
Abstract
Introduction
Extensive research over the past decade provides largely consistent findings that lower neighborhood (usually defined by census blocks or other geographic markers for residential/proximal communities) socioeconomic status (SES) and social capital (e.g., norms of reciprocity, civic participation, trust in others, benefits of membership) contribute to poorer physical health outcomes, independently of such individual-level risk factors as age, sex, education, and income (Braveman, Egerter, & Mockenhaupt, 2011; Kawachi, Subramanian, & Kim, 2008; Marmot, 2005; Mohnen, Groenewegen, Völker, & Flap, 2011). Previous research also shows that higher levels of neighborhood social problems (e.g., social disorder and violence) and lower levels of social cohesion and connectedness are associated with poorer mental health among adult samples, controlling for individual socioeconomic risk factors and stressful life events (De Silva, McKenzie, Harpham, & Huttly, 2005; Echeverría, Diez-Roux, Shea, Borrell, & Jackson, 2008; Fone et al., 2007; Kim, 2008; Mair, Diez Roux, & Galea, 2008; Mair, Diez Roux, & Morenoff, 2010; Stafford, De Silva, Stansfeld, & Marmot, 2008; Wilkinson & Pickett, 2006).
Neighborhood/proximal community environment is considered more important for older than younger adults’ physical and mental health, because older adults tend to be less mobile and rely more on social support and services/resources available in their proximal communities (Glass & Balfour, 2003; Kubzansky et al., 2005). Accordingly, substantial research has examined associations between older adults’ physical and mental health and diverse measures of neighborhood environment. A systematic review provides modest evidence that neighborhood material or physical environments, neighborhood-level SES in particular, significantly influence older adults’ (aged 55+) physical health and functioning (Yen, Michael, & Perdue, 2009).
A systematic review of 19 mostly cross-sectional studies also found that neighborhood material or physical environments in general were associated with depressive symptoms in older adults (aged 65+), although the unique contributions of these variables appear to be small (Julien, Richard, Gauvin, & Kestens, 2012). Specifically, neighborhood or county-level income, poverty, or affluence were significantly correlated with depressive symptoms in U.S. and Canadian older adults (Kubzansky et al., 2005; Menec, Shooshtari, Nowicki, & Fournier, 2010; Muramatsu, 2003; Ostir, Eschbach, Markides, & Goodwin, 2003). Neighborhood factors such as concentration of minorities or older adults, residential stability, and/or neighborhood problems/social disorder (e.g., noise, heavy traffic, vandalism, crime/violence, poor perceptions of neighborhood safety, poor housing conditions and sanitation, and/or alcohol and drug use) were also found to be significantly associated with older adults’ depressive symptoms (Aneshensel et al., 2007; Beard et al., 2009; Gerst et al., 2011; Kubzansky et al., 2005; Menec et al., 2010; Ostir et al., 2003; Schieman & Meersman, 2004). Yet other cross-sectional studies have found no relationship between older adults’ depressive symptoms and neighborhood SES, racial/ethnic and age group compositions, and residential stability (Hybels et al., 2006; Johnson, Corley, Starr, & Deary, 2011; Wight, Cummings, Karlamangla, & Aneshensel, 2009).
Three longitudinal studies (Beard et al., 2009; Bierman, 2009; Wight et al., 2009) included in Julien et al.’s (2012) systematic review also show inconsistent findings. For example, Beard et al.’s 2-year study of New York City residents (aged 50+) found that although neighborhood affluence protected against worsening depressive symptoms after adjusting for individual-level covariates, residential stability and racial/ethnic composition were not associated with depressive symptoms. Bierman’s 2-year study of adults (aged 65+) in the District of Columbia and adjacent Maryland counties found that neighborhood disorder was not associated with changes in depressive symptoms among married people, while it was among nonmarried people. Wight et al.’s 5-year study of a nationally representative sample of older adults (aged 70+ at baseline) found no statistically significant associations between neighborhood disadvantage and ethnic minority composition and change in depressive symptoms once individual-level characteristics were controlled.
Compared with research on the effect of neighborhood material/physical environments, research on the effects of neighborhood social environments (e.g., perceived social cohesion/support, sense of belonging, and other neighborhood social capital and collective efficacy) on older adults’ mental health is less extensive, but findings tend to be more consistent. A study of older residents (aged 65+) in New York found that higher levels of perceived neighborhood collective efficacy (i.e., neighborhood-level social cohesion and informal social control or expectations for action) were associated with a lower prevalence of major depression in adults 65+ years (Ahern & Galea, 2011). A study based on Dutch older adults’ (aged 70+) self-reports found that neighborhood services and neighborhood social cohesion and other social capital predicted their physical (e.g., comfort and stimulation) and social (e.g., behavioral confirmation, affection, and status) well-being (Cramm, van Dijk, & Nieboer, 2013). Another study, this one of older Hispanic immigrants in Miami, Florida, found that individuals’ more positive perception of their neighborhood social environment was directly associated with better cognitive functioning and indirectly associated with lower depressive symptoms and anxiety through perceived satisfaction with instrumental social support and positive social interactions (Brown et al., 2009). A study of older Chicagoans also found that higher perceived neighborhood social cohesion was associated with more companionship among those who lived alone, though not among those who resided with others, suggesting that solo-living older adults are more likely to benefit from a supportive social environment (Bromell & Cagney, 2014).
Although these previous studies provide important insights into relationship between neighborhood physical and social environments and late-life depression, significant knowledge gaps remain. First, to date, longitudinal effects of perceived social cohesion on older adults’ depression have not been examined. Longitudinal studies are better suited to examining the effects of neighborhood/community characteristics on depression, because cross-sectional studies may not be able to discern whether neighborhood characteristics influence depression (social causation) or whether people with depression are more likely to reside in certain neighborhoods (social selection; Oakes, 2004). Cross-sectional relationship between perceived social cohesion and depressive symptoms may also be subjected to same-source bias (i.e., depressed people may report lower perceived sense of social cohesion when depression and social cohesion data are collected from them at the same time; Julien et al., 2012). Second, previous research has not identified psychosocial processes and mediating pathways by which perceived social cohesion may be related to depressive symptoms (Kim, 2008; Julien et al., 2012). The present study fills these knowledge gaps by examining (a) both cross-sectional and longitudinal associations between perceived social cohesion and depressive symptoms and (b) potential mediating effects of the frequency of going outside one’s home/building (e.g., for exercise, socialization, and other activities) in a nationally representative sample of older adults.
Conceptual Framework and Study Hypotheses
This study is based on the ecological theory of aging (Lawton, 1982, 1998; Nahemow, 2000) and the stress-buffering model of social support/resources and mental health (Cohen & Wills, 1985). Ecological theory of aging posits that there is a dynamic interplay between individuals’ level of competence and both objective and subjective environmental press/forces (i.e., the environment surrounding an older adult affects the challenge particular activities present). In person–environment transaction or interaction, “the less competent are controlled by and the more competent are in control of the environment” (Lawton, 1998, p. 4). The person–environment fit or lack thereof determines positive or negative affect and adaptive or maladaptive behaviors. However, the ecological model also posits that individuals’ appraisal of their environment is likely to elicit individually distinct responses and influence their behavior and affect, over and above the effects derived from the purely physical environment (Lawton, 1998; Scheidt & Norris-Baker, 2003). According to the stress-buffering model, people engage in a more benign appraisal of stressful situations when they perceive availability of social support and resources that can buffer the effects of stress, which leads to reducing negative emotional reactions to the stressful event and/or dampening physiologic/behavioral responses to it and enhances individuals’ coping abilities (Cohen & Wills, 1985). High levels of perceived cohesion are also likely to buffer against many life stressors through shared values and support, leading to less depressive symptoms (Cohen & Wills, 1985; Cramm et al., 2013; Echeverría et al., 2008).
Older adults often experience their neighborhood/proximal communities as the most salient environmental context (Kubzansky et al., 2005; Lawton, 1982). High perceived neighborhood/community social cohesion (e.g., being close-knit, willingness to help, shared values, trust among neighbors) is likely to have beneficial effects on older adults’ physical and mental health as it may influence psychosocial processes by contributing to their motivation to go outside their home/building and by providing them with more social interactions, meaningful social ties, greater connectedness, and mutual respect (Cagney et al., 2009; Kawachi & Berkman, 2000, 2001). Older adults may also feel more at ease and integrated into the community when they believe they can depend on neighbors and other local support systems for help in times of instrumental and emotional need (Bisconti & Bergeman, 1999; Krause, 1993). Social cohesion is also hypothesized to influence health because it facilitates dissemination and adoption of healthy behaviors and collective action among residents to promote service/amenity provision and access (Kim, 2008).
Conversely, older adults may be more vulnerable to neighborhood social disintegration and disorder (Wilson-Genderson & Pruchno, 2013). Objective and perceived threats to their safety and fear of victimization in neighborhoods with a high level of social disorder may lead older adults to avoid neighborhood-based exercise (e.g., walking), activities (e.g., visiting neighbors), and services/amenities, and the chronic stress from fear and isolation can contribute to unhealthy coping behaviors, reduced social engagement/activities, increased social isolation, and depression (Bowling & Stafford, 2007; Cagney et al., 2009; Echeverría et al., 2008; King, 2008; Mendes de Leon et al., 2009; Sun, Stijacic Cenzer, Kao, Ahalt, & Williams, 2012).
Ecological and stress-buffering theories and cross-sectional studies suggest significant associations between perceptions of neighborhood/community social cohesion and depressive symptoms. However, research also demonstrates that baseline depressive symptoms are a powerful predictor of subsequent depressive symptoms in late life (Choi & Bohman, 2007) and that any relationship between perceived neighborhood social cohesion and depressive symptoms over time may disappear once baseline depressive symptoms are controlled (Fujiwara & Kawachi, 2007). Based on these theories and previous studies, specific hypotheses for the current study were as follows:
Method
Data and Sample
Data are from Waves 1 and 2 (T1 and T2) of the National Health and Aging Trends Study (NHATS) collected in 2011 and 2012, respectively. The NHATS sample (N = 8,077) is representative of U.S. Medicare beneficiaries aged 65+ years who resided in the community in their own or another’s home (n = 7,197) or in residential care settings (n = 468 in nursing homes and n = 412 in other care settings; Kasper & Freedman, 2012). Those in older age groups and Blacks were oversampled to ensure sufficient sample sizes by age group and race/ethnicity (Montaquila, Freedman, Edwards, & Kasper, 2012). Our study focuses on the 5,326 sample persons who (a) resided in their own or another’s home and were self-interviewed at T1, (b) were interviewed again at T2, and (c) continued to reside in the community at T2. (Of the original 7,197 residing in their or another’s home at T1, 1,871 were excluded for the following reasons: 517 were proxy interviewed at T1, 88 had moved to nursing homes or other residential care facilities between T1 and T2, and 1,266 did not participate at T2 due to refusal [n = 881], death and/or proxy refusal [n = 301], or other reasons [n = 84]).
Measures
Depressive symptoms (dependent variable) at T1 and T2 were measured with the two-item Patient Health Questionnaire-2 (PHQ-2; Kroenke, Spitzer, & Williams, 2003), which captures the cognitive/affective symptoms of anhedonia and depressed mood by asking “Over the last month, how often have you (a) had little interest or pleasure in doing things; and (b) felt down, depressed, or hopeless?” Responses were based on a 4-point scale (1 = not at all, 2 = several days, 3 = more than half the days, 4 = nearly every day). The combined score (ranging from 2 to 8) represents symptom severity. Kroenke et al. (2003) reported PHQ-2 scores >3 as having a sensitivity of 83% and a specificity of 92% for major depression in primary and specialty care patients. The PHQ-2’s criterion validity for major depression in older adults is also reported to be good (sensitivity = 100%, specificity = 77%, area under the curve = 0.88; Li, Friedman, Conwell, & Fiscella, 2007).
Perceived social cohesion (independent variable) was measured with three items—people in this community know each other very well, are willing to help each other, and can be trusted—each on a 3-point scale (1 = do not agree, 2 = agree a little, and 3 = agree a lot). These items were drawn from the social cohesion scale originally developed by Sampson (1997). “Community” in NHATS was not defined by geographic boundaries but left to the sample person’s subjective interpretation. Cronbach’s alpha for the 3-item scale was .74.
Frequency of going outside home/building (putative mediator) was measured with the question, “In the last month, how often did you leave your home/building to go outside?” on a 5-point scale (1 = never, 2 = rarely [once a week or less], 3 = some days [2-4 days a week], 4 = most days [5-6 days a week], and 5 = every day). It was treated as a continuous variable, with higher ratings indicating higher frequencies.
Covariates were age in years, gender, race/ethnicity (non-Hispanic White vs. Black, Hispanic, or Other), level of education (college degree or higher vs. no college degree), and the number (0-14) of activities of daily living and instrumental activities of daily living (ADLs/IADLs) impairments.
Analysis
All descriptive analyses were performed using Stata13/MP’s svy function to account for NHATS’ multistage cluster sampling design and to adjust results based on the NHATS-specified stratification and personal analysis weights at T2 (which account for attrition since T1). All estimates presented are weighted except for sample sizes. Hypotheses were tested with structural equation modeling (SEM) using Mplus 7.11 (Muthén & Muthén, 1998-2012) to simultaneously estimate whether (a) perceived social cohesion predicted depressive symptoms at T1 and T2 (direct effect; Hypothesis 1), (b) perceived social cohesion also predicted depressive symptoms at T1 and T2 through its effect on frequency of going out (indirect [mediation] effect; Hypothesis 2), and (c) T1 perceived social cohesion predicted T2 depressive symptoms (Hypothesis 3; longitudinal direct effect). We first used gender-stratified linear regression models to test the significance of the indirect association between the independent variable (perceived social cohesion) and the outcome (depressive symptoms), controlling for covariates, age, race/ethnicity, education, number of ADL/IADL impairments, and, at T2, T1 depressive symptoms. Regression results showed significant associations between perceived social cohesion and depressive symptoms for both genders at both T1 and T2: B(SE) of perceived social cohesion = −0.042 (0.015), t = −2.80, p = .007 for men and −0.065 (0.014), t = −4.59, p < .001 for women at T1; and B(SE) of perceived social cohesion = −0.035 (0.013), t = −2.62, p = .011 for men and −0.031(0.012), t = −2.55, p = .013 for women at T2. We then tested the indirect effect with SEM following MacKinnon’s (2008) guidelines, which specify two critical conditions for mediation: (a) a relationship between the independent variable and the mediator and (b) a relationship between the mediator and the outcome.
Figure 1 depicts the analytic model. Age, race/ethnicity, education, and the number of ADL/IADL impairments were included as covariates of perceived social cohesion, frequency of going out, and depressive symptoms at T1. The model also specifies the direct effects of T1 perceived social cohesion on T2 perceived social cohesion, T1 frequency of going out on T2 frequency of going out, T1 depressive symptoms on T2 depressive symptoms, and T1 depressive symptoms on T2 perceived social cohesion. Because only two or three indicators were used to measure each of the two latent variables (social cohesion and depressive symptoms) at T1 and T2, lack of model identification precluded a separate confirmatory factor analysis (CFA) for each of these variables. Instead, the overall measurement models, including the set of latent variables, were specified and tested using CFA. Given significant gender difference in depressive symptoms in the sample, we fit gender-stratified models. Missing values (between 0.22% and 0.64%) in observed indicators for T1 and T2 depressive symptoms and one or two cases for T1 and T2 frequency of going out were accounted for with full information maximum likelihood estimates, which make use of all available data in model estimation and is considered an optimal method for analyses with missing data (Graham, 2009). Model fit was evaluated using root mean square error of approximation (RMSEA) < .05 (MacCallum, Browne, & Sugawara, 1996), the comparative fit index (CFI) > .95, Tucker Lewis Index (TLI) > .95, and the standardized root mean square residual (SRMR) < .08 (Hu & Bentler, 1999). RMSEA and SRMR are absolute indices that measure the extent to which a model differs from the best fitting model, which has a value of zero, and thus, larger values indicate greater divergence from the best fitting model. TLI and CFI are relative indices that compare an unconstrained model with the fitted model on an index ranging from zero to one, representing the worst and best possible models, respectively.

Analytic model.
Results
Sample Characteristics
Table 1 shows that the sample was 56% female, average age was 74 years, 82% were non-Hispanic White, 26% had a college degree, and the average number of ADL/IADL impairments was one. The mean perceived social cohesion score was 7.1 (of a maximum possible score of 9) at both T1 and T2, and the mean score for frequency of going out was 4.6 (i.e., most days to every day). The average depressive symptom scores at T1 and T2 were 2.9 and 2.8, respectively, which are slightly below the clinically significant cutoff. Significant gender differences were found in age, education, frequency of going out, and overall depressive symptoms. As expected, women were older, had less education, went out less frequently, and had higher depressive symptoms. Perceived social cohesion did not differ by gender.
Sample Characteristics.
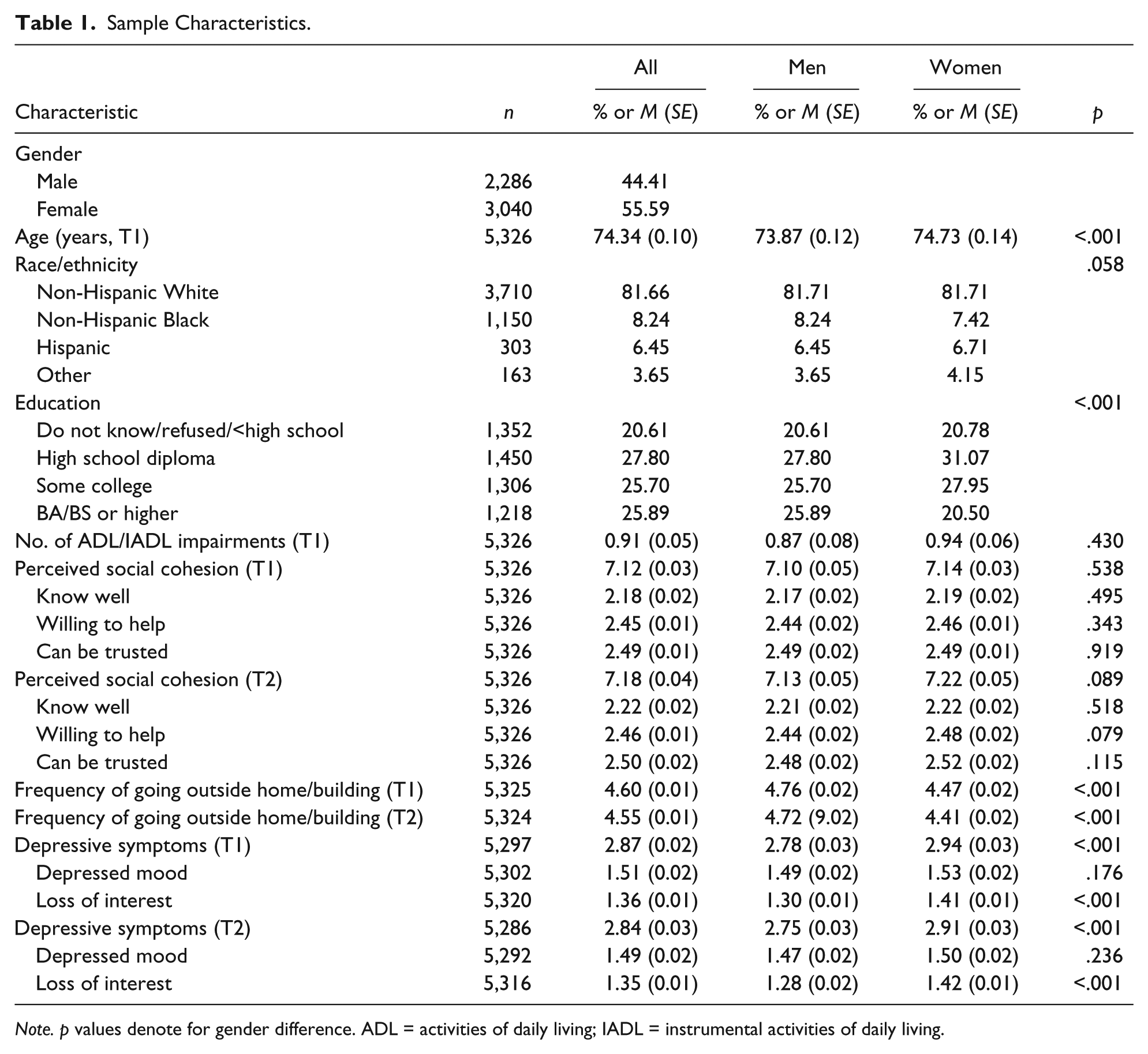
Note. p values denote for gender difference. ADL = activities of daily living; IADL = instrumental activities of daily living.
Direct and Indirect Effects of Perceived Social Cohesion on Depressive Symptoms
Table 2 presents the results of the structural equation models by gender. Model fit indices were good for both genders: RMSEA = .033 for men and .036 for women; CFI = .961 for men and .956 for women; TLI = .944 for men and .936 for women; and SRMR = .030 for men and .031 for women. The coefficients show that at T1, higher perceived social cohesion was associated with being non-Hispanic White for both genders and with younger age for women only. Lower perceived social cohesion was associated with college education for men only. Frequency of going out was negatively associated with age and ADL/IADL impairments but positively associated with being non-Hispanic White for both genders. However, frequency of going out was positively associated with perceived social cohesion for women only. Lower perceived social cohesion and lower frequencies of going out predicted higher depressive symptoms for both genders. More ADL/IADL impairments were also associated with higher depressive symptoms for both genders; however, being non-Hispanic White was associated with lower T1 depressive symptoms among women only. Thus, for both genders, T1 perceived social cohesion and frequency of going out were directly associated with T1 depressive symptoms. In addition, through T1 frequency of going out, T1 perceived social cohesion was also indirectly associated with T1 depressive symptoms for women but not for men: women, B(SE) = −0.024(0.005), p < .001; men, B(SE) = −0.011(0.007), p = .116. These results support Hypothesis 1 (direct effect of social cohesion on depressive symptoms) for both genders, and Hypothesis 2 (indirect effect) for women only at T1 only.
Linearized Coefficients and Standard Errors From Gender-Stratified Structural Models.

Note. ADL = activities of daily living; IADL = instrumental activities of daily living; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker Lewis Index; SRMR = standardized root mean square residual.
p < .05. **p < .01. ***p < .001.
Both T1 perceived social cohesion and T1 depressive symptoms predicted T2 perceived social cohesion among men, but only T1 social cohesion predicted T2 perceived social cohesion among women. As expected, higher T1 perceived social cohesion led to higher T2 perceived social cohesion for both genders, and higher T1 depressive symptoms led to lower T2 perceived social cohesion among men. Both, T1 frequency of going out and T2 perceived social cohesion predicted T2 frequency of going out for both genders. Finally, higher T1 depressive symptoms and a lower T2 frequency of going out predicted higher T2 depressive symptoms for both genders; however, neither T1 nor T2 perceived social cohesion was directly associated with T2 depressive symptoms for either gender. With the significant association between T2 perceived social cohesion and T2 frequency of going out for both genders, T2 frequency of going out mediated the effect of T2 perceived social cohesion on T2 depressive symptoms: male, B(SE) = −0.011(0.005), p = .012; female, B(SE) = −0.011(0.004), p = .004. These results do not support Hypothesis 1 (the direct effect of social cohesion) but support Hypothesis 2 (its indirect effect) and Hypothesis 3 (the lack of a longitudinal direct effect on depressive symptoms) at T2.
Discussion
This study examined whether older adults’ perception of social cohesion in their self-defined community was associated with their depressive symptoms, and, if so, whether frequency of going outside their home/building mediated the association. Adding to the largely cross-sectional body of research on the relationship between older adults’ social environment and depressive symptoms, this study examined both cross-sectional and longitudinal relationships.
The findings show that at T1, for both genders, more positive perceptions of social cohesion and higher frequency of going out were associated with lower depressive symptoms independently/directly. However, the indirect effect of perceived social cohesion through frequency of going out was significant only among women. At T2, for both genders, only the indirect effect of perceptions of social cohesion through frequency of going out was significantly associated with depressive symptoms. The findings support previous research showing that older adults who hold more positive perceptions of their community are likely to feel safer and more connected with other residents, which in turn may contribute to their motivation to go out, join activities, and engage in exercise outside their home (Cagney et al., 2009). Going outside one’s home/building is especially important for the physical and mental health of those older adults who are no longer employed and who have health problems, as it can reduce social isolation and promote physical activity and social engagement. The findings also show that T1 perceived social cohesion predicted T2 perceived social cohesion, T1 frequency of going out also predicted T2 frequency of going out, and T1 depressive symptoms were the strongest predictor of T2 depressive symptoms for both genders.
This study’s key finding is that there was no direct, independent effect of T1 or T2 perceived social cohesion on T2 depressive symptoms, controlling for T1 depressive symptoms. An earlier study of adults aged 45 through 84 years found that neighborhood characteristics including perceived social cohesion, aesthetic quality, and violence did not predict incident depression 4 to 5 years after baseline among either men or women with baseline depression (Mair et al., 2009). The strong impact of T1 depressive symptoms on T2 symptoms may have eclipsed any direct effect of T1 or T2 perceived social cohesion on T2 depressive symptoms. However, the absence of a direct, longitudinal effect of perceived social cohesion on depression may also be due to insufficient follow-up intervals (1 year in the current study and 1-5 years in previous studies). Older adults have often resided in the same neighborhood longer than younger adults (Glass & Balfour, 2003), and any effects of neighborhood factors are likely to be cumulative over a longer period of time. Findings of the stability/significant association between T1 and T2 perceived social cohesion as well as between T1 and T2 frequency of going out support this reasoning. Using the same logic, the significant cross-sectional relationships between social cohesion and depression may in reality reflect the underlying long-term, cumulative effects of neighborhood social environment on older adults’ mental health.
The study’s findings also raise some questions about gender differences. It appears that at T1 perceived social cohesion significantly affected women’s, but not men’s, frequency of going out. It is understandable that women, who were older, had less education, went out less frequently, and had higher depressive symptoms than men, may have been more sensitive than men about neighborhood/community characteristics and adjusted their frequency of going out accordingly. The significant indirect effect of T2 perceived social cohesion on T2 depression through frequency of going out for both genders may indicate that some men may have also become more sensitive about their community environment as they aged. The finding that T1 depressive symptoms predicted T2 perceived social cohesion among men, but not women, suggests that depression may have also contributed to men’s increasing sensitivity about their community social environment.
The significant direct relationship at T1 and indirect relationship at T2 between perceived social cohesion and depressive symptoms provide general support for the ecological theory of aging and stress-buffering model. As stated, neighborhood/proximal community environment is especially significant for older than younger adults. The present study findings show that older adults’ appraisal of their community social environments influences their behavior (going out) and affect (depressive symptoms). However, given gender differences and the lack of a direct, longitudinal relationship between social cohesion and depressive symptoms, further empirical studies are needed to examine the complexity of the behavioral and affective impact, or lack thereof, of older adults’ perceptions of their community social environments.
The study has some limitations. First, while previous research has mostly examined the physical and social environments of geographically defined neighborhoods, the definition of “community” in this study was left to older adults themselves. Although MacQueen et al. (2001) found that people tend to define the core of community using geographical locations and settings, they also included shared perspective, social ties, and joint action/activities as key elements. Thus, participants in the present study may have applied different definitions of community because specific features of community were not specified for them. Second, “going outside home/building” was also broadly defined, and reasons or purposes for going outside were not examined. Future research should more clearly define community or neighborhood, identify the specific features of community and social contexts that may influence perceived social cohesion, consider how those features may influence older adults to go out, and identify the activities that lead to lower depressive symptoms. Third, as noted, the 1-year interval between T1 and T2 may not have been a sufficient time to examine longitudinal relationships between neighborhood social environment and changes in depressive symptoms.
Despite these limitations, the study shows how the social environment may impact late-life mental health. It offers empirical support for the importance of perceived quality of neighborhood social environment and frequency of going out for older adults’ depressive symptoms. This study underscores the importance of enhancing the social environment to improve mental health in late life through active aging. Fostering mutual trust and solidarity among neighbors/community residents is a complex psychosocial process that may also require policy interventions involving substantial capital investment (e.g., for infrastructure and activities that bring people together and promote connectedness). Venues such as neighborhood senior centers and intergenerational community centers can provide safe and trusting environments where older adults engage with peers in the community, younger volunteers, and service providers; foster a sense of social cohesion; and increase older adults’ participation in exercise and social, educational, and other activities. In a rapidly aging society, other neighborhood/community organizations and institutions that are age-friendly and promote connections among community members of all ages are likely to help decrease older adults’ social isolation and increase social integration. According to World Health Organization (WHO), an age-friendly community encourages active aging by optimizing opportunities for health, participation, and security to enhance quality of life as people age (WHO, 2007).
Along with community-level and policy interventions, the findings also suggest the importance of individual-level interventions for late-life depression. Depressive symptoms may be prevented by helping older adults get out of their homes/buildings and remain or become engaged in their communities. Because research consistently shows that untreated depressive symptoms among older adults, even if subsyndromal, tend to worsen over time (Cui, Lyness, Tang, Tu, & Conwell, 2008; Lyness et al., 2007), both pharmacotherapy and psychosocial interventions should be available and readily accessible for older adults with depression and other mental health problems. Attitudinal barriers prevalent among older adults, such as misconceptions about mental health problems and stigma about receiving treatment, must also be addressed through both individual-level interventions and universal and targeted public health campaigns.
This study also underscores the importance of conducting research on the effects of neighborhood characteristics on older adults’ mental health. More longitudinal and experimental studies are needed to identify the trajectories and direction of causal relationships between neighborhood/community social environment and late-life depression. Given the well-established evidence on gender differences in the prevalence and impact of late-life depression (Chou & Cheung, 2013; Forlani et al., 2014), the potentially different courses of influence and impacts of both physical/material and social environment on older women versus older men also need examination.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.