
Abstract
Keywords
Background
Older adults in the U.S. is aging rapidly, the number of Americans age 65+ years is projected to nearly double from 2018 to 2060, and the 65+ age group will increase to 23% (PRB, 2019). U.S. Census reported that by 2034, there will be more older adults age 65+ years than children under 18 years (U.S. Census, 2018). According to American Association of Retired Persons (AARP), approximately 91% of older adults prefer to continue living in their homes and communities (AARP, 2012).
Aging-in-Community
Aging in community (AIC) is “a grassroots movement of like-minded citizens who come together to create systems of mutual support and caring to enhance their well-being, improve their quality of life, and maximize their ability to remain, as they age, in their homes and communities” (Blanchard, 2013, p. 7). The core mission of AIC is building interdependence and mutual support among older adults and create social capital to support aging improve quality of life and avoid social isolation (Blanchard, 2013). AIC underlines both aging in supportive and affordable neighborhood but also aging together (Blanchard, 2013).
Given the fast approaching “super-aged society” in the U.S.A., there is a critical need to identify and assess the impact of AIC programs aiming to help older adults remain independent at own home and community; while at the same time provide a sense of belonging neighborhood social cohesive environment to promote their wellbeing as they age.
Remain Independence at Own Home and Community
Remain independence (RI) has been a key factor essential to help older adults remain at home and in the communities (Yuen et al., 2007). Surprisingly, very limited empirical studies have examined RI among community-dwelling older adults (Kabayama et al., 2018; Lee et al., 2014). The few existing studies mostly used ADL or IADL to measure functional independence level among older adults. A population-based longitudinal study conducted in the Japan and a comparative study among Community-Dwelling Older Adults in China and South Korea found that risk factors towards functional independence included advanced age, low physical function, low nutritional status, low cognitive function and high depression risk (Kabayama et al., 2018; Lee et al., 2014). RI can be a subjective and dynamic concept for older adults. Yet, there has been a lack of clear definitions of and how RI is perceived by community-dwelling older adults.
Neighborhood Social Cohesion
Neighborhood social cohesion (NSC) is another key factor to be considered as older adult aging in community. NSC represented to neighbors’ mutual trust, connectedness, shared values, and support (Sampson, 2012). NSC fosters positive health outcomes, including better physical and social well beings (Cramm et al., 2013). Existing studies focusing on NSC and physical wellbeing among older adults have examined its relationships with walking and physical activities. Findings from a large national sample of 2013 to 2016 NHIS older adults age 60+ years shows that neighborhood social cohesion is associated with walking limitations among diverse groups of older Latinos (Vasquez et al., 2019). Another study analyzed 2017 NHIS adult sample also concluded that neighborhood social cohesion is positively related to meeting physical activity guidelines (Quinn et al., 2019). One large Netherland study surveying community-dwelling older people (aged ≥70 years) further reports that NSC reduced frailty (Cramm & Nieboer, 2013).
Multiple studies have shown that the reciprocal exchange occurs with stronger NSC lead to increased wellbeing, which further encourages older adults’ social and civic participation and reduced social isolation (Latham & Clarke, 2018; Parekh et al., 2018). In a study conducted among age-friendly communities in diverse urban neighborhoods, researchers found that older adults who had opportunities and were connected to their communities, regardless of race, ethnicity, or gender, were more likely to be civically involved (Parekh et al., 2018). This increased physical activity in turn lead to better mental health as well (Kim et al., 2020).
Community-Based Programs Promoting AIC
Researchers in the gerontology fields have discussed several existing and emerging AIC programs and models aiming to provide support and facilitate older adults building social connection among community-dwelling older adults (Bookman, 2008; Hou, 2019a; Hou et al., 2017, 2019; Thomas & Blanchard, 2009). Three programs were highlighted below and examined in the current study: (1) the village program with neighbors help neighbors grassroots network, (2) the neighborhood lunch program (i.e., congregate meals) authorized under Title III of the Older Americana Act to provide meals and nutritional services in group settings (Lloyd & Wellman, 2015; Mabli et al., 2015)., and (3) University-based lifelong learning programs meeting the learning and social engagement needs (American Council on Education, 2007). These programs represent different AIC options for community-dwelling older adults with different demographic and background characteristics (Hou, 2019b; Thomas et al., 2017).
Village program
The village program is a grass-root program run by trained volunteers and paid staff to connect members with free, low cost, or discounted services as needed, as well as coordinate village-wide programs and activities (VtVN, 2017). A key mission of the village program is to strengthen members’ social connections and reducing social isolation to promote AIC (Davitt et al., 2015; Scharlach et al., 2014).
Yet, there have been limited empirical studies examine the impact of village programs. There is some preliminary evidence supports that village program may have protective effect till 85+ years as demonstrated via self-rated higher quality-of-life across pre-old, young old, and old-old age groups. Study showed the quality-of-life dropped significantly once an individual reached the oldest group (Hou et al., 2017). A mixed-methods research study reports that village participants across all age voiced strong desire to stay connected (Hou, 2019c). Overall study participants reported high quality-of-life and there was no significant difference by living arrangements. However, further qualitative analyses found that those who live alone preferred informal socialization; while those who live with others preferred formal socialization (Purdie et al., 2017). Other studies also show village programs help promote social connection (Gardner, 2011; Graham et al., 2014). Specifically, village members with higher self-efficacy of maintaining independence were found in better health or participated in more social activities (Graham et al., 2014).
Congregate meal programs
Government supported neighborhood lunch program (NLP) (i.e., congregate meals) provides meals and nutritional services among older adults in group settings (Lloyd & Wellman, 2015; Mabli et al., 2015; Porter et al., 2016). The mission of such NLP is to enhance older adults’ quality of life by providing nutritious meals and support services to help older adults maintain independence and dignity (Meals on Wheels, etc., 2017). Eating together and participating in educational activities can also facilitate social connection and information sharing (Winterton et al., 2013). Such programs provide older adults opportunities to socialize while addressing their nutritional needs at the same time (Porter et al., 2016). Studies have shown effectiveness of NLPs to reach our diverse aging groups with various racial and income profiles (Brewer et al., 2016; Hou, 2019b; Thomas et al., 2017).
University lifelong learning
University-based lifelong learning program is another type of AIC program which provides high-quality education for older adults, opportunities to connect with young people, and engage in various campus programs and services (Park et al., 2016). However, there has been no study investigating the NSC or RI in the context of university lifelong learning programs for older adults. One study evaluated emotional and intellectual health among older adults in a university-based lifelong learning program, Program 60, found that the program increases older adults’ emotional satisfaction as they enjoyed the intergenerational connection with young people, and empowered new-learned skills for daily life (Park et al., 2016).
Gap and Objectives
Overall, there have been limited studies examine the impact of AIC programs on RI or NSC among community-dwelling older adults (Graham et al., 2014; Hou et al., 2018). Existing evidence suggest RI and NSC may impact older adults with different characteristics or support system differently (Hou et al., 2018; Kabayama et al., 2018; Lee et al., 2014). It is critical to exam how RI and NSC operate among older adults participating in different community-based programs promoting aging in community. How older adults participate in programs promoting AIC perceived their NSC and or RI levels?
Studies showed that neighborhood lunch program (NLP) participants were mostly older adults with diverse racial and income levels (Brewer et al., 2016; Thomas et al., 2017). Older adults participating in university-based lifelong learning programs (LLP) are more likely to be white and have higher education (Park et al., 2016). Village programs mainly consist of middle-income white older adults (Gardner, 2011; Graham et al., 2014; Hou, 2019a–2019c; Hou et al., 2017, 2018). An empirical study further reported that LLP and village participants were more likely to drive or share rides, while NLP participants more likely to take public transportation or walk to the site (Hou, 2019b). Thus, deeper discussions on the perceived RI and NSC among older adults in different AIC programs are important and can have policy implication to better help identify service gaps to meet the diverse older adult population and their growing needs. This study examines remaining independent (RI) and neighborhood social cohesiveness (NSC) among older adults participating in three aging-in-community programs in a southern state in the U.S.A. for tailored program development.
Research Design and Methods
Study Sample
This was a cross-sectional study design. Older adults from three community-based programs in a southern state of the U.S. with high concentration of retired individuals were recruited. The study consisted of a convenient sample of older adults from a village program, a county neighborhood lunch program (NLP), and a university-based lifelong learning program (LLP). These AIC programs were selected due to their common mission of promoting aging-in-community and existing connections with the researcher. Two open villages in the area, both were part of the Village-to-Village network, jointly participated in the study. The NLP was a county-wide program with multiple sites across the counties. Three of the larger sites from the NLPs were selected by the NLP executive director to participated in the study. The LLP was located at a large public university in the same mid-size city as the village and NLP programs in the current study. All older adults participated in the study programs were eligible to participate in the study survey.
Data Collection
A self-administered aging-in-community survey was conducted. The mode of survey administration was decided in consultation with program site coordinators. Paper-pencil survey was administered on sites among members of the village and NLP programs since not all members used email and some were older and needed assistance with completing the survey. Site coordinators assisted with the coordination and administration of the study survey. About 80% of the participants from both villages and NLP programs participated in the study. An online survey was setup with survey link sent via emails to over 400 LLP members since email was the primary mode of communication with members. About 25% of the LLP members completed the survey. The survey took about 15 to 20 min. to complete. The study was approved by the human subject office at the PI’s institution (IRB # SBE-17-12893).
Measures
The self-efficacy for remaining independence (RI) at own home was measured by asking three statements: “I have an easier time taking care of myself than I used to,” “I have an easier time taking care of my home than I used to,” and “I am more likely to be able to stay in my own home as I get older” (Graham et al., 2014). The reliability was moderate in this original study (Cronbach’s α = .66).
The NSC is adapted from the National Health Interview Survey (National Center for Health Statistics, 2017). Participants were asked whether they agreed or disagreed with the following four statements: “(1) People in this neighborhood help each other out; (2) There are people I can count on in this neighborhood; (3) People in this neighborhood can be trusted; and (4) This is a close-knit neighborhood.” The internal consistency of the items in this scale was high (Cronbach’s α = .92).
Data Analyses
Descriptive analyses were used to describe the three samples. Normality tests of the two dependent variables (RI and NSC) were checked using Kolmogorov-Smirnov tests. Data showed significant results with p < .001, indicating data was not normally distributed. Therefore, non-parametric tests were used. Non-parametric Chi-square tests were used to compare categorical variables and non-parametric Kruskal-Wallis one-way Analysis of Variance (ANOVA) tests were used to compare continuous variables among participants in the three AIC programs. Cronbach’s alpha was used to assess the reliabilities of the RI and SC scales to ensure internal consistency of the scale items among the current sample. Multiple regression analyses were used to assess RI and SC among older adults participating in different AIC programs, controlling for demographics (age, marital, and education). Normal P-P plots were used to check normality, scatter plots of residuals were used to check homoscedasticity, and variance inflation factor (VIF) was used to check the multi-collinearity of the data before the regression analyses were carried out (Statistics Solutions, 2020). All regression assumptions were met with the current study data.
Results
A total of 289 older adults participated, with pretty equal sample size from each AIC program: 33% from the village programs (n = 96), 38% from lifelong (n = 110), and 29% from neighborhood lunch programs (n = 83). Mean age was 72.4 (SD = 8.68) years, with majority female (78%). NLP participants were significantly older (77 vs. 70 years; p < .001). More village participants were in pre-old age (≤64 years) (26% vs. 5%–17%), NLP had highest proportion of the oldest old group (age 85+ years) (20% vs. 2%–7%), while LLP had the majority participants in young old group (62% vs. 32%–38%). NLP group had the lowest proportion of participants who were married (25% vs. 57%–70%; p < .001), had a college education (31% vs. 86%–92%), or being white (24% vs. 91%–95%). Data showed a higher proportion of village older adults were living alone (46%), compared with the NLP (35%) and LLP (25%) (p < .05) (Table 1).
Demographics Among Participants in the Three Aging-in-Community Programs: Lifelong Learning Program (LLP), Neighborhood Lunch Program (NLP), and Village Programs.

Note. chi-square (6) = 49.591 (p < .001). LLP = lifelong learning program; NLP = neighborhood lunch program; Village = village program.
p < .05. **p < .001.
Reliabilities analyses of the 3-item remain independence (RI) scale was satisfactory, with Cronbach’s alpha of .804 showing good internal consistencies. Overall study participants rated moderate RI level with scale item mean of 3.37 on 5-point Liker scales. Kruskal-Wallis ANOVA analysis showed significant group differences (p < .001). Post-hoc Bonferroni pairwise comparisons analyses found NLP participants ranked significantly higher than village participants (rank orders of 152.13 vs. 116.40; p = .008), with scale mean of 11.56 versus 10.05 between groups. And NLP participants also ranked significantly higher and LLP participants (rank order of 152.13 vs. 91.13; p < .001), with scale mean of 11.56 versus 9.22 between groups (Table 2).
Reliabilities of the Remain Independence (RI) and Neighborhood Social Cohesiveness (NSC) Scales Among Older Adults (n = 289).

Note. RI = remain independence; NSC = neighborhood social cohesion; CITC = corrected item-total correlation.
Reliabilities of the 4-item neighborhood social cohesiveness (NSC) also showed satisfactory internal consistencies with Cronbach’s alpha of .878. Overall, program participants rated high NSC level with scale item mean of 3.77 on 5-point Liker scales (Table 3). Kruskal-Wallis One-way ANOVA analysis also showed significant group differences (p = .011). Post-hoc Bonferroni pairwise comparisons analyses found NLP participants ranked significantly lower than village participants (ranks of 115.92 vs. 152.50; p = .009), with scale means of 14.06 versus 15.72 between groups.
Kruskal-Wallis ANOVA Analyses on RI and NSC by Three AIC Programs.
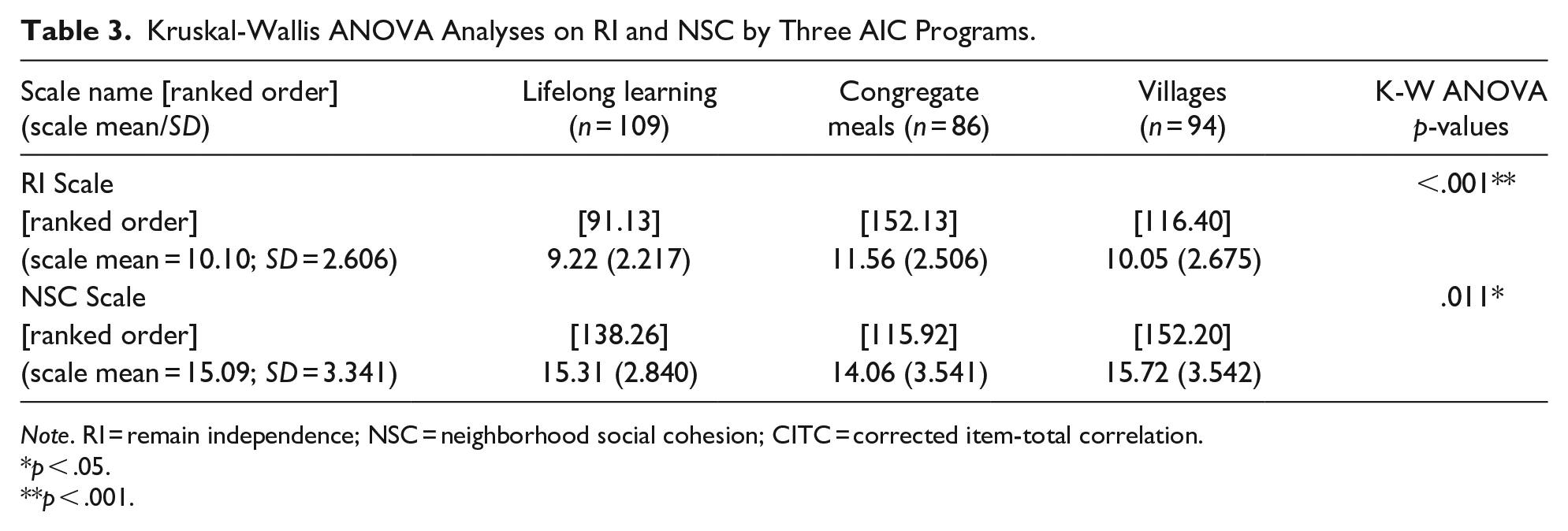
Note. RI = remain independence; NSC = neighborhood social cohesion; CITC = corrected item-total correlation.
p < .05.
p < .001.
After controlling for age, marital status, and education, regression analyses showed the inter-group differences remained for RI (p = .031), while the inter-group significance disappeared for NSC. Data further showed that education level had significant inverse relationship with RI (beta = –1.22; p = .003), while married status had a positive relationship with NSC scores (beta = 1.02; p = .021).
Discussion and Implications
This study showed significant different demographic profiles among participants in the three AIC programs. Overall, NLP participants tended to be the oldest. More village participants were in pre-old age (≤64 years), although the majority were in young old (38.3%) or old old age (28.7%). NLP had more age over 85 years, while LLP had the majority participants in the young old group (65–74 years). The current study finds that NLP group had the lowest proportion of participants who were married (25%), had a college education (31%), or being white (24%).
Current results showed interesting and somewhat surprising findings on the higher RI scores among the NLP participants, and the inverse relationship between RI and education. There has been very limited study specifically examined relationships between RI and education. Interestingly, in a comparative study of China and S. Korea community dwelling older adults, researchers also reported higher education had an inverse association with self-reported functional independence (poorer ADL and IADL) among community-dwelling older adults (Lee et al., 2014). The average education level was very low in both the Chinese and South Korean samples. Older adults with lower education may more likely to be blue-collar workers, which may lead to more physically active and strenuous lifestyle, which could serve as a protective factor from cognitive or physical impairment (Lee et al., 2014). Lee et al. (2014) suspected that the inverse relationship between socioeconomics and functional independence might not be unique in these two East Asian countries, but a phenomenon in rapidly developing countries (Lee et al., 2014). Although not significant finding, one village program also reported data trend approached borderline significance of higher self-efficacy of remaining independence among those with less than college education or who used companionship services more frequently members (Graham et al., 2014). Yet, future studies should further examine underlining mechanism of the NLP on maintaining RI for the older adults and clarify the potential inverse relationship between RI and education.
Current study showed the significant differences of NSC scores among different AIC program participants disappeared after controlling for demographics including age, marital status, education. Yet, current data further indicated that married older adults scored higher on NSC among regardless of AIC program participated. NSC may act as a buffer against the adverse effects of being single and poor on the well-being of older adults (Cramm et al., 2013). Existing study also reported married individuals or those with higher SES have higher level of NSC, which in turn improves their well-being (Cramm et al., 2013). Being single or not married, older, and poorly educated are more likely fall into the frail population (Cramm & Nieboer, 2013). A mixed-method study conducted among people who were over age fifty in the British found that there was a moderate association between NSC and mental wellbeing. The association was stronger for individuals in the older cohort groups (60s–70s years) than in the younger cohort in their 50s (Elliott et al., 2014). One large study supports that older adults who live alone particularly benefit from the socially cohesive neighborhood environments as it predicted companionship, whereas NSC might not provide as significant benefits to those who resided with others (Bromell & Cagney, 2014).
Limitation
This study is limited to convenience samples from three aging-in-community programs in a southern state in the U.S. Results may not be generalizable to other older adult groups. Current study findings were also limited to its cross-sectional survey design. An experiment study with before and after program comparisons to assess the changes would have make the findings stronger. In addition, future studies are recommended to consider mixed methods research approach to provide deeper and nuanced insights with rich contextual information than the quantitative scores alone (Creswell & Plano Clark, 2018). There is still lack of both qualitative and quantitative empirical evidence regarding if and how AIC programs help community dwelling older adults improve remaining independence and neighborhood social cohesion.
One main strength of the current study is the direct comparisons of demographic and background profiles across group on the same variables. More importantly, this study provides direct comparisons of RI and NSC across older adults in different AIC programs to assess the potential impact such program may have to promote aging in community. This is among the first study attempted to explore the perceived RI and NSC levels among older adults in different AIC programs in the U.S.A., and directly compare these key AIC related factors. Results provide interesting and somewhat unexpected findings which warrant further investigations.
Recommendations
It should be noted that RI is a dynamic and subjective perception. Future studies are recommended to examine factors affecting older adults’ independence from multiple and multi-level perspectives, including individual level and environmental level (Kabayama et al., 2018). In addition, how NSC might influence older adult’s relocation intention choices of aging and living environment as they age in community and the mechanism behind that impact warrant attention as it provides guidance to the development of community-level interventions.
Implications
Current findings have both methodological and policy implications. From methodological perspectives, current study is a first attempt to examine RI and NSC among convenient samples of older adults participating in different AIC programs. More representative samples from larger national studies are needed to further examine these important AIC issues. In addition, besides quantitative results, mixed methods studies and longitudinal or experiment designs are recommended to better assess the impact of programs on RI and NSC among older adults with diverse characteristics and needs aging in community.
From policy perspectives, policy makers may consider providing funding to conduct larger evaluation studies to assess the impact of various community-based programs on key factors such as RI and NSC facilitating AIC. Policy and programs to continue support for structural changes and encourage age-friendly communities development are in strong need as our global society aging rapidly.
Conclusion
Current findings noted the diverse characteristics of older adults participating in different community-based programs. Data also showed the higher RI yet lower NSC among the NLP older adults comparing with the village and LLP participants. Programs and services to promote NSC and RI among community-dwelling older adults warrants continued research (Cramm et al., 2013; Graham et al., 2014). Future studies are recommended to explore potential mechanisms congregate meal program had on promoting RI (Meals on Wheels, 2007). Findings also call attentions to RI among higher education and NSC among single or widowed older adults as we continue strengthen community-based services and programs facilitating aging-in-community.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the faculty start-up research funding at the University of Central Florida, Orlando, FL.
Ethical Approval
This study has been approved as an exempt study by the UCF Institutional Review Board (SBE-17-12893). A cover page with consent information was provided with the paper-survey version and “click-through consent page” for the online survey version, before participants voluntarily agreed to take part of the anonymous survey.