
Abstract
Informal caregivers of children and adolescents with cancer, predominantly women, frequently manage complex treatment and care demands with minimal support. This study explores the unmet supportive care needs of informal caregivers of children and adolescents with cancer, as well as their experiences and relationships with oncology health navigators, who have recently been incorporated into the Chilean public healthcare system. A qualitative multiple-case study was employed, with macro-regions (north, center, and south) defined as cases and caregivers as embedded units, selected to capture regional variability in carers’ experiences. Twenty-three in-depth interviews were conducted with female caregivers. Based on conventional content analysis, four unmet supportive care needs were identified: the need for humanized treatment, clear and timely information, adequate psychosocial support, and sufficient social protection. It was also observed that participants’ limited knowledge of the role of oncology health navigators in healthcare services limits the potential of these navigators to reduce inequities. These findings reveal substantial gaps in caregiver support, emphasizing the importance of enhancing oncology health navigator programs and integrating the role of civil society organizations within the care system. Integrating caregivers’ unmet supportive care needs in the design of pediatric oncology services, with a gender perspective, is essential to ensure a more equitable health system.
Introduction
Childhood and adolescent cancer represent a significant public health challenge globally, being one of the leading causes of death worldwide (Pan American Health Organization, 2025). In Latin America, about 29,000 new cases are estimated each year, and in Chile, incidence reaches 676 cases per year in the 0 to 19 age group, with an average of 518.7 cases per year, specifically in the 0 to 14 age group (Ministerio de Salud, 2024).
Given this context, significant progress has been made worldwide in the diagnosis and treatment of cancer in the pediatric and adolescent population, which has led to five-year survival rates of over 80% in developed countries. However, this figure remains below 30% in low and middle-income countries due to inequalities in access to medical care, infrastructure, and treatment availability (Bhakta et al., 2019; Lam et al., 2019). Five-year survival has improved considerably in Chile, reaching 78.4%, close to the levels observed in high-income countries (Ministerio de Salud, 2023, 2024).
In this scenario, it is essential to recognize the role of informal caregivers, who accompany children and adolescents throughout their illness and healthcare process. This role is defined as someone who provides unpaid and unprofessionalized care, usually a close relative (Baum et al., 2022). The literature indicates that caregivers experience a major disruption to their daily routines when they become involved in the medical and care system. This involvement often leads to substantial physical, emotional, and social strain, negatively impacting their quality of life, personal relationships, and work performance (Rosado Pulido et al., 2021; Toledano-Toledano et al., 2020). Furthermore, prolonged caregiving has been linked to physical and mental health issues, including symptoms of post-traumatic stress disorder, depression, and anxiety (Borrescio-Higa & Valdés, 2022; Cristina Batista Da Silva et al., 2019; Reuvers et al., 2023).
In addition, international studies have identified a wide range of unmet supportive care needs—referring to the broad array of services that people with cancer and those close to them may require from diagnosis and throughout treatment, follow-up care, survivorship, palliative care, and bereavement, if necessary—to address physical, emotional, social, psychological, informational, spiritual, and practical concerns (Fitch, 2008). These needs often center on timely access to information, financial assistance, education and spiritual support, among other aspects (Aziza et al., 2019; Lewandowska, 2022; Lopez-Leon et al., 2023).
It is essential to highlight the gender differences in informal care. Evidence shows that women are the leading providers of informal care globally (Cascella Carbó et al., 2020). This creates and exacerbates significant gender inequalities, as it is women who experience the most severe physical, psychological, emotional, and economic consequences of informal caregiving, as recognized in the relevant literature (Davies & O’Connor, 2023; Peña-Longobardo et al., 2021; Skinner & Sogstad, 2022; Vaalavuo et al., 2023).
Due to the complexity of the cancer care process and the various supportive care needs that arise for those diagnosed with cancer and their carers, Chile has developed initiatives to address the specifics of child and adolescent cancer that take into account the particularities of the Chilean healthcare system. A key feature of the Chilean healthcare system is its segmentation and fragmentation, involving both public and private participation. It is segmented because different subsystems with various financing and provision modalities coexist, each specializing in a different income-based population segment. The lack of integration within the service provision network highlights significant fragmentation (Castillo-Laborde et al., 2017). In this context, approximately 80% of children and adolescents receive care through the public healthcare system under the PINDA program (Programa Infantil Nacional de Drogas Antineoplásicas) (Cecilia et al., 2023). This program operates across the country’s northern, central, and southern macro-regions through health centers with varying levels of complexity. High-complexity pediatric oncology services are concentrated in the center macro-region, so the PINDA program has established referral pathways from the north and south to this area.
The National Plan for Childhood and Adolescent Cancer, presented in 2024, is among the initiatives that have been developed. This plan explicitly recognizes the impact of the disease on families and caregivers (Ministerio de Salud, 2024). Of particular relevance is also the implementation of the role of ‘gestor de casos oncológico’, established in the public healthcare system following the enactment of the National Cancer Law in 2020. Inspired by the patient navigation model developed in the United States, this role aims to support individuals diagnosed with cancer and their caregivers throughout treatment, facilitating access to care and ensuring continuity, particularly in fragmented healthcare systems (Chan et al., 2023; Franklin et al., 2022; Ministerio de Salud, 2024; Simbaña et al., 2022). As there is no direct English translation, this article will use the term ‘oncology health navigator’ to refer to this role following the model on which it is based.
Although the international literature has documented the consequences of informal caregiving and the unmet supportive care needs of caregivers, evidence from Chile remains limited. Studies have shown that when these needs are not adequately identified and addressed, the well-being and health of children and adolescents in care can also be negatively affected (Rosado Pulido et al., 2021). Therefore, it is crucial to recognize and highlight the unmet supportive care needs of informal caregivers from a gender perspective as an integral part of pediatric and adolescent oncology care (Khanali Mojen et al., 2022; Reuvers et al., 2023).
Within this framework, while the experiences of informal caregivers of children and adolescents with cancer have been documented, there is limited evidence on their interaction with oncology health navigators, particularly in Latin American settings. Therefore, the present study explores the unmet supportive care needs of informal caregivers of children and adolescents with cancer, as well as their experiences and relationships with oncology health navigators, who have recently been incorporated into the Chilean public healthcare system. This will enrich the national and international scientific literature on this topic and support the design of supportive care strategies in pediatric oncology services that involve oncology health navigators and caregivers as key actors.
Methods
Study Design
This study is framed within the qualitative research paradigm, which recognizes the coexistence of multiple experiences regarding the same phenomenon, valuing and making visible the subjective account of individuals around a given topic (Curtis, 2022). From this perspective, we explore how people interpret and give meaning to their social environment (Patton, 2002), in this case, caregivers of children and adolescents with cancer. Given the scarcity of national literature on the subject, the study is descriptive and exploratory.
The methodological design is a multiple case study, which examines several cases or bounded systems through in-depth data collection to develop a thorough understanding of the phenomenon being studied (Anthony & Jack, 2009). This design was adopted to capture regional variability in caregivers’ experiences with pediatric oncology services. Therefore, the macro-regions (North, Center, and South) constitute the cases, and informal caregivers are the embedded units of analysis. Each case is bounded by the following: (i) territorial context, (ii) regional pediatric-oncology service configuration and referral pathways; and (iii) the study period (April to August 2024).
Recruitment and Selection of Participants
Participants were selected using a purposeful sampling strategy (Ahmad & Wilkins, 2025; Czernek-Marszałek & McCabe, 2024). First, information-rich caregiver profiles were defined in accordance with the study’s objectives and inclusion and exclusion criteria. Caregivers who met the following criteria were included: they were over 18 years old; they had internet access; the public healthcare system provided their child’s treatment; and they resided in one of the three designated macro-regions at the time of diagnosis (north, center, or south of Chile). These residence criteria were intended to deepen the analysis of Chile’s territorial contexts and explore potential regional differences in caregivers’ experiences with the healthcare system. This approach supports our case logic but does not imply statistical representativeness. Participants whose children had been diagnosed more than 5 years ago were excluded due to the recent incorporation of oncology health navigators into the healthcare system.
Then, purposive recruitment was initiated based on access feasibility and carried out through civil society organizations focused on child and adolescent cancer, which were initially contacted via email. These organizations received all the information on the study and subsequently extended the invitation to participate to the caregivers. Based on those who agreed to participate, snowball sampling was used to contact profiles that remained under-represented (Naderifar et al., 2017), inviting enrolled participants and key informants to refer additional eligible caregivers. Each person contacted was given an information sheet detailing the objectives and purposes of the study, the institutions responsible, its source of financing, and the topics to be addressed in the interview. The voluntary nature of participation was emphasized.
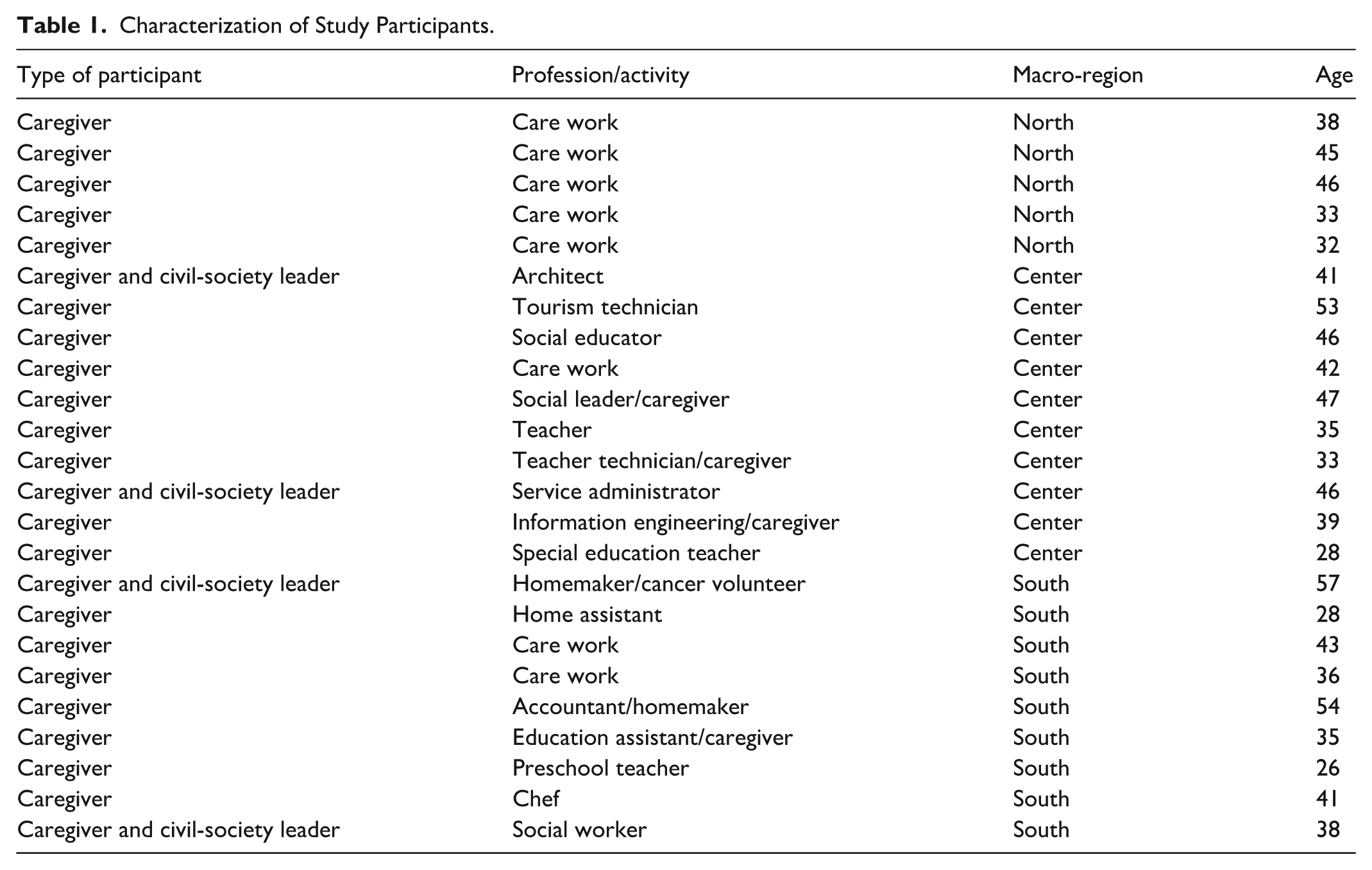
Of the 38 caregivers contacted, 23 participated, while 15 declined due to insufficient time for the interview. Consistent with data adequacy—understood as privileging the richness and complexity of evidence needed to address the study aim rather than a numeric sample target—we closed recruitment at 23 interviews, once the dataset captured a reasonable range of experiences across macro-regions, which was sufficient for our analysis (Braun & Clarke, 2021; Thorne, 2020; Varpio et al., 2017). All participants were women aged between 26 and 57 years. Most were dedicated exclusively to caring for their children at the time of the interview, although thirteen of them had a profession. Four participants also had leadership roles in civil society organizations related to childhood and adolescent cancer, and sixteen were supported or actively involved in these organizations. Regarding territorial distribution, ten resided in the Metropolitan Region (central macro-region), nine in the southern macro-region, and four in the northern macro-region. The difficulty of contacting participants in the northern area is worth noting, which explains the lower number of interviews conducted in that macro-region. The profile of the participants is detailed in Table 1.
Characterization of Study Participants.
Data Collection
Data were collected through semi-structured individual interviews. A pre-determined interview guide, developed from the study aim and relevant literature, ensured coverage of key topics in a flexible manner, allowing the emergence of new information (Kallio et al., 2016). The interviews covered three main topics: (i) diagnosis and treatment experience of children and adolescents with cancer, (ii) unmet supportive care needs, challenges, and facilitating factors during the process, and (iii) relationship with healthcare professionals and oncology health navigators.
The interviews lasted between 45 and 60 min and were conducted between April and August 2024. Depending on the participants’ availability, they took place either in person at the premises of shelters led by civil society organizations or virtually via Zoom or WhatsApp video calls. Virtual platforms were crucial in facilitating participation, given that many caregivers dedicate significant time to caring for their children and did not feel comfortable leaving them alone for an in-person interview. The interviews were conducted by FV, AR, and CC, researchers with extensive experience in qualitative research and interviews in sensitive contexts. To safeguard confidentiality, an informed consent form was signed virtually beforehand.
Data Analysis
Data analysis was conducted using conventional content analysis, in which categories are derived from the data during the analysis process rather than being predefined (Graneheim & Lundman, 2004; Mayring, 2015). First, a professional transcriptionist manually transcribed the interviews, and then FV, CC, and AR reviewed them to ensure fidelity. The second stage consisted of immersion through repeated reading of the transcripts. In the third stage, meaning units relevant to the study aim were identified, and open coding was performed using the Atlas.ti software. The codes were then compared and clustered into subcategories, which were further abstracted into higher-order categories. The interview guide only structured data collection and did not function as a predefined coding scheme. All codes and categories were inductively generated from the narratives. FV, CC, and AR conducted the initial open coding. Then, FV, CC, and AR, together with AO, BC, and ME, engaged in codebook refinement and consensus meetings to consolidate the final coding system. The textual quotations used in this article were translated from Spanish to English by a native speaker and reviewed by the authors to ensure fidelity to the original meaning.
Qualitative Scientific Rigor
To enhance the study’s methodological rigor and trustworthiness, investigator triangulation was employed under a constructivist orientation. Therefore, the data were analyzed through independent coding, iterative refinement of the codebook, and consensus meetings. These analyses were conducted among the teams’ researchers, who have different social and health sciences disciplines, to minimize interpretive biases and enhance breadth and comprehensiveness, rather than force convergence on a single truth (Carter et al., 2014; Ellingson, 2009).
Ethical Considerations
From an ethical perspective, the study followed the ethical recommendations for qualitative research (Moriña, 2021; Morse, 2007) and the universal principles of scientific ethics, including respect, beneficence, nonmaleficence, and justice. Each participant was given a detailed information sheet, and the team was constantly available to resolve doubts and ensure full voluntary participation. The informed consent was digitally signed through the encrypted Alchemer platform. A PDF document of the signed informed consent form is then generated, with one copy given to the participant and another kept by the research team. Each participant was assigned a code to protect their anonymity.
The risk-benefit analysis concluded that the risks were minimal. However, as women are primarily responsible for providing informal care, they may experience greater psychological and emotional consequences. Therefore, the researchers conducting the interviews received training in psychological first aid. Contact details for civil society organizations offering social support, including free psychological care, were also made available. The Scientific Ethics Committee of Universidad del Desarrollo approved the study (#2024-01).
Results
The results are divided into two sections. The first presents the unmet supportive care needs of informal caregivers concerning the healthcare system and other needs, such as social protection. The second section examines the potential role that oncology health navigators can play in addressing these needs.
Unmet Supportive Care Needs of Informal Caregivers of Children and Adolescents with Cancer
Based on the interviews, caregivers’ primary unmet supportive care needs can be grouped into three categories specifically related to the healthcare system: humanized treatment, access to information, and mental health support. A fourth category not necessarily associated with the healthcare system was also identified, referring to unmet supportive care needs in social protection.
Humanized Treatment
In the interviewees’ narratives, one of the primary unmet supportive care needs identified during the process of diagnosis of children and adolescents was the lack of humanized treatment by healthcare professionals. Caregivers report feeling neither listened to nor validated by healthcare professionals when they express concerns about signs or symptoms they consider abnormal in their children. This lack of attention, coupled with the perception of a lack of empathy towards children and adolescents among some professionals, creates barriers that hinder continuity of care and delay timely diagnosis. Therefore, participants emphasize the importance of humanized treatment that translates into active and empathetic listening.
They told me we have to send him to the regional hospital for a hemogram, where they give the results of the type of cancer he may have. He was two years and five months old, and I said no, I was angry with the hospital because I had had a bad experience, and so I didn’t want to go there. I said, ‘I need help in another hospital, they treated me badly in that hospital.’ (E1, south macro-zone) I was asking the doctor to please see him because the child began to deteriorate. And the doctors told me, literally, ‘your son is exaggerating.’ I started to cry, and I insisted again, Doctor, look how my son is. He was pale, he stopped eating. . .I knew he had something, so I took him to the emergency room again. I begged the doctor, I cried, I swear to you that my son is not like that. Three months later, they told me he had leukemia, and we were hospitalized. (E14, center macro-zone)
Notably, most interviewees recognize an improvement in healthcare professionals’ treatment once the diagnosis has been established and treatment has begun. However, some caregivers whose children are in adolescence report unsatisfactory experiences. In particular, they perceive that some healthcare professionals are not sufficiently trained to address the emotional, social, and communication needs of this stage of development.
But here [in the hospital], the staff is not even trained to show a little empathy towards a child with cancer. Because the children are little, they don’t understand much. By the time they enter adolescence, they have developed their character. (E12, center macro-zone)
Access to Information
In accordance with the preceding paragraph, access to timely, clear, and understandable information is essential for humanized treatment in pediatric oncology care settings. Based on the interviews, it is identified that providing information, both at the time of diagnosis and during treatment, significantly impacts the emotional experience, decision-making capacity, and establishment of a relationship of trust with healthcare teams.
The participants point out the need for prior knowledge about cancer to enable them to identify early signs and symptoms that could be related to childhood or adolescent cancer. From their experience, they warn that the general population, including medical personnel, is unaware of the early signs, which delays diagnostic suspicion and timely care.
[It is important] to inform the general population. I know that [child cancer] is something uncommon, but it happens. We have to be informed about [the symptoms]. . .For example, I never would have thought that my son’s symptoms could be related to cancer because they are very ambiguous. No doctor had ever told me, ‘Hey, we suspect it could be. . .’ so starting with the informational aspect is important. (E3, south macro-zone) I think it is very important the issue of information, of access to information. Dissemination: I even think it is relevant to get out of the bubble of those of us who know a little more, who are the mothers of children with cancer. Because suddenly, I mean, and I will give you my case clearly, when I saw my son’s symptoms separately, it would not have occurred to me, just in case, it is a cold, I do not know, at the most, anemia, you know? And then, putting all the pieces of the puzzle together, one says, ‘Maybe I should have worried before.’ (E6, center macro-zone)
On the other hand, once the diagnosis has been made, the interviewees state that there is still inadequate information on the disease, its treatment, and its evolution. In particular, they highlight a lack of guidance on the side effects of the therapies and the specific care they should provide to their children. This lack of communication forces them to insist on obtaining information, which leads to emotional exhaustion and the feeling that they are bothering the medical team. Sometimes, they avoid asking questions out of fear of causing conflict or negatively impacting their children’s medical care.
The following quote illustrates caregivers’ need for clear information and guidance regarding the diagnosis and treatment of cancer in children. It also shows that caregivers fear adverse reactions from healthcare professionals when asking for information, since doctors sometimes fail to explain in an assertive and understandable manner: I believe that information, above all [is key] to us, the parents. [We] have to go around chasing [healthcare professionals] to get them to explain things to us. For example, I always ask the oncologist, “Doctor, what are the risks of this [treatment]? What are the risks of this other [treatment]?” They respond with a shouted answer because that’s how they talk. So, the doctor says something, and you understand three percent of it. To me, I think what’s most important is that the information is very clear. (E8, south macro-zone)
Mental Health Support
According to the testimonies, it is evident that the diagnosis of cancer in a child or adolescent is a profoundly emotionally distressing process. Feelings such as fear, anguish, uncertainty, and sadness mark this process, which is also often accompanied by a prolonged period of physical and social isolation, as well as a sustained overload in the caregiving role. In this context, mental health support appears to be a critical unmet supportive care need.
The caregivers agree that although psychological care is available in some healthcare centers, it is usually focused on the children and does not systematically or sufficiently consider the caregivers. In many cases, they report that they have never received psychological care or that it has been sporadic and without follow-up. According to the participants, this is associated with a lack of human resources and a low institutional prioritization of the emotional dimension of support.
We have never had psychological support, never ever. They visit the children talk to them, but. . . the parents don’t even talk, I don’t know any parent who has told me ‘no, the hospital psychologist has the time to talk to us or ask how we are doing’, I don’t know what is going on. (E5, south macro-zone)
The need for emotional support is particularly intensified in cases where caregivers must move from their regions of residence and live for a prolonged period away from their homes and support networks. In these cases, geographic isolation is added to emotional isolation, generating a sense of loneliness that aggravates the psychological impact of the process.
It is hard to leave everything behind, especially when you have more children, do you understand me? It’s going to be three months now, I can’t see them, I can’t work, I can’t. . . and my life is from the foundation [civil society organization] to the hospital, and from the hospital to the foundation. . .Sometimes I still break down, I need to talk or give a hug. . . and no, I don’t have my family. I have to do with just a video call, with phone calls, and sometimes I don’t always have that. (E20, north maro-zone)
In addition to isolation, caregivers mention the prolonged exhaustion caused by the confinement imposed by treatment, the constant fear of infection, and the need to limit the family’s social life. These types of experiences, similar to those experienced by the general population during the pandemic, are the norm for many families of children with cancer, who see their routines, bonds, and family dynamics altered. The interviewees also emphasize that this mainly impacts women.
The isolation. . . Look, it’s like what everybody experienced with the pandemic. Having to live locked up and having to live in fear, that you can’t go out and you can’t receive visitors, all that is experienced by a family with children with cancer. . . many women were very lonely on the road, many absent fathers. (E11, center macro-zone)
On the other hand, one of the interviewees points to the lack of emotional support after the death of the children as a critical dimension not covered by the healthcare system. The mourning of mothers and fathers who lose their sons or daughters is not accompanied by institutional support, leaving them, in their words, ‘adrift’.
The issue of psychological help, both for the families that are going through this process and also for those who have lost their child. . . because we know that when their children die, the parents are only there, they have told me ‘I was left adrift, I lost my son, and now I am here adrift’. (E9, center macro-zone)
Social Protection
The interviewees identified economic needs as a persistent and ongoing challenge throughout childhood oncology care, even when state coverage is provided through the Explicit Health Guarantees (GES) regime. Caregivers report that, despite such coverage, they must assume multiple costs not considered within the guaranteed benefit, such as private transportation, special food, hygiene items, and other supplies associated with the daily care of children and adolescents. This situation is especially aggravated in cases where families must travel from regions other than the region where the treatment takes place, which also entails expenses associated with housing and living expenditures for long periods. It is also stressed that these costs are particularly challenging for women who must manage these processes independently.
[It is difficult]to support a family financially for a while, especially for women in economic matters, such as transportation, housing, food, and special food. [Additionally], people often stop working or get fired. There are social issues that remain unresolved, and I have the impression that no one will address them. Social organizations try to solve certain issues, but the volume is too high. (E17, central macro-zone)
From this perspective, an oncological diagnosis generates a profound disruption in the family economy, which can compromise the stability of the entire family group. In particular, many mothers leave their jobs to devote themselves exclusively to caring for their children, which is not always compensated by institutional support. Likewise, some caregivers—especially the ones who must go to another region—face this situation without support networks, with higher levels of social, emotional, and economic vulnerability.
I was alone; I didn’t know the city. I felt terrible, alone, because I was crying alone. We didn’t know where to stay. Then we remembered the foundation [civil society organization], and the truth is that it was indeed necessary [to seek the help of the organization]. In this organization, they bring us food, a roof, everything. So, they understood us, they reached out to us. (E20, north macro-zone) The support we have is very low. Even though we are in a hospital that gives us paid treatment, there are many needs regarding finances. Although they help them with medications and all those things. . .this is a costly disease because you go to oncology and they tell you, ‘you cannot eat this, you cannot eat this, you cannot eat this’. So, the options of things they give you so that your child can eat are too expensive, no pocketbook can stand with a child with cancer. (E18, center macro-zone)
From these testimonies, it can be seen that support networks—such as foundations or civil organizations—play an essential role in providing economic and housing support to families. However, these solutions are perceived as insufficient in the face of the magnitude of the needs. The experience of caregivers reveals that the perception of the cost of cancer treatment goes beyond the formal coverage guaranteed by the GES. These costs extend beyond medical expenses to include those related to private transportation, specialized food, hygiene products, and daily essentials. Additionally, there are costs associated with travel and accommodation if treatment is received outside the region where the family resides. Furthermore, there is a loss of income, particularly among mothers who leave their jobs permanently or temporarily to become caregivers. Women who travel with their children to a different region often face a lack of support networks. Therefore, a cancer diagnosis in a child can lead to significant destabilization.
Unmet Supportive Care Needs of Caregivers and the Role of Oncology Health Navigators
In general, the interviewees were not initially familiar with the oncology health navigator and their responsibilities. However, once the role was explained to them, many were able to recognize nurses who had performed these tasks and valued them as fundamental actors in their sons’ and daughters’ therapeutic process. The aspects that stood out the most were the continuous accompaniment, the clear explanation of treatment information, and the assistance scheduling medical appointments.
When she arrived [the oncology health navigator], it was a great relief. She takes care of making appointments and reminds us everything: ‘you have a hemogram tomorrow, mom, remember, you have to come at one o’clock. . .I don’t know, ‘here is the hospitalization order’. . .It is a great relief for me, and almost everything rests on her. (E6, center macro-zone) Yes, I always go to her [oncology health navigator] for information, I mean, she’s like the first one I ask. So, she guides me, she is like the channeler of all my consultations, my doubts. (E8, south macro-zone)
In this sense, the participants perceive the role of oncology health navigators as one with high potential for improving the quality of care and humanizing the care experience. Since this is a sustained accompaniment over time, caregivers particularly value the opportunity to receive this type of support, especially in contexts where they lack family or community support networks, which often occurs among those who must travel to treatment centers from other macro-regions of the country.
Many moms in my case don’t have support networks. In that case, [the oncology health navigator] is like a support network for oncology moms. Because that way one could communicate when necessary. (E12, center macro-zone)
In this scenario, oncology health navigators emerge as key figures in addressing the multiple needs of caregivers. Their role is not limited to clinical-administrative coordination—such as managing medical appointments—but can be expanded to include comprehensive support that includes emotional, social, and practical dimensions of care.
The interviews highlight that, in contexts where support networks are limited, the presence of an oncology health navigator becomes crucial in reducing the burden of navigating the healthcare system. Furthermore, a significant opportunity was identified for these professionals to articulate and strengthen ties between families and civil society organizations, especially those that offer material resources, emotional support, guidance, and accommodation. Given the numerous social protection issues expressed by caregivers that exceed the healthcare system’s capacity, strengthening connections between oncology health navigators and these organizations could be an effective strategy for providing more comprehensive, sustained, and humane support throughout the oncological trajectory.
Discussion
This study explores the unmet supportive care needs of caregivers of children and adolescents with cancer in Chile. The primary needs identified are related to a) humanized treatment, b) access to clear and timely information, c) mental health, and d) social protection. These needs coincide with those reported in the international literature (Møller et al., 2020; Neves et al., 2023; Nightingale et al., 2022; Reuvers et al., 2024), which is evidence of the shortcomings in the healthcare system’s ability to provide sufficient support to caregivers.
The narratives of the caregivers interviewed show that the diagnosis of childhood and adolescent cancer not only represents a disruption for the children but also implies a profound reconfiguration of family, affective, work, and economic dynamics, especially for women who assume the primary caregiving role. As has been documented in the literature, informal care in contexts of illness continues to be profoundly feminized (Montalvo et al., 2022; Orozco-Rocha et al., 2021; Pacheco Barzallo et al., 2024; Rolle Cáceres, 2023), a phenomenon that is reproduced in the pediatric oncology context, where it is mostly mothers who interrupt their work, social and personal trajectories to devote themselves entirely to the care of the child (Li et al., 2025; Reuvers et al., 2024). This pattern perpetuates traditional gender stereotypes and reinforces the structural inequality faced by women, who must assume the burden of unpaid care without receiving sufficient support from the health system or social protection (Paredes-Fernández et al., 2021).
Although in Chile there is guaranteed coverage through the Explicit Health Guarantees (GES) for the treatment of child and adolescent cancer, the interviews reveal the persistence of multiple unmet supportive care needs that have a direct impact on the therapeutic process and the quality of life of caregivers. These include housing, food, transportation, emotional support, psychological support, and access to clear and understandable information. These needs are exacerbated by territorial factors, such as living far from the treatment centers. In low-income families or those living far from care centers, the responsibility for care often relies on women who lack support networks and stable employment. Although advances have been made at the state level, such as the enactment of the SANNA Law (Law 21.063), which mandates insurance for working parents, and progress is being made toward a national care system, significant debt remains for those who provide full-time informal care. This is especially true for women who are not part of the formal labor market and therefore do not receive economic compensation for their work (ONU Mujeres, 2023).
The psychosocial impact of these intersecting structural and contextual conditions—territorial distance from treatment centers, gendered reliance on unpaid care with limited social-protection coverage, lack of clear information, and scarce psychosocial support—is profound and multifactorial. International and national evidence has documented that experiences of distress, isolation, uncertainty, and overload affect the mental health of mothers, and this, in turn, can negatively impact the emotional well-being of children and adolescents with cancer (Borrescio-Higa & Valdés, 2022; Cecilia et al., 2023; Lopez-Leon et al., 2023). Although some health centers give psychological support, the interviewees agree that these resources are scarce and insufficient to meet the emotional demands of both children and their caregivers. In this regard, the literature recommends systematically incorporating psychosocial assessment tools in clinical protocols to detect unmet supportive care needs and respond to the psychosocial distress of caregivers (Manikowski et al., 2022; Skrabal Ross et al., 2025).
Another key finding of the study is the role that civil society organizations play in addressing unmet supportive care needs. Organizations and shelters compensate for the shortcomings of the state and public healthcare system, for example, in terms of housing or guidance on medical processes, and provide spaces for emotional containment and mutual support. As evidenced in the literature, for many caregivers, these spaces become fundamental affective and community networks (Mensah et al., 2023; Rao et al., 2022; Sajjad et al., 2025). In this context, oncology health navigators emerge as key figures with the potential to articulate a more comprehensive response to the multiple unmet supportive care needs identified (Chan et al., 2023; Mohammed et al., 2024; Petts et al., 2021), taking into consideration the overload women usually have as primary informal caregivers. Although many interviewees were unfamiliar with this role, upon learning about its function, they acknowledged having interacted with professionals who provided guidance, accompaniment, and intermediation, highlighting its value in the care experience.
The findings of this study suggest that caregivers view oncology health navigators as a fundamental support figure, especially in contexts of geographic isolation or a lack of family networks, where a single person—usually the mother—must face all the demands of the process. In this sense, strengthening the role of oncology health navigators toward the function of accompaniment would not only ease the burden of navigation within the health system but also facilitate access to information, community support, linkages with civil society organizations, and respond more humanely to the unmet supportive care needs of caregivers.
It is essential to acknowledge that this study has limitations that should be considered. First, although the study aimed to represent different geographic regions of Chile, participation was uneven among caregivers from northern Chile. This disparity could hinder our understanding of regional differences in access to services and support. Second, all of the study participants were women. While this reflects a widely documented reality regarding the feminization of informal caregiving, the absence of male caregivers prevents us from exploring other experiences and possible gender differences in the exercise of the informal caregiving role.
Ultimately, understanding caregivers’ unmet supportive care needs is crucial for developing more responsive pediatric oncology services and crafting policies that account for the multifaceted nature of these needs. From a human rights and gender perspective—the same approach that inspired Chile’s recent caregiving policies (ONU Mujeres, 2023)—it’s crucial to recognize informal caregivers as subjects of rights. Ensuring adequate economic, social, emotional, and community support for people facing serious illnesses and their caregivers is crucial. This comprehensive perspective is essential for transitioning to more just, equitable, and family-centered health systems.
Implications for Practice
Our results suggest that pediatric oncology services should acknowledge informal caregivers as users of care and address their needs systematically throughout the care process. In this context, oncology health navigators can serve as a dedicated point of contact for families, providing orientation at diagnosis, facilitating the timely delivery of comprehensible information, coordinating appointments and referrals, and connecting caregivers with psychosocial resources and social protection benefits. Due to Chile’s macro-regional configuration, implementation should be flexible and tailored to each macro-region while promoting equity. This approach combines in-person support with tele-navigation to reduce travel burden and ensure continuity of care outside the center macro-region.
Conclusions
The results of this study show that, despite advances in biomedical coverage of childhood and adolescent cancer in Chile, there are still multiple unmet supportive care needs that directly affect those who assume the caregiving role, especially mothers. The caregivers’ experiences reveal an emotional, economic, and organizational overload that the health system or social protection policies have not sufficiently addressed. In this scenario, it is essential to broaden the view towards a comprehensive supportive care approach that recognizes and values the role of informal caregivers—emphasizing gender disparities—and promotes sustained support mechanisms. Promoting the strategic incorporation of oncology health navigators with a comprehensive approach could effectively articulate institutional and community responses, moving towards more humane, equitable, and family-centered care.
Footnotes
Acknowledgements
We gratefully acknowledge the generous participation of the caregivers and the valuable collaboration of the civil society organizations that supported this study.
Ethical Considerations
This study was approved by the Scientific Ethics Committee of Universidad del Desarrollo, Approval Number 2024-01. All participants gave written informed consent.
Author Contributions
BC, AO, FV, CC and ME, contributed to the study conception and design. BC, AO, FV, CC and AR contributed to the acquisition, analysis and interpretation of data. FV drafted the work and AO, BC, AR, CC and ME have substantively revised it. All the authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Center for Cancer Prevention and Control (CECAN), FONDAP (Grant Number 152220002), ANID.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available upon request from the corresponding author, BC. The data are not publicly available since they contain information that could compromise the privacy of research participants.*
Declaration of AI-Assisted Technology in the Writing Process
During the preparation of this work, the authors used Grammarly to review the manuscript’s wording. After using this tool/service, the authors reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.