
Abstract
Keywords
Introduction
Strong evidence shows that physical activity has beneficial effects on well-being, health, and longevity in older ages. When studying different intense levels of exercise, moderate exercise (moderate physical activity, MPA) has been repeatedly suggested as most preferable (Bellavia, Bottai, Wolk, & Orsini, 2013; Rennemark, Lindwall, Halling, & Berglund, 2009; Stessman, Hammerman-Rozenberg, Cohen, Ein-Mor, & Jacobs, 2009; Lindwall, Rennemark, & Berggren, 2008). There are, however, several variables that may affect these results and thus have to be controlled for in future research.
In this study, we focus on the relationship between MPA and longevity, taking into account age, gender, smoking habits, cohabitation status, body mass index (BMI), leg strength and balance, education level, and cognitive function.
It has long been known that smoking increases the risk of premature death considerably (Doll & Hill, 1954, 1956; Doll, Peto, Boreham, & Sutherland, 2004; Heir, Erikssen, & Sandvik, 2013) and also that cohabitation may decrease that risk (Siegler, Brummett, Martin, & Helms, 2013). Loneliness in general is known to increase the risk of death, for reasons of both physical and social behavior (Luo & Waite, 2014). The role of weight seems more complicated. Underweight increases the risk of death for the elderly (Lin et al., 2011), while moderate over-weight (BMI 25-30) seems to be beneficial in some studies and increase the risk of death in other studies (Heir et al., 2013). Obesity (BMI >35), however, increases that death risk (Coombs, Stamatakis, & Lee, 2015; Köster-Rasmussen et al, 2016). Weak leg strength and balance, operationalized as the ability to get up from a chair by using leg strength alone (the Chair Stand Test) has been shown to predict mortality risk, nursing home admission and disability in the Instrumental Activities of Daily Living (IADL) scale (Guralnik et al., 1994; Seeman et al., 1994; Zhang et al., 2013). In addition, it has been ascertained (Luo, Zhang, & Gu, 2015; Montez, Hummer, & Hayward, 2012) that higher education decreases the risk of death. A relationship between cognitive function and longevity has also been found (Robitaille et al., 2014).
The survival effect of physical exercise has received support by a large study of more than 40,000 athletes, which shows that the Standardized Mortality Ratio (SMR) for athletes compared to the standard population was 33% lower (Sanchis-Gomar et al., 2014). There are also other studies showing that physical exercise decreases mortality. In one study (Moore et al., 2012) it was found that jogging or brisk walking more than 7.5 hr every week was associated with a higher life expectancy. In another study (Buchman, Yu, Boyle, Shah, & Bennet, 2012), non-exercise physical activity was also included supposedly minimizing the risk of recall bias in the self-reported exercise. For a person engaged in more frequent physical activity, the mortality risk in that study was about 25% lower than for those less frequently active.
The longevity effect of physical activity seems, however, in a number of studies, in which both light and intense physical activity levels have been used, to be U-shaped according to frequency and intensity. (Merghani, Malhotra, & Sharma, 2016; Schnohr, O’Keefe, Marrott, Lange, & Jensen, 2015). Some researchers have tried to establish a dose–response relationship between the amount of exercise and decrease of mortality (Schnohr et al., 2015; Zhao et al., 2015). Public health recommendations of physical activity have been made by, for example, the World Health Organization and the American College of Sports Medicine (Nelson et al., 2007), in which 30 min regular moderate physical activity almost every day is generally recommended. The Swedish National Board of Health and Welfare recommended being active on a moderate level every day in combination with more intense exercise 2 to 3 times per week (Socialstyrelsen, 1971). Assuming the existence of a U-shaped relationship, moderate activity levels seem most preferable. This assumption has also been empirically supported with regard to the relationship between the amount of exercise and cardiac morbidity (Merghani et al., 2016), quality of life and cognitive functioning (Lindwall, Rennemark, & Berggren, 2008; Rennemark et al., 2009; Robitaille et al., 2014). In addition, people with more frequent MPA were engaged in more cognitive activities (Zhao et al., 2015). It has also been found that only one to two hr of jogging weekly decreased the risk by 71% (Eijsvogels, Molossi, Lee, Emery, & Thompson, 2016).
Assuming the existence of a U-shaped relationship, it has been suggested that while the largest decrease in the risk of death takes place when going from zero to any moderate physical activity, more frequent and intense physical activity is beneficial only for a very small part of the population, such as trained athletes (Eijsvogels et al., 2016).
These studies indicate that a physical activity level larger than some minimum amount of intensity and frequency, can slow down the aging process in both psychological and physiological respects (Gremeaux et al., 2012) while more intense exercise does not seem to improve health and survivability (Bellavia et al., 2013; Merghani et al., 2016).
In sum, with regard to the relationships between physical activity and longevity, most studies support the assumption that a moderate activity level is most beneficial. Therefore, the aim of this study is to find the answer to the following questions:
How is the frequency of MPA distributed among older adults aged 60 to 96 by gender and age?
How is the frequency of MPA associated to the risk of death adjusted for gender and age?
What is the impact of the control variables age, BMI, smoking, leg strength, Mini Mental State Examination (MMSE), education, and living alone or not on these relationships?
Method
Participants
This study included men and women aged 60 to 96. The characteristics of the general population of elderly people in Sweden are closely reflected in the sample which may be seen as representative for older adults in Sweden. Data were collected from physical examinations, patient records, and questionnaires. The purpose of the data collection design was to receive a randomly selected sample, representing the old population in a broad variation of ages. In the present study, the sample of women and men were divided into 10 age cohorts (aged 60, 66, 72, 78, 81, 84, 87, 90, 93, and 96 years). The individuals are thereafter followed regularly—the younger ones every sixth year and the older ones every third year. Every sixth year a new cohort of 60-year-olds is added to the study population. Of the total sample of individuals drawn from the municipality registers (N = 12.995), 8,462 participated in the study (65.2%; Table 1)
Number of Participants by Age and Gender, Participation Rate and Number of Total Population From Which the Sample Was Drawn.

Instruments and Procedures: Data Collection
The examinations were performed at geriatric research centers in four Swedish regions (Malmö, Karlskrona, Kungsholmen [Stockholm], and Nordanstig).
The baseline data collection was concluded in 2004. The outcome variable, survival, was collected from the Swedish National Death register of 2015. All additional variables were collected from the baseline database. In that data collection, participants were examined medically, answered interview questions and survey questions including the variables used in the present study. The examinations were carried out by trained research staff. The participants were invited to the clinic in which the examinations took place. Those who agreed to participate but were unable to come to the center were investigated in their homes. Written informed consent was obtained from the participants before the examinations. The information included full anonymization and nonidentifiability.
The independent variable, MPA, was based on a survey question worded: “How often have you been engaged in light physical activity (such as going for walks, taking short bicycle tours, doing light gymnastics, playing golf or engaging in similar activities) during the last 12 months?” The answer alternatives were 1 = Never, 2 = Once a month, 3 = Two to three times a month, 4 = More than once a week but not every day, 5 = Every day.
Age was measured by years. When measuring BMI, weight (in kilograms) was measured by a precision balance scale with light clothes on and without shoes. The balance was manufactured by the Japanese Tanita Corporation ± 50 g precision. Height was measured with the participant standing, and re-readings were made in centimeter within one decimal. Low BMI was defined as 18.5 or less while high BMI was defined as 35 kg/m2 or more. Smoking habits was measured by a survey question involving whether the participants smoked regularly or not. Leg strength and balance were measured by the Chair Stand Test whereby participants were asked to keep their arms crossed over their chests and to stand up from a sitting position and then sit down five times in succession, as quickly as possible (Guralnik et al., 1994; Seeman et al., 1994). High education was defined as having completed secondary school and living alone was defined as living in a single household. MMSE was used as a continuous variable.
Statistical Analyses
The statistical analyses consisted of descriptive measures and Cox Proportional Hazard models. In the latter analyses, the Cox survival model (Cox, 1972) was used as implemented in SPSS version 23. The variables were entered in blocks, beginning with MPA, which was dichotomized into either once every month or less, or 2 to 3 times every month or more. In the next step, physically affecting variables such as age, BMI, and smoking habits were entered, followed by functional capacity variables such as cognitive function and leg strength and balance. In the last step, social conditions such as education level and living alone or not were entered. In addition, Cox regression analyses, the MPA variable was dichotomized using one for “once every month” or less and two for “2-3 times every month” or more as cut points.
Results
A majority of the participants were performing MPA 2 to 3 times every month or more (82.1%). In the younger group (aged 60-79), this activity level was reached by 94.2% and in the older group (aged 80-96) by 82.1% (χ2 417.49***, df = 1). In the male group there were 83.2% who performed MPA 2 to 3 times every month or more while for the women, the corresponding figure was 81.4% (χ2 3.99*, df = 1). Doing MPA more than once a week including every day was performed by 71.4% of the participants. In the younger group, the corresponding figure was 78.8%, while in the older group it was 59.6% (χ2 179.73***, df = 1). In the female group, there were 62.4% performing MPA more than once a week including every day and the corresponding figure for the male group was 70.4% (χ2 3.26, df = 1). The gender difference was not statistically significant.
The distribution of MPA frequency in the total group and in each subgroups is shown in Tables 1 and 2. In all groups, differences in MPA levels at baseline between survivors and non-survivors at the follow-up are statistically significant as measured by χ2. Generally, those still alive at the 11-year follow-up measure were more often physically active at the baseline measure (Tables 2 and 3).
Distribution of Moderate Physical Activity Habits Among Living and Not Living Participants During a 10-Year Time Span in the Total Group and by Age Group.

p < .05. **p < .01. ***p < .001.
Distribution of Moderate Physical Activity Habits Among Living and Not Living Participants During a 10-Year Time Span by Gender.
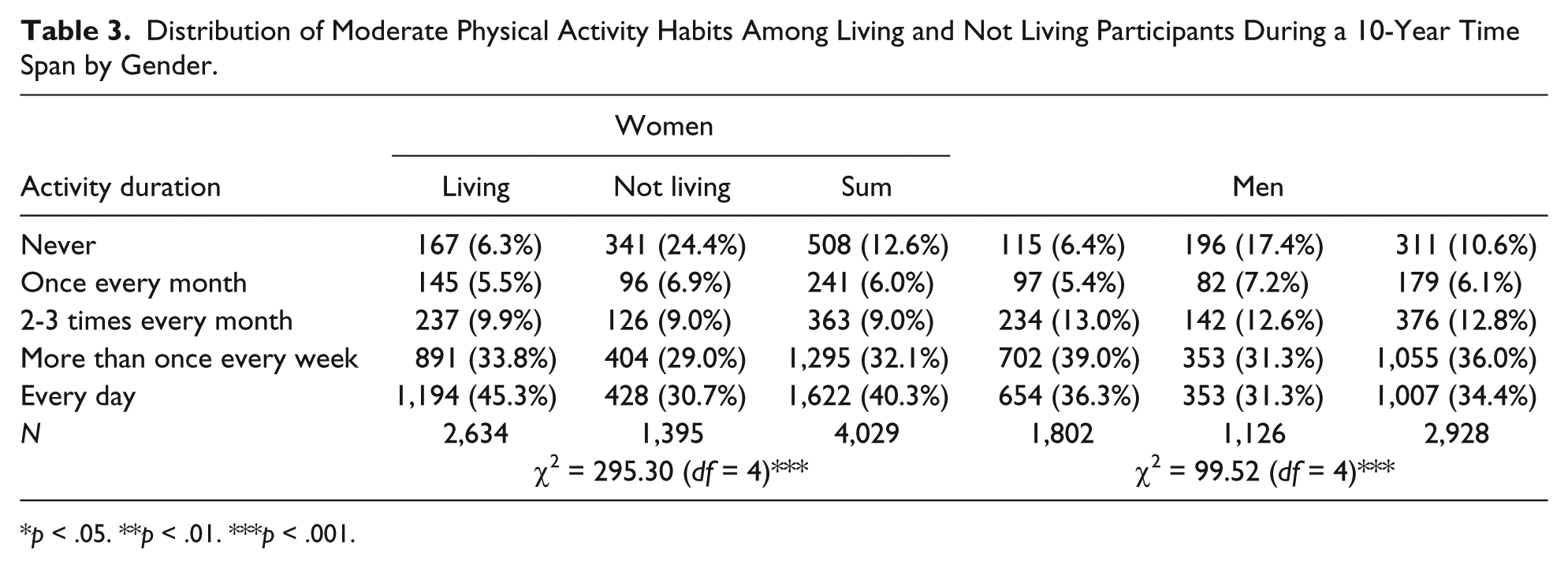
p < .05. **p < .01. ***p < .001.
To investigate whether other factors influenced the relationships between MPA habits and risk of death, Cox regression analyses were performed with stepwise inclusion of covariates. Bivariate correlations (Spearmans rho) between all included variables showed that high age (r = −12**), a high BMI (>35; r = −.07**) and weak leg strength (r = −.20**) were significantly correlated with low MPA levels while high education (r = .07**) and not living alone (r = .05**) were correlated with high levels of MPA.
The Cox regression analyses were performed in four steps for the total group. In these analyses, the hazard ratio (RR) of dying was 51% higher (RR = .49**) for those who were active less than 2 to 3 times every month when no covariates were controlled for. After entering three biologically related variables (age, BMI, and smoking), the risk became 34% higher (RR = .66**). In the next step, two functional status variables (MMSE and Chair Stand) were entered, changing the increased risk to 29% (RR = .71**). In the final step two social variables (low education and living alone) were entered, giving an increased risk of dying of 28% (RR = .72; Table 4). In the final model, MPA was the strongest predictor of longevity together with education level which showed the same RR level (RR = .72).
Cox Regression: RR of Dying in the Total Group (N = 5,923).
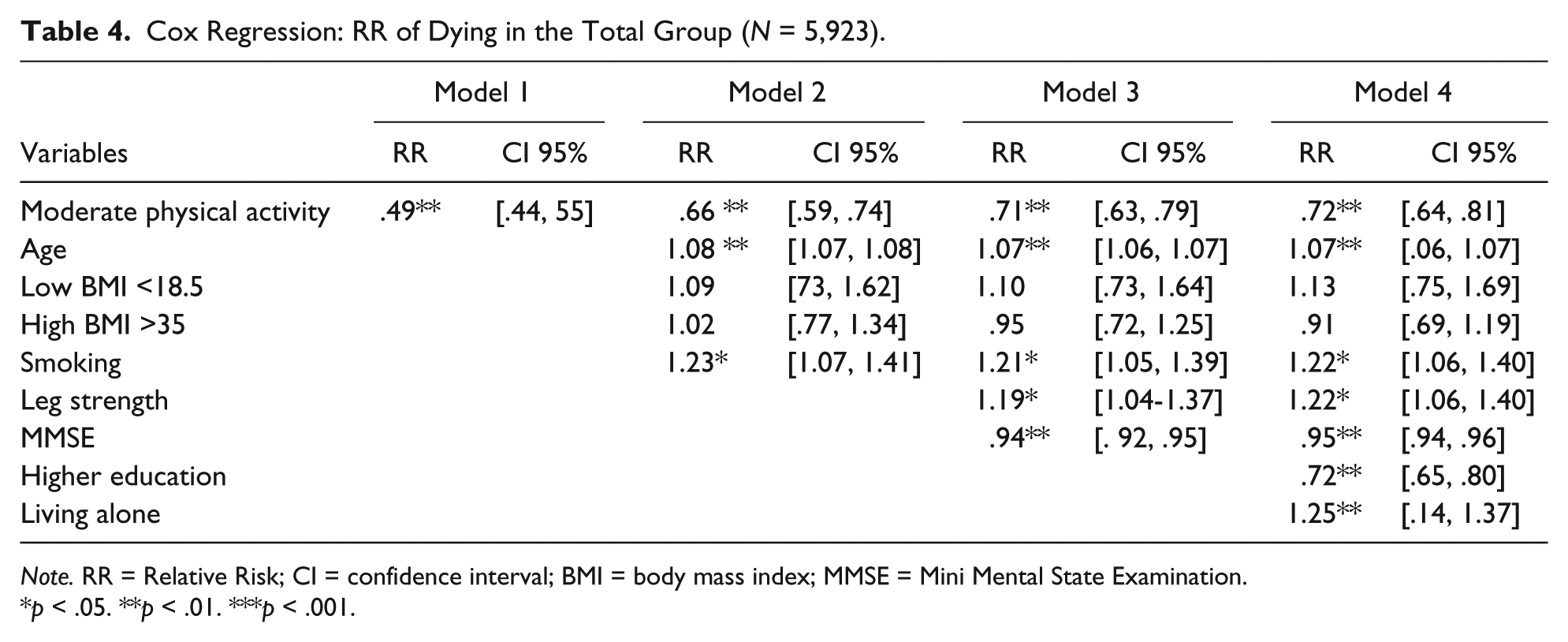
Note. RR = Relative Risk; CI = confidence interval; BMI = body mass index; MMSE = Mini Mental State Examination.
p < .05. **p < .01. ***p < .001.
In the next step, the full model was tested in four subgroups: women only, men only, participants aged 60 to 79 years and participants aged 80 to 96 years.
In the female group, a low MPA increased the risk of dying (Table 4). The RR value was .66, indicating an increased risk of 34%. In this group, MPA was the strongest predictor of longevity followed by low education, which increased the risk by 32% (RR = .68). In the male group, another pattern emerged showing a low MPA giving a 23% increased risk (RR = .77). In this group, the strongest predictor of longevity was leg strength (Chair Stand), which decreased the risk of dying by 51% (RR = 1.51), followed by smoking with an increased risk of 41% and low education with a 26% higher risk (RR = .74) In the older group (aged 80-96), the risk of dying among those with a low MPA was 29% (RR = 71). In this group, a low BMI (<18.5) increased the risk of dying by 64% (RR = 1.64), while high BMI seemed to decrease the risk by 51% (RR = .49). Other variables included in the model were only marginally related to survival (Table 5). In the younger group (aged 60-79) the risk of dying in the high MPA group was 22% lower (RR = .78), while smoking increased the risk by 24% (RR = 1.24), weak leg strength by 56% and living alone by 43%. (RR = 1.43). In addition, a higher education level decreased the risk by 35% (RR = .65). Two additional Cox regression analyses using the same control variables were performed with more frequent physical activity as independent variables. In the first model, RR for those who were active more than once a week compared to those less active was calculated, giving a hazard ratio decreased by 29%, RR = .71***, 95% confidence interval (CI) = [.645, .783]. In the second model, RR for those active every day were compared to those less active, giving a 28% decreased Hazard Ratio compared to those less active, (RR = .72***, 95% CI = [.654, .798]. Thus, higher frequencies of MPA than 2 to 3 times per months did not further decrease the risk of dying.
Cox regression: RR of Dying. Model 4 in Subsamples.

Note. RR = Relative Risk; CI = confidence interval; BMI = body mass index; MMSE = Mini Mental State Examination.*p < .05. **p < .01. ***p < .001.
Discussion
The results show that 82.1% of the total sample performed MPA 2 to 3 times every month or more. The younger participants were more active and men were slightly more active than women.
In addition, the results showed that those who performed MPA 2 to 3 times every month or more were, in an 11-year perspective, more often still alive. This was shown for the total sample but also for both men and women as well as for both the younger and the older groups when RR was calculated for these groups separately. These results support previous findings showing that MPA benefits longevity (Bellavia et al., 2013; Moore et al., 2012; Stessman et al., 2009).
In comparison with other studies, the low frequency of MPA needed for an effect on longevity was remarkable (Buchman, Yu, Boyle, Shah, & Bennett, 2012; Montez et al., 2012), although low levels have been suggested previously (Moore et al., 2012). The results do not contradict the general recommendations of daily moderate physical activity (Schnohr et al., 2015; WHA, 2004; Zhao et al, 2015), but the present results also indicate that health advantages, at least in terms of longevity, can be achieved by an even lower activity frequency. The previously made suggestion (Schnohr et al., 2015) that the strongest difference in health outcomes can be observed between those not active at all and those performing any moderate activity (Schnohr et al., 2015) is confirmed by the result of this study.
When control variables were adjusted for in Cox regression analyses, the relationships between MPA and longevity showed to be robust. The decreased relative risk of dying for those performing MPA 2 to 3 times every month or more were still significant albeit on lower levels. In the total group, the relative risk decreased from 51% unadjusted to 28% after adjustment for all control variables. In Model 2, adjustment for the biologically related variables of age, BMI, and smoking habits decreased the effect by 17% (from 51% to 34%). The inclusion of the two functional variables (MMSE and Chair Stand) decreased the effect by an additional 5% (from 34% to 29%) and in the final model, which also included two social variables, an additional decrease of 1% (from 29% to 28%) was shown. This may be explained by the previously known relationships between longevity and these variables, which show that advanced age is a main predictor of dying (Bellavia et al., 2013) as well as smoking (Doll and Hill, 1956; Doll and Hill, 1954; Doll et al., 2004) and weight loss (Köster-Rasmussen et al., 2016), while the Chair Stand ability (Guralnik et al., 1994), cognitive function (Ferrucci et al., 2013; Lindwall et al., 2008), education (Seeman et al., 1994), and cohabitation benefit survival (Siegler et al., 2013).
The decreased relative risk in the adjusted model was slightly stronger for women than men and for the older group compared to the younger. The gender difference may be partly explained by the slightly lower activity level of the women. In addition, only three control variables increased the relative risk in the female group (age, MMT, and low education) while in the male group six control variables (age, low BMI, smoking, MMT, and low education) were significant predictors. The stronger effect on the older participants supports previous findings (Stessman et al., 2009) and may, as in the woman’s group, be partly explained by the smaller number of significant control variables for predicting longevity in the model. For the younger group six control variables were significant predictors (age, smoking, leg strength and balance, MMT, low education, and living alone) while in the older group, there were only four variables involved (age, low BMI, MMT, and low education).
The remarkably low levels of activity, necessary for survival benefits, found in this study supports previous findings showing that the largest differences in death risk appear when comparisons between zero and any physical activity are made (Bellavia et al., 2013; Moore et al., 2012). This should be considered by health promoters and public health workers. Usually, more frequent and intense activity levels are recommended (Schnohr et al., 2015; Zhao et al., 2015), which may make less capable individuals inclined to give up and believe that health promotion by physical activity is not attainable for them.
A limitation of the study, however, is that the physical activity variable was self-reported, which may increase the risk of recall bias. Still, the study contains several strengths. It is based on a sample that is representative for the Swedish population and covers age groups as high as 60 to 96 years. In addition, few previous studies have adjusted for biological, functional, and social variables in survival analyses. Other strengths include the long observation time (11 years) and the large N of the study (N = 6,896).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for this study from the Swedish government, department of social affairs, and from the participating universities, local governments and county counsils.