
Abstract
Introduction
Cancer is the second leading cause of death in the United States. In 2014, about 23% of the 2.6 million deaths in the United States were attributed to cancer (National Center for Health Statistics, Centers for Disease Control Prevention, 2015). Cancer screening has been identified as an effective way to detecting colon cancer, breast cancer, and cervical cancer at an early stage and to reducing mortality rates (U.S. Preventive Services Task Force, 2011). In 2015, the aged-adjusted screening rates for colorectal cancer, breast cancer, and cervical cancer among U.S. adults were 62.4%, 71.5%, and 83.0%, respectively (Sabatino, White, Thompson, Klabunde, & Centers for Disease Control and Prevention 2015). Healthy People 2020 (US Department of Health and Human Services et al., 2010) established a long-term goal for achieving rates of 70.5% for colon cancer screening, 81.1% for breast cancer screening, 93% for cervical cancer screening, and 15.9% for discussion with health providers about the prostate specific antigen (PSA) test for prostate cancer.
Among Asian Americans, cancer is the leading cause of death (Kochanek, Xu, Murphy, Miniño, & Kung, 2014). Chinese Americans, with a population of 4 million, represent the largest Asian group in the United States (Hoeffel, Rastogi, Kim, & Hasan, 2012). Among Chinese American men and women, prostate cancer, breast cancer, and colorectal cancer are among the top five aged-adjusted cancers and causes of death (Miller, Chu, Hankey, & Ries, 2008). Prior research had found that older Chinese Americans were less likely to participate in early detection cancer screening compared to other Americans (Chen, Diamant, Kagawa-Singer, Pourat, & Wold, 2004; Kagawa-Singer & Pourat, 2000; Simon, Li, & Dong, 2014; Tang, Solomon, & McCracken, 2001). For example, study results from the Population Study of Chinese Elderly in Chicago (PINE; Dong, Wong, & Simon, 2014), which is a community-engaged, population-based epidemiological study of U.S. Chinese older adults aged 60 years and above in the Greater Chicago area, showed the screening rate for colon cancer, breast cancer, cervical cancer, and prostate cancer were low (Simon et al., 2014). Prior research, while informative, had not examined adherence to current cancer screening recommendations and factors associated with adherence to lifetime and current screening.
Acculturation and health literacy have been shown to predict access to health care and engagement in cancer screening behaviors (Levy & Janke, 2016; Pirisi, 2000; Solis, Marks, Garcia, & Shelton, 1990). Acculturation is known as the complex process of individualized internal adaptation of beliefs, practices, and values to a host culture (Padilla & Perez, 2003). Health literacy is commonly defined as “the degree to which individuals have the capacity to obtain, process and understand basic health information needed to make appropriate health decisions” (U.S. Department of Health and Human Services, 2014). Prior studies further showed relationship between, acculturation, health literacy, and cancer screening behaviors among racial/ethnic minorities and immigrant populations (Johnson-Kozlow, 2010; Peterson, Dwyer, Mulvaney, Dietrich, & Rothman, 2007; Sentell, Tsoh, Davis, Davis, & Braun, 2015). However, the aforementioned relationships have not been extensively studied among older Chinese Americans.
Our study adopted the well-known Andersen’s Behavioral Model of Health Services Utilization (R. Andersen, 1968; R. M. Andersen, 1995) as a framework to identify participants’ characteristics that may influence cancer screening behavior based on predisposing, enabling, and need factors. Predisposing factors are those that describe an individual’s propensity to use health services. Enabling factors are those that describe an individual’s access to and ability to use health services. Finally, need factors describe an individual’s probability of using health services for the occurrence of illness. The purpose of this study was to examine the influence of acculturation and health literacy on lifetime cancer screening utilizations and adherence to age-appropriate cancer screening guidelines. We hypothesized that higher health literacy and acculturation levels were associated with an increased likelihood of lifetime and current cancer screening among older Chinese Americans.
Method
Population and Settings
This study utilized a cross-sectional study design to analyze existing data obtained from the larger Population Study of Chinese Elderly in Chicago (PINE) collected between 2011 and 2013 (N = 3,157). The PINE study is a community-engaged, population-based epidemiological study that collects data from Chinese people aged 60 years and above, who self-identified as Chinese and live in the greater Chicago area (Dong, 2014; Dong et al., 2014).
Study Measurements
Predisposing factors
Predisposing factors measured for this study included age (in years), gender, education (in years), marital status (married/not married), language preference (Mandarin/others), years in the United States (in years), and years in the community (in years), and country of origin (China/Other).
Enabling factors
In this study, personal income in a 10-point scale (1 = US$0-US$4,999; 2 = US$5,000-US$9,999; 3 = US$10,000-US$14,999; 4 = US$15,000-US$19,999; 5 = US$20,000-US$24,999; 6 = US$25,000-US$29,999; 7 = US$30,000-US$34,999; 8 = US$35,000-US$39,999; 9 = US$40,000-US$44,999; 10 = ≥ US$45,000), health insurance coverage (yes/no), number of alive children, and living arrangement (in a scale of 0-10) were measured as enabling factors.
Need factors
Need factors measured were overall health status, health changes over the past year, and quality of life. Overall, health status was measured by the question, “In general, how would you rate your health?” (1 = poor, 2 = fair, 3 = good, 4 = very good). Health changes over the last year was measured by the question, “Compared to 1 year ago, how would you rate your health now?” (1 = worsened, 2 = same, 3 = improved). In addition, quality of life was assessed by asking “in general, how would you rate your quality of life” on a 4-point scale ranging from 1 = poor to 4 = very good.
Acculturation and health literacy
Acculturation was measured based on the PINE study Acculturation Scale with a Cronbach’s alpha of .88 (Dong, Bergren, & Chang, 2015), which was derived from a validated acculturation scale used in minority populations (Marin, Sabogal, Marin, Otero-Sabogal, & Perez-Stable, 1987). The PINE Study Acculturation Scale is multidimensional, including (a) language use—questions address proficiency and preferences for speaking a given language in five different settings (read and speak, as a child, at home, while thinking, with friends) on a 5-point scale (1 = only Chinese, 5 = only English); (b) media use—questions address use and preference of English and Chinese media (television and radio) on a 5-point scale (1 = only Chinese, 5 = only English); and (c) ethnic social relations—questions address preferred ethnicity of those with whom the participant interacts (close friends, people at parties, visitors, children’s friends) on a 5-point scale (1 = only Chinese, 5 = only Americans). For each participant, total acculturation scores ranged from 12 to 60. Higher numbers correspond to higher levels of acculturation. The tertiles of total acculturation scores among the participants were then calculated and were labeled as (a) least acculturated (scored 12-13), (b) medium acculturated (scored 14), and (c) high acculturated (scored ≥15; González, Haan, & Hinton, 2001).
Health literacy was measured using the Chinese version of the Rapid Estimate of Adult Literacy in Medicine, Revised (REALM-R) test (Bass, Wilson, & Griffith, 2003). Study participants were asked to read 11 items, including Fat, Flu, Pill, Osteoporosis, Allergic, Jaundice, Anemia, Fatigue, Directed, Colitis, and Constipation, written in Chinese. Because three items, Fat, Flu, and Pill, were included to minimize study participants’ anxiety, the test score for each study participant was determined by his or her reading of the remaining eight items: Osteoporosis, Allergic, Jaundice, Anemia, Fatigue, Directed, Colitis, and Constipation. The overall REALM-R test score ranged from 0 to 8. Test participants receiving a score of 6 or less were categorized as having a low literacy level.
Cancer screening behaviors
Four cancer screening behaviors, including (a) breast cancer screening, (b) cervical cancer screening, (c) colorectal cancer, and (d) prostate cancer screening, were examined. Depending on the participant’s gender, individuals were asked the following: “Have you ever had colonoscopy exam, mammogram, Pap test, or Prostate-Specific Antigen (PSA) test? (yes, no)” and “How long has it been since you had your last colonoscopy exam, mammogram, Pap test, or PSA test?” (within the past year, within the past 2 years, within the past 3 years, within the past 5 years, or 5 or more years. Reponses collected from the two cancer screening questions were used to measure participant’s “adherence to cancer screening (yes, no)” according to the 2011-2013 American Cancer Society (ACS, 2015) Guidelines for the Early Detection of Cancer: (a) Adherence to breast cancer screening. ACS recommends mammograms for all women at age 40 years and above every year. Female participants who reported having received a mammogram within past year were coded as adherers; (b) Adherence to cervical cancer screening. ACS Screening Guidelines recommend that all women who are 30 years and above should have a Pap test every 3 years. Female participants who reported having done a Pap test within past 3 years were coded as adherers; and (c) Adherence to colorectal cancer screening. ACS Screening Guidelines recommend that both men and women starting at age 50 years old should have receive a colonoscopy every 10 years. All participants who reported receiving a colonoscopy within past 10 years were coded as adherer. In addition, ACS guideline indicated that men should make an informed decision with their health care provider whether to be screened for prostate cancer. As such, no specific age-related screening guidelines exist. Consequently, we only asked about ever screening for prostate cancer.
Data analysis
The analytic sample included 3,157 older Chinese American from the PINE study. Descriptive statistics (M, SD, frequency, and percentage) were used to describe the characteristics of study participants. Bivariate analyses (Chi-square and Wilcoxon rank sum test) were conducted to identify significant predisposing, enabling, and need predictors of cancer screening behaviors among older Chinese population (data not shown). Finally, logistic regression analysis was performed to access the influences of health literacy and acculturation on cancer screening utilizations and adherence to cancer screening guideline after controlling for significant predisposing, enabling, and need factors identified from bivariate analyses. All analyses were performed using SAS, a statistical software package.
Results
Sample Characteristics
The mean age of the participants was 72.81± 8.30 years. Over two thirds of the participants had completed no more than a high school degree (78.91%, n = 2,476), were insured (75.98%, n = 2,385), had an annual income of less than US$10,000 (85.10%, n = 2,656), were born in China (92.62%, n = 2,924), and preferred to speak language other than English (98.99%, n = 3,125).
Cancer Screening Behaviors
Participant’s cancer screening behaviors are shown in Table 1. Lifetime rates of ever screening were low for PSA test (27.73%, n = 353), followed by colonoscopy (28.44%, n = 895), Pap test (40.73%, n = 740), and mammography (59.57%, n = 1,083). According to the ACS guidelines, rates of adherence for recent screening was also low each cancer screening site: breast cancer (26.72%, n = 481), cervical cancer (24.24%, n = 440), and colorectal cancer (24.60%, n = 771) screening.
Cancer Screening Behaviors Among Older Chinese American (N = 3,157).
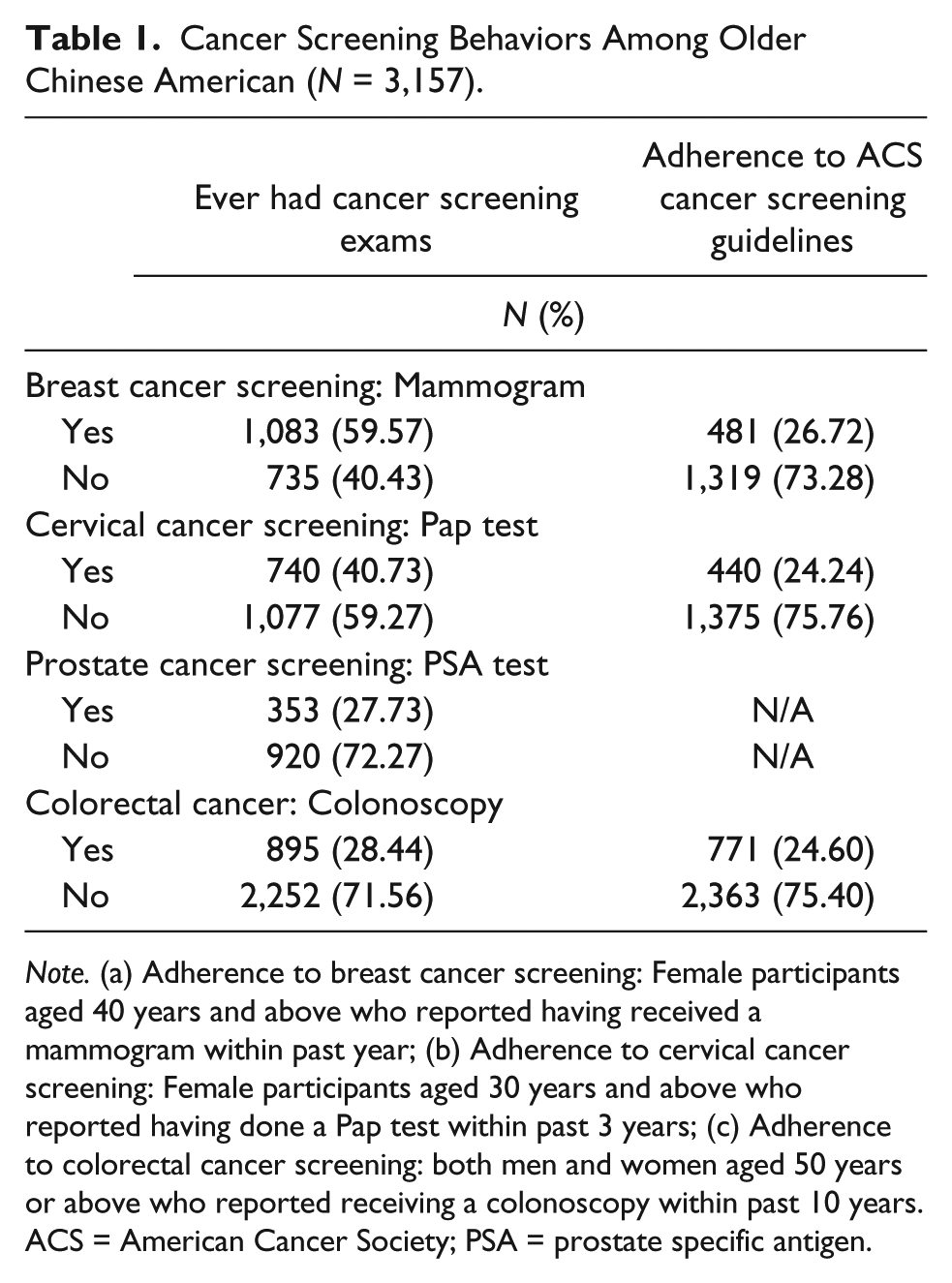
Note. (a) Adherence to breast cancer screening: Female participants aged 40 years and above who reported having received a mammogram within past year; (b) Adherence to cervical cancer screening: Female participants aged 30 years and above who reported having done a Pap test within past 3 years; (c) Adherence to colorectal cancer screening: both men and women aged 50 years or above who reported receiving a colonoscopy within past 10 years. ACS = American Cancer Society; PSA = prostate specific antigen.
Acculturation, Health Literacy, and Cancer Screening Behaviors
In the study, 40.01% and 64.64% of the participants were identified as being in “least acculturated” group (n = 1,263) and having lower level of health literacy (n = 1,172), respectively. Results from logistic regression models showed that acculturation and health literacy were significantly associated with lifetime cancer screening utilizations after controlling for significant predisposing, enabling, and need factors. High acculturated, (odds ratio [OR] = 1.72, 95% confidence interval (CI) = [1.35, 2.20]), or medium acculturated (OR = 1.51, 95% CI = [1.19, 1.94]) people, and high health literacy people (OR = 1.72, 95% CI = [1.31, 2.25]) were more likely to have ever had mammogram compared to least acculturated and low health literacy people, respectively. The same trend was observed for Pap test among high (OR = 1.84, 95% CI = [1.41, 2.42]) or medium acculturated (OR = 1.64, 95% CI = [1.27, 2.11]) people and high health literacy people (OR = 1.64, 95% CI = [1.25, 2.14]; Table 2). In addition, individuals with high health literacy (OR = 1.68, 95% CI = [1.02, 2.78]) were more likely to have ever had PSA test compared with those with low health literacy. Medium (OR = 1.28, 95% CI = [1.03, 1.59]) and high acculturated (OR = 1.79, 95% CI = [1.44, 2.23]) groups were associated with higher odds of colonoscopy exam utilization (Table 2). Furthermore some common factors (age, years in the United States, language preference, income, overall health status, and quality of life) were significantly associated with lifetime cancer screening utilizations (Table 2).
The Influence of Acculturation and Health Literacy Levels on Ever Had Cancer Screening Exams.
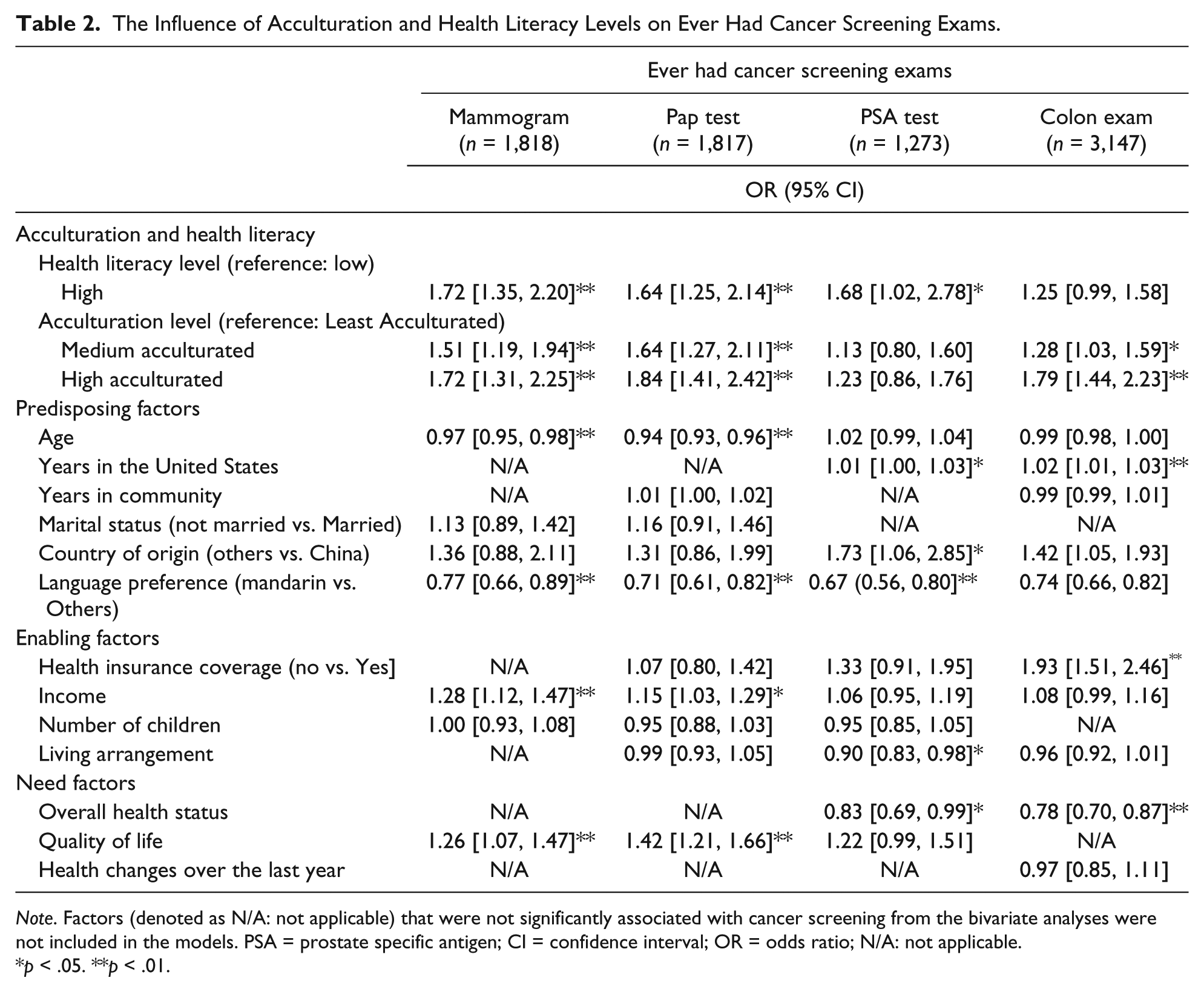
Note. Factors (denoted as N/A: not applicable) that were not significantly associated with cancer screening from the bivariate analyses were not included in the models. PSA = prostate specific antigen; CI = confidence interval; OR = odds ratio; N/A: not applicable.
p < .05. **p < .01.
Next, we examined the relationship between acculturation, health literacy, and adherence to ACS cancer screening guidelines (Table 3). High level of health literacy was associated with higher odds of being adherent to colonoscopy exam (OR = 1.39, 95% CI = [1.08, 1.77]). Higher levels of acculturation was associated with an increased likelihood of adherence to mammography (OR = 1.75, 95% CI = [1.30, 2.34]), Pap test (OR = 1.60, 95% CI = [1.16, 2.19]), and colonoscopy guidelines (OR = 2.06, 95% CI = [1.63, 2.59]) compared with those who were less acculturated. In addition, people in the medium acculturated group were also more likely to being adherent to Pap test (OR = 1.40, 95% CI = [1.03, 1.89]) and colonoscopy exam (OR = 1.43, 95% CI = [1.14, 1.79]; Table 3). Common factors that had impact on adherence to cancer screening guideline were age, language spoken, income, and quality of life.
The Influence of Acculturation and Health Literacy Levels on Adherence to ACS Cancer Screening Guidelines.

Note. Factors (denoted as N/A: not applicable) that were not significantly associated with cancer screening from the bivariate analyses were not included in the models. ACS = American Cancer Society; PSA = prostate specific antigen; CI = confidence interval; OR = odds ratio; N/A: not applicable.
p < .05. **p < .01.
Discussion
In the study, over two in five older Chinese Americans were least acculturated or had a low health literacy. Most people did not meet the recommendations for early detection cancer screening guidelines made by ACS. Our study further shows that health literacy and acculturation are factors that have important impact on lifetime cancer screening utilizations and adherence to cancer screening guideline after controlling predisposing, enabling and need factors among older Chinese Americans.
The average years of living in the United States were over 20 years among study participants. However, more than 90% preferred to speak Mandarin or dialects such as Cantonese or Toishanese rather than English. This was reflected on low acculturation levels among older Chinese. In addition, low health literacy levels are associated with low education levels. In the study, only one fifth of study participants had college or above education degree. Furthermore, our findings are consistent with prior research, showing that health literacy (Sentell et al., 2015; U.S. Department of Health and Human Services, 2014) or acculturation levels (Yi, 1998; Juon, Seo, & Kim, 2002; S. Lee, Chen, Jung, Baezconde-Garbanati, & Juon, 2014; Pourat, Kagawa-Singer, Breen, & Sripipatana, 2010) were associated with cancer screening utilizations. Health literacy and acculturation are further associated with adherence to cancer screening guidelines among older Chinese Americans. In addition, consistent with Anderson’s Model, predisposing, enabling and need factors were associated with cancer screening utilizations. Among these factors, older age, living in the United States shorter, prefer speaking Mandarin, lower income, uninsured, and lower quality of life were associated with a decreased likelihood of ever had and being adherent to cancer screening such as mammogram, Pap test, or colon exam. These findings are consistent with the extant literature that highlights the role of demographic, socioeconomic, and health factors as contributing to lower cancer screening utilizations among Asian Americans (Kim & Casado, 2016; H. Y. Lee, Lundquist, Ju, Luo, & Townsend, 2011; Pourat et al., 2010; Wong, Gildengorin, Nguyen, & Mock, 2005).
This study has implications for research and practice. To our best knowledge, this is the first study that uses the data from a largest epidemiological study of Chinese older adults in the United States to examine the influence of acculturation and health literacy on cancer screening behaviors. Future study can examine the distinct roles of acculturation and health literacy by examining the combined burdens of low acculturation and low health literacy on cancer screening utilizations and guideline adherence in older Chinese population. Furthermore, this study utilized a cross-sectional design and future study can apply a longitudinal design to investigate the relationship of changes in acculturation or health literacy overtime on cancer screening behavior. In practice, to uptake cancer screening among older Chinese Americans, the first is to improve the health literacy. In this study, the majority were low health literacy and low-educated people who may not have sufficient knowledge on cancer screening. The development of health education material on cancer screening is necessary and should be tailored to the needs of older Chinese by simplifying and translating information into the language (e.g., Mandarin) they can better understand. The second is to provide not only linguistically but also culturally appropriate cancer screening services. Prior research have shown that culturally related health beliefs can have an impact on cancer screening behaviors (Gifford, 1991; Rajaram & Rashidi, 1998). Among Chinese populations, culture-specific beliefs about cancer causation include that cancer is the result of God’s will or due to fate, or is the punishment as a result of one’s ancestor’s conduct (Wong-Kim, Sun, & DeMattos, 2003). These findings suggest the ongoing need for cancer screening interventions in this lower-acculturated older Chinese population and highlight the importance of health literacy, language, acculturation, and culturally influenced beliefs in screening. Furthermore, cancer screening intervention can be combined with patient navigation, which is a well-established strategy for improving access to health care services (Freeman, 2015) and reducing the barriers that contribute to cancer health disparities in vulnerable populations (Jandorf et al., 2013). Patient navigators who share the same language, culture, and beliefs as the community members they serve are an effective link between health promotion programs and the community (Genoff et al., 2016) and can address patients’ informational, emotional, and practical needs associated with cancer care (Stephens, 2015). Prior research among Chinese population has shown that patient navigation is feasible and can increase patient satisfaction, knowledge, and participation in cancer treatment (McClung et al., 2015) and has demonstrated a positive impact of patient navigation on actual cancer screening rates (Wang, Fang, Tan, Liu, & Ma, 2010). In addition, developmental research has shown that Chinese immigrant cancer patients are more interested in patient navigation that is culturally and linguistically tailored (Leng et al., 2014).
Finally, some study limitations should be concerned in this study. First, the Chinese version of REALM-R test was used to assess health literacy level among older Chinese people. The original REALM-R instrument was developed and administered among Americans. Therefore, Chinese version of REALM-R may not correctly reflect older Chinese people’s ability to understand health information. Second, acculturation is not unidimensional (Padilla & Perez, 2003) and could be influenced by the changes within immigrant groups and the host cultural. Therefore, the overall level of acculturation measured among older Chinese in the greater Chicago area cannot be generalized to other older Chinese populations in the Unites States. Finally, given the nature of survey data, the accuracy of cancer screening behaviors measured among older Chinese population might be concerned due to self-reported bias.
Conclusion
Acculturation and health literacy have been recognized as important factors that are associated with engagement in preventive health behaviors such as cancer screening. Our study shows that levels of acculturation and health literacy are associated with lifetime cancer screening utilizations and adherence to cancer screening guideline among older Chinese Americans living in the greater Chicago area. In the future, local community organizations can work with primary care practice, older adults, and family members to develop a culturally and linguistically intervention combined with patient navigation to engage older Chinese adults in cancer screening.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.