
Abstract
Older adults are at high risk for alcohol and medication interactions (AMI). Pharmacies have the potential to act as ideal locations for AMI education, as pharmacy staff play an important role in the community. This study examined the perspectives of pharmacy staff on AMI prevention programming messaging, potential barriers to and facilitators of older adult participation in such programming, and dissemination methods for AMI prevention information. Flyers, telephone calls, and site visits were used to recruit 31 pharmacy staff members who participated in semistructured interviews. A content analysis of interview transcriptions was conducted to identify major themes, categories, and subcategories. The main categories identified for AMI prevention messaging were Informational, Health Significance, and Recommendations. Within barriers to participation, the main categories identified were Health Illiteracy, Personal Attitudes, and Feasibility. The main categories identified for program facilitators were Understanding, Beneficial Consequences, and Practicality. Multimethod dissemination strategies were commonly suggested. This study found positive pharmacy staff perspectives for the planning and implementation of AMI prevention programming, and future development and feasibility testing of such programming in the pharmacy setting is warranted.
Introduction
From 1983 to 2004, there was a 3,000% increase in fatal medication errors related to alcohol and/or illicit drug use in the United States, surpassing increases in deaths from medication or alcohol and illicit drug use alone (Phillips, Barker, & Eguchi, 2008). At particular risk for these alcohol and medication interactions (AMI) are older adults, as this population has high prevalence of both alcohol and medication use (Aira, Hartikainen, & Sulkava, 2005; Qato et al., 2008). Older adults often use multiple medications simultaneously (Qato et al., 2008), including medications known to have potential interactions with alcohol (Aira et al., 2005), complicating risk for experiencing an AMI. Prescription drug use also increases with age, with 87% of 65- to 79-year-old adults taking prescription drugs in comparison to 91% of adults aged 80 and older (Ihara, Summer, & Shirey, 2002). Alarmingly, almost 80% of older adults who take prescription drugs are exposed to at least one medication that is considered alcohol-interactive (Pringle, Ahern, Heller, Gold, & Brown, 2005). It is estimated that over half of older adults consume alcohol, with about 15% consuming more than seven drinks a week, on average (Zanjani, Downer, Kruger, Willis, & Schaie, 2013). Prevalence of alcohol use is also expected to increase in future aging cohorts (Patterson & Jeste, 1999).
Despite high risk for alcohol and medication interactions among older adults, there is an absence of available AMI management options (Schultz, Arndt, Lutz, Petersen, & Turvey, 2002), beyond drug labeling, to reduce increasing AMI among aging adults. Pharmacists are ideal candidates for providing input for this type of health promotion programing, as they perceive preventive services and health promotion to be important health objectives within their profession (Suh, Greenberg, Schneider, & Colaizzi, 2002). Pharmacists also inherently have medication interaction expertise (Schmiedt & Ellingson, 2010) and an intent and ability to improve medication safety (American Society of Health-System Pharmacists, 2016). Pharmacies have been successfully involved in community substance use–related health promotion programming in the past (Hoch et al., 2012; Kotecki, 2003; Meshack, Moultry, Hu, & McAlister, 2009; Nimpitakpong, Chaiyakunapruk, & Dhippayom, 2010), making them an ideal group for understanding best practices for promoting prescription drug safety, specifically surrounding AMI prevention for older adults in the community.
The United Nations has identified ensuring health and well-being of people of all ages as one of their Sustainable Development Goals, with a focus on substance use (United Nations, 2018). In addition, experts in the fields of public health and aging have called for increased development and evaluation of community-level awareness interventions and behavior change programs for aging adults. Specifically, programs are needed that emphasize recommended drinking limits and age- and disease-related risks of the combined use of alcohol-interactive medication with alcohol (Heuberger, 2009; Kuerbis, Moore, Sacco, & Zanjani, 2017). The need for alcohol screenings when prescribing alcohol-interactive medications has also been recognized (Cain, 1993).
One possible strategy for reducing alcohol-medication interactions is the use of low-intensity, brief interventions and advice that are considered cost-effective, practical techniques to change behavior (Barry & Panel, 1999). Brief interventions are time-limited, nonconfrontational approaches to behavior change that are based on techniques from the behavioral self-control literature as well as the concept of motivational interviewing (Miller & Rollnick, 1991). Randomized clinical trials of brief interventions for alcohol use among older adult populations indicate that older adults can be engaged in brief intervention protocols and find these protocols acceptable (Fink, Elliott, Tsai, & Beck, 2005; Fleming, Manwell, Barry, Adams, & Stauffacher, 1999; Gordon et al., 2003), even over the phone (Oslin et al., 2003). Results of such trials point to a greater reduction in alcohol consumption among drinkers receiving brief interventions as compared with those in the control groups (Lee, Mericle, Ayalon, & Areán, 2009; Zanjani et al., 2008). Despite extensive contextual research in primary care, brief interventions have not been utilized to motivate community members to prevent alcohol-medication interactions. Pharmacist counsel would aid in the creation of tailored messaging for older adults to reduce AMI risk.
Preliminary work has indicated that pharmacists are willing to convey prescription drug safety information to older adults through a variety of formats, including displaying or distributing a flyer and directly administering a brief intervention (Zanjani et al., 2016; Zanjani, Hoogland, & Downer, 2013). This study seeks to further explore pharmacy staff perspectives on AMI prevention programming by collecting information from pharmacy staff on program messaging, barriers to and facilitators of program participation, and intervention dissemination methods.
Method
Recruitment
Participants were recruited from two counties in Kentucky, two counties in Maryland, and two counties in Virginia between 2013 and 2014. Counties were selected based on the Robert Wood Johnson County Health Rankings for rural and national health risk profiles (University of Wisconsin Population Health Institute, 2010), and a complete list of pharmacies in each county was obtained through the state government. Pharmacies and pharmacists with available addresses were mailed a recruitment flyer (n = 96), and those with a provided phone number were also contacted by telephone (n = 62). Site visits to pharmacies were also completed to leave recruitment flyers and discuss the study with pharmacy staff. Individuals expressed interest in participation either in person during a site visit or through a phone call or email to the research team.
Interviews were scheduled at a time and place of participants’ choosing to address potential confidentiality and privacy concerns. All participants were informed that the interview was being recorded prior to the start of the interview so that they may end the call or choose not to respond to questions during the interview, with no effect on study compensation. Recruitment continued until subjective saturation was achieved, which was determined when the research team did not perceive any new content or themes emerging from participant interviews. All interview recordings were transcribed by an independent paid consultant.
Ethics approval was obtained from the supporting institutional review board, and written consent was obtained from all participants prior to the interview.
Interviews
Semistructured interviews were conducted either in person or over the telephone. Group interviews were held in person, and individual interviews were conducted over the phone. On average, the interviews were an hour in duration, and all participants were compensated US $50 for their participation.
Based on prior AMI research (Zanjani, Hoogland, & Downer, 2013), the interviews covered four main topic areas: AMI prevention messaging, barriers, facilitators, and approaches to AMI prevention programming. Interview questions were created in collaboration with pharmacists as well as informed by the scientific literature to address the theoretical principles of the Health Belief Model (Janz & Becker, 1984) and the Information–Motivation–Behavioral Skills Model (Fisher & Fisher, 2002), using the information–education, threat, motivation, skills, and barrier/motivator domains that create and sustain behavior change (Noar, 2004).
The following specific questions were asked during the interviews:
What do older adults need to know about alcohol and medication interactions?
What’s the best way to get AMI messaging information to older adults? What would it look like in your pharmacy?
Why would older adults not want to participate in AMI prevention programming?
What do you think may be some reasons that older adults in the community would want to participate in a program to reduce alcohol and medication interactions?
After each of these questions, participants were asked to identify which of the discussed concepts they found to be most important within each category (i.e., messaging, dissemination, barriers, and facilitators). Suggestions for the dissemination of prevention programming and the similarities and differences between regions were also discussed.
Data Analysis
All interviews were recorded and later transcribed by an independent contractor. The text was then analyzed through line-by-line coding to conduct a content analysis of the interviews to identify themes for messaging, barriers, facilitators, and AMI prevention programming dissemination. Subthemes were also coded for specific content information. Two types of coding were completed. Initially, open coding was used to make sense of the data, and focused coding was later used to develop categories from these initial codes. Frequencies of codes were then calculated, and any exemplifying quotes, outliers, and case evidence were highlighted within the text. Some quotes were edited for readability. Frequencies and percentages across themes were provided for comparison purposes.
Results
The research team conducted a total of 31 interviews with pharmacists and pharmacy technicians. All participants were white, and their ages ranged from 27 to 45 years, with a mean age of 38. The average participant income was US $80,000 a year, 33% had a Pharm.D degree, 76% lived in rural counties, 95% worked full-time, and 81% worked in independent pharmacies.
Table 1 shows the major themes, categories, and subcategories that emerged from interviews with participants. Themes for the four main areas were identified: AMI prevention messaging, barriers to AMI prevention programming, facilitators of AMI prevention programming, and AMI prevention programming dissemination methods. The main categories within AMI prevention programming messages were Informational, Health Significance, and Recommendations. Within barriers to AMI prevention programming, the main categories identified were Health Illiteracy, Personal Attitudes, and Feasibility, and the main categories that emerged for facilitators of AMI prevention programming were Understanding, Beneficial Consequences, and Practicality. Each of these categories was further broken into subcategories.
Frequencies of the Most Important Categories and Subcategories, by Theme.
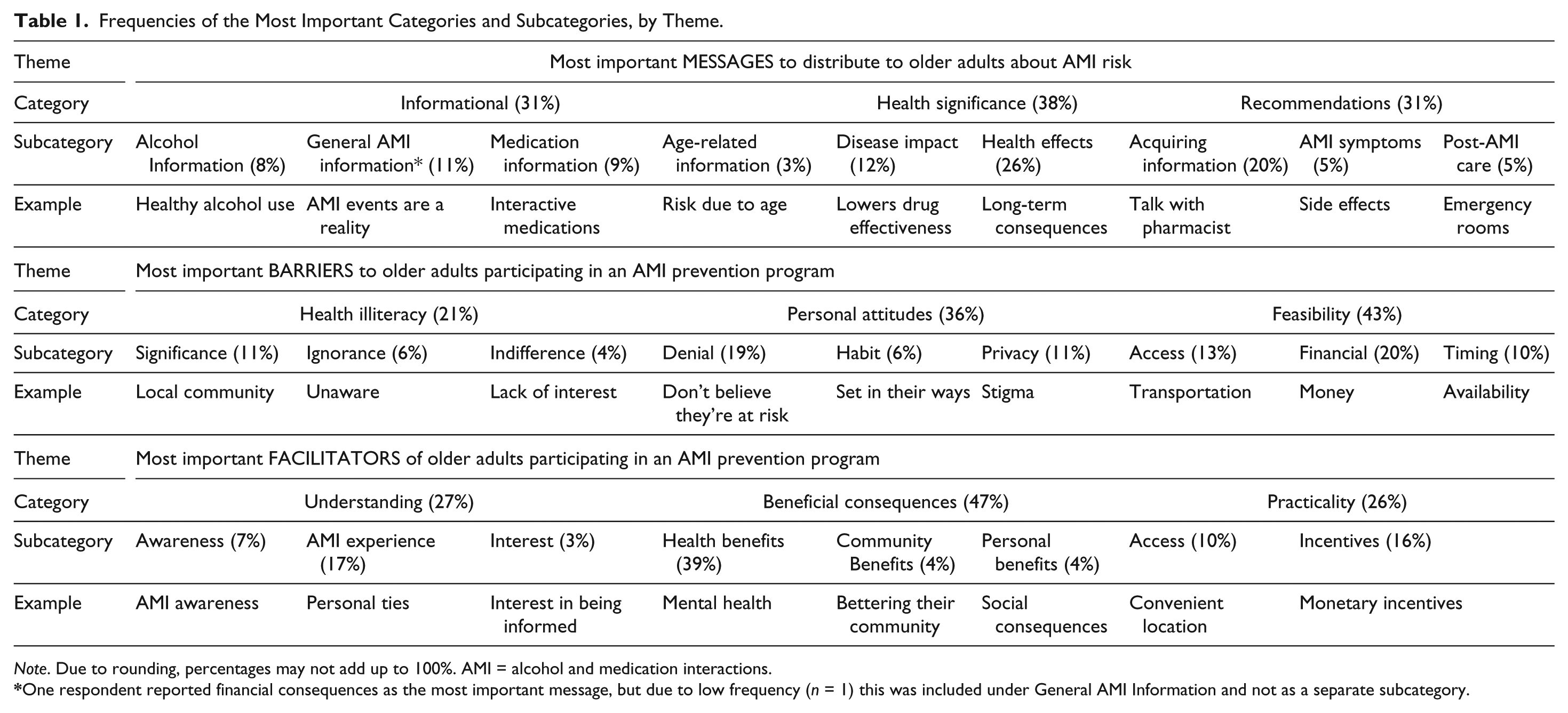
Note. Due to rounding, percentages may not add up to 100%. AMI = alcohol and medication interactions.
One respondent reported financial consequences as the most important message, but due to low frequency (n = 1) this was included under General AMI Information and not as a separate subcategory.
AMI Prevention Messaging
Health significance
Participants reported that the most important AMI messages to distribute to older adults were those that pertained to health significance, with 38% of messages presented categorized as describing health consequences. The category of Health Significance captured messages that emphasized the potential consequences of alcohol and medication interactions and included the subcategories of Disease Impact and Health Effects. Health Effects constituted over one quarter of the messages that respondents reported were most important: I think knowing exactly what the alcohol will do to your medication inside your body is the most important one. Because you need to know if it’s going to be fatal or if it’s going to reduce the effect of the medicine, because you’re on those medicines for a reason. (Pharmacy Technician, Maryland)
Many pharmacy staff members emphasized that older adults weren’t aware of how serious AMI events can actually be. One participant argued that this was particularly true for less severe AMI events, where the individual might experience “a slight headache and a slight . . . stomach upset,” and the older adult doesn’t “take those seriously.”
There was a mixed response from participants as to the importance of short-term or long-term health consequences. Several respondents who identified messages pertaining to the long-term effects of AMI suggested including specific complications that could occur: [There are] severe consequences . . . like losing autonomy, falling, even like the delirium and not being able to function cognitively well. [AMI events] can lead to not taking their medications, not following up with nutrition, leading to undernutrition, malnutrition, and just not being able to manage their disease states well just because you know they’re not cognitively there, not able to think properly, and not able to take their medications on time. (Pharmacist, Virginia)
The Disease Impact subcategory, which emphasized the potential impact that AMI events could have on older adults’ existing diseases or on lowering a drug’s effectiveness, was reported as the most important message by 12% of respondents. Participants agreed with existing literature reporting on the increased risk that older adults face because of their heightened number of average medications: Because older adults have more health problems, they generally have more heart problems, they generally tend to have more lung disorders or depression; alcohol mixed with the depression itself, not even including medications for it but with alcohol being a depressant, that can make their depression worse, and then if they’re on medication for the depression, it could also make that worse. (Pharmacist, Kentucky)
Informational
The Informational and Recommendations messages were subsequently mentioned, with 31% of total messages sorted into each of these classifications. The Informational category includes messages for alcohol and medications separately, as well as defining AMI event/risk, within the subcategories of General AMI Information, Alcohol Information, Medication Information, and Age-Related Information. For General AMI Information, the most common message focused on the prevalence and risk of alcohol medication interactions. As one pharmacy staff member stated, the most important thing is “letting patients know what these [AMI events] are; that this is a pretty common thing and . . . it’s something that they need to be aware of.”
Several respondents also reported healthy alcohol consumption recommendations as one of the most important messages that should be delivered to older adults. One participant stated the importance of informing older adults about a safe amount of alcohol they can consume while taking medications because “it can be hard [and] discouraging when you tell them you can never have alcohol anymore.” Another participant stated that addressing healthy alcohol use
will [help] not discourage [patients] from first of all, reading the pamphlet, and second of all, you know, not taking their medications at all, and third of all, there might be a way that they can drink their alcohol, but in a more safe way.
In addition to the information about interactions between alcohol and medications, respondents mentioned a need for increased knowledge about alcohol and medications individually. Pharmacy staff members stated low level of knowledge among their patients regarding the medications they take as a key factor that needs to be resolved to prevent AMI events: There’s so many people who don’t even know the names of their medications and you see it so often in a retail environment. I think that’s what kind of, you know, pains me the most—that these people just don’t know what they’re taking. They don’t know the difference between their cholesterol medication and their blood pressure medication. (Pharmacy Technician, Virginia)
Similarly, respondents also highlighted the need for more alcohol consumption education, arguing, “Most people don’t think of [alcohol] as being a drug, but it does have dangerous side effects—interactions as you stated with every medication, even if it’s minor versus major.”
Recommendations
The Recommendations category consisted of messages that provided advice to older adults, including the subcategories of Acquiring Information, Post-AMI Care, and AMI Symptoms. Most of the messages for this category fell in the Acquiring Information subcategory and advised older adults to educate themselves about AMI risk by talking to a pharmacist, doctor, or other professionals. Several pharmacy staff members suggested that AMI prevention should start with doctors; specifically, that doctors should be fully aware of individual alcohol consumption habits before prescribing any medications, and that patients should not be afraid to start a discussion with their physician about their AMI risk: Maybe their doctor should be the one telling, asking if they’re using alcohol or not or just warning them when they’re giving them the prescriptions—“Hey, if you’re taking, drinking this, you may want to, you know, wait a little while before drinking,” or, you know, “Don’t drink if you’re taking this medicine until you finish taking it.” (Pharmacy Technician, Maryland)
Respondents also reported that it was not important who older adults talked to about their AMI risk, as long as they were talking to a health professional. One such individual commented that older adults should
[start] a conversation with anybody. Any . . . healthcare professional, physician, pharmacist, anybody that has knowledge in this area that you know they can definitely go out and talk to them if they have any questions about this.
Other participants reported it would be better to encourage older adults to talk to pharmacists in particular, as “there are some [patients] that just won’t ask their doctor [medical questions] because I’ve heard a couple of them come into my store and they refuse to ask their doctor; they would rather ask the pharmacist.” AMI Symptoms and Post-AMI Care accounted for very few of the messages that pharmacy staff deemed as the most important, with only 5% of total messages represented in each of these two subcategories.
Barriers to Participation
The most frequently reported category for barriers to participation in AMI prevention programming was Feasibility, with 43% of the most important barriers falling into this classification. Feasibility included functional hurdles to participation, with Access, Financial, and Timing subcategories. Thirty-six percent of reported barriers were about Personal Attitudes, a category that contained the subcategories of Denial, Habit, and Privacy. Finally, 21% of barriers mentioned as the most likely to prevent participation were related to Health Illiteracy. This classification included the subcategories of Significance, Ignorance, and Indifference.
Feasibility
Under the Feasibility category, messages falling into the Access and Financial subcategories were reported most frequently. One participant straightforwardly stated that money was “always a barrier,” while another agreed, stating that “if they had to pay for [AMI counseling], they would never come” to a program. Respondents reported that cost might be of particular importance to older adults, mentioning that they are already “paying huge amounts of money for their care and their prescriptions” and that “most [older adults] are on fixed incomes or just get aid to help them and don’t have any spare money.”
Participants also indicated that access could be a significant barrier to participating in an AMI prevention program, specifically for rural older adults: [Patient] access, the ability of the patients to actually either get out of their home to get to the centers or to even . . . get this type of information, this type of counseling done depends on . . . how, if they can drive, if they have a car available, if they are physically able to get there via bus or anything else. You know, sometimes just because of the amount of pain, disabilities that they have, they’re not going to be able to come to, to go out and get this type of information . . . that’s definitely something, like some sort of obstacle here to overcome. (Pharmacist, Virginia)
Participants also stated timing, or the availability of older adults to participate in AMI prevention programming, as a potential barrier. When asked if time could be a potential barrier, one participant stated: Time is a big deal . . . [and] it would depend on what kind of program. So if it’s just a brochure, people will have no issue grabbing it. And if it’s just like a quick consult with the pharmacist, no issue usually talking to me, even if they’re on, they seem like they’re on the run or you know whatever. I think the biggest issue would be a long sit down kind of program where it’s like more than like 20 or 30 minutes. That’s when you’re going to have people that are saying, “I don’t think I’m going to spend my time on this.” (Pharmacist, Maryland)
However, other respondents reported that time would not be an issue, for older adults in particular, arguing that the majority of this population is retired.
Health illiteracy
Under the Health Illiteracy category, a few participants (11%) indicated that a significant barrier to engaging in AMI prevention is an absence of AMI messaging and awareness on a national scale and in their own communities: [AMI prevention] is not broadcasted enough and it’s not taken seriously enough. Like people started [MADD] because people were dying from drunk driving and young kids were dying and everything, and texting and driving has become a new one as well. So the fact that it’s not broadcasted on a national scale would affect people . . . They’re like, “Oh well, well I shouldn’t take this seriously when no one else is taking it seriously.” (Pharmacy Technician, Maryland)
In addition to Significance, the other subcategories of Health Illiteracy were Ignorance and Indifference, accounting for 6% and 4% of the most significant barriers, respectively. Pharmacy staff members reported that being either unaware of the AMI problem or being uninterested in AMI prevention could be barriers to participation for older adults. When one respondent was asked whether lack of interest could be a barrier, they responded, “Yeah, I could see that. That would definitely be a good one. They just don’t care, you know, if there is an interaction or not . . . They’re going to keep doing what they’re doing.” Another participant, referencing the age of the population, stated that the lack of interest would be “a huge barrier” and that “most people that are drinking at that age are not going to care. I think by the time . . . you get to the older adult stage, you know, I think the alcohol use is pretty well set.” However, another participant reported that age would be beneficial: The majority of the people that I’ve met are very interested in their well-being, especially the older ones. . . You can tell that, you know, they aren’t just sitting at home; they know the risks, they know they have been educated on what to do and you know they’re interested in coming and getting it done. . . So in my opinion, I think the majority of them are very interested in taking care of themselves. (Pharmacist, Virginia)
Many participants reported that older adults just aren’t aware of their AMI risk, which may be a potential barrier for participation. One respondent called the lack of awareness a “huge concern” and indicated that older adults are “left to ask questions [about AMI] instead of being told.” Other participants said that for most older adults it “doesn’t even cross their mind” that there might be a problem with drinking alcohol while on medication, and that “if nobody’s telling them, they’re going to keep on doing it.”
Personal attitudes
Thirty-six percent of the most significant barriers identified by pharmacy staff fell into the Personal Attitudes classification. Nineteen percent of the most important barriers pertained to denial, as participants reported that certain older adults wouldn’t perceive themselves at risk for an AMI. While the majority of pharmacy staff members felt that, in general, older adults were aware that AMI risk could happen, they also reported that the population didn’t personally perceive themselves at risk, arguing that “Like everybody else, they always think it’s not going to happen to them so they would just choose to ignore it.”
I mean I’d say [older adults] are aware of the problem, but I would say that they would not be aware they’re at risk themselves . . . unless we specifically tell them they are at risk, you know, based on something that they’re already taking or that they’re going to be taking, then they’re just going to move on the assumption that, “They would’ve told me if it was important.” (Pharmacist, Virginia) Yeah, because a lot of people [have been] drinking alcohol like all the days of their life, and . . . then you come out and tell them that at the age of 75 they cannot drink wine, you know a glass of wine and, or they cannot have this and that and to them, they feel like okay, what is the big deal anyway? You know, I’ve been drinking for years, so what is the big deal? (Pharmacist, Virginia)
Facilitators of Participation
When participants were asked about potential facilitators of participation in AMI prevention programming, 47% of facilitators were categorized as Beneficial Consequences, which included the subcategories of Community Benefits, Health Benefits, and Personal Benefits. Twenty-seven percent of facilitators were categorized as Understanding, and this category included messages within the subcategories of Awareness, AMI Experience, and Interest. Finally, 26% of facilitators were under the category of Practicality, which included the subcategories of Access and Incentives.
Beneficial consequences
The most frequently indicated motivating factor was that participating in an AMI program would support an overall healthy lifestyle. Pharmacy staff members reported that focusing on the potential for better health and a longer life was the best and most effective way to motivate older adults to participate in an AMI prevention program: Of course just letting them know that . . . if they don’t, if they’re not aware [of AMI risk], you know, they don’t take this kind of seriously, that it can lead to, you know mortality, death, things like that that maybe at that time they’re not ready to go or that their family members definitely don’t want them to go, especially children, grandchildren. Just keeping those people in mind. (Pharmacist, Virginia)
Understanding
The second most frequently reported motivator was having AMI Experience (17%), which could include older adults seeing it in their community, seeing it on a national scale, having personal ties, or believing that they are at risk for an AMI. Many respondents reported that knowing somebody who has experienced problems with alcohol, medication, or the interactions between the two would drastically increase that person’s interest in participating in an AMI prevention program: The biggest reason why somebody would want to participate is definitely if they’ve had a previous issue with medication, which is a lot of people. Like if they had a previous interaction or if they had a family member that had like a really severe interaction, I think that would, you know, they would want to know as much as possible so that would motivate them. (Pharmacist, Maryland)
Participants noted that knowing that AMI events are problematic and may affect family, friends, and neighbors would facilitate participation because “it makes it more personal to have it in your own community.”
Practicality
Practicality was the least frequently reported facilitator of participation (26%). Participants reported that promoting the beneficial consequences and dealing with understanding would be more beneficial to recruitment than tackling access, convenience, and incentive issues. While most participants responded positively to the idea of providing incentives and holding the program in a convenient location and at a convenient time, they reported that these were not the most important motivators: Compensation definitely is not one of those things that I would put as high priority on their list. Yeah, just because I think at that age, then it seems as though they’re not, they don’t like purchasing the things that aren’t completely necessary and everything else, they don’t seem to be like just you know being reckless about. Oh they’ll come in and purchase the things that they need, medications, things like that, but you know if like if we were for instance to say, “Hey, we’ll compensate you if you come and then do like this study or if you want counseling, you know we’ll give you some sort of reward or benefit, you know, like monetarily,” they’re not going to be down for that. (Pharmacist, Virginia)
Dissemination of Information
The most frequently identified dissemination method was pamphlets, with 83% of participants mentioning that pamphlets could be used as a tool that the doctor or pharmacist could pick up, discuss with older adults, and then give it to them as a takeaway for reinforcement. The majority of participants who supported the use of pamphlets advocated for making them available at the pharmacy itself, while others suggested distributing pamphlets to doctors’ offices, waiting rooms, and health departments: Like on, you know, the pharmacy counters, if there’s like little pamphlets, you know that’s nice because not every single patient gets a chance to speak with a pharmacist . . . There’s so many patients and like retail’s really crazy sometimes so you’re not going to have the opportunity to talk to, you know, patients so I think . . . pamphlets on the pharmacy counter is a good idea. (Pharmacist, Maryland)
However, some interviewees felt that pamphlets weren’t the best way to go, stating that, “I feel like a lot of the information on pamphlets or sheets are not as effective, because I don’t feel like a lot of people actually take the time to read those or go over it.” Another participant echoed this sentiment, noting that “We have like all kinds of pamphlets that sit around [the pharmacy] and nobody ever takes them.”
The next most popular method of dissemination was pharmacist consultation, where the pharmacist delivers the information about AMI events and risk. A few participants did mention that although being able to counsel everyone would be ideal, this tactic is not very practical because the pharmacy technicians are not qualified to complete alcohol and drug counseling, and “there’s obviously not enough time in a day for a pharmacist to do that.” However, for older adults who regularly consume alcohol and are taking potentially harmful medications, the counseling might be more feasible. Many respondents suggested using a combination of methods, particularly the pharmacist consultation with another tool, such as pamphlets or a helpline: I think what works the best would be a face-to-face communication with the patient [and pharmacist], giving specific examples, providing some sort of pamphlet or brochure that highlights the risks and the benefits and just helping them to apply that to their lives and helping them to see the difference that it would make [in] their life. (Pharmacist, Kentucky)
Television and radio were also frequently mentioned methods: Pamphlets are okay, but anything with a lot of text in it like newspaper clippings or any sort of, anything that’s you know kind of wordy, patients, especially like the older they are, if they have difficulty with vision and things like that, then that’s going to be something that they’re not going to be fully into. I mean if it’s, if the main points are highlighted for a pamphlet, then I think they would be okay with that, but having it conveyed through either the television, some sort of TV programming [would be best]. (Pharmacist, Virginia)
Comparisons by Region
Overall, Kentucky (KY) and Maryland/Virginia (MD/VA) pharmacy staff similarly placed importance on AMI programming. Participants from both regions emphasized the significance of AMI knowledge, including the disease impact and health effects of AMI events as the most important. The most important category for barriers, Practicality, was the same for both Kentucky and Maryland/Virginia participants. Kentucky participants prioritized Personal Attitudes as the second most important category of barriers to participation, while Maryland/Virginia placed Personal Attitudes at a very low priority. Participants alike reported that the most important motivators to encourage older adults to participate in prevention programming would be highlighting the Beneficial Consequences. In general, participants from both regions had similar ideas about the most effective dissemination methods for getting AMI information to older adults, with the greatest percentage of participants (90% MD/VA, 79% KY) identifying pamphlets as a means of distributing information, followed closely in number by pharmacist consultations (80% MD/VA, 71% KY) and television (80% MD/VA, 64% KY). While 64% of the KY participants believed using educational programs or classes would be useful, only 20% of MD/VA participants agreed. Going through the family and caregivers as a route of dissemination was reported by 43% of KY participants but by only 10% of MD/VA participants. Participants in both regions similarly agreed on the use of doctor consultation as a dissemination method (40% MD/VA, 43% KY). Very few participants in either region recommended using support groups, grocery stores, phone hotlines, or the Internet.
Discussion
This study explored pharmacy staff perspectives on the implementation and importance of programming for older adults on the prevention of alcohol and medication interactions. Several main themes emerged from interviews with pharmacy staff about AMI prevention messaging, barriers, and facilitators for older adult participation in prevention programming, as well as the best methods for disseminating information about AMI risk. Overall, participants felt that program messaging should focus on long-term health consequences of AMI events as well as advising older adults to discuss AMI risk with their doctors and pharmacists. In terms of implementation of prevention programming for older adults, participants placed emphasis on several potential barriers. Pharmacy staff members were concerned that older adults wouldn’t participate in programming for denial and financial reasons, specifically if the program cost money or they had to pay for transportation to the program location. Also, more widespread local and national dissemination information about AMI in the population could address individual denial of AMI as a potential health problem. Pharmacy staff mentioned that highlighting the potential health benefits of AMI prevention programming would facilitate participation by older adults. Other frequently mentioned suggestions were to target older adults who had personal experience with AMI events, as those who have witnessed the potential harms are more likely to see the value in participating in AMI prevention programming. Monetary incentives for participation were also mentioned by several participants, which is a common strategy used to increase participation in health promotion programs, but it raises issues of sustainability. Participants also encouraged the use of pamphlets, pharmacy consultation, and television or radio as methods to disseminate AMI prevention information to older adults.
In addition to considering the facilitators of and barriers to participation by older adults, program planners should also take geographic region into consideration when planning AMI prevention programming. Results of this study showed that pharmacy staff from the Maryland, Virginia, and Kentucky areas held similar beliefs about the importance of messages surrounding the significance of AMI knowledge and the need for programs to address the practical barriers and potential benefits to participation. However, participants from the MD/VA area placed more emphasis on lack of awareness and interest in AMI prevention as a barrier to participation, while participants from Kentucky were more concerned that older adults would not participate in AMI prevention programs due to personal attitudes, such as privacy. In addition, participants from Kentucky were more likely to note that incentives would motivate participation, while participants from the MD/VA region felt that older adults would be likely to participate if they had experience with or wanted to learn more about AMI risk.
The interview questions were created based on the principles of the Health Belief Model (Janz & Becker, 1984) and the Information–Motivation–Behavioral Skills Model (Fisher & Fisher, 2002). Findings on the importance of intervention messaging containing information about how alcohol can be dangerous at any level and how AMI events can result in negative mental and physical health consequences were in line with the perceived severity construct of the Health Belief Model and the information and motivation constructs of the Information–Motivation–Behavioral Skills Model. Both the Health Belief Model and Information–Motivation–Behavioral Skills Model highlight the importance of potential barriers to health behavior change, and several barriers were discussed by participants in the current study. One potential barrier to participation was denial that AMI was an issue, indicating that perceived susceptibility among this population, a major construct of the Health belief model, may be low and should be addressed during program development. The information–motivation–behavioral skills model posits that the combination of information, motivation, and skills increase the likelihood of behavior change, and pharmacists in this study greatly emphasized the need for the dissemination of information on AMI risk through multiple modalities at the community and national levels.
The findings of this study should be considered in the context of its limitations. There was a relatively small sample size from each county, making comparisons by region difficult. Pharmacy staff members who agreed to participate in the study may be more invested in community-based health promotion and may, therefore, have a more positive view of AMI programming than pharmacy staff members who did not agree to participate. In addition, interviews were held in both individual and group sessions, so participant responses may have differed based on the type of interview.
The pharmacists and pharmacy technicians in this study appeared to understand the important role they play in health promotion for their patients, which is consistent with prior research in this population (Suh et al., 2002). Prior research has also shown a willingness among pharmacists to communicate with their patients regarding drug safety through various formats, including flyers or brief interventions (Zanjani et al., 2016; Zanjani, Hoogland, & Downer, 2013). The same willingness was seen among participants in the current study, and future prevention work should capitalize on this population’s openness to engaging in programs that aim to reduce alcohol and medication interactions among older adults.
This study is an important foundational step in the development of AMI prevention programming based out of community pharmacies. Positive perspectives from pharmacy staff obtained during these interviews informs the planning and implementation of AMI prevention programming, and future development and feasibility testing of such programming in the pharmacy setting is warranted.
Footnotes
Authors’ Note
This research was approved by the Institutional Review Board at the University of Maryland College Park (No. 499568-21).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health [1K01DA031764 to F.Z.].