
Abstract
Background
As life expectancy continues to rise, the impact of demographic change on health and disease is already evident: increases in age-related illnesses, psychosocial limitations, need for assistance and nursing care present individual, and economic and health policy challenges. Little is known about how patterns of morbidity, frailty, and social determinants are associated with care dependency (CD) in old age. For the purposes of our study, CD means that a person requires substantial assistance in activities of daily living and is therefore receiving benefits covered by long-term care insurance within the German social insurance system. Currently, around 2.9 million people in Germany meet the CD criteria set forth in the German Social Code (SGB XI). The number of care-dependent persons has increased by around 500,000 since 2010 and is projected to reach around 3.4 million by 2030 (Statistisches Bundesamt, 2017). The CD ratio, that is, the percentage of persons requiring care in relation to their peer group, increases significantly with age. Within the 80 to 84 age group, the ratio is approximately 24% for women and 18% for men. In the 85 to 89 age group, this rises to approximately 44% for women and 31% for men. Among the over-90s, 70% of women and more than 50% of men are care-dependent as defined in the German Social Code (Statistisches Bundesamt, 2015).
In the international context, assessment of functional impairments using the Barthel Index (Mahoney & Barthel, 1965; Shah, Vanclay, & Cooper, 1989) or scales for measuring activities of daily living (Katz, Downs, Cash, & Grotz, 1970; Lawton & Brody, 1969; Wallace & Herzog, 1995) may be regarded as broadly approximating the German definition of CD. Corresponding assessment categories are feeding, transfers (bed to chair and back), grooming (personal care), toilet use, independent bathing, mobility (wheelchair/walking), use of stairs, dressing/undressing, and fecal and urinary incontinence.
Very few studies have investigated determinants of CD so far. In a German study by Van den Bussche et al. (2014), which was based on claims data, the authors identified old age, dementia, urinary incontinence, stroke, and cardiac insufficiency as being significantly associated with CD. A German population-based prospective cohort study by Hajek et al. (2017) revealed that the probability that a patient would become care-dependent significantly increased with the onset of old age and dementia. The authors also analyzed the effect of mobility impairment on CD. An international study on longitudinal predictors of functional impairments in older adults in Europe showed that limitations increased significantly with age, depression, cognitive impairment, the number of chronic conditions, less than daily alcohol consumption, smoking, and living without a spouse/partner in the household (Hajek & König, 2016). Borchert and Rothgang (2008) emphasized the protective effect of partnership on CD risk for older men. Information about the sociodemographic determinants of CD (education, income) is particularly patchy and inconsistent (Ramsay, Whincup, Morris, Lennon, & Wannamethee, 2008; Sulander et al., 2012).
Against the background of the limited number of studies on determinants of CD, our exploratory study investigated risk profiles for CD. The Roper–Logan–Tierney (RLT) Model of Nursing (Roper, Logan, & Tierney, 2009) was our theoretical starting point. The RLT Model offers a broader perspective on the emergence and definition of CD since it is based on (health-relevant) activities of daily living and the physical, psychological, and social factors affecting them. Crucially, it is the combination of these various factors that determines the need for care and assistance on a continuum that ranges from complete dependency to complete independence.
Our study therefore investigated how different sets of physical and social determinants were associated with CD. It focused on the following research questions:
Our research was based on the Berlin Initiative Study (BIS), a prospective, longitudinal, population-based cohort study (Ebert et al., 2017; Schaeffner et al., 2010). Because geriatric assessment tools were not integrated until the first follow-up, we will present cross-sectional analyses.
Method
Study Design
The BIS methodology has been described in detail elsewhere (Ebert et al., 2017; Schaeffner et al., 2010). Briefly, BIS is a prospective, longitudinal, population-based cohort study of 2,069 randomly selected elderly participants (≥70 years of age) covered by Germany’s largest health insurance provider. The study was set up to investigate the epidemiology of chronic kidney disease in elderly people and provides information on demographics, lifestyle variables, comorbidities, and cardiovascular events. Study visits took place in 2009, 2011, and 2013. The first follow-up between December 2011 and 2013 with 1,699 respondents from the first wave (response rate: 90.9%, without taking deaths into account) incorporated additional geriatric assessment tools. This article focuses on the first follow-up and provides a cross-sectional analysis of the cohort. The study participants agreed to the collection and transfer of their data in compliance with data protection regulations. The study was approved by the Ethics Commission of Charité – Universitätsmedizin Berlin (Ref. EA2/009/08).
Outcome Measures of CD
In the German health care system, CD is measured by the amount of time (at least 90 min per day over a period of at least 6 months) needed daily for substantial assistance in at least two activities of daily living in the personal hygiene, nutrition, and mobility categories, and, additionally, assistance with domestic tasks. Insurance benefits must be applied for by the person in need of care. The level of care to be provided is determined by an expert assessment conducted in the applicant’s home and may be reviewed at a later date (Buchmann, 2014; Koller et al., 2014). Care services are provided regardless of where the person lives, whether at home or in a retirement or nursing care facility (Schnitzer et al., 2017). In this study, the information about the need for care was obtained from claims data supplied by the participant’s health insurance provider (data were linked to patient survey data).
Morbidities and Health Behavior
Various studies have revealed the association between CD/functional impairments and chronic conditions (Hajek & König, 2016; Koller et al., 2014). We therefore included all chronic conditions and morbidities covered by the BIS dataset: history of stroke, myocardial infarction, cancer, kidney disease (eGFR < 60 ml/min/1.73 m²), diabetes mellitus (intake of antidiabetic medication and/or HbA1c level >6.5%, yes/no), and body mass index (<25, 25-30, >30). Data were collected at baseline through self-reporting, with validation of all defined endpoints (myocardial infarction, stroke) provided by physicians’ letters, generally 2 years after the visit. Certain chronic diseases, for example, diabetes, were additionally validated through laboratory test results (HbA1c) and documented medication. More details are provided in Schaeffner et al. (2010) and Ebert et al. (2017). As regards health behavior, there is some evidence that functional impairments increase with tobacco consumption (Hajek et al., 2017). Physical activity is a protective health factor in older adults (Paterson & Warburton, 2010) and we assumed that the same holds true for CD. We therefore integrated smoking (never smoked or stopped smoking >10 years, current smoker or stopped ≤ 10 years) and physical activity (self-reported frequency of walking at least 30 min: <1 time a week; 1-2 times a week; 3-5 times a week; >5 times a week) in our analyses.
Geriatric Assessment
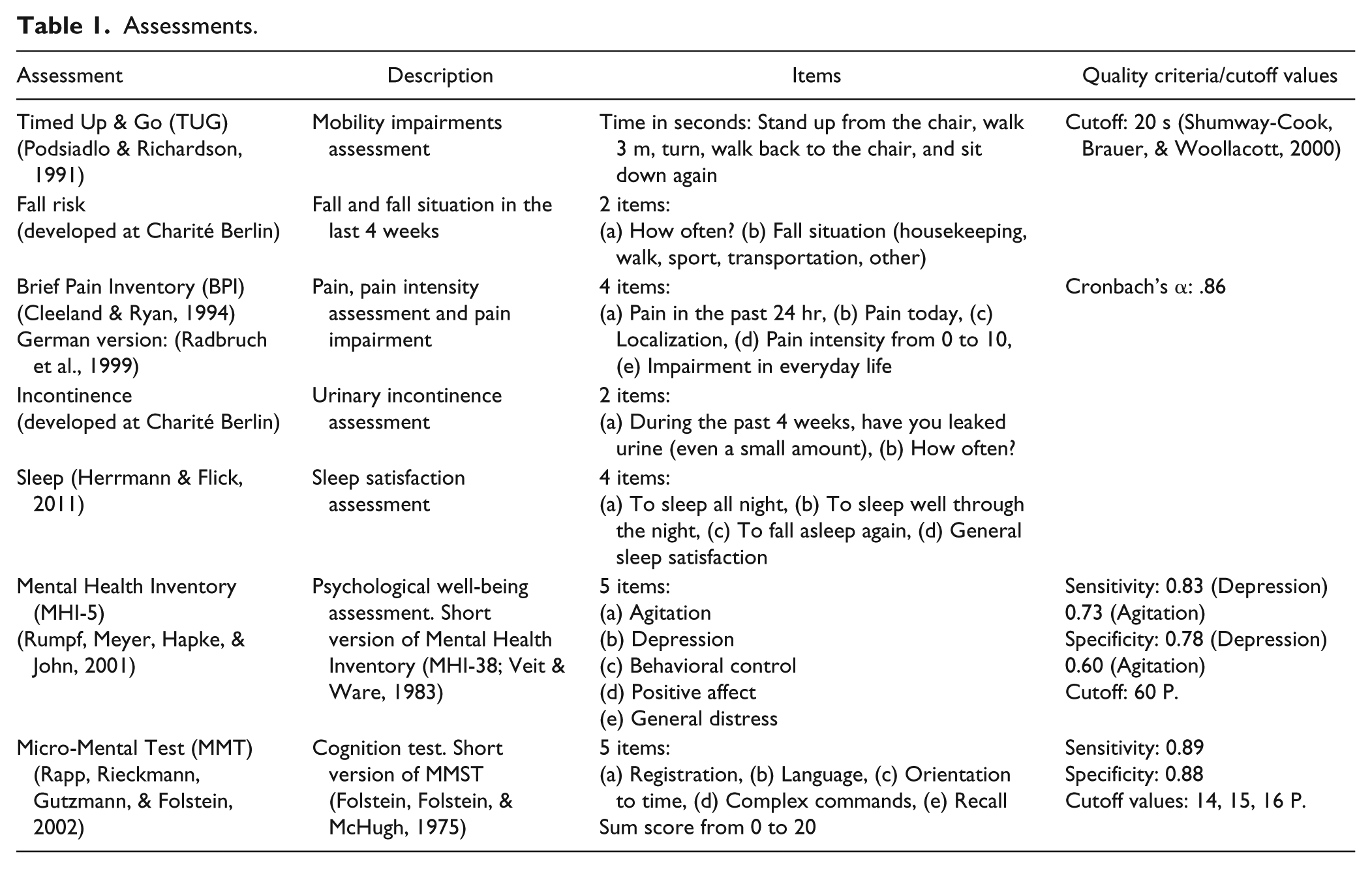
To assess participants’ mobility, we used the Timed Up and Go (TUG) Test and defined limited mobility if participants were unable to perform the TUG Test within 20 s (cutoff value). Pain was assessed using the Brief Pain Inventory. Psychological well-being was assessed with the Mental Health Inventory (MHI-5) and cognitive impairment with the Micro-Mental Test (MMT). Questions about falls, urinary incontinence, and sleep were developed as part of research on geriatric health at Charité Berlin. Table 1 provides an overview of the assessments used, their sources, a brief description, the items included, and their quality criteria (Cleeland & Ryan, 1994; Folstein, Folstein, & McHugh, 1975; Herrmann & Flick, 2011; Podsiadlo & Richardson, 1991; Radbruch et al., 1999; Rapp, Rieckmann, Gutzmann, & Folstein, 2002; Rumpf, Meyer, Hapke, & John, 2001; Shumway-Cook, Brauer, & Woollacott, 2000; Veit & Ware, 1983).
Assessments.
Social Determinants
A large body of scientific evidence has shown that social determinants influence health. This applies particularly to socioeconomic factors such as income and education, but also to gender, age, and social circumstances such as partnership status or networks (Marmot, 2005, 2018). Information about the social determinants of CD is particularly patchy at present. We analyzed gender and age as nonmodifiable determinants and partnership status (“Do you have a partner?”), income (monthly individual net income: low <€1000; moderate €1000-2000; high >€2000), and education (Comparative Analysis of Social Mobility in Industrial Nations [CASMIN]) as modifiable social determinants (Hradil, 2001). The CASMIN index is based on two classification systems, taking into account the qualitative differences between school-based and vocational education (Kunst, 2006). CASMIN’s nine levels of classification were collapsed into three categories: (a) no school-leaving qualifications or low educational level (primary education), (b) intermediate educational level (lower and upper secondary education), and (c) high educational level (bachelor’s, master’s, PhD).
Statistical Analyses
We used the chi-square test or the Mann–Whitney U test to explore group differences between care-dependent and non–care-dependent participants. Statistical significance was set at p < .05. A series of nested binary logistic regression models were used to examine which health-related and social determinants were associated with CD. The stepwise forward procedure was chosen to detect unadjusted and adjusted results and to determine associations between potential explanatory factors. Four models were considered in a manual part by defining the blocks of variable sets. In a first step, we included social determinants (Model 1) and, additionally, parameters of geriatric assessment (Model 2) in a second step. In Model 3, we added morbidities, and in Model 4, we included health behavior (physical activity, smoking) in addition to all previously included variables. The forward Wald procedure was used to guide model entry; only those variables that showed significant effects were selected in the final models. The standard procedure was applied to adjust for gender in all models. We used Nagelkerke R2 to assess the level of explained variance and the Hosmer–Lemeshow test to ascertain the quality of fit. Omnibus tests were conducted to determine whether changes (additions of variables in the different steps) were significant. Test results are listed as footnotes at the bottom of Table 4. The regression results are shown as odds ratios (ORs) and 95% confidence intervals (CIs). All statistical analyses were performed using SPSS 22.
Results
Comparison Between Non–Care-Dependent and Care-Dependent Participants
Of the 1,699 participants studied and surveyed at first follow-up, 18.9% were care-dependent (N = 321; Table 2). The average age of the cohort was 82 years. Care-dependent participants were significantly older (M: 86 years) than participants who were not accessing care services (M: 81 years). Participants with low or intermediate education were care-dependent more often than those with a higher level of formal education. Participants who were not care-dependent reported being in a stable partnership significantly more often (58.0% vs. 36.0%). Regarding mobility, nearly half (47.1%) of all care-dependent participants were unable to do the TUG Test within 20 s, whereas only 8.3% of non–care-dependent people were unable to do so (Table 3). Although more than half (60.9%) of all care-dependent participants were physically inactive (<once a week), 17% reported that they were physically active 1 or 2 times a week and 22.1% reported being active 3 to 4 times a week or more.
Description of the BIS Cohort and Comparison of Participants With and Without Care Dependency at the First Follow-Up.
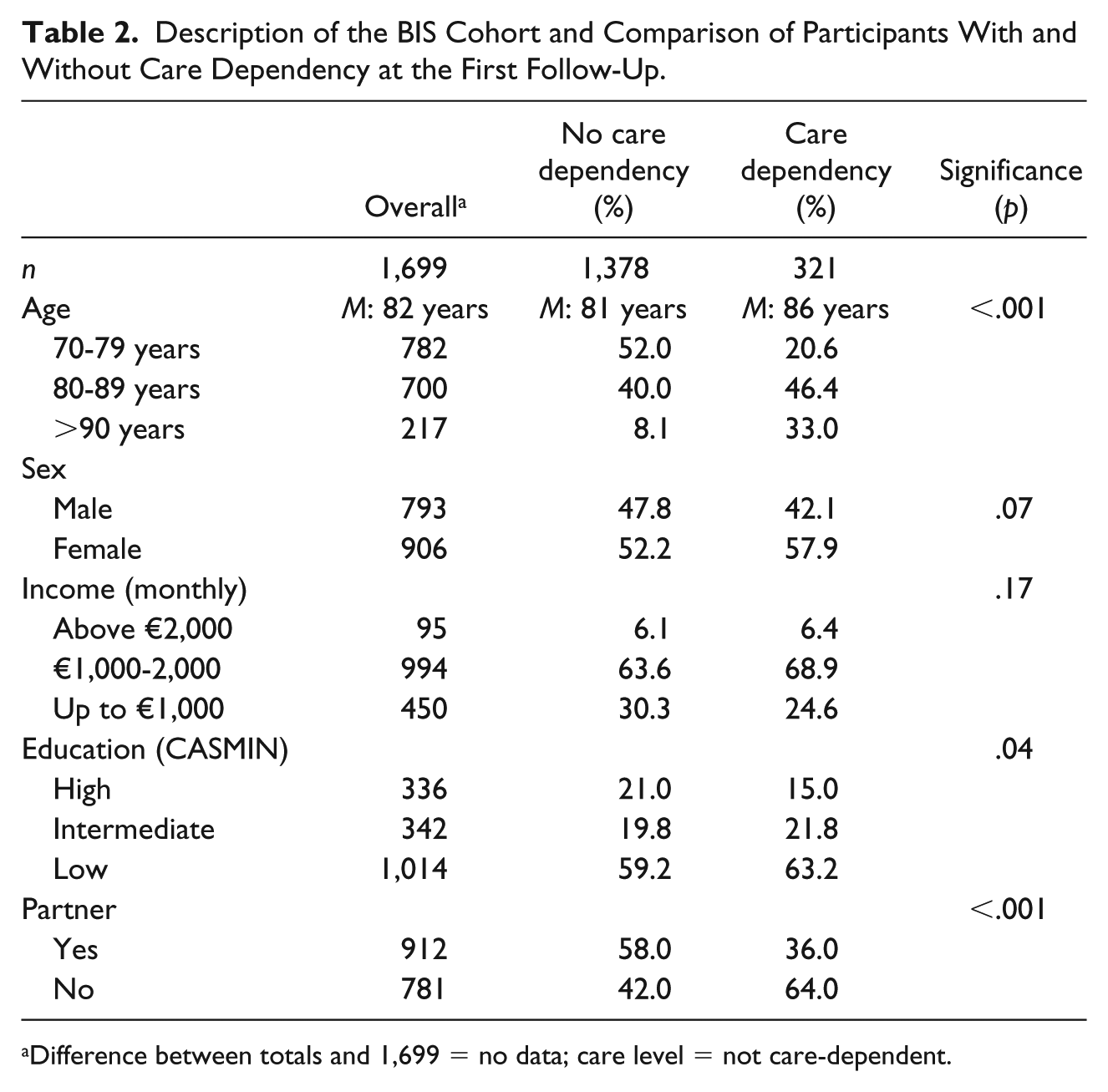
Difference between totals and 1,699 = no data; care level = not care-dependent.
Health (Behavior) of Non–Care-Dependent and Care-Dependent Participants.
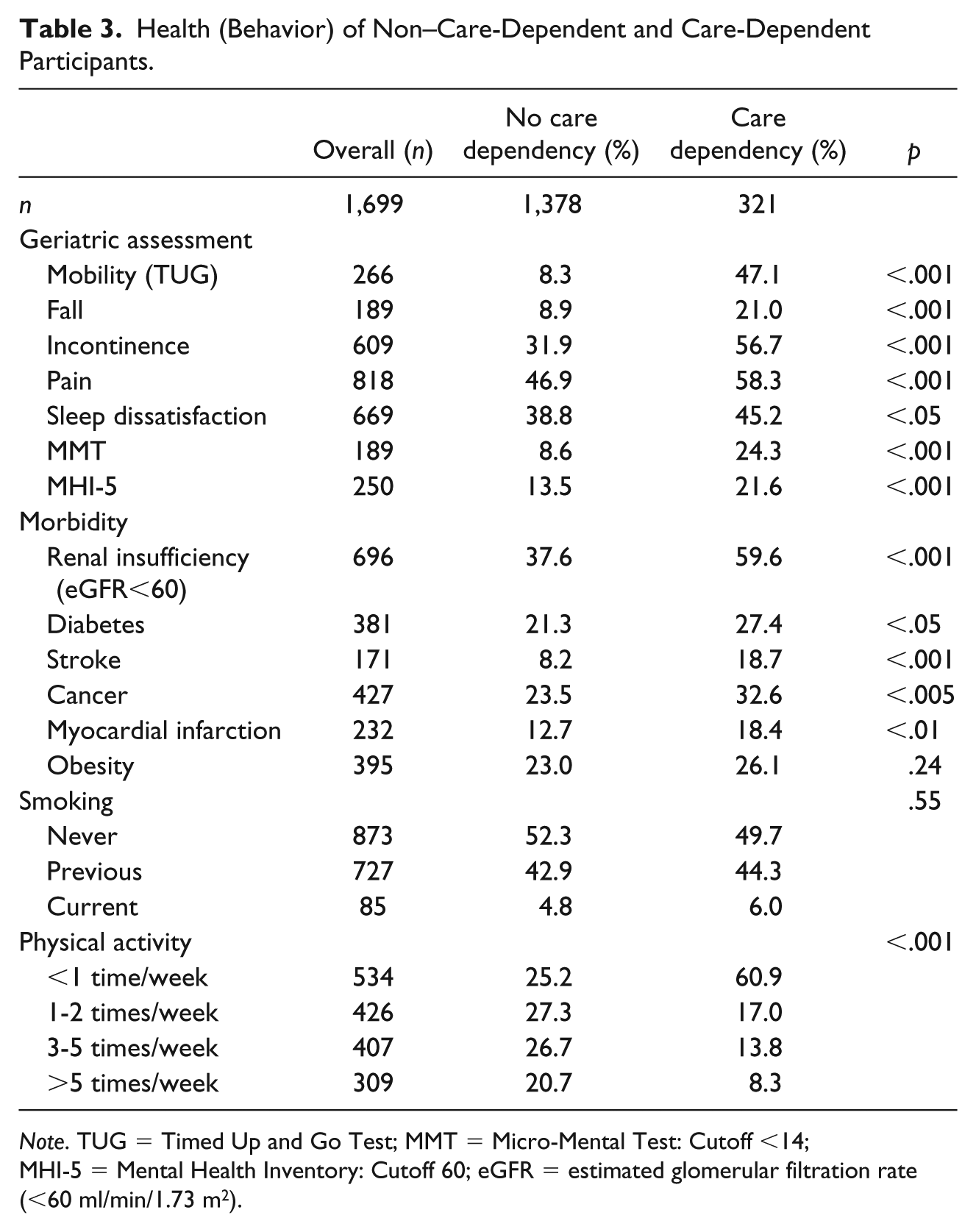
Note. TUG = Timed Up and Go Test; MMT = Micro-Mental Test: Cutoff <14; MHI-5 = Mental Health Inventory: Cutoff 60; eGFR = estimated glomerular filtration rate (<60 ml/min/1.73 m2).
Regression Analysis
When all health-related and social determinants were integrated into the final model (Model 4), the following risk profiles were produced: CD was significantly associated with older age, limited mobility (TUG), falls, urinary incontinence, stroke, cancer, diabetes, limited physical activity, partnership status, and education level (Table 4). ORs for participants with limited mobility were more than 6 times higher than for mobile participants (OR: 6.10; CI: [4.08, 9.11]). Physical activity was not generally associated with CD. Only participants who were physically active less than once a week had a higher risk of being care-dependent (OR: 2.50; CI: [1.47, 4.26]).
Multivariate Associations Between CD, Health-Related and Social Determinants (N = 1,425).
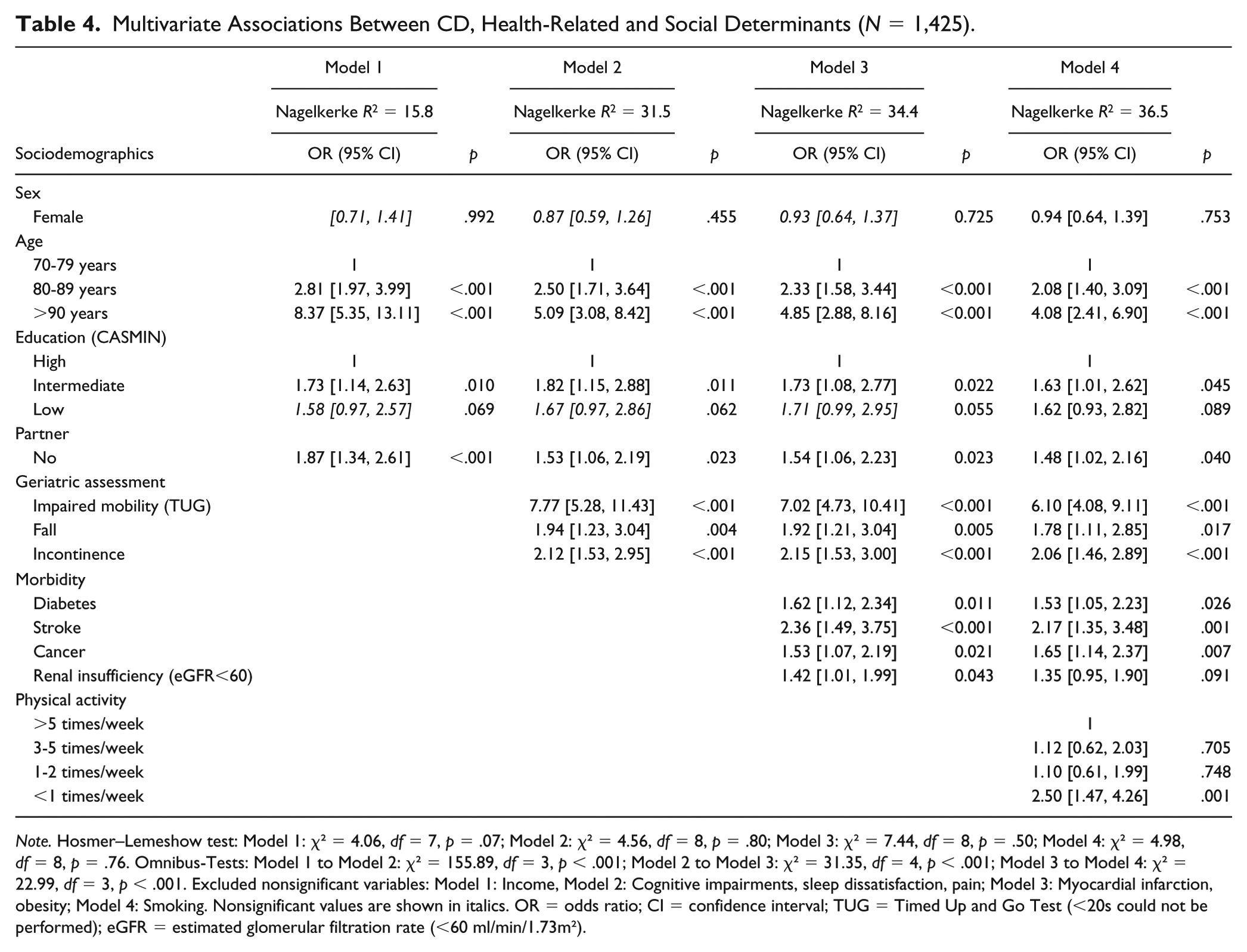
Note. Hosmer–Lemeshow test: Model 1: χ² = 4.06, df = 7, p = .07; Model 2: χ² = 4.56, df = 8, p = .80; Model 3: χ² = 7.44, df = 8, p = .50; Model 4: χ² = 4.98, df = 8, p = .76. Omnibus-Tests: Model 1 to Model 2: χ² = 155.89, df = 3, p < .001; Model 2 to Model 3: χ² = 31.35, df = 4, p < .001; Model 3 to Model 4: χ² = 22.99, df = 3, p < .001. Excluded nonsignificant variables: Model 1: Income, Model 2: Cognitive impairments, sleep dissatisfaction, pain; Model 3: Myocardial infarction, obesity; Model 4: Smoking. Nonsignificant values are shown in italics. OR = odds ratio; CI = confidence interval; TUG = Timed Up and Go Test (<20s could not be performed); eGFR = estimated glomerular filtration rate (<60 ml/min/1.73m²).
Results of Stepwise Regression
In Model 2, when geriatric assessment parameters were included, there was the highest increase in explained variance, from 15.8% in Model 1 to 31.5% in Model 2 (Table 4). Compared to this, the model fit increased less with the inclusion of the morbidities (from 31.5% in Model 2 to 34.4% in Model 3). This indicates that the reported morbidities were reflected in the geriatric assessment tools. With the inclusion of physical activity in the final model (Model 5), more than one third of the total variance could be explained (36.5%). The stepwise forward procedure revealed that the significant association between intermediate education and CD remained stable in all four models, that is, after adjustment for morbidity and geriatric assessment. Although the association between CD and partnership status remained significant in all models as well, here ORs decreased noticeably with the inclusion of geriatric assessment parameters in Model 2 (from OR 1.87 in Model 1 to OR 1.53 in Model 2) and physical activity in Model 4 (from OR 1.54 in Model 3 to OR 1.48 in Model 4). This indicates that the association between partnership status and CD may be partly explained by factors such as limited mobility, falls, and physical activity.
Discussion
Main Results
Our study revealed the following risk profile for CD: older age, urinary incontinence, stroke, falls, cancer, diabetes, education level, and having no partner were significantly associated with CD. Furthermore, care-dependent participants had higher odds of having limited mobility and being less physically active. However, more than half of all care-dependent participants were able to manage the TUG Test and more than one third of all care-dependent participants were physically active on a low level one or more times a week. Our research thus highlights the importance of promoting mobility, even in care-dependent people.
Morbidity
Few studies have explored associations between CD/functional impairments and morbidities. In most of these studies, a multimorbidity index was used (Hajek & König, 2016; Koller et al., 2014). In conformity with our findings, some studies found stroke, cancer, diabetes, and urinary incontinence as determinants (Appelros, Nydevik, & Viitanen, 2003; Kemper, Koller, Glaeske, & van den Bussche, 2011; Koller et al., 2014; McCallum, Simons, Simons, & Friedlander, 2005). Our results thus add to existing knowledge in this context. Urinary incontinence in particular is a well-known risk factor for CD and various authors emphasize that therapeutic measures such as supporting mobility may prevent or delay its onset (Schnitzer et al., 2017). Cognitive impairment was not a predictor in our multivariate analysis. However, this result is difficult to compare with previous studies. Either the tools differ from those applied in our assessment (Hajek & König, 2016) or dementia was used to assess cognitive impairment. Because our assessment is a screening tool used prior to dementia onset (Rapp et al., 2002), comparison of the results was impossible.
Mobility and Physical Activity
Regarding mobility, our findings correspond to the study by Hajek et al. (2017). Here, mobility impairment was a predictor for CD, despite some lack of clarity in connection with the question of how mobility was assessed. It is not surprising that care-dependent participants showed limited mobility more often than non–care-dependent participants due to their worse health status. However, because our data showed that more than half of all care-dependent participants were able to manage the TUG Test, our findings highlight the importance of promoting mobility. This conclusion is reinforced by the results for physical activity. Our analyses showed that nearly 40% of all care-dependent participants were physically active (on a low level) at least once a week. The results of other studies support the finding that physical activity (categorized by a variety of methods) is a protective factor in older adults (Paterson & Warburton, 2010; World Health Organization, 2010). Supporting physical activity, even in care-dependent people, may thus be beneficial to health. In a review of the effects of physical activity and exercise on cognitive and brain functions in older adults, the authors found that frailty is not a contraindication for physical activity; on the contrary, it is a compelling reason to prescribe physical exercise (Bherer, Erickson, & Liu-Ambrose, 2013). Our results confirm this recommendation.
Social Determinants
The association between age and CD/functional impairments is well established (Hajek & König, 2016; Schnitzer et al., 2015). By contrast, research findings on gender-specific differences are less consistent, varying according to whether they are adjusted for age and morbidities (Hajek et al., 2016; Schnitzer et al., 2017). Regarding the effect of education on CD, results are scarce and inconsistent. Some studies identified an increased risk of disability (Sulander et al., 2012) and functional impairments (Huisman et al., 2005) for less educated older adults. Because results were not adjusted for morbidities in these studies, this may be explained by subjects’ poorer health. However, in our study a significant association between CD and rather low (intermediate) education remained even after adjustment for morbidities and geriatric assessment parameters. Our findings thus indicate that the higher odds of participants with rather low (intermediate) education being care-dependent can only partially be explained by their poorer health.
Due to the various measures used for partnership and living situation (marital status, partnership irrespective of marital status, living together), our findings are difficult to compare. However, most of the studies revealed a higher risk of CD or functional impairments onset for older adults without a partner/living alone (Hajek & König, 2016; Kharicha et al., 2007; Nilsson, Avlund, & Lund, 2010). Hajek assumed that “living alone” as a risk factor for FI might be explained by the fact that it reflects other factors that increase the risk of FI, such as falls or decreased physical activity (Hajek & König, 2016). This hypothesis may be supported by our data as the effects of partnership decreased after adjustment for limited mobility, falls, urinary incontinence, and physical activity. Further research is required to investigate the possible role of partnership status in preventing and delaying CD.
Strengths and Weaknesses
In our data, morbidities, laboratory and study parameters such as body mass index, and a broad range of survey data were collected. These data were merged with health insurance data to obtain information about participant’s need for care. This combination of survey, study, and health insurance data, along with participants’ high average age, is our study’s particular strength. Few previous studies have combined these various data sources; however, this approach is increasingly recommended (Unger, Giersiepen, & Windzio, 2015). Another strength of our study is that it assesses a fairly comprehensive list of social determinants and the CD measurement, something that has not been done systematically before in the way the authors did.
Some limitations should be mentioned. Only 8.1% of the participants contacted for the baseline survey could be included. However, this response rate is not unusual, especially with elderly people, as the willingness to participate in studies is known to decrease with age (Murphy, Schwerin, Eyerman, & Kennet, 2008). The low response rate had no impact on the morbidity structure of the participants, as was shown by a rigorous comparison of the distribution of chronic diseases in the study cohort and among the provider’s insurees of the same age and gender from which the study population was drawn (Ebert et al., 2017). Another limitation may be that the number of care-dependent participants in the BIS cohort was underestimated, as participants who are receiving informal care without accessing care services or who have not (yet) applied for care-related benefits were not included. The number of physically active participants may have been underestimated as well, because we only assessed regular walking, not activities such as household chores, or cycling (World Health Organization, 2010). For our statistical analysis, we conducted stepwise regression analyses to explore unadjusted and adjusted results and to assess the percentage variability explained by the models. This may be a limitation because the degree of explained variance will always increase when variables are added to the model. To mitigate this limitation, we compared the different models’ Nagelkerke values and conducted the Hosmer–Lemeshow test to obtain more information about the quality of fit. As in other observational studies, we cannot exclude potential residual confounding, although—based on the literature—we considered a wide range of relevant determinants.
As the results described above are based on cross-sectional analyses, it is not possible to draw firm conclusions about causality between health-relevant factors (morbidities, health behavior, geriatric testing, and social variables) and the onset of CD. It does, however, seem plausible that morbidities (stroke, cancer, myocardial infarction, kidney disease and diabetes) often occur ahead of the need for care—in that these diagnoses give rise to a requirement for care—whereas limited physical activity and mobility may often be the consequence of existing CD.
Conclusion
Our research highlights the importance of promoting mobility, even in care-dependent people. Physical activity and mobility are significant in two respects: First, these factors make appropriate interventions highly accessible and influenceable. Second, the present study shows that almost 40% of participants who are already care-dependent report being physically active to some degree despite limitations. This shows that even after the onset of CD, activity and mobility remain important starting points for tertiary prevention.
Footnotes
Authors’ Note
Susanne Schnitzer and Stefan Blüher shared first authorship.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the KfH Foundation of Preventive Medicine. Responsibility for the content lies with the authors.