
Abstract
Background
Social isolation is a public health concern (Holt-Lunstad et al., 2010; Steptoe et al., 2013). Risk of mortality associated with diminished social connection is greater than those associated with obesity, physical inactivity, and smoking 15 cigarettes per day (Holt-Lunstad et al., 2015). Although no single definition exists, social isolation refers to an objective state of having few social contacts (family/friends) or infrequent contact with others (Victor et al., 2008). Research aimed at quantifying social isolation often measures the size and composition of an individual’s social network including number of contacts, living arrangements, and frequency of participation in social activities (Dickens et al., 2011; Dury, 2014). It is related to, but distinct from loneliness, the subjective feelings from a discrepancy between desired and actual social connections (Cacioppo et al., 2015; Ong et al., 2016; Perissinotto & Covinsky, 2014).
Causes of social isolation are multifactorial and include socio demographics (older age, less education, lower income), changes in work (retirement) and family roles (caregiving), and environmental (living alone, safety of living situation, geographic area) (Nicholson, 2012). Older adults (65+) are at heightened risk of social isolation because of age-related changes in their social networks (e.g., widowhood, retirement), relocation, and physical changes, which can impede their ability to participate socially (Grundy, 2006; Nicholson, 2012). Social isolation is a particular challenge for older adults because it reflects a limited reserve of support to draw on when in need (Machielse, 2015).
Although the health implications of social isolation are well established, research often focuses solely on community-dwelling older adults and excludes those living in congregate settings, such as long-term care (LTC) homes (i.e., nursing homes, personal care homes) (Valtorta et al., 2018). Systematically conducted literature reviews aimed to identify interventions to address social connection in older adults have found that most studies focused on community-dwelling populations rather than older adults in LTC homes (O’Rourke et al., 2018; Quan et al., 2019). Research on social isolation in LTC homes is critical because of the unique congregate setting and population characteristics. LTC homes provide 24-hour nursing care, personal care, recreation programming, and a physical environment that can include communal dining, living and activity space, and often shared bedrooms. Residents in LTC settings are often older (over age 85), have a dementia, and multiple chronic conditions (Canadian Institutes of Health Information, 2018; Hoben et al., 2019). Reasons for the lack of research on social isolation in LTC settings may include the perception that individuals in care settings—who are surrounded by staff and other residents—are objectively less isolated and therefore the effects of isolation less of a concern (Victor, 2012). However, while social and recreational programming exist in LTC homes, there is mixed evidence about the effectiveness of these activities to reduce social isolation and loneliness (Theurer et al., 2015; Victor, 2012). LTC residents still rely on family and friends for support even after they move to a LTC home (Barken et al., 2017; Baumbusch & Phinney, 2014; Gaugler, 2005; Williams et al., 2012). Family can provide critical hands-on support with direct care (feeding, dressing), advocacy and monitoring, and psychosocial support. Yet, we know that not all residents have external social support, and little is known about the health and well-being of socially isolated LTC residents (Chamberlain et al., 2018).
Identifying social isolation in LTC homes is crucial to determining its influence on health and quality of life. We lack a clear and robust evidence base with which to identify and assess social outcomes in health data in general and LTC specifically (National Academies of Sciences & Medicine, 2020; Perissinotto et al., 2019; Quan et al., 2019). Although numerous interventions have been developed to reduce social isolation and the related concept of loneliness (e.g., social contact interventions, reminiscence therapy), we need ongoing monitoring in health data to assess the effectiveness of these interventions (O’Rourke et al., 2018). Introducing additional assessments is particularly challenging in LTC settings where direct care staff have limited resources (time, training) to undertake new assessments. Therefore, using items in existing, routinely collected instruments may be an effective and efficient way to assess social isolation and its outcomes in LTC settings without adding new documentation. This study used data from the Resident Assessment Instrument-Minimum Data Set 2.0 (RAI-MDS) to identify socially isolated LTC residents. The purpose of this descriptive study was to examine the prevalence, characteristics, health conditions, and functional status of socially isolated LTC residents and to compare these characteristics and health conditions to residents who are not socially isolated.
Methods
Design
This study is a retrospective, cross-sectional cohort study that assessed the demographic characteristics, clinical and functional status, and disease diagnoses of socially isolated LTC residents in Alberta, Canada. We conducted a secondary analysis of data collected using the RAI-MDS.
Data Source
The RAI-MDS is a comprehensive longitudinal assessment tool that collects information on clinical and functional status of residents in LTC homes (Poss et al., 2008). Its administration is mandated in most Canadian provinces. Assessments are completed by a staff member (typically a registered nurse) upon admission, every 3 months, and following a significant change in resident health status, and discharge. Assessments include information regarding resident demographics, physical functioning, cognition, hearing, vision, responsive behaviors, depression, disease diagnoses, medications, oral health, social engagement, mobility, and treatments. Outcome scales (e.g., social engagement, responsive behaviors, depression) are used to identify actual or potential resident needs and serve as a basis for resident care planning (Bedowitz et al., 1997).
Setting and Sample
We analyzed data from a sample of 34 LTC homes in Alberta, Canada. Our sample of LTC homes are from the Translating Research in Elder Care (TREC) program of research (2007–2022) (Chamberlain, Hoben, et al., 2019; Estabrooks et al., 2015; Estabrooks et al., 2013; Estabrooks et al., 2009). Since 2014, the TREC program has collected RAI-MDS data in a sample 34 nursing homes from Alberta. TREC facilities are a representative sample, stratified by region (Edmonton, Central, Calgary), facility owner-operator (private for profit, public not for profit, voluntary not for profit), and bed size (small [<80 beds], medium [80–120 beds], large [>120 beds]). We included residents from Alberta to enable comparisons with our larger provincial study examining the prevalence and unmet needs of unbefriended residents in LTC homes (Chamberlain, Duggleby, et al., 2019; Chamberlain, Duggleby, Teaster, & Estabrooks, 2020; Chamberlain, Duggleby, Teaster, Fast, et al., 2020).
We analyzed RAI-MDS data from April 1, 2008 to March 31, 2018. This timeline reflects the introduction of the RAI-MDS in Alberta LTC homes. This timeline resulted in a total of 199,337 assessments reflecting 26,102 unique individuals. From the available RAI-MDS data, we excluded residents who did not have the outcome variable of interest (Item F2e: no family contact) completed (n = 769) and who were discharged prior to completing an initial assessment (n = 3). This resulted in a total sample of 25, 330 residents. Quarterly assessments account for 64% of all the available RAI assessments, and our outcome of interest (no family contact) was only captured on the admission and annual assessment. Therefore, if the last/most recent assessment was a quarterly assessment, we carried forward the assessment details to the most recent assessment.
Measures
We classified residents as socially isolated if they had no personal contact with family or friends at the time of their RAI-MDS assessment. This item is available in the “Unsettled Relationships” scale, which asks assessors to indicate if in the last 7 days the item (absence of personal contact with family/friends) applies to that resident (Yes, No). We identified residents who were identified as ”Yes,” having had no contact with family or friends.
We reported on resident demographic characteristics including sex (male, female), age (years), and marital status (never married, married, widowed, separated, divorced, unknown). We estimated Length of resident stay, based on the date of admission and the date of last assessment, was collected as well as the following disease diagnoses or disorders: diabetes, heart disease, congestive heart failure, hypertension, arthritis, Alzheimer’s disease or other dementia, cerebrovascular accident, Parkinson’s disease, seizure disorder, traumatic brain injury, anxiety disorder, depression, bipolar disorder, schizophrenia, emphysema/chronic obstructive pulmonary disease, and liver disease. These diseases or disorders were chosen based on findings from relevant reviews of the literature on social isolation and older adults (Chamberlain et al., 2018; Chamberlain, Duggleby, Teaster, & Estabrooks, 2020; Holt-Lunstad et al., 2015; Nicholson, 2012).
We assessed resident clinical and functional status using outcome scales available in the RAI-MDS. The outcome scales assessed the following: cognitive performance, depression, activities of daily living, pain, aggressive behaviors, changes at the end of life, and social engagement. We assessed resident cognitive performance using the Cognitive Performance Scale (CPS) (Hartmaier et al., 1995), for which a higher score indicates severity of impairment. We examined resident depression using the Depression Rating Scale (DRS) (Burrows et al., 2000). Resident functional abilities were measured using the Activities of Daily Living Scale-Long Form (ADL) (Morris et al., 1999). A higher score indicates more impairment in ADL performance. The Pain Scale assessed resident pain (Fries et al., 2001). A Pain Scale score of two or greater indicates more frequent and intense pain. We examined resident aggressive behaviors using the Aggressive Behavior Scale (ABS). An ABS score of five or greater indicates more physical, verbal, and socially inappropriate behavior. We assessed social engagement using the Index of Social Engagement (ISE) scale (Mor et al., 1995). A higher score on the ISE indicates higher (better) social engagement.
Ethics
We received ethical approvals for this study from the University of Alberta Research Ethics Board (Pro00071410) and the Northern Alberta Clinical Trials Research (PB74409). We received approval for secondary analysis of the RAI-MDS data from the Translating Research in Elder Care (TREC) Data Management Committee.
Analysis
We analyzed the data using SAS 9.4 (SAS Institute, Inc., Cary, NC). Prevalence of socially isolated residents was calculated based on the total number of individuals identified in the RAI-MDS as having no contact with family or friends (socially isolated) and the total number of residents in the cohort (n = 25, 330). We calculated descriptive statistics were used for all items (mean, 95% Confidence Intervals [CI]). Statistical differences in the scale scores were determined using two-sample t-tests. For ordinal and dichotomous variables, we used 95% CI for proportions. We used binary logistic regression to assess differences between residents who were socially isolated (no contact with family or friends) and residents who were not socially isolated (contact with family or friends). Unadjusted and adjusted odds ratios (OR) can be found in Table 1. Odds ratios were adjusted for age (years) and sex (reference: female).
Odds Ratios for Residents with No Family Contact.
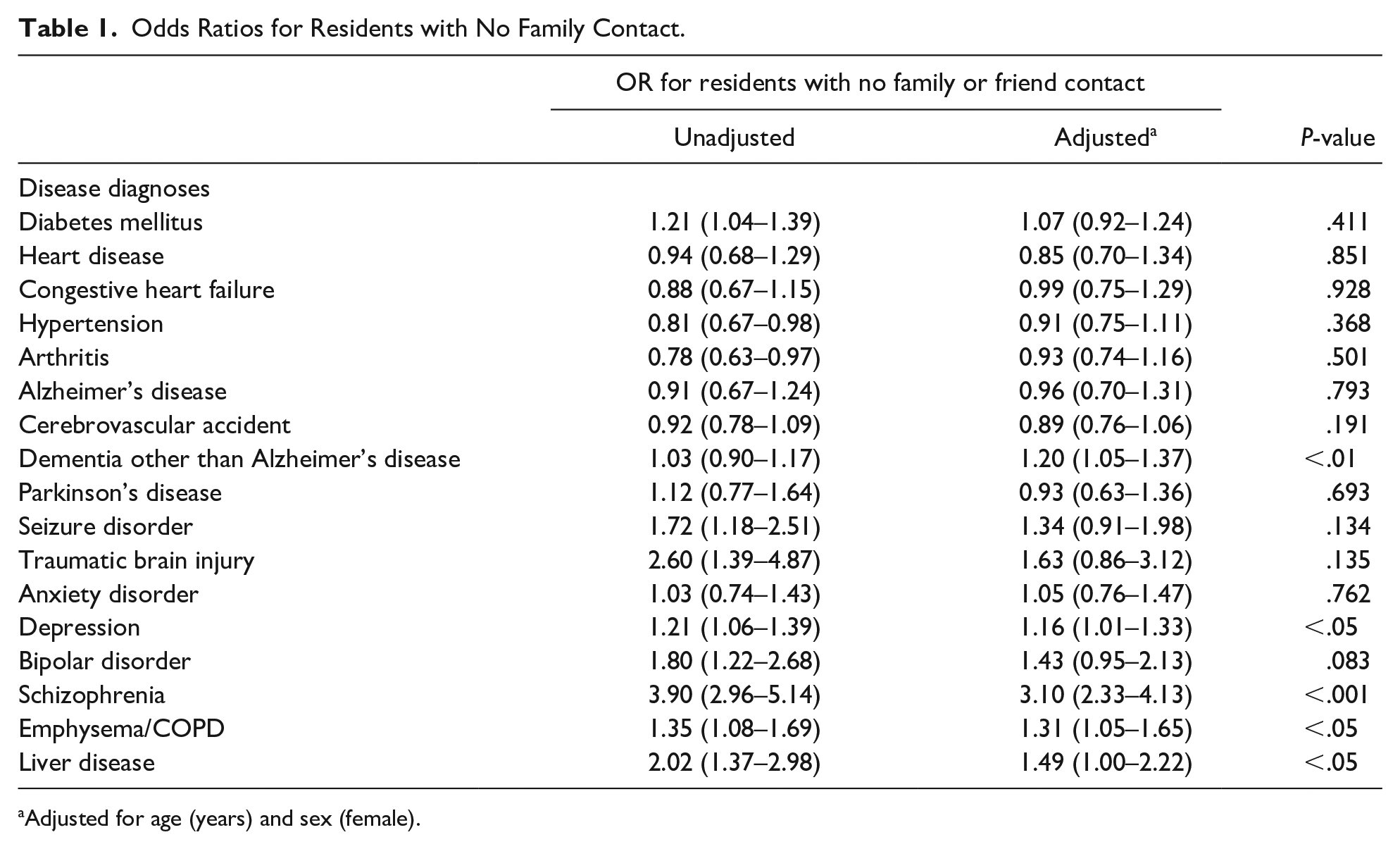
Adjusted for age (years) and sex (female).
Reporting standards in Canada for RAI-MDS data require residents to have completed assessments. Therefore, our final dataset did not include missing variables. More advanced statistical tests of association (e.g., multivariable regression) were not utilized because our intention was to describe these residents and provide a foundation for future research.
Results
The prevalence of socially isolated residents in our sample was nearly 4% (945/25330[3.73%]). Among socially isolated residents, there were proportionally more males (439/945 [47%]) compared to non-isolated residents (9494/24385 [39%]) (Table 2). Residents who were socially isolated were younger and had a longer length of stay in the LTC facility than did residents who were not socially isolated. We found statistically significant differences in the instances of mental health diagnoses, including a diagnosis of depression (adjusted OR: 1.16), and schizophrenia (adjusted OR: 3.10) in socially isolated individuals. Socially isolated residents had a higher likelihood of a dementia other than Alzheimer’s disease (adjusted OR: 1.20), emphysema/chronic obstructive pulmonary disease (COPD) (adjusted OR: 1.31), and liver disease (adjusted OR: 1.49).
Characteristics of Residents with and without Family or Friend Contact (April 1, 2008 to March 31, 2018).

Residents who were socially isolated had higher mean scores (higher is worse) on each of the depression rating scale, pain scale, and responsive behavior scale (Table 3), than residents who were not socially isolated. They had significantly lower scores on social engagement (lower is worse). We found no significant differences in cognitive performance.
RAI-MDS 2.0 Outcome Scales for Residents with and Without Family or Friend Contact (April 1, 2008 to March 31, 2018).
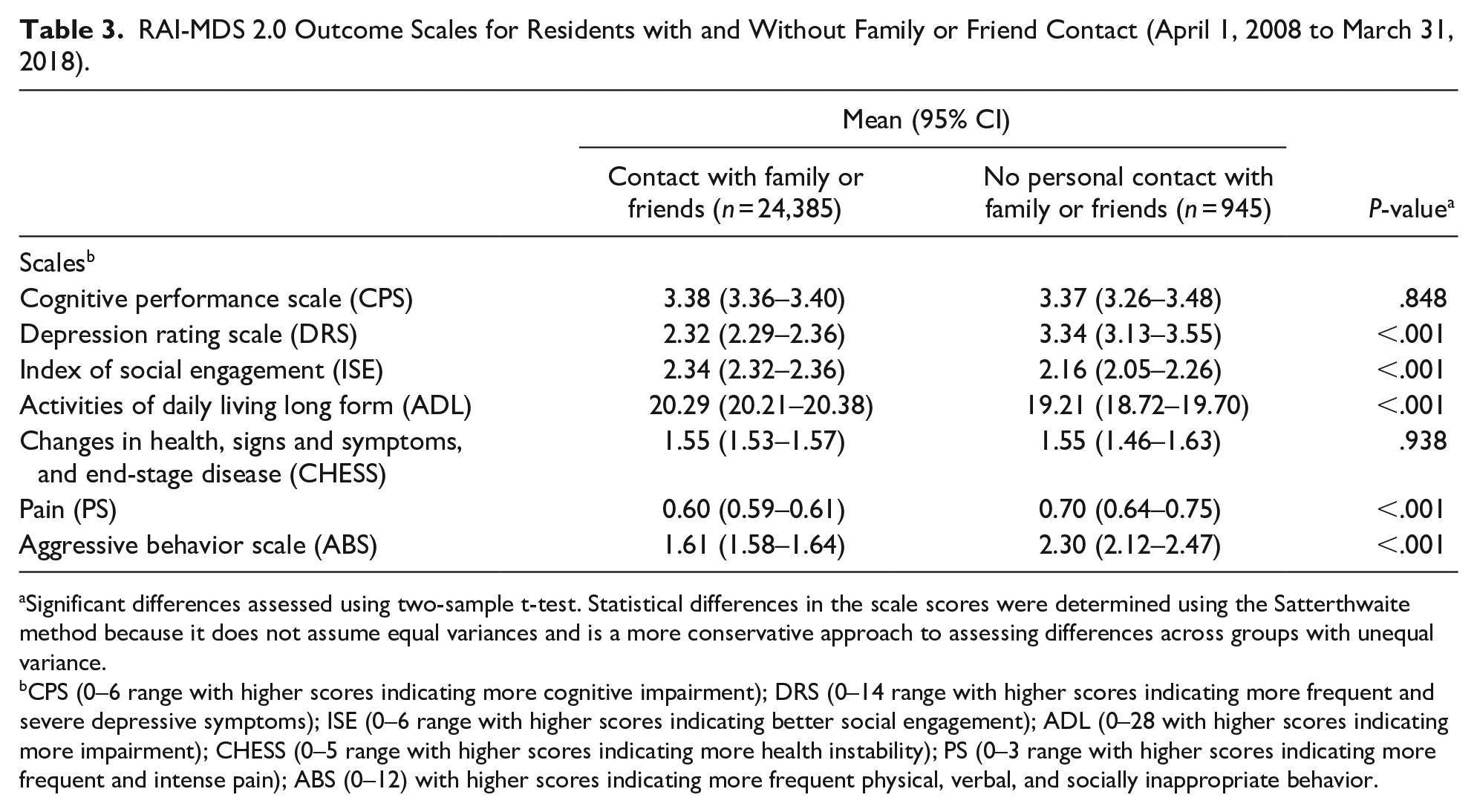
Significant differences assessed using two-sample t-test. Statistical differences in the scale scores were determined using the Satterthwaite method because it does not assume equal variances and is a more conservative approach to assessing differences across groups with unequal variance.
CPS (0–6 range with higher scores indicating more cognitive impairment); DRS (0–14 range with higher scores indicating more frequent and severe depressive symptoms); ISE (0–6 range with higher scores indicating better social engagement); ADL (0–28 with higher scores indicating more impairment); CHESS (0–5 range with higher scores indicating more health instability); PS (0–3 range with higher scores indicating more frequent and intense pain); ABS (0–12) with higher scores indicating more frequent physical, verbal, and socially inappropriate behavior.
Discussion
In this study, we found that socially isolated LTC residents, as defined by having no contact with family or friends on their most recent assessment, had worse functional abilities, more depressive symptoms, and lower social engagement than residents who were not socially isolated. We found the prevalence of social isolation was nearly 4% in our sample. This is comparable to the findings from a prevalence survey of LTC residents that found a little over 4% of residents in Alberta were unbefriended (without a family or friend guardian) (Chamberlain, Duggleby, et al., 2019). Data from the Canadian Longitudinal Study on Aging, a nationally representative survey revealed that the prevalence of social isolation was 5.1% in community-dwelling older adults (Menec et al., 2019). It is challenging to compare our prevalence to existing studies because social isolation has received little consistency in definition or measurement in the research literature (Keefe et al., 2006). Disparate definitions and study designs make it difficult to assess the comparability or quality of the available research (Health Quality Council of Ontario, 2008). However, our findings appear to be consistent with related research that has found that social isolation is associated with increased functional decline and depression (Holt-Lunstad et al., 2010; Neeleman & Power, 1994).
Research consistently demonstrates that LTC residents have unmet needs for intimate social relationships (Cadieux et al., 2013) and residents in LTC homes experience low levels of social engagement (Achterberg et al., 2003; Bliss et al., 2015; Gilbart & Hirdes, 2000; Lou et al., 2013; Resnick et al., 1997; van Beek et al., 2011). We found that socially isolated residents had significantly lower social engagement than residents who were not socially isolated. Social engagement is a crucial component of resident health, as lower levels are associated with increased risk of depression and mortality (Achterberg et al., 2003; Hjaltadottir et al., 2011; Kang, 2012; Kiely & Flacker, 2003; Lou et al., 2013). Lower social engagement has a negative impact on residents’ quality of life (Gilbart & Hirdes, 2000; Moyle & O’Dwyer, 2012). Social isolation and its associated conditions have significant health implications, and therefore, warrant routine assessment. For clinicians and staff in LTC, routine screening and assessment using existing administrative data, such as the RAI-MDS, may be one useful way to identify socially isolated residents. Once social isolation is identified, appropriate resources can be mobilized (e.g., private companion, group activities) and their impact on health may be monitored over time. Using the RAI-MDS as a preliminary screening tool to identify potential problems (i.e., social isolation) could facilitate proactive care planning and intervention for isolation and its related health outcomes. Although our study is descriptive, our methods and findings offer a potential approach for clinicians and the broader health system to develop a robust evidence base to identify social isolation in the LTC settings and monitor effects and outcomes of interventions.
Social isolation is influenced by sex (biological) and gender-related (socio-cultural) characteristics (Dahlberg et al., 2015). We found that socially isolated residents had a greater likelihood of being male, being single or divorced, than did non-socially isolated residents. Factors that predict social isolation often differ between men and women (Nicolaisen & Thorsen, 2014). Women are more likely to have a higher level of social contact than men due to their more robust social networks, which may alleviate isolation (Victor et al., 2006; Victor & Yang, 2012). Our finding that a greater proportion of men are socially isolated is consistent with other research that revealed a higher resident prevalence of men without a family or friend guardian in Alberta LTC homes (Chamberlain, Duggleby, et al., 2019). These findings suggest that there are important sex and/or gender-related differences that must be considered in future multivariable analysis.
A significant body of research describes the complex, but largely positive, impact of family member involvement on LTC resident health and well-being (Gaugler, 2005). In comparison, very little is known about those residents without family or friend involvement. Our study offers new insights into the demographic characteristics and functional status of residents without family or friend contact. To draw meaningful comparisons to the research literature, we compared our study findings to research examining older adults without a family or friend guardian. These residents typically have no contact with their family/friends (consistent with our operational definition of social isolation) and are often estranged due to histories of mental health diagnoses (schizophrenia, bipolar disorder) and/or experienced previous substance and alcohol use (Chamberlain et al., 2018; Chamberlain, Duggleby, Teaster, & Estabrooks, 2020). These resident characteristics are consistent with our findings that residents without family or friend contact had a greater likelihood of a diagnosis of schizophrenia, depression, and liver disease, compared to residents with family contact. Including a validated measure of social connections, whether it be social isolation or related concepts such as social support availability, in routinely collected data is a critical step to understanding the overall prevalence of these vulnerable residents in our LTC homes so health systems can deploy resources to support resident mental and physical health.
Limitations
This study focused on RAI-MDS data from 34 LTC facilities in one province. Our analysis was cross-sectional and descriptive; therefore, we are unable to make any causal claims. Given the limitations of secondary analysis, we were unable to compare our findings to other studies that used more comprehensive scales to assess social isolation (Menec et al., 2019, 2020; Shankar et al., 2011). However, by using a currently utilized databased (RAI-MDS) it will be easier for clinicians to use similar data in their practice to assess residents. Our future work will validate this RAI-MDS measure against first hand assessments of social isolation with residents and staff in LTC settings. We aim to undertake longitudinal observation of social isolation in congregate care settings and conduct multivariable analysis with population-level data to examine the associations between social isolation and resident health and stratified by resident sex. Another limitation of using the RAI-MDS 2.0 is that we were unable to examine relevant demographic characteristics (e.g., number and/or involvement of children/friends) and related concepts, such as loneliness, which are not assessed in the instrument (National Academies of Sciences, Engineering, and Medicine, 2020). It is important that future research look at ways to measure loneliness, as loneliness has an impact on the quality of life and mortality of LTC residents.
Conclusion
Socially isolated residents had more depressive symptoms, more frequent and severe pain, and lower social engagement compared to residents who were not socially isolated. Depression and a lack of social engagement can have devastating health effects, including increased risk of morbidity and mortality and a direct and deleterious impact on quality of life. Assessing resident social isolation is both ethical and critical to identify potential problems that may be readily amenable to relatively low-cost social interventions rather than high-cost medical interventions. Although clinicians struggle with identifying these vulnerable individuals through traditional screening methods, our approach, using a single item in an existing data source, has the potential to assist and alert clinicians and health systems screening for socially isolated LTC residents.
Footnotes
Author Contributions
SAC, CAE, WD, and PT planned the study. CAE assisted in data acquisition. SAC conducted the preliminary data analysis and drafted the manuscript. All authors contributed to the subsequent analysis and interpretation of the data. All authors contributed to revising the final manuscript and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Alzheimer Society of Canada Doctoral Fellowship to SC and a Tier 1 Canada Research Chair in Knowledge Translation to CE. The funding agency had no role in the study design, data collection, data analysis, interpretation of the data, writing of the report, or decision to submit the article for publication.
Availability of Data and Materials
The data supporting the conclusions of this article are housed in the secure and confidential Health Research Data Repository (HRDR) in the Faculty of Nursing at the University of Alberta (![]() ) in accordance with the health privacy legislation of participating TREC jurisdictions. These health privacy legislations as well as the ethics approval covering TREC data does not allow the removal of completely disaggregated data (i.e., resident-level records) from the HRDR – even if de-identified. Aggregated summary data specific to this manuscript can be requested through the TREC Data Management Committee (
) in accordance with the health privacy legislation of participating TREC jurisdictions. These health privacy legislations as well as the ethics approval covering TREC data does not allow the removal of completely disaggregated data (i.e., resident-level records) from the HRDR – even if de-identified. Aggregated summary data specific to this manuscript can be requested through the TREC Data Management Committee (