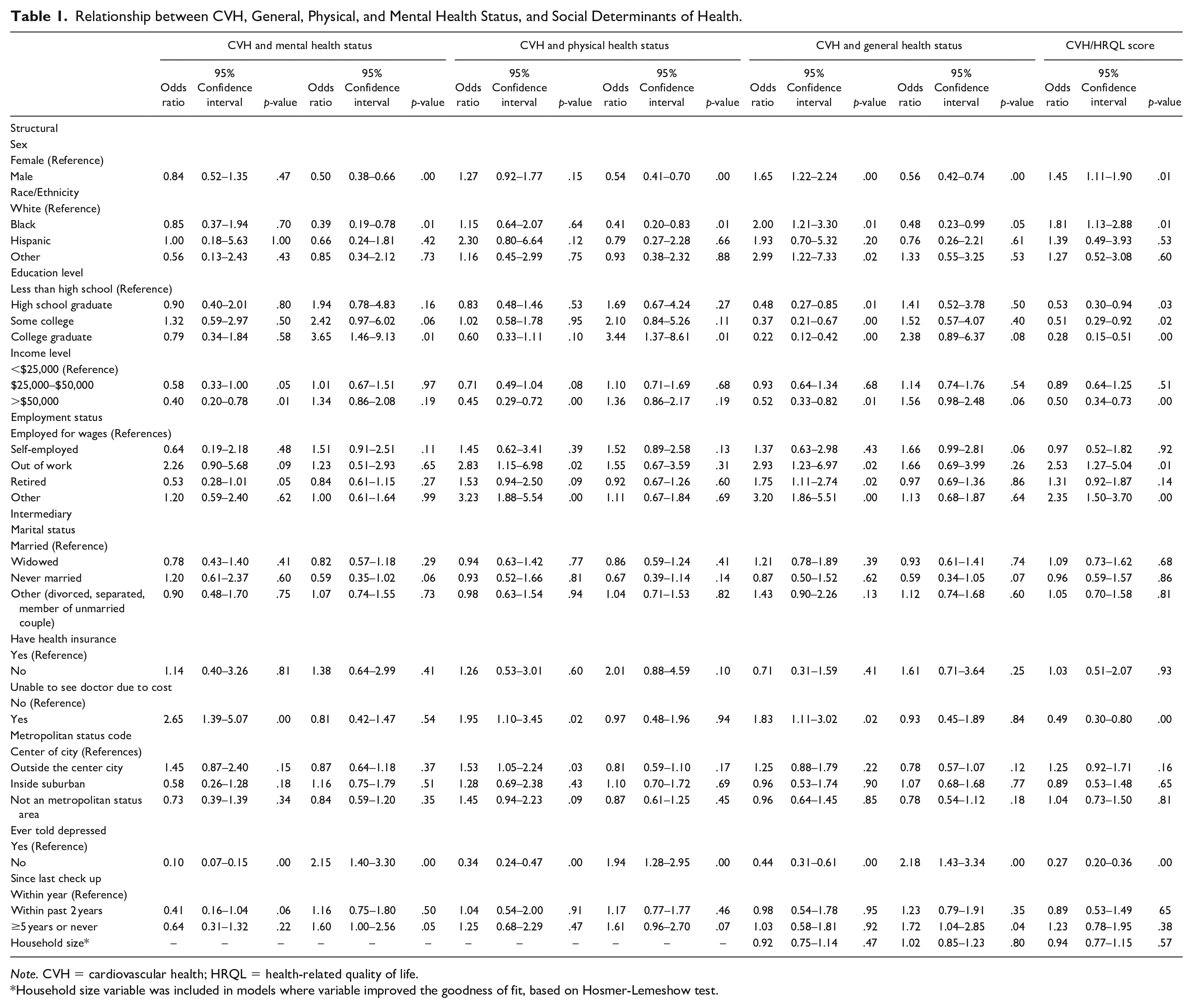
Note. CVH = cardiovascular health; HRQL = health-related quality of life.
Household size variable was included in models where variable improved the goodness of fit, based on Hosmer-Lemeshow test.
Among structural determinants, compared to residents with a moderate CVH and mental health status, residents who reported unable to visit a doctor due to costs were two times more likely than those who were able to visit a provider to have a non-ideal CVH and mental health status (OR = 2.65; 95% CI: 1.39–5.07). This relationship was also reflected among non-ideal CVH and physical health status (OR = 1.95; 95% CI: 1.10–3.45) and non-ideal CVH and general health status individuals (OR = 1.83; 95% CI: 1.11–3.02) when compared to their moderate counterparts.
Discussion
This is the first study to examine CVH, HRQL, and SDOH among adults ≥50 years in which significant structural and intermediary determinants were identified. Males were more likely to have a lower CVH/HRQL score than females. Residents who reported unable to visit a doctor due to costs had higher odds of having a non-ideal CVH and HRQL status. Although no previous studies have examined the relationship between CVH, HRQL, and SDOH among adults ≥50 years, previous research has demonstrated the impact of SDOH on CVH status (Dean et al., 2020). Specifically, research has shown males ≥50 years and individuals unable to visit a doctor due to cost to have a lower CVH score (Dean et al., 2020). This study’s findings add to the literature by highlighting that a non-ideal HRQL increases the risk among residents with these determinants.
Several study limitations should be considered. Diet is one of the leading CVH metrics; however, the BRFSS survey does not collect comprehensive dietary data. Not including this information may have led to an under- or over-estimation of the findings. The number of activity limitation days have been previously included in research to examine HRQL, but it was not included in this study because of limited responses by the number of activity limitation days and CVH status. This also may have led to the over- or under-estimation of participants’ HRQL. Participants self-reported their CVH metrics (e.g., height, weight), which allows for bias within the findings.
Conclusion
The study’s outcomes identified SDOH associated with non-ideal CVH and HRQL status among Michiganders ≥50 years. Moreover, it illustrates the need for a multifactorial intervention that fosters CVH behavior changes, enhances perceive HRQL, and addresses influential SDOH among residents. Further research should be performed to determine the generalizability of the results.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
This study consist of secondary de-identified data; therefore, participant consent was not obtained.