
Abstract
The 2019 novel coronavirus disease (COVID-19) has broadly impacted our daily lives. Here, we used a longitudinal approach to investigate older adults’ mood and expectations regarding aging before and during the global pandemic (Study 1). We also examined age differences in mood, expectations regarding aging, COVID-19 attitudes, and loneliness using a cross-sectional approach (Study 2). In Study 1, older adults completed a mood and expectations regarding aging survey up to 2 years prior to the pandemic and again in April, 2020 (during the pandemic). Participants also completed surveys regarding COVID-19 attitudes and loneliness. In Study 2, a United States sample of younger and older adults completed these surveys during the pandemic. Older adults’ mood and expectations regarding aging remained fairly constant, and younger adults showed lower mood and expectations regarding aging than did older adults, despite older adults showing greater concern about COVID-19. Overall, we find that some older adults seem to be resilient with respect to their mood and expectations regarding aging. These findings reveal important preliminary implications for how older adults may be impacted as a result of lifestyle changes necessary for well-being and the well-being of society.
When the World Health Organization declared the 2019 novel coronavirus disease (COVID-19) a pandemic in March 2020, people were urged to “social distance” by limiting their activity in public spaces, refraining from in-person visits with family and friends, and maintaining a distance of 6 feet from others when engaging in essential activities. As a consequence, many older adults who had active social lives likely experienced major changes in their routines, leading them to feel isolated, lonely, or have decreased mood. Further, almost one third of older adults live alone (Administration on Aging, 2018), many already experience loneliness (Gerst-Emerson & Jayawardhana, 2015), and increased loneliness may lead to a multitude of negative mental and physical health outcomes in both younger adults (Jaremka et al., 2014) and older adults (Ong et al., 2016). Some work has investigated older adults’ worries about COVID-19 (Barber & Kim, 2020), but it is unclear whether COVID-19 has influenced older adults’ overall mood.
COVID-19 can be dangerous for people of any age, but mortality rates are higher for those aged 65 and older (CDC, 2020; Hauser et al., 2020). At the onset of the pandemic, older adults (aged 65+) made up 43.4% of COVID-19-related hospitalizations, and the rate of hospitalization for this group was almost double that of those aged 50 to 64 years, which was three times higher than for 18 to 49 year-olds, demonstrating the striking increase in COVID-19-related health risks with increasing age (Garg, 2020). Widespread media focus on the impact of COVID-19 on older adults as a fragile population could also lead older adults to feel more vulnerable and affect attitudes about aging (Ayalon et al., 2020). Some work has shown that older adults’ physical and mental health can be influenced by societal attitudes about aging (Chang et al., 2020). Swift et al. (2017) describe the Risks of Ageism Model (RAM), which posits that societal ageism (e.g., economic, social, and psychological factors) contributes to both negative self-perceptions of age stereotypes and an increased likelihood of being a target of ageism in older adults. These experiences, in turn, serve as barriers to experiencing independence, autonomy, and higher quality of life. Thus, a widespread focus on the fragility of older populations during the pandemic could have negative effects on older adults’ attitudes or expectations about aging. Unfortunately, negative attitudes about aging are related to a variety of health outcomes in older adults, including lower survival rates and physical and mental health issues (Breda & Watts, 2017; Han & Richardson, 2014). Anxiety about aging can even explain some of the relationship between one’s environment and loneliness (Ayalon, 2018), suggesting that negative aging attitudes could exacerbate feelings of loneliness (see also Shiovitz-Ezra et al., 2018). On the other hand, positive attitudes about aging have been associated with more new friends in older adulthood (Menkin et al., 2017), which could prevent loneliness.
Given the increased risk of hospitalization or death due to COVID-19, older adults may take greater preventive measures and hold more serious attitudes toward COVID-19 than younger adults. It is unclear, however, how attitudes about COVID-19 relate to outcomes like mood or attitudes about aging, or whether this relationship is different between younger and older adults. Those with more serious attitudes about COVID-19 may experience greater loneliness or decreased mood if they are isolating to a greater extent, but people may also feel safer and thus more positive if they are taking the recommended precautions. In the current studies, we examined mood, expectations regarding aging, coronavirus attitudes, and loneliness in younger and older adults.
Study 1
In the first study, we examined mood and expectations regarding aging before and during the coronavirus pandemic. A sample of older adults who provided responses to surveys from January 2018 to December 2019 completed follow-up surveys during the course of the pandemic, and response differences were analyzed.
Method
Participants
Eighty-six older adults who completed the Expectations Regarding Aging (ERA) and Brief Mood Introspection Scale (BMIS) between January 2018 and December 2019 (Time 1) were contacted to participate. Forty-nine participants (Mage = 73.90 years, SDage = 7.50 years) provided responses between April 7 and May 2, 2020 (Time 2). Two participants did not respond to the BMIS at Time 1 but did respond to all surveys at Time 2. All participants reported residing in the United States at the time of data collection, and all other demographic information is presented in Table 1. Of those who did not respond at Time 2, 17 never responded to outreach, 12 were contacted and interested but did not participate before the deadline, three were unreachable, and five were reached but were not interested. To examine whether those who responded were demographically different from those who did not, we conducted chi-square tests for independence and found that older adults who participated at Time 2 and those who did not showed no significantly different makeup of gender, χ2 (1, N = 86) = 0.16, p = .69, ethnicity, χ2 (2, N = 86) = 1.17, p = .34, race, χ2 (4, N = 86) = 4.93, p = .29, nor education, χ2 (3, N = 86) = 4.41, p = .22. There was also no difference in age, t(84) = 1.08, p = .29, nor in self-reported health, t(84) = 0.24, p = .81, between participants who responded at Time 2 and those who did not.
Demographic Information for Participants in Studies 1 and 2.

Note. Study 1 participants’ data from Time 2. Self-reported health was provided on a scale from 1 (poor) to 10 (excellent).
Materials and procedures
This study used a longitudinal approach to examine differences in outcomes across two time points. Participants were contacted by email, but given the option of completing the surveys over the phone if they were uncomfortable with computers or if it was easier for them. Most (n = 41) chose to complete the surveys online. All procedures were approved by the University of California, Los Angeles Institutional Review Board, and informed consent was obtained. After self-reporting health on a 1 (poor) to 10 (excellent) scale, participants completed the BMIS (Mayer & Gaschke, 1988), which contains 16 adjectives rated on a 1 (definitely do not feel) to 7 (definitely feel) Likert scale, as well as an overall mood item rated from −10 (very unpleasant) to 10 (very pleasant). The BMIS assesses four constructs related to participants’ mood. First, the pleasant-unpleasant scale, which includes responses from all items, indicates a participant’s overall mood valence, with higher scores indicating more pleasant mood. The arousal-calm subscale provides a measure of how aroused (i.e., jittery, excited, nervous) participants are, independent of the valence of those emotions, with lower scores indicating less aroused or more calm mood. The positive-tired subscale assesses positive mood, with lower scores indicating less positive or more tired mood, and the negative-relaxed subscale measures negative mood, with lower scores indicating less negative or more calm mood.
Participants also completed the 12-item ERA scale (Sarkisian et al., 2005), which measures attitudes about aging. Participants rated statements about older age that apply both personally (e.g., “I expect that as I get older, I will become more forgetful.”) and more broadly (e.g., “Having more aches and pains is an accepted part of aging.”). The ERA is composed of three subscales: Cognitive Function, Physical Health, and Mental Health, all rated from 1 (definitely true) to 4 (definitely false), and then converted to a 0 to 100 scale. Lower scores indicate expectations of decline in older age, while higher scores represent higher expectations, including expecting achievement and high functioning in older age.
Participants then completed the Attitudes and Prevention subscales of a new COVID-19 Pandemic scale (Priniski, 2020), which measures participants’ attitudes and opinions about the impact of COVID-19. The scale was modeled after a scale measuring vaccine skepticism and beliefs about diseases like measles and mumps (Powell et al., 2018). After reading a brief definition of COVID-19, participants provided responses on a Likert scale from 1 (strongly disagree) to 7 (strongly agree) to a series of statements such as “COVID-19, commonly referred to as coronavirus, is no more severe than the flu.” Lower scores indicate more serious attitudes and prevention intentions. After responding to a few open-ended questions about their behavior during the pandemic, participants then completed a 3-item version of the UCLA Loneliness Scale (Hughs et al., 2004). The items (e.g., “How often do you feel that you lack companionship?”) were rated on a scale of 1 (hardly ever) to 3 (often), with higher scores indicating greater feelings of loneliness.
Results
Expectations regarding aging
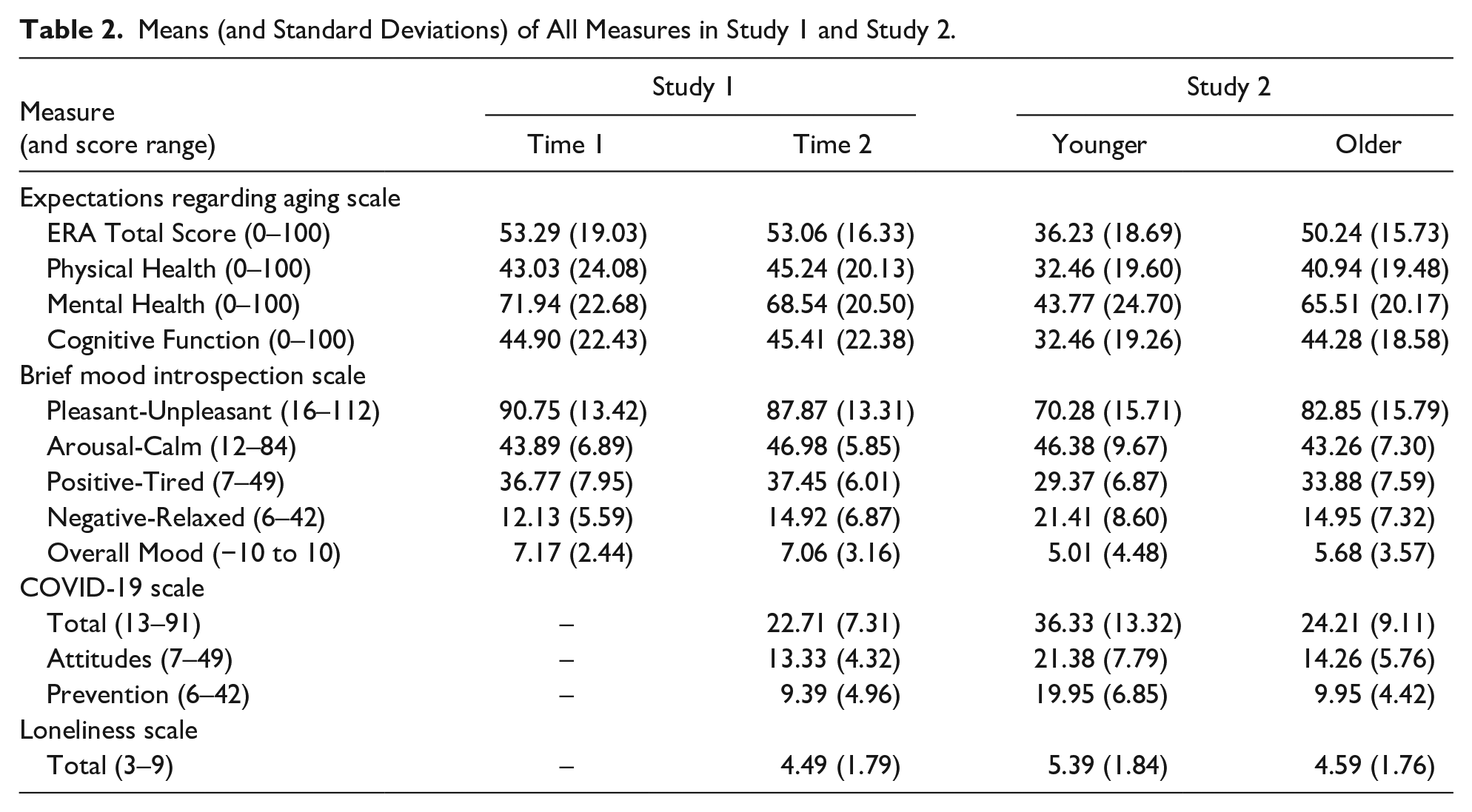
We conducted dependent-samples t-tests on each of the ERA subscales and on the total ERA score. All means and standard deviations are reported in Table 2. There were no significant differences between Time 1 and Time 2 scores on the Physical Health, t(48) = 0.65, p = .52, d = 0.09, Mental Health, t(48) = 1.42, p = .16, d = 0.20, or Cognitive Function subscales, t(48) = 0.16, p = .87, d = 0.02. There was also no change in total ERA score from Time 1 to Time 2, t(48) = 0.11, p = .91, d = 0.02.
Means (and Standard Deviations) of All Measures in Study 1 and Study 2.
To determine the validity of the null effects between time points, we calculated a Bayes Factor for each test, which gives a measure of the strength of the evidence for the null or alternative hypotheses based on a priori hypotheses and the data (see Kruschke, 2013; Wagenmakers et al., 2017 for discussions of the benefits of using Bayes Factors). As interpreted by guidelines in Lee and Wagenmakers (2013), the Bayesian paired-samples t-tests using default Cauchy priors indicated “moderate” evidence in favor of the null hypothesis (i.e., no difference between Time 1 and 2) on the Physical Health (BF01 = 5.26), Cognitive Function (BF01 = 6.36), and total ERA (BF01 = 6.40) scores, but only “anecdotal” evidence on the Mental Health score (BF01 = 2.53). These values indicate that the data for the Physical Health measure were 5.26 times more likely to occur under the null relative to the alternative model, the data for Cognitive Health were 6.36 times more likely under the null model, and so on. Thus, the results provide moderate evidence of consistent ERA physical, cognitive, and total scores between Time 1 and 2, with inconclusive evidence on mental health scores. In subsequent analyses, we report Bayes Factors for null effects.
Mood
We scored the BMIS according to Mayer (2018) to obtain subscale scores on the following dimensions: pleasant-unpleasant (ranging from 16 to 112), arousal-calm (ranging from 12 to 84), positive-tired (ranging from 7 to 49), and negative-relaxed (ranging from 6 to 42). There were no differences between Time 1 and Time 2 on overall mood ratings, t(46) = 0.23, p = .82, d = 0.03, BF01 = 6.16, or overall pleasant-unpleasant ratings, t(46) = 1.77, p = .08, d = 0.26, BF01 = 1.50. In addition, there were no significant differences in the positive-tired subscale at Time 1 and Time 2, t(46) = 0.71, p = .48, d = 0.10, BF01 = 4.97. However, scores on the arousal-calm subscale were significantly higher at Time 2 than Time 1, t(46) = 3.06, p = .004, d = 0.45, as were scores on the negative-relaxed subscale, t(46) = 3.35, p = .002, d = 0.49. The Bayes Factors for the null effects here support moderate evidence for the lack of change in positive mood, but only anecdotal evidence for the lack of change in pleasant mood. Thus, while mood did not become less positive, participants were more aroused and had more negative (less calm) mood at Time 2 than at Time 1.
Correlations between expectations, mood, and COVID-19
The means for the COVID-19 and loneliness scales are displayed in Table 2. Relevant Pearson’s correlations are discussed here, and all correlations between measures at Time 2 are shown in Figure 1. In all analyses, correlation matrices were computed in R (Version 4.0.1, R Core Team, 2020) using the stats (Version 4.0.1, R Core Team, 2020) package, and p-values were computed using the “cor_pmat” function in the ggcorrplot (Version 0.1.3, Kassambara, 2019) package; correlation matrix figures were generated using the corrplot (Version 0.84, Wei & Simko, 2017) package with RColorBrewer (Version 1.1-2, Neuwirth, 2014). The correlations revealed that those with higher expectations about aging had more pleasant mood, r(47) = 0.50, p < .001. In addition, higher loneliness scores were associated with significantly lower ERA scores, r(47) = −.33, p = .02, and BMIS scores, r(47) = −.43, p = .003. Higher health ratings were associated with higher ERA scores, r(47) = .37, p = .01, and BMIS scores, r(47) = .36, p = .01. Lastly, COVID-19 scores were not associated with health, r(47) = .02, p = .89, ERA scores, r(47) = .08, p = .58, or BMIS scores, r(47) = .18, p = .24, but were associated with loneliness scores, r(47) = −.30, p = .04, such that taking COVID-19 more seriously was associated with greater loneliness.

Pearson’s correlations between measures from older adults in Study 1 (left) and younger and older adults in Study 2 (right). Each cell shows the correlation coefficients, with significant correlations containing a circle (p-values are represented in the top-right corner). The size and color of each circle is proportional to the magnitude of the correlation, with cooler colors indicating positive correlations and warmer colors indicating negative correlations.
Discussion
In Study 1, we found that overall, our sample of older adults was maintaining positive mood and expectations about aging during the COVID-19 pandemic, but that they reported more negative arousal. In addition, loneliness was negatively related to both attitudes about aging and mood pleasantness. Thus, while older adults do not seem to be entirely unaffected by the COVID-19 pandemic, this sample of older adults seemed to maintain positive mood and attitudes about aging overall.
Study 2
In Study 2, we attempted to replicate findings from Study 1 regarding loneliness, COVID-19 attitudes, mood, and expectations regarding aging in a larger sample of older adults. We also examined age-related differences in mood, expectations about aging, loneliness, and attitudes toward COVID-19 in a national sample of older and younger adults.
Method
Participants
The participants in Study 2 were younger and older adults recruited using Prime Panels on CloudResearch (formerly known as TurkPrime; www.cloudresearch.com). Similar to other online data collection platforms like Amazon Mechanical Turk (MTurk), CloudResearch’s Prime Panels allows for researchers to target and collect large, diverse samples of participants. Prime Panels participants have been shown to produce similar rates of passing attention checks and similar effect sizes as other online and in-lab samples, while being more representative of the U.S. population (Chandler et al., 2019). Prime Panels also has a larger proportion of older adults, with over 23% of participants over the age of 60 relative to 3.3% of MTurk participants meeting the same criterion (Chandler et al., 2019; Huff & Tingley, 2015). As such, despite obvious limitations inherent to online data collection, Prime Panels is a useful tool to efficiently obtain quality older adult data.
Participants were restricted to be ages 18 to 30 or 60+ and to reside in the United States. The older adult age range was restricted so as to match that of Study 1, and the younger adult range is consistent with recent similar research (e.g., Barber & Kim, 2020). To ensure participants were paying attention, we used a measure of participants’ focus (i.e., the proportion of time in which a participant’s computer mouse was present on the browser page), and participants were excluded from the experiment if they had less than 0.75 (out of 1.00) focus for the duration of the survey. Participants were also excluded if they selected the incorrect response on an attention check question. The survey was completed in median time of 9.59 min (IQR = 6.46–13.25 min). The final sample consisted of 115 younger adults (Mage = 25.15 years, SDage = 3.63 years) and 115 older adults (Mage = 69.70 years, SDage = 6.16 years) who were compensated $2.00 for their participation. Other relevant demographic information is presented in Table 1.
Materials and procedure
The same materials used in Study 1 were also used in Study 2. Participants completed a demographics form and the ERA, BMIS, COVID-19 Pandemic, and loneliness surveys. This study used a cross-sectional design to examine age differences in outcomes.
Results
Expectations regarding aging
We conducted independent samples t-tests on each of the ERA subscales and the total ERA score. 1 Means for all measures are shown in Table 2. Older adults had higher scores on the Physical Health, t(228) = 3.29, p = .001, d = 0.43, Mental Health, t(219.2) = 7.31, p < .001, d = 0.96, and Cognitive Function, t(228) = 4.73, p < .001, d = 0.62 subscales than did younger adults. Additionally, older adults provided higher total ERA ratings than did younger adults, t(221.6) = 6.15, p < .001, d = 0.81.
Mood
On average, there was no difference between older and younger adults’ overall mood, t(228) = 1.25, p = .21, d = 0.17, BF01 = 3.40. However, older adults scored significantly higher than younger adults on the pleasant-unpleasant scale, t(228) = 6.05, p < .001, d = 0.80, and on the positive-tired subscale, t(228) = 4.72, p < .001, d = 0.62. Conversely, younger adults scored significantly higher than older adults on the arousal-calm subscale, t(228) = 2.76, p = .01, d = 0.36, and on the negative-relaxed subscale, t(222.3) = 6.14, p < .001, d = 0.81. Younger adults were also significantly lonelier than older adults, t(228) = 3.37, p < .001, d = 0.44. Overall, younger adults had less positive and more negative mood and reported experiencing greater arousal than older adults.
COVID-19 pandemic behaviors, attitudes, and opinions
We calculated attitude and prevention subscale scores for the COVID-19 survey. Older adults had more positive attitudes about the COVID-19 pandemic than younger adults, t(210) = 7.88, p < .001, d = 1.04. Older adults also reported more concern about COVID-19 prevention than younger adults, t(195) = 6.58, p < .001, d = 0.87. Overall scores on the COVID-19 scale were higher in younger adults than in older adults, t(202) = 8.06, p < .001, d = 1.06. Thus, older adults reported taking the COVID-19 pandemic more seriously and engaging in preventative behaviors to a greater extent than younger adults.
Correlations between expectations, mood, and COVID-19
Pearson’s correlations were conducted within each age group to examine associations between overall ERA score, BMIS pleasant-unpleasant mood, COVID-19 score, loneliness rating, and relevant demographic factors like age, gender, education, income, and overall health. Significant correlations of interest are discussed here (with additional correlations presented in Figure 1). For older adults, higher ERA scores were associated with more pleasant mood, r(113) = .40, p < .001, lower loneliness ratings, r(113) = −.25, p = .006, higher health ratings, r(113) = .34, p < .001, and gender, r(113) = .22, p = .02. In addition, greater loneliness was associated with more unpleasant mood, r(113) = −.48, p < .001, lower health ratings, r(113) = −.20, p = .03, lower income, r(113) = −.21, p = .03, and being female, r(113) = .29, p = .002. More pleasant mood was also associated with better health, r(113) = .37, p < .001, and higher income, r(113) = .25, p = .01. Lastly, COVID-19 scores were not significantly correlated with ERA, r(113) = −.02, p = .87, BMIS, r(113) = .03, p = .78, loneliness, r(113) = −.17, p = .07, nor health, r(113) = .06, p = .50, but were correlated with gender, r(113) = −.34, p < .001, such that females expressed more serious attitudes and prevention toward COVID-19 than males.
In younger adults, lower expectations regarding aging were associated with more unpleasant mood, r(113) = .27, p = .004, higher loneliness, r(113) = −.20, p = .03, higher age, r(113) = −.25, p = .01, higher income, r(113) = −.19, p = .04, higher education, r(113) = −.30, p = .001, and being male, r(113) = .28, p = .002. More unpleasant mood was associated with less COVID-19 concern and prevention intent, r(113) = −.21, p = .02, higher loneliness, r(113) = −.43, p < .001, and lower health ratings, r(113) = .26, p = .01. Similar to older adults, female younger adults reported higher COVID-19 concern, r(113) = −.31, p < .001.
Discussion
In Study 2, we found that older adults reported more positive mood and higher expectations about aging than younger adults did, supporting the finding that older adults, in general, were maintaining positivity following the onset of the COVID-19 pandemic. We also replicated in both younger and older adults the finding that more frequent feelings of loneliness were related to lower expectations regarding aging and more unpleasant mood. In addition, females were taking COVID-19 more seriously, reported higher expectations regarding aging, and were in better health, but female older adults were lonelier than males. Lastly, older adults expressed greater concern for COVID-19 than younger adults did, suggesting that they are taking it more seriously.
General Discussion
The current findings suggest older adults are, in general, maintaining their expectations about aging and mood amidst a global pandemic, showing similar ratings of pleasant mood, positive mood, and expectations regarding aging before and during the pandemic and rating mood and expectations about aging more positively than younger adults, despite being more concerned with the virus and its prevention. In general, older adults tend to have more positive attitudes toward aging than younger adults (Chopik & Giasson, 2017; Kornadt et al., 2017), and these findings suggest that this is also true during a global pandemic even when there is increased societal focus on older adults’ vulnerability. Some recent work suggests that positive attitudes about aging can act as a protective factor against stress (Bellingtier & Neupert, 2018; Levy et al., 2016), which could potentially explain why these older adults are maintaining positive attitudes. In addition, our sample of older adults initially rated their mood as fairly positive and pleasant, but their positivity in mood was not reduced by the pandemic.
Both younger and older adults with higher expectations regarding aging tended to have higher mood, better health, and experience less loneliness, suggesting that maintaining high expectations regarding aging is related to positive outcomes like health and mood, consistent with prior work (e.g., Pietrzak et al., 2014). Although we cannot make claims about the direction of these constructs in the current study, the stereotype embodiment theory (Levy, 2009) posits that older adults may internalize attitudes about aging, leading to influences on their health and everyday behaviors. In addition, positive attitudes have been shown to protect against cognitive decline and stress (Levy et al., 2016, 2018), which may affect health status and mood. However, older adults did report more negative mood and greater arousal during the pandemic than before, despite maintaining positive mood, suggesting that the pandemic may have some influence on older adults’ mood, but that overall older adults are demonstrating resilience.
Additionally, COVID-19 attitudes and behaviors did not seem to be related to mood or expectations in older adults (and were related to loneliness in Study 1 only), but were related to mood in younger adults, such that those who took COVID-19 less seriously reported more unpleasant mood. This finding suggests that older adults’ mood may be less affected by their opinions about the pandemic than younger adults’ and further suggests that older adults are resilient during this global pandemic, despite being more at-risk for serious complications.
Although these findings suggest some older adults are resilient during a global pandemic, it is important to interpret the results in light of sample demographics. In general, our samples were overwhelmingly White and educated. In addition, older adults in Study 1 were mostly high-income, though participants in Study 2 did have greater variation in income. This limitation in Study 1 was inherently present due to the nature of our local older adult subject pool and collecting these follow-up data during the COVID-19 pandemic was not an event we anticipated. This motivated the collection of a more diverse, nationally-representative sample of participants through the CloudResearch platform in Study 2, and this sample is similar in demographics to recent studies on COVID-19 and aging (e.g., Barber & Kim, 2020).
These findings have implications for both future research and practice. We find that some older adults are resilient and maintaining positive attitudes, and future research may seek to determine what factors contribute to this resilience, such as positive attitudes about aging (e.g., Bellingtier & Neupert, 2018; Levy et al., 2016), an increase in focus on close friends and family during challenging times, consistent with socioemotional selectivity theory (e.g., Fung & Carstensen, 2006), and/or demographic factors. In addition, younger adults do not seem to be as resilient (although we do not have data from these measures prior to the onset of the pandemic). Thus, future work can examine why younger adults are less resilient, and clinical practice may focus on improving mood and resiliency in younger adults. Finally, males reported less serious attitudes and prevention intent toward COVID-19 than females, consistent with other recent work (e.g., Capraro & Barcelo, 2020; Galasso et al., 2020), and this was true for both older and younger adults. However, males make up a larger portion of hospitalizations and deaths (Jin et al., 2020), so it is important to target this demographic to prevent the spread of COVID-19 and increase preventive behaviors.
In sum, despite imposed social distancing measures that may have reduced typical levels of social interaction and financial stability, older adults in the current studies maintained their overall mood and expectations regarding aging compared to before the onset of the pandemic, while younger adults reported lower expectations about aging and mood compared to older adults, suggesting some older adults may be steadfast in the face of a global pandemic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institutes of Health (National Institute on Aging), Award Number R01AG044335.