
Abstract
Introduction
Cancer screening is an important strategy for the early detection of cancers. It plays a crucial role in reducing the burden of morbidity and mortality due to cancer. A lack of screening is associated with increased late stage cancer diagnosis and lower cancer survival rates. Despite the benefits, disparities in cancer screening exist among minority populations in the United States (Smith et al., 2015). It is imperative to explore associated factors that influence cancer screening utilization in these populations.
Disparities in cancer screening have been addressed in the overall Asian American population (Hou, Sealy, & Kabiru, 2011). However, heterogeneity in cancer screening behaviors has been noted among different Asian American subgroups as well (Le et al., 2014). The Chinese community constitutes the largest Asian subgroup in the United States. Prior studies demonstrate the distinct health needs and medical conditions of this population from other Asian subgroups (Dong et al., 2011; Dong, Chen, & Simon, 2014). Furthermore, our previous study reveals that cancer screening utilization was lower among Chinese American older adults than the national level (Simon, Li, & Dong, 2014b). This may be one of the risk factors related to high incidence of some cancers among Chinese American population (McCracken et al., 2007).
In the general population, common barriers to cancer screening have been recognized, such as a lack of knowledge, health insurance, and physician recommendations, as well as lower socioeconomic status (Simon et al., 2013; Simon et al., 2015; Womeodu & Bailey, 1996). In addition to these common barriers, unique sociocultural barriers to cancer screening have been considered being more influential on cancer screening behaviors among Chinese American population especially among older adults (Holroyd, Twinn, & Adab, 2004; Tang, Solomon, & McCracken, 2000). Prior studies emphasize the uniqueness of traditional Chinese cultural health beliefs and views, such as fatalism and a preference for Chinese medicine and demonstrate their influences on cancer screening in older adults (Dong, Bergren, & Chang, 2015b; Liang et al., 2009; Simon, Tom, & Dong, 2017). Within the Chinese health promotion paradigm, Wu, West, Chen, and Hergert (2006) found that the main reason for nonparticipation in cancer screening among Chinese elders is the absence of any symptoms. Therefore, it is pivotal to expand understanding of sociocultural factors in cancer screening to provide tailored information for cancer screening promotion among this population.
Social engagement, as an important sociocultural factor, is a core component of “successful aging.” It involves engaging cognitive, social and productive activities that range from watching TV, visiting friends, and participating in community groups, to volunteering (Rowe & Kahn, 1997). Active social engagement contributes to promoting health outcomes among older adults (Bath & Deeg, 2005). Prior findings indicate that active community participation was more likely to increase cancer screening utilization among Black and White Americans (Kinney, Bloor, Martin, & Sandler, 2005). In addition, a recent study reports that a change in social engagement was associated with changes in cancer screening intentions among Hispanics and others (Molina, Briant, Sanchez, O’Connell, & Thompson, 2018). These findings support the notion of social engagement as a potential facilitator of cancer screening utilization.
With respect to social engagement among Chinese Americans, our previous study has identified unique social engagement patterns among Chinese older adults (Dong, Li, & Simon, 2014). However, little is known about the relationship between these distinct social engagement patterns and cancer screening behaviors among this population. To fill this gap in knowledge, assuming that social engagement has the potential to promote cancer screening, the purpose of this study was to examine the association between social engagement and cancer screening utilization among a community-dwelling Chinese American older population.
Method
Study Population
Data were drawn from the PINE study, a cross-sectional epidemiological study of Chinese American older adults conducted from 2011 to 2013 in the Greater Chicago area. Older adults who aged 60 years and above and self- identified as Chinese were eligible to participate in the study. Using community-based participatory research strategy, eligible candidates were approached and recruited with more than 20 social services agencies, community centers, health advocacy agencies, senior apartments, and social organizations serving as the basis of recruitment sites. Out of 3,542 eligible participants, 3,157 agreed to participate in the study. Face-to-face interviews were conducted by trained multilingual interviewers in participants’ preferred language and dialect. More details of the study design and procedure have been published (Dong, Chang, Simon, & Wong, 2011; Dong, Wong, & Simon, 2014). The PINE Study is representative of the aging Chinese population in the Greater Chicago area with respect to important demographic attributes (Simon, Chang, Rajan, Welch, & Dong, 2014). The study was approved by the Institutional Review Board of the Rush University Medical Center.
Cancer Screening Utilization
Cancer screening utilization was assessed by asking participants whether they had ever utilized a blood stool test and colonoscopy for colon cancer screening, mammography for breast cancer screening, a Pap test for cervical cancer screening, or a prostate specific antigen (PSA) test for prostate cancer screening. In this study, cancer screening utilization was categorized dichotomously as either “Yes” or “No.”
Social Engagement
Social engagement was assessed using a 16-question instrument, which categorized social engagement activities into two subdomains: cognitive activity and social activity (Dong et al., 2014). Briefly, cognitive activity was measured by asking how often the participants: (a) watch TV; (b) listen to the radio; (c) read newspapers; (d) read magazines; (e) read books; (f) play games; (g) play mahjong, and (h) how much time they spend reading each day. Items “a” to “g” were scored using a 4-point scale from 0 = once a year or less to 4 = every day or almost every day. Item “h” was scored using a 5-point scale from 0 = none to 5 = more than 3 hr. The score for cognitive activity ranged from 0 to 33. Social activity was measured by asking how often the participants: (a) go out to a movie, restaurant, or sporting event; (b) visit relatives, friends or neighbors; (c) have friends or relatives for a dinner or a party; (d) go on day trips or overnight trips, and asking in the past 5 years, how many times they: (e) have visited a museum; (f) attended a concert, play, or a musical; (g) visited a library; (h) visited community centers. The eight items were scored using the same 4-point scale as above. The score for social activity ranged from 0 to 32. The overall social engagement level was assessed by summing up the scores of two subdomains and ranged from 0 to 65 points. The overall social engagement level and each subdomain level were then categorized into low, medium, and high level group using the tertile method.
Covariates
Sociodemographic and socioeconomic factors including age, gender, education, income, marital status, living arrangement (alone, with one person, with two-three persons, with ≥four persons), number of children, years in the United States, years in the community, country of origin, language preference (Cantonese, Toisanese, Mandarin, or English) and self-reported health status (poor, fair, good, very good) were controlled in the regression analyses.
Statistical Analysis Approach
Descriptive statistics were used to describe the average levels of social engagement and each subdomain among participants by cancer screening utilization. Differences were examined using t tests. Pearson correlations between social engagement and cancer screening utilization were measured. Then, a series of logistic regression analyses was performed to examine the associations between social engagement and cancer screening utilization. Model A was adjusted for age and gender. Model B was additionally adjusted for education and income. Marital status, living arrangement and number of children were further added into Model C. Based on Model C, years in the United States, years in the community, country of origin and language preference were added to Model D. Self-reported health status was additionally controlled in the final model (Model E). In all the above models, the odds ratios (ORs) for cancer screening utilization and the corresponding 95% confidence intervals (CIs) and significance levels were reported in each model in which social engagement and its subdomains were treated as continuous variables or tertiles, respectively. The “low level” group was used as a reference group. All statistical analyses were conducted using SAS, Version 9.2 (SAS Institute Inc., Cary, NC).
Results
Of the 3,157 participants in this study, the mean age was 72.8 years (SD = 8.3), and 58.9% were female. About 78.9% had equal or less than a high school education. About 85.1% had an annual income less than US$10,000. About 95% reported that they could not read or speak English. Table 1 shows the average levels of social engagement and each subdomain among cancer screening attenders and nonattenders. The levels of social engagement among cancer screening attenders were significantly higher than the levels among nonattenders. Similar significances were observed in cognitive activity and social activity. Table 2 presents the correlations between social engagement and cancer screening utilization. The data indicated that social engagement was positively correlated with all the five cancer-screening utilizations. Similar correlations were observed in both cognitive activity and social activity.
Social Engagement Characteristics by Cancer Screening.

Note. PSA = prostate specific antigen.
p < .05. **p < .01. ***p < .001.
Correlation Between Social Engagement and Cancer Screening Utilization.
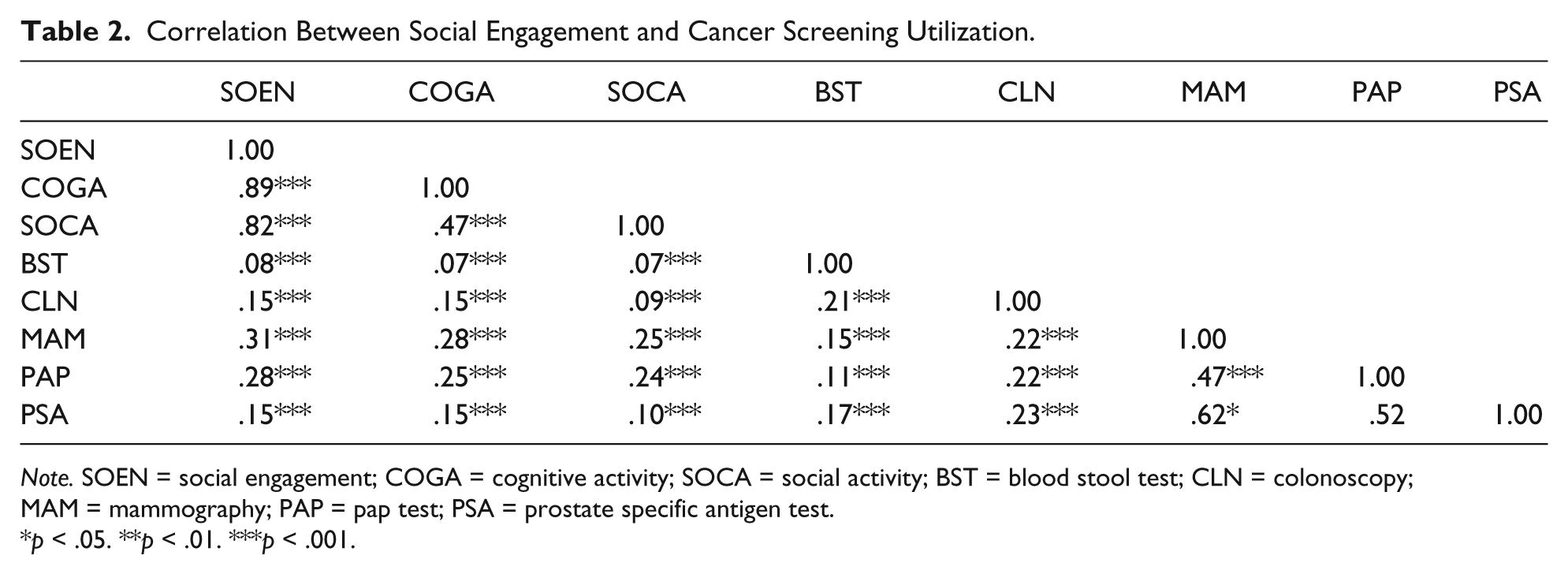
Note. SOEN = social engagement; COGA = cognitive activity; SOCA = social activity; BST = blood stool test; CLN = colonoscopy; MAM = mammography; PAP = pap test; PSA = prostate specific antigen test.
p < .05. **p < .01. ***p < .001.
Table 3 shows the associations between social engagement continuous level and cancer screening utilization. After controlling for confounders, a higher level of social engagement was associated with increased utilization in blood stool test (odds ratio [OR] 1.03, [1.02, 1.05]), colonoscopy (OR 1.02, [1.01, 1.03]), mammography (OR 1.06, [1.05, 1.08]), Pap test (OR 1.04, [1.03, 1.06]), and PSA test (OR 1.03, [1.01, 1.05]).
Associations Between Social Engagement (Continuous) and Cancer Screening Utilization.

Note. Models: A: adjusted for age and gender; B = adjusted for A + education and income; C = adjusted for B + marital status, living arrangement and number of Children; D = adjusted for C + years in the United States, years in the community, born in China and language preference; E = adjusted for D + self-reported health status; OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Table 4 summarized the associations between the tertiles of social engagement and cancer screening utilization. Compared with those with low levels of social engagement, older adults with high levels of social engagement were more likely to have utilized a blood stool test (OR 1.85, [1.46, 2.35]), a colonoscopy (OR 1.37, [1.09, 1.72]), a mammography (OR 3.05, [2.25, 4.14]), and a Pap test (OR 1.99, [1.49, 2.66]), but not significantly to have utilized a PSA test (OR 1.40, [0.97, 2.03]).
Associations Between Social Engagement (Tertiles) and Cancer Screening Utilization.

Note. Models: A: adjusted for age and gender; B = adjusted for A + education and income; C = adjusted for B + marital status, living arrangement and number of Children; D = adjusted for C + years in the United States, years in the community, born in China and language preference; E = adjusted for D + self-reported health status; OR = odds ratio; CI = confidence interval.
Significance levels: *p < .05. **p < .01. ***p < .001.
Table 5 presents the associations between social engagement subdomains and cancer screening utilization. In the fully adjusted model (Model E), a higher level of cognitive activity was associated with increased utilization in blood stool test (OR 1.04, [1.02, 1.06]), colonoscopy (OR 1.03, [1.02, 1.05]), mammography (OR 1.08, [1.06, 1.11]), Pap test (OR 1.05, [1.03, 1.08]), and PSA test (OR 1.04, [1.01, 1.07]). Similarly, a higher level of social activity was associated with increased utilization in blood stool test (OR 1.05, [1.03, 1.07]), colonoscopy (OR 1.03, [1.01, 1.05]), mammography (OR 1.08, [1.06, 1.11]), Pap test (OR 1.05, [1.03, 1.08]), and PSA test (OR 1.04, [1.01, 1.07]). Older adults with high levels of cognitive activity were more likely to have utilized a blood stool test (OR 1.81, [1.41, 2.32]), a colonoscopy (OR 1.52, [1.19, 1.93]), a mammography (OR 2.62, [1.92, 3.57]), a Pap test (OR 1.71, [1.27, 2.31]), and a PSA test (OR 1.58, [1.03, 2.43]) as compared with those with low-level counterparts. By contrast, compared with those with low levels of social activity, older adults with high levels of social activity were more likely to have utilized a blood stool test (OR 1.66, [1.33, 2.07]), a mammography (OR 1.93, [1.47, 2.54]), a Pap test (OR 1.72, [1.32, 2.26]), and a PSA test (OR 1.57, [1.12, 2.21]), but not more likely to have utilized a colonoscopy (OR 1.23, [0.96, 1.43]).
Associations Between Social Engagement Subdomains and Cancer Screening Utilization.
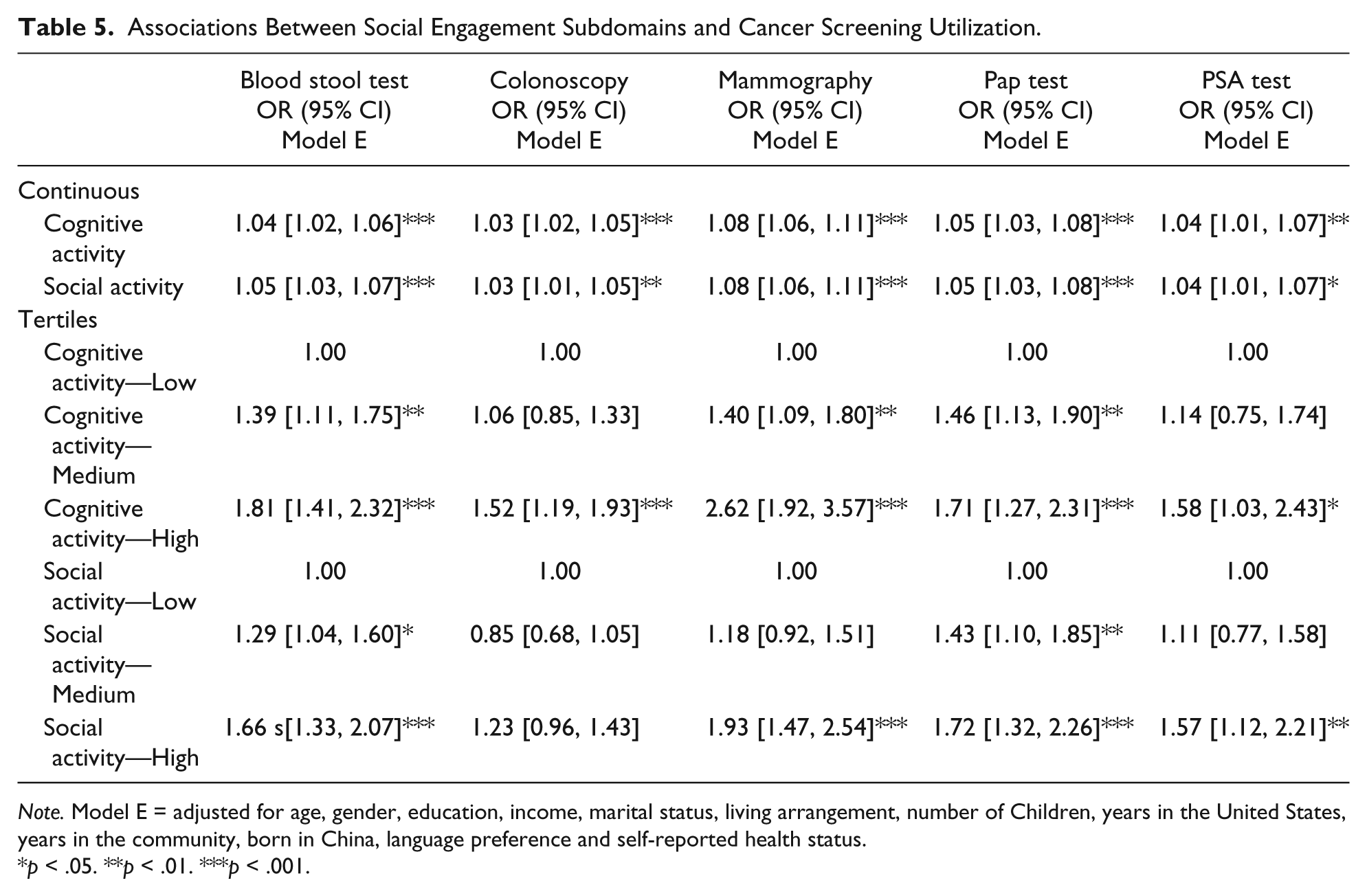
Note. Model E = adjusted for age, gender, education, income, marital status, living arrangement, number of Children, years in the United States, years in the community, born in China, language preference and self-reported health status.
p < .05. **p < .01. ***p < .001.
Discussion
Our study suggests that higher levels of social engagement are associated with increased utilization of cancer screening among Chinese older adults in the Greater Chicago area. Compared with those with low levels of social engagement, older adults with high levels of social engagement were significantly more likely to utilize cancer screenings. This study provides advanced knowledge for understanding the relationship between social engagement and cancer screening behavior in a Chinese American older population.
Social Engagement Level and Cancer Screening Utilization
In this study, we found that older adults reporting cancer screening utilization presented significantly higher level of social engagement than those reporting no utilization. The significant differences suggested that older adults who had attended cancer screening were more likely to engage in cognitive and social activities in their daily life. We also found that social engagement was positively associated with each cancer screening.
Meanwhile, our data indicated that higher levels of social engagement were associated with increased utilization of all the five cancer screening examinations. The results are consistent with prior study’s findings for colon cancer screening among Black and White Americans (Kinney et al., 2005). Furthermore, our findings showed that Chinese older adults with high levels of social engagement were more likely to have utilized a blood stool test, colonoscopy, mammography, and Pap test as compared with those with low levels, but not more likely to have utilized a PSA test. This finding suggested that low level of social engagement may be a risk factor for cancer screening utilization. In fact, our prior study reveals that a relatively low level of social engagement persisted in this population (Dong et al., 2014). Therefore, enhancing social engagement may benefit cancer-screening promotion in this population.
In the present study, no significant association was observed between the tertiles of overall social engagement and PSA test utilization. However, interestingly, significant associations were found between the tertiles of each subdomain and PSA test utilization. Why were these significances canceled out after combining the two subdomains? One possible explanation is that variances may be potentially amplified after the combination. Another possibility may be due to the relatively smaller sample size of the PSA test group (349 cases). Future research is needed to verify this observation.
Social engagement has been reported to promote positive health outcomes, probably by providing a greater sense of purpose, control, and self-efficacy and enhancing resilience in older adults (Mendes de Leon, Glass, & Berkman, 2003). Given this potential mechanism, our findings could be explained that high levels of social engagement may improve individuals’ cancer screening awareness and enhance the desire to seek preventive tools to promote their health and quality of life.
Social Engagement Pattern and Cancer Screening Utilization
Social engagement patterns may differ between different populations due to their diverse sociodemographic and socioeconomic characteristics and cultural diversity (Dong et al., 2014). In the current study, by clustering social engagement into two subdomains, we compared the differences in association between each subdomain and cancer screening utilization. We found that both higher levels of cognitive activity and social activity were significantly associated with higher likelihood of cancer screening utilization. Moreover, Chinese older adults with high levels of cognitive activity or social activity were both more likely to utilize a blood stool test, mammography, Pap test, and PSA test as compared with those with low-level groups. However, the associations between the two subdomains and colonoscopy utilization were different. Unlike cognitive activity, a high level of social activity did not show a significant association with increased colonoscopy utilization. The reason is probably that colonoscopy is recognized as an invasive procedure that involves anxiety and discomfort, along with the risk of complications (Ussui et al., 2013). Therefore, for older adults, promoting colonoscopy participation may require more intense cognitive activities to help them better understand the colonoscopy examination, strengthen their confidence, and thus allow them to conquer their fears and anxieties.
Covariates and Cancer Screening Utilization
Overall, after adding covariates into the full model, the associations between social engagement and cancer screening utilization remained significant. Our prior studies indicate that Chinese older adults still have low levels of health literacy and acculturation, (Dong, Bergren, & Chang, 2015a; Simon, Li, & Dong, 2014a). In this study, we found that a language preference for Chinese was associated with decreased cancer screening utilization. The result is consistent with prior study (Liang et al., 2009). We also found that better self-reported health status was associated with increased cancer screening utilization. It is in line with prior study, which demonstrates self-reported health status to be a prospective predictor of cancer screening uptake (Neter, Stein, Rennert, & Hagoel, 2016).
Limitations
This study has several limitations. First, the analysis was cross-sectional. Future longitudinal studies are required to investigate the temporal relations within this specific population. Second, all variables in this study were based on the self-report method, which could introduce the possibility of bias. Third, other cultural factors, such as a preference for traditional Chinese medicine, may influence cancer screening. These potential factors will be considered in the future studies. Fourth, for the social engagement measurement, we mainly focused on cognitive activity and social activity participation, which may have narrowed the scope of social engagement assessment. Future studies may incorporate productive activity to social engagement assessment.
Implications
Despite these limitations, this study has notable strengths. As the first epidemiological study to explore the association between social engagement and cancer screening utilization, our findings contributed to the understanding of the potential facilitating effect of social engagement on cancer screening utilization. This study has important practical implications for researchers, health care providers, and policy-makers.
This study synthesized new evidence that social engagement is associated with cancer screening utilization among Chinese American older population. These findings may lead to speculation that future cancer screening promotion outreach programs would gear toward older adults with low levels of social engagement. Furthermore, addressing various barriers in combination may be the best way to facilitate cancer screening utilization. For health care providers, these findings may provide in-depth evidence to support clinical professionals facilitating cancer-screening services such as building up community partnership education programs (Ragas et al., 2014). This study would present new thoughts to policy-makers in formulating relevant policies in cancer screening among Chinese American population.
Conclusion
In summary, this study found active social engagement was associated with increased cancer screening utilization among Chinese American older adults in the Greater Chicago area. Older adults with high levels of social engagement were more likely to have utilized cancer screening. Improving social engagement could be helpful in promoting cancer screening utilization. However, future longitudinal studies are needed to better explain the temporary associations found in this study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.