
Abstract
Older adults who live in long-term care settings are at risk for functional decline, which may be mitigated by regular exercise. Using a single-group repeated measures design, this pilot study explored the feasibility, acceptability, and preliminary effects of a Waltz-based dance intervention delivered to 13 Canadian, English-speaking, long-term care residents with mild to moderate cognitive impairment. The findings supported intervention feasibility, based on a high completion rate (93%), level of attendance (M = 7.15 of 10 sessions) and level of engagement during dance sessions (M = 1.75 to 1.97 out of 2.00). On average, residents perceived dance sessions positively, and staff and family participants (N = 26) rated them as somewhat acceptable overall (M = 2.37, 0 to 4 scale). Additional research is needed to assess intervention efficacy in a larger sample.
Dance, defined as rhythmic physical movement to music (Jain & Brown, 2001; Lapum & Bar, 2016), is an exercise that can promote health for long-term care (LTC) residents with cognitive impairment (CI). Evidence supports that dance interventions may improve (a) physical functions like balance and motor skills in older adults (Abreu & Hartley, 2013; Krampe et al., 2010), mobility in LTC residents (Guzmán-García, Hughes, James, & Rochester, 2013), and self-care in people with CI (Hokkanen et al., 2008); (b) cognitive function for people with traumatic brain injury or stroke (Berrol, Ooi, & Katz, 1997), LTC residents with dementia (Hokkanen et al., 2008), and older people with CI (Adam, Ramli, & Shahar, 2016); (c) psychological function of LTC residents with CI, including fewer responsive behaviors (e.g., aggression) and more happiness (Guzmán-García et al., 2013), improved life satisfaction (Kim, June, & Song, 2003), and lower levels of anxiety and depression (Adam et al., 2016); and (d) social function, specifically sharing a familiar and enjoyable activity with others (Jain & Brown, 2001) and increased feelings of connection to others (Olvera, 2008). To achieve these positive effects, participants need to be motivated to engage fully in the intervention activities (Sidani & Braden, 2011).
People may be more motivated to participate in a dance that includes familiar steps and music (Adam et al., 2016; Lukach et al., 2016; Shanahan et al., 2015). Familiar repetitive movement and music can also cue people with CI to be physically active (Earhart, 2009; Lapum & Bar, 2016). The effects of interventions that use familiar music and steps, matched to participants’ social, historical, or cultural backgrounds and modified to meet their abilities, have been studied and include Salsa dance (Abreu & Hartley, 2013), African dance (Lukach et al., 2016), Malaysian poco-poco dance (Adam et al., 2016), Irish set dance (Shanahan et al., 2015), the Tango (Hackney et al., 2015), and dance-based movement to traditional Korean music (Kim et al., 2003).
However, there are limitations to tailoring dance interventions according to a group’s shared background characteristics. Countries that may appear culturally homogeneous to an outsider are, upon a deeper examination, characterized by much ethnic and cultural diversity (Fearon, 2003). Therefore, tailoring dance interventions to participants’ cultural background based on country of origin does not guarantee that participants will find sessions familiar, enjoyable, or acceptable, which affects level of engagement in the activity and ability of the intervention to affect health outcomes (Sidani & Braden, 2011). There is limited evidence of the feasibility and acceptability of dance interventions tailored to align with participants’ cultural background. This pilot study explored the feasibility and acceptability of a dance intervention tailored to the background characteristics (i.e., age, cultural background, and language spoken) of a group of residents with CI in a multicultural Canadian LTC setting.
Study Aims
The pilot study assessed feasibility based on consent rates, attendance rates, level of resident engagement during sessions, and rates and reasons for missing outcome data (i.e., measures of resident physical, cognitive, psychological, and social functions). Acceptability was assessed using LTC staff and resident self-report.
Method
Design
A one group with repeated measure design was used. Dance sessions were offered to groups of residents from four units of an Ontario LTC facility. Feasibility and resident acceptability data were collected at the end of every dance session, to enable recall. Staff acceptability data were collected 1 week post-intervention, to ensure familiarity with the intervention. Outcome data were obtained 1 week pre-intervention, at week 3, and 1 week post-intervention.
Intervention
The most prevalent cultural group at the participating site was Caucasian, English speaking, Canadian residents. Three consultants, who had previous experience leading dance classes for older adults and people with disabilities, helped to select the dance type (Waltz) and music (e.g., Blue Danube, Silver, and Gold Waltz) that may be familiar to this cultural group and to simplify the dance steps to fit the residents’ abilities.
Two outgoing female interventionists led each session. One had a dance background and was trained in strategies to communicate with people with CI, and the other was a PhD-prepared registered nurse experienced in the care of people with CI. Twice weekly, 30-min sessions were offered for 5 weeks to small (n = 4-5) groups of residents. The dose and group size were feasible, safe, and promising to improve LTC residents’ functions in previous research (Guzmán-García et al., 2013; Krampe et al., 2010). Each session comprised (a) a warm up of light stretching and unstructured movement to an upbeat song; (b) instructions and cueing to complete the dance steps; (c) practice of dance steps to music; and (d) a cool down of light stretching to a calming song. At each session, participants were taught the steps and cued to use their mobility aides. New dance steps and music were added as needed to maintain the participants’ interest. Participants were encouraged to stand but could sit if fatigued.
Sample
Eligible residents were identified based on their clinical Resident Assessment Instrument Minimum Data Set (RAI MDS) Version 2.0 data and were 65 or older, lived at the LTC facility for ≥3 weeks, walked independently or with a mobility aide (e.g., walker), understood English (required to follow dance instructions and complete measures), and had a Cognitive Performance Score of ≤3 suggesting mild-to-moderate impairment. The Cognitive Performance Scale (CPS) is based on comatose status, decision-making ability, short-term memory, making oneself understand, and eating and can range from 0 (may have mild cognitive impairment) to 6 (severely impaired) (Morris et al., 1994). Direct care staff who worked on units where participating residents lived (employed by the facility or privately paid), and family/friends who attended at least one session, were eligible to rate the acceptability of the dance intervention.
Recruitment
Two LTC staff reviewed clinical RAI 2.0 data to identify eligible residents and, at their discretion, contacted either the resident or the power of attorney (POA) to ascertain interest in the study. The researcher followed up with those interested to obtain consent. Staff and family/friends were recruited by word of mouth and with an invitation letter, placed in meeting and consenting residents’ rooms.
Measures
Feasibility
A participant log was used to track recruitment, dance session attendance, outcome measure completion, and residents’ reasons for nonenrollment, nonattendance, and study withdrawal. A checklist based on the intervention protocol was used to document residents’ level of engagement in the sessions.
Acceptability
Staff and family/friends read a description of the intervention and then rated its effectiveness, logic, suitability, risk, ease of use, and overall acceptability. Items were adapted from the Treatment Perception and Preference (TPP) Measure (α > .85; Sidani, Epstein, Fox, & Miranda, 2016) resulting in six items presented in a response-tree format (Fox, Sidani, Streiner, McGilton, & Grady, 2011) about whether they enjoyed the session, felt better, and thought the dance session helped them (α = 0.75 at baseline). Items were informed by the TPP but simplified for use with people with CI.
Resident outcomes
Reliable, valid measures for use with older adults with CI were used to assess functional mobility (Timed Up and Go [TUG; Christofoletti et al., 2008 and 2-Minute Walk Test [2MWT; Bernstein, Despars, & Singh, 1994]); CI (Mini Mental Status Examination [MMSE; Folstein, Folstein, & McHugh, 1975]); psychological function (subscales of self-esteem, pleasure from surroundings, positive and negative impact, and an overall quality of life item [Dementia Quality of Life; DQOL; Brod, Stewart, Sands, & Walton, 1999]); and social function (3-Item Loneliness Scale [Hughes, Waite, Hawkley, & Cacioppo, 2004] and the DQOL belonging subscale [Brod et al., 1999]).
Analysis
Statistical Package for the Social Sciences (version 22.0) was used. Frequency, central tendency, and dispersion were calculated to assess feasibility and acceptability.
Ethics
The researchers obtained written, informed consent from residents or their POAs, staff, and family/friends. Resident’s verbal assent was also obtained at each dance session. The Research Ethics Board at (Ryerson University; institutional review board [IRB] protocol 2015-208) approved this study.
Results
Enrollment and Attrition Rates
Of 20 residents who were eligible and agreed to be contacted by a researcher, 14 consented to participate (70% enrollment rate), and 13 completed the study (93% completion rate). One participant, whose POA was enthusiastic about the study, declined to participate in baseline data collection and three consecutive dance sessions, withdrew from the study (7% attrition rate; Figure 1). Twenty-five staff and one family member rated acceptability.
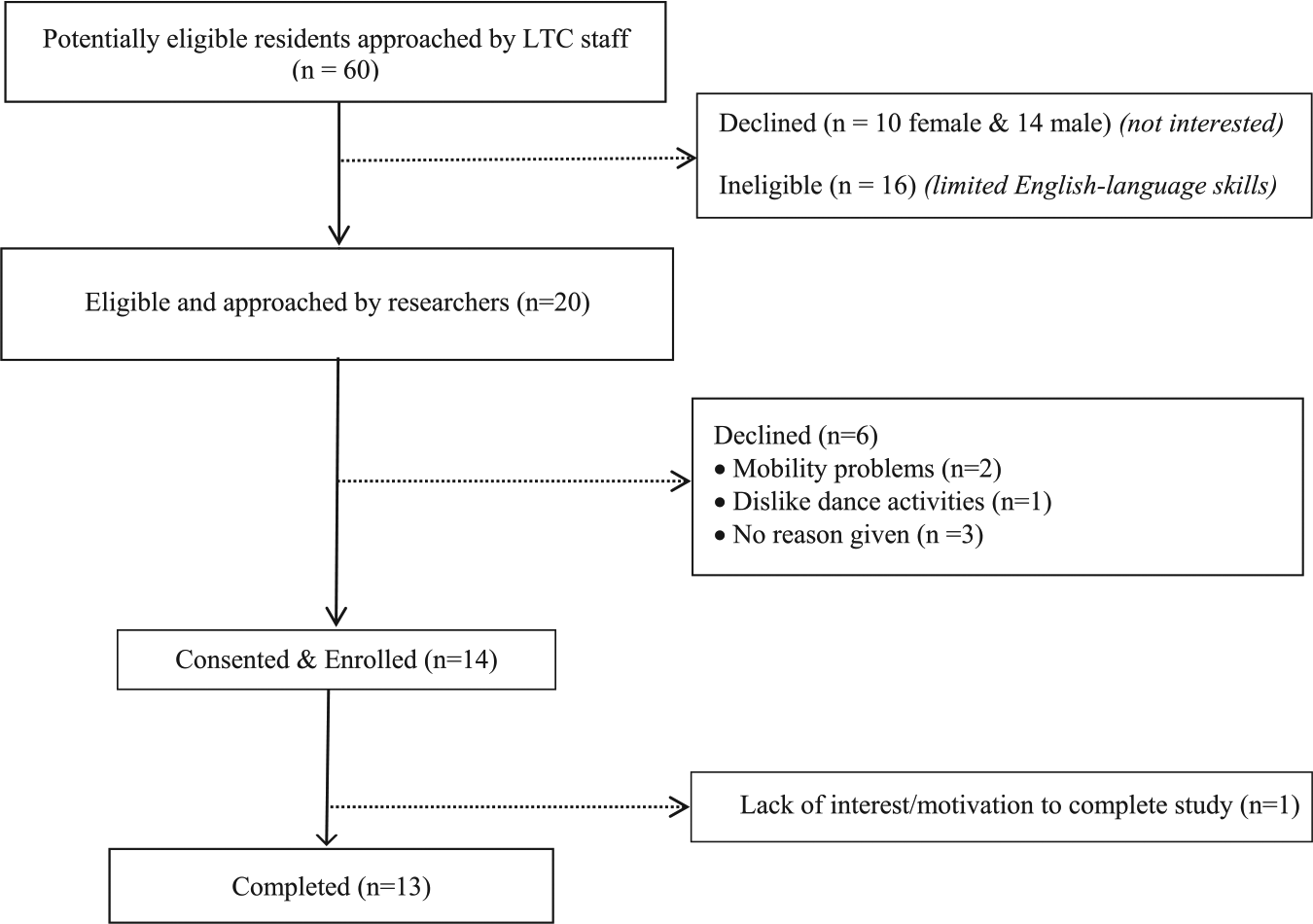
Flowchart of participant enrollment.
Participant Characteristics
On average, residents were 90 years old (range = 71-102), mostly women (68.8%), who identified as Canadian (69.2%), had moderate CI (53.8%), and rated their psychological function above the scale midpoints at baseline (Table 1). Staff had an average age of 40 (range = 24-60); most of them were women (80.8%) and health care aides (38.5%; Table 1). The family member was a woman, aged 70 years.
Demographic Profile of Residents (N = 13) and Staff (n = 25) and Resident Outcomes at Baseline.

Note. MMSE = Mini Mental State Examination.
Cognitive function based on MMSE scores, categorized as intact (MMSE 26-30) or impaired to a mild (MMSE = 21-25), moderate (MMSE = 11-20) or severe (MMSE ≤10) degree.
The category “other” included staff from life enhancement (i.e., staff who support residents’ activity engagement; n = 5), restorative care (n = 1), volunteer services (n = 1), and a registered practical nursing student (n = 1); social worker (n = 1); and privately paid health care aide (n = 1).
Sample sizes vary due to missing data.
The response-tree strategy was applied as follows: first, older adults were asked whether they experienced each of the feelings described (yes or no), if yes, then the frequency was ascertained (1 = hardly ever, 2 = some of the time, or 3 = often). “No” and “hardly ever” were both coded as a 1 to maintain the original response scale.
Attendance and Engagement
Residents attended an average of seven of 10 sessions, and the participation rates for each session ranged from 62% to 92% (Table 2). At least 50% of participants used a four-wheeled walker in nine of 10 sessions (Table 2). Overall mean engagement ranged from 1.75 to 1.97 (of 2.00) over the 10 sessions (Figure 2); engagement was lower for the cool down (M range = 1.42-1.88) as compared with the warm up (range = 1.60-2.00), instruction without music (range = 1.62-2.00), and practice with music (range = 1.50-2.00). One family member and two staff attended one session for 20 min; a privately paid caregiver participated in 10 full sessions.
Participation Rate and Proportion of Mobility Aide Use of Residents (N = 13) Across 10 Dance Sessions.

Mobility aide used was a four-wheeled walker.

Resident level of engagement in dance sessions.
Acceptability
Residents rated the acceptability of the dance sessions above the scale midpoint of 1.5, and ratings ranged from 1.83 to 2.33 across sessions (Figure 3). Residents found the sessions enjoyable (range = 2.05-2.42), helpful (range = 1.55-2.57), and reported feeling better after the sessions (range = 1.45-2.25). Staff (n = 25) and family (n = 1) rated the intervention as somewhat acceptable overall (M = 2.37), effective (item mean >2.50), appropriate (item mean >2.50), low risk (M = 0.50), and somewhat convenient (item Ms = 1.28-2.48; 0 to 4 scale; Table 3).

Resident acceptability by dance session.
Staff and Family Acceptability of Dance Intervention (N = 26).

Note. CI = cognitive impairment.
Feasibility of Outcome Measures
Missing data at each time point were observed primarily for the physical function tests (8% to 23% missing) and the DQOL, especially the belonging subscale (8%-31% missing). The DQOL data could not be completed with residents who had a MMSE ≤12, and tired or sick residents declined to complete physical assessments.
Discussion
The dance intervention, tailored to English-speaking Canadians, was feasible in the LTC context. Residents and staff rated the dance sessions positively, supporting the acceptability of this intervention. Further research is warranted to test its efficacy in promoting resident functions in larger samples (Leon, Davis, & Kraemer, 2012). As functional decline is common for many subgroups of LTC residents (e.g., over 80, the cognitively impaired; Payette et al., 2011), maintenance of function should also be considered as a potential desirable outcome in future research (Doran, 2011). At least 246 people would be needed for a randomized study with two groups (i.e., 123 per group) to detect a small, statistically significant effect (80% power, Cohen’s d = 0.2 [Sullivan & Feinn, 2012], alpha = 0.05).
This dance intervention was implemented in a small group format; such interventions are often conceptualized as being inherently social in nature (Guzmán-García et al., 2013). However, research suggests that simply offering an activity in a group setting is insufficient to impact loneliness. Studies of other group-based activities, given to older adults over weeks or years, have been unable to demonstrate any statistically or clinically significant impact on loneliness (Baker & Ballantyne, 2013; Brown, Allen, Dwozan, Mercer, & Warren, 2004; Cohen, 2006; Cohen et al., 2006; Cohen-Mansfield et al., 2007; Pitkala, Routasalo, Kautiainen, & Tilvis, 2009; Routasalo, Tilvis, Kautiainen, & Pitkala, 2009; Savikko, Routasalo, Tilvis, & Pitkälä, 2010). New components that are aimed at determinants of loneliness (e.g., facilitation techniques to support friendship development) could be added to this dance intervention to augment impact of the dance intervention on social function (O’Rourke & Sidani, 2017).
It was unsurprising that very few staff, family, or friends attended the dance sessions. LTC home staff often lack the time to participate in intervention research (Kaasalainen et al., 2010) and, while the majority of LTC residents receive regular visits from family and friends who may provide instrumental support, little is known about how to integrate family and friends into other aspects of residents’ lives (Gaugler, 2005). Future research could explore strategies to encourage staff, family, and friends to join residents’ group activities.
Resident recruitment was challenging. Eligible residents were not always interested in the dance intervention or were less enthusiastic about the study than the POAs who consented on their behalf. Scheduling conflicts prevented some residents from attending the dance sessions. Multiple study sites should be used in future efficacy research to accrue a larger, more generalizable sample.
To reduce participant burden, clinical administrative RAI data could be used in future research in lieu of some measures. For example, the RAI 2.0 contains valid and reliable measures of physical function (Morris, Fries, & Morris, 1999) and psychological well-being (e.g., anxiety; Morris et al., 2010). The Preferences for Everyday Living Inventory, which may be included in newer versions of the RAI, includes questions about preferences for music and favorite activities and may assist in identifying people who would benefit most from the intervention (Curyto, Van Haitsma, & Towsley, 2016). Since RAI data collection occurs every 3 months (Morris et al., 2010), the intervention time frame may need to be adjusted (e.g., extended over several months) in a study that used RAI outcome data. Most missing data occurred in this study for residents who were tired or sick, so future efficacy research should consider fatigue and illness as possible effect modifiers.
Limitations
Many residents were excluded because they did not speak and understand English, highlighting the importance of developing dance interventions for use with people from other cultural backgrounds who live in multicultural settings. Findings from one LTC facility may not be generalizable, and future efficacy studies should include an embedded pilot to work out logistical issues.
Conclusion
These pilot findings support the feasibility and acceptability of a tailored dance intervention that used music and steps familiar to LTC residents who identified as “Canadian” and spoke English. The intervention is promising and warrants further research to determine its efficacy in a larger sample.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Gerontological Nursing Association (CGNA Research Grant Competition 2014). The first author was supported by a Postdoctoral Fellowship from the Canadian Institutes of Health Research.