
Abstract
Objective:
This study explores the supportive needs of informal caregivers of people with amyotrophic lateral sclerosis (ALS) in Switzerland.
Method:
We conducted semi-structured interviews with nine informal caregivers currently providing care to a person with ALS, 14 bereaved informal caregivers, and 13 healthcare professionals. Interviews were recorded on digital audio and analysed using an inductive thematic analysis within a realist framework.
Result:
Informal caregivers discussed five themes of support needs relating to being overburdened by administrative demand, in contact with healthcare providers, home support, especially during the terminal phase, and having or lacking social support. Healthcare professionals discussed three themes of support needs of informal caregivers which related to the general institutional support for informal caregivers, their own work as caring for informal caregivers, and the challenges in healthcare for families with ALS they encountered.
Significance of results:
Informal caregiving for people with ALS can be demanding. This study provides evidence for improvements in supporting informal caregivers. It shows administrative needs of informal caregivers, stresses their needs regarding advance care planning early in the context of ALS, and underlines the importance of social support, be it in peer-groups or community care.
Keywords
Introduction
Amyotrophic lateral sclerosis (ALS) is a terminal, neurodegenerative disease leading to progressive immobilization and paralysis. Due to its fatality, people with ALS (pwALS) need intensive and complex care. This essential care is most often provided by family and friends, the informal caregivers of pwALS.
Due to the high burden of care for informal caregivers 1 support needs have been studied in the context of ALS,2–4 particularly, challenges with diagnosis of ALS,5–8 healthcare service use, 2 psychosocial support,9,10 as well as palliative care and bereavement support11,12 exist. For instance, receiving the news of the fatal diagnosis can result in a ‘shock of diagnosis’ to the family system.5–8 After diagnosis, professional support for informal caregivers should be adapted to the specific caregiving situation.3,13 Many support needs of informal caregivers are met by other sources of support such as peer-groups and community help. 11 Informal caregivers and patients form a distinctive caregiving dyad, and personal characteristics and relationship dynamics play a role in how needs form out. 14
Caring for informal caregivers is part of the definition of palliative care by the World Health Organization. 15 Alongside the person with ALS, multidisciplinary teams at ALS and neuromuscular centres support informal caregivers.16,17 Further support comes from ALS patient organizations. 18
To the existing corpus of knowledge available on informal caregivers’ needs, this article adds new information using interview data. The article asks what supportive needs informal caregivers of pwALS have from the perspective of informal caregivers and healthcare professionals supporting families with ALS. We understand needs as capacities of informal caregivers to benefit from support. 19
Methods
Sample
The sample consisted of 9 current caregivers, 14 bereaved informal caregivers, and 13 healthcare professionals. The healthcare professionals included five physicians (palliative or hospice care, neurology, and general practice), three physio- or respiratory therapists (ALS clinic and private practice), and five specialized nurses (neuromuscular centres or private practice) providing care to individuals with ALS and their families. Informal caregivers were almost exclusively family members except one childhood friend, with an age range from 28 to 74 years. From the family caregivers, most were spouses or daughters of individuals diagnosed with ALS. Of the 23, nine informal caregivers were currently providing care to a pwALS. Informal caregivers were recruited purposefully through ALS clinics in the German-speaking part of Switzerland, through patient initiatives (Verein ALS Schweiz), peer contacts of former caregivers, and snowball sampling.
Informal caregivers contacted the interviewers via phone, mail, or email after having heard of the study through healthcare providers and handouts in peer-groups. With informal caregivers, interviews took place mainly in person in the participants’ homes to accommodate time and caregiving constraints. Healthcare professionals were mostly contacted in advance and interviewed via telephone. Interviewees were comprehensively informed about the study aims during informed consent procedure. In two interviews with current caregivers, pwALS were present and participated in the interviews. None of the interviewees dropped out of the study or refused to participate.
Interviews were conducted and digitally recorded after all participants had provided written informed consent. Interviews were between 25 and 130 minutes in length and interviews with healthcare professionals were typically shorter than interviews with caregivers. Each participant was interviewed only one time during the time of 2018–2020. Interviews were transcribed verbatim in Standard German using MAXQDA. 20 All quotations included in this article were translated to English from Standard German.
The interviewers were a female physician (MD) working in general practice and a male clinical psychologist (MSc) working in the academic setting. Both had prior practice in conducting qualitative research interviews or analysis and were repeatedly trained in qualitative data collection. The first four interviews served as a pilot for the semi-structured interview guide and the interviewers’ interview skills, which were supervised by a senior researcher. For informal caregivers, the interview guide comprised questions regarding practical supportive needs during caregiving, difficult situations, advance care planning, and end-of-life, as well as the time after bereavement (for more information see interview guides for all groups in the Appendix). For healthcare professionals, the interview guide centred on support for caregivers. The interviewers did not have any prior relationship to the research participants, nor did the participants have specific knowledge about the interviewers apart from general information about the project.
Analysis
We conducted an inductive thematic analysis within a realist framework by reporting “experiences, meanings, and the reality of participants.” 21 Correspondingly, we approached this by inductively coding segment by segment of the interview data. Segments consisted of units that relayed a meaning relevant for the context (usually one to three sentences).
Data analysis was performed in parallel to data collection. Data saturation was monitored while inductively coding and achieved when recurrent coding occurred. Data saturation was therefore understood as post hoc information redundancy achieved during data analysis. 22 Overall, 20 interview transcripts were coded by hand by teams of two to three coders (six coders overall) to satisfy inter-coder agreement of approach to the data. The remaining interviews were coded inductively using MaxQDA solely by the first author. Inductive codes were grouped by themes and subthemes. In the results section, we present the results from the analysis of interview of informal caregivers and healthcare professionals in two parts to provide a comparison of themes.
Setting
Cultural context is important in end-of-life research 23 and our study highlights needs within the Swiss context. This context includes a specific political and legal system influencing caregiving and the availability of financial and personal support, as well as specialist palliative care. 24 While healthcare costs within hospitals and outpatient services are covered by mandatory medical insurances, formal support at home is largely funded by local public institutions as well as out-of-pocket payments. 25 Publicly funded support at home is time limited resulting in a need to pay for private care.25,26 Welfare state support for family care is highly restricted. 27 Multidisciplinary care for people with ALS and their families is provided primarily within neuromuscular centres specialized in ALS as well as neurological hospitals. 17
Generally, most people in Switzerland want to die at home, but they die in nursing homes and hospitals. 26 Palliative care support is varied throughout the country due to the federalist structure.26,28 In 2013, 26 mobile palliative care teams existed while the European Association of Palliative Care recommends 80 mobile palliative care teams for Switzerland. 28 A National Strategy for Palliative Care 2010–2015 has addressed shortcomings of palliative care and paved the way for improvements throughout Switzerland. 29 However, still in 2018, a study reported shortcomings with regard to financial support for coordination of palliative care. 30
Ethics approval
The project was submitted for review by the cantonal research ethics committee (Ethikkommission Nordwest- und Zentralschweiz, EKNZ) through swissethics. As the project does not qualify as research with human subjects under Swiss laws, a certificate of non-objection was issued by the EKNZ. Despite not being subject to human research laws, we felt that it was necessary to uphold the standards required by the same laws of Switzerland, that is, having written informed consent of every participant, as well as storing data separately in a de-identified manner. Furthermore, no identifying information is presented in the article that could jeopardize confidentiality.
Results
Informal caregivers
Informal caregivers discussed five support needs: (1) administrative demand, (2) healthcare providers, (3) home support, (4) end-of-life support, and (5) social and other support.
Administrative demand
Informal caregivers highlighted the support needs with administrative demands. Vital was the importance of information about administrative tasks at hand, about available support options, being referred to the responsible institutions, and to have someone else perform administrative tasks.
A source of need was problematic interactions with insurance providers. During working age, informal caregivers, and patients in Switzerland have in principle access to invalidity insurance which allows them to access different lines of support. Caregivers noted regional differences and a need for openness and the willingness of services providers to support them. PwALS could get support through disability reimbursement which in turn provided the informal caregivers with additional respite help and financial aid. However, disability was assessed momentarily and only reassessed once a year. This means that help came sometimes too late for patients and informal caregivers (Table 1, quote 1).
Themes of supportive needs of informal caregivers.
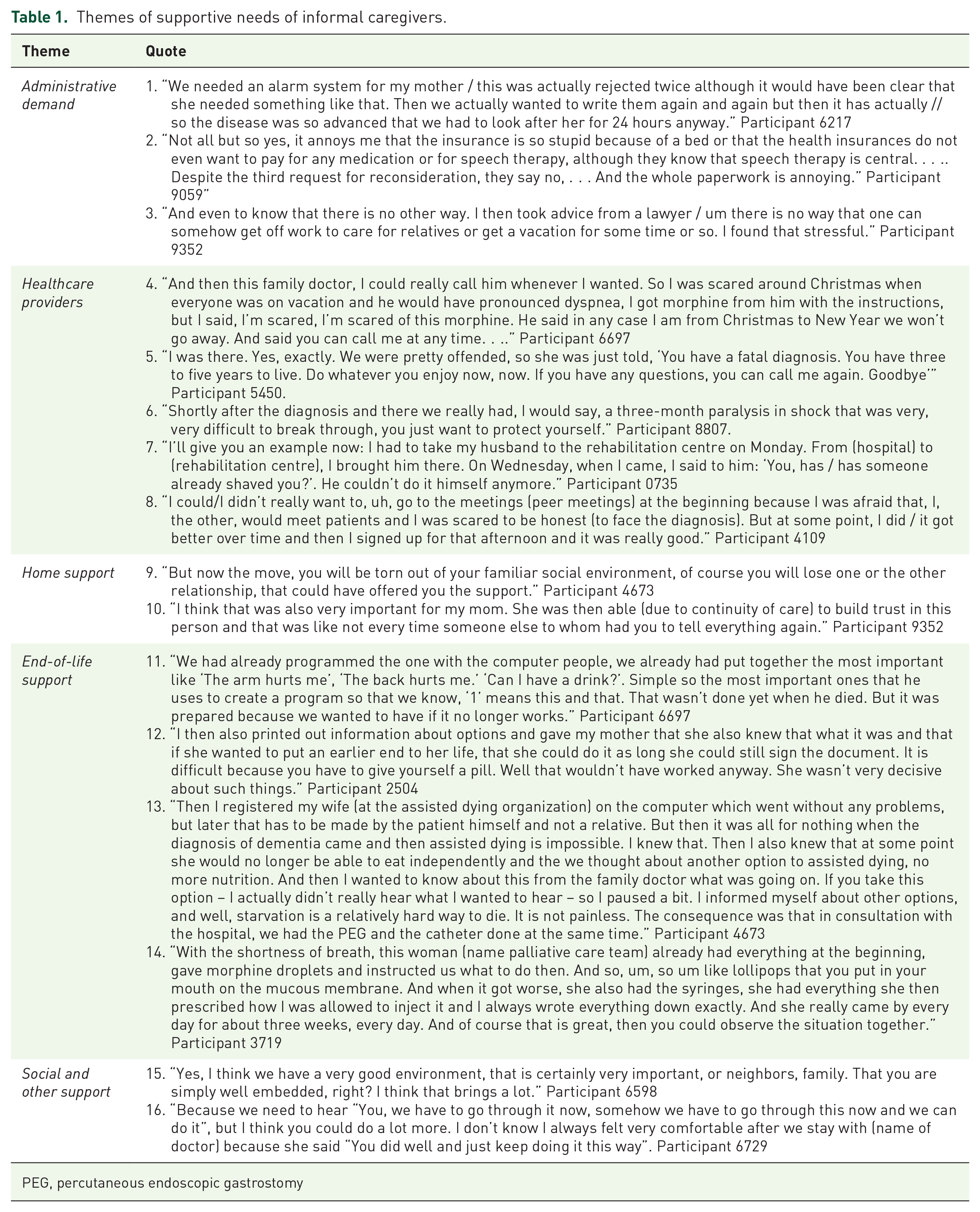
PEG, percutaneous endoscopic gastrostomy
For insurance, especially the transition from working to retirement age came as a predicament for caregivers. Many privileges associated with invalidity insurance were lost with old age insurance. Generally, informal caregivers viewed administrative work metaphorically as a fight, where they needed support (Table 1, quote 2).
Another source of need was work obligations; flexible working hours, an understanding employer, and supportive colleagues are needed. Self-employed informal caregivers had trouble finding people able to replace their positions. The lack of legal possibility to reduce working hours was mentioned by some informal caregivers, while others resolved this by taking sick leave (Table 1, quote 3).
Healthcare providers
Informal caregivers mentioned several needs in relation to physicians, for example, a need for a caring physician, especially during the diagnosis communication. Moreover, they expected engagement in the treatment and acting as a patient advocate. Especially family physicians were expected to perform this role, working as a contact point in the healthcare system (Table 1, quote 4).
However, some informal caregivers complained about the lack of information and empathic support following a diagnosis of ALS from physicians (Table 1, quote 5). Active engagement of physicians to coordinate care, ensure transfer to specialist centres, and clear communications with informal caregivers regarding time needed to deal with the diagnosis and coping in general were mentioned as important to have (Table 1, quote 6). Furthermore, informal caregivers mentioned that they needed support when pwALS avoided facing the diagnosis and its fatal implications.
When pwALS were hospitalized, some informal caregiver experienced patient-related needs which were not completely met (Table, 1, quote 7). Here, informal caregivers filled the essential gaps. Generally, healthcare professionals were needed to coordinate care and provide case management. Specialized support came through specialist nurses providing information, counselling, coordination, instruction, and key contact. Instructive modular care trainings were provided by them to informal caregivers every 3 months dealing with a variety of skills. Due to the modularity, informal caregivers sometimes missed certain training. For example, the progression of ALS was quicker than the availability of care trainings. Another problem was the emotional toll of these trainings (Table 1, quote 8).
For informal caregivers, proximity to ALS centre was of advantage. As pwALS becomes more immobile, the harder travel to ALS centres becomes. Hence, telephone support was highly valued.
Home support
Most of the care for pwALS took place at home and it must be adapted for that purpose. Informal caregivers discussed needs to make the home fit to provide care. There, support from architects was needed who knew about ALS and the progredient disability. A lift and wheelchair-ready cars were need for mobility. If they are unable to do these changes in their homes, they had to move. Moves are difficult because social support is then lacking (Table 1, quote 9).
At home, informal caregivers reported having and needing care assistants to provide them respite and difficulties finding experienced assistants. They communicated a lack of respite structures at home or outside. One of the most vital needs at home were support with specialized care aids to keep up with the deteriorating condition of pwALS. Often informal caregivers organized care aids too late, that is, by the time equipment was at home, the health of pwALS had changed so that the equipment is no longer needed or appropriate (e.g. wheelchair to electric wheelchair). Hence, informal caregivers expressed a need for a central depot of care aids that would address the changing needs of pwALS, as well as being able to get accessible financial support even if the care aids would only been used in the future. However, these kinds of depots were already used by other informal caregivers.
Competent homecare services were valued support but were often limited to a short period. For instance, homecare nursing support only came in the mornings and afternoons, while informal caregivers would require readily available round-the-clock care. Continuity and flexibility of care were both much desired, but often unmet (Table 1, quote 10). Due to immobility, therapies accessed by pwALS were increasingly delivered at home. Informal caregivers needed therapists and physicians to come to their home but only a part of physicians and therapists provided such services.
End-of-life support
For support in the terminal phase, informal caregivers highlighted the need to plan care in advance. This encompasses early organization and information as well as the opportunity to do so in the institutional context.
Informal caregivers needed help with communication in the later stages. While in their private life communication could often be established by family caregivers and pwALS, in the healthcare systems problems were encountered when healthcare professionals equated communication incapacity with stupidity or dementia. Here, information and training for involved personnel was considered as a need as well as early integration and calibration of electronic communication devices, including integration with ventilation devices (Table 1, quote 11). Generally, ventilation was a situation of need for caregivers with patients being afraid of dying of dyspnoea pointing to a gap of information about palliative care. There were problems with non-invasive ventilation, especially when pwALS could not remove the mask.
A key mistake that bereaved caregivers spoke about is planning too late. Informal caregivers needed earlier and clear communication of possible medical interventions and end-of-life options as well as of support with prognostic uncertainty. Problems were the decision-making capacity as well as when pwALS left it to the family caregivers to decide or were not decisive (Table 1, quote 12).
The end-of-life was characterized by increased need for support. Informal caregivers were significantly involved in decision-making surrounding decisions that pwALS had protracted during their illness like insertion of a feeding tube and invasive ventilation, as well as in end-of-life decisions (e.g. deep sedation and termination of ventilation). As many of the decisions rendered by pwALS hinged on the provision of care at home, informal caregivers were key and often decided together with or in place of pwALS (Table 1, quote 13). Here, they needed time to weigh all the options and get support through specialist palliative care teams (Table 1, quote 14). During these decisions, feeling supported and not alone was vital. If the place of death was not the home, some informal caregivers reported having a hard time finding a suitable institution to support pwALS at the end-of-life.
During the end-of-life stage, informal caregivers report emotional needs. Thus, early access to psychological and spiritual care were necessary support needs, as well as the activation of resources needed to provide care.
Social and other support
Social support from other family members and friends was very important for informal caregivers. Their social network needed to have knowledge of ALS’ intricacies and being able to accept ALS. Often, informal caregivers had problems if their friends feared ALS and withdrew from contact. In their communities, informal caregivers valued if neighbours helped them out (Table 1, quote 15).
Societal factors played a big role; while informal caregivers noticed that knowledge about ALS has improved in the last 15 years, there was not extensive knowledge even among healthcare professionals. Informal caregivers valued if healthcare professionals recognized the work of caregivers (Table 1, quote 16).
When asked directly, informal caregivers remarked that they in general need more holistic support, being met where they stand regarding ALS, someone to talk to, specific situations of care (e.g. waking up to accompany pwALS to the toilet), friends for moral support and someone to take the initiative to care for them.
Healthcare professionals
There are three themes delineating support needs of informal caregivers from the analysis of the interviews conducted with healthcare professionals: Institutional support for informal caregivers, professional care for caregivers, and challenges in healthcare for families with ALS.
Institutional support for informal caregivers
Healthcare professionals discussed the importance of support offered to informal caregivers, by themselves and other professionals. Depending on their professional role, they described their professional responsibilities. Specialized nurses reported a variety of general task and being involved from diagnosis. They also reported visiting families at home, planning, and coordinating care at home and providing case management. Healthcare professionals provided care within a network (Table 2, quote 1).
Themes of support of healthcare professionals.

ALS, amyotrophic lateral sclerosis.
A valuable source of support for informal caregivers is assistants for daily help. Healthcare professionals highlighted the need for specialized medical care; this encompassed early integration of palliative care, adapted to the needs (Table 2, quote 2).
Generally, healthcare professionals reported how support of informal caregivers depended on the demand for and acceptance of support. Professional caregivers noted how support for financial and administrative needs was often lacking, especially regarding social insurances.
Support offers identified by healthcare professionals ranged from organizing care aids and appliances, instructing, and supporting involved care teams, and organizing respite services. They point to the need for more volunteers to provide respite care, peer groups, and self-help groups in the context of ALS (Table 2, quote 3).
The end-of-life was marked as a crucial phase of support. Healthcare professionals mentioned different lines of support for informal caregivers and pwALS (mobile palliative care, hospice care, and assisted dying), but also lack of institutions for long-term care, especially with invasive ventilation (Table 2, quote 4).
Professional care for informal caregivers
Professional caregivers from multiple disciplines stated that support for informal caregivers started when first meeting the family, often after diagnosis. Healthcare professionals highlighted the burden informal caregivers had to deal with as they saw the disease progress (Table 2, quote 5).
Support through the disease course, advice, and counselling were identified as key task where professional caregivers met needs of informal caregivers. Furthermore, professional caregivers revealed their role as advocates of patients and families, as well as providing recognition of the work done by informal caregivers. Being trusted by informal caregivers was central in caring for them.
Healthcare professionals highlighted the fatality of ALS and the need for a professional role understanding, encompassing both compassion and professional distance. They reported doing unpaid work because they needed time for extensive counselling (Table 2, quote 6).
Most professional caregivers reported having learned to support patients and families with ALS by ‘learning by doing’. While some had extensive training before coming to support families, they also noted how the novelty of support for ALS required constant training, education, and information (Table 2, quote 7). In turn, professional caregivers informed, trained, and instructed informal caregivers and thereby meeting their needs.
The care the professionals provided which addressed the supportive needs of informal caregivers was orientated towards the resources of informal caregivers and was planned out proactively in advance. Especially decision-making and planning in the later stages was a key activity where professional caregivers supported caregivers. Other supportive activities included planning and coordinating medical care, setting up advance directives, preparing the caregivers and pwALS for impeding death by talking frankly with them (Table 2, quote 8). Professionals regarded the possibility to visit families at home to observe the situation as important, as well as the advantage of continuously providing care for pwALS.
Challenges in supporting families with ALS
Healthcare professionals identified a range of challenges when supporting family caregivers and pwALS. In itself, working with the difficult diagnosis of ALS was perceived as burdening as well as a learning experience from different ways of coping with a fatal illness. Most often a first challenge was when the contact with the families came too late, and there was severe disability and an inability to plan ahead (Table 2, quote 9).
Neurocognitive and behavioural impairments of pwALS were noted by healthcare professionals as particularly troubling for informal caregivers (Table 2, quote 10). Healthcare professionals remarked how neurocognitive impairment might influence the caregiving relationship.
The end-of-life gave rise to challenges and moral dilemmas. Dying and planning in advance for death were viewed as different depending on the cultural background. Ventilation, both non-invasive and invasive, was a key issue (Table 2, quote 11). Professionals noted problems with mask ventilation in ALS and most notably, problematized invasive ventilation by tracheostomy in the restricted healthcare context of Switzerland. Care at home until death was viewed as costly and burdening, where round-the-clock care was needed and had to be organized, as well as the implications of high symptom load for all involved were discussed. Professionals viewed communication at the end-of-life as a key challenge within palliative care. In contrast to palliative care in oncological patients, palliative medicine in the context of ALS was viewed as more complex and symptomatic treatment as difficult to control at times. Wishes to die and wishes to hasten death portrayed situations where professionals reported having difficulty.
Generally, challenges reported by healthcare professionals were the voluntariness of caregiving, as well as the gendered nature of caregiving in ALS with women providing the majority of care, and the problems arising from societal challenges such a lack of financial resources in the healthcare sector. In addition, financially burdened families were a challenge for professionals. That is, they underlined that fact that for families, financial support was missing to pay for care aids and appliances as well as respite workers. From the perspective of institutions, resources for home care professionals, home visits, and night support were lacking. For their own work, professionals problematised interdisciplinary cooperation and the lack of supervision (Table 2, quote 12).
Discussion
Both interviews with informal and professional caregivers stressed the need for early care and advance care planning, depending on the needs and resources of the families. Both groups also converge on the idea of the importance of social support, be it in peer-groups or community care. The value of support through peers is a common finding, for example, in a recent study by de Wit et al. 31
From caregivers and healthcare professionals, administrative demand is seen as a need where caregivers would appreciate support, especially when such support could result in avoiding time-delayed resources, financial, and otherwise, offered by the welfare state. de Wit et al. 31 write for the Dutch context that this work ‘is generally time-consuming and bureaucratic, whereas the need is often urgent’ (p. 195) with which our data concur.
The home as a central place of care brings with it specific supportive needs. The decision to care at home until death of pwALS is highly depended on several factors. These include knowledge of and skills in early advance care planning including emergency plans tailored to the disease and individualized goals of care, the availability of respite care and palliative care support when needed, as well as informal caregivers being able to take the time to provide such care. These results map well onto the existing qualitative data.32–34 Professional caregivers offer home visits but also point to the difficulty to finance such visits and to finance complex palliative care at home. Similar to the study by Galvin et al., 35 external support and services and patient-related behaviour were key support needs reported by both informal caregivers and healthcare professionals. Psychological support was not mentioned as a need by informal caregivers in our study. On one hand, it could be possible that informal caregivers did not consider themselves being in need of care as they restricted the scope of their tasks to daily caregiving. On the other hand, given the absence of evidence for psychosocial interventions 36 and the lack of time caregivers have may indicate that psychological support might be only needed in specific circumstances, for example, complicated grief in bereaved caregivers. 37
Our results have implications for provision of care and support for informal caregivers in Switzerland. One is that the role of family physician is crucial. Alvarado and Liebig 38 show that general physicians lack opportunities to acquire the needed skills for palliative care. For ALS, these skills need to include advance care planning and serious conversations around severe illness and death. However, as general physicians might only see few ALS patients, they may act more as an intermediary and contact person and bring in specialist palliative care.
Future research on palliative care in Switzerland is still needed. 30 Financing and educational opportunities for palliative care are highly varied in the Swiss cantons resulting in different experiences of informal caregivers in our sample. The Swiss national palliative care strategy 2010–2015 has improved the situation of caregivers as shown by the availability of mobile palliative care services supporting some informal caregivers in this study. Low-threshold psychosocial interventions for informal caregivers demand more research. While informal caregivers valued ALS-specific peer group meetings, infrequency of these meetings gives rise to a need for continuously available support. Volunteers trained in palliative care, 39 ideally with experience in ALS, might be an example of low-threshold support that could be organized regionally. In addition, the availability of professional respite support seems crucial to enable caregiving.
Healthcare professionals highlighted different challenges for informal caregivers, notably neurocognitive impairments, and implications upon the caregiving dyad. This issue was not brought up by informal caregivers. It is possible that these are implicit factors in relationship which are easier viewed from the outside or that the informal caregivers involved did not have or want to voice these issues. It might also be that healthcare professionals have learned to recognize signs of neurocognitive impairment, while family caregivers normalize impairments. This demands more research as there is evidence that behavioural impairments particularly relate to the subjective burden of caregiving. 40
Finally, this study adds to the literature on needs of informal caregivers of pwALS and the need to tailor interventions to each unique family system. Some informal caregivers brought up privacy concerns for external help, while others would have been most thankful for it. Hence, supporting informal caregivers for pwALS needs to be highly adapted to their needs.
Limitations
This qualitative study is necessarily limited, as our data are not generalizable. Caregiving is a context-dependent activity (e.g. cultural background, welfare-state support), and these results should be viewed within the Swiss context. In addition, the participants were sampled by purposive sampling, and this necessarily selects for informal caregivers who felt able to give an interview (e.g. where not overburdened or amid severe grief). Furthermore, while our interview questions were open and varied, social desirability might have played a role in the interviews (e.g. refraining from talking about socially undesirable feelings towards pwALS).
Conclusion
This study outlined supportive needs of informal caregivers in Switzerland. While supportive needs are highly individual, our study highlights the importance of catering to the administrative needs of informal caregivers, stresses caregivers’ needs regarding advance care planning early in the context of ALS, and underlines the importance of social support, be it in peer-groups or community care.
Footnotes
Appendix
Acknowledgements
The authors want to thank wholeheartedly the participating informal caregivers and healthcare professionals. Furthermore, they are indebted to Martine Verwey, Luzia Iseli, and Prof. Dr. Bernice Elger who have supported the project.
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project on ALS informal caregivers’ needs is funded by the Swiss Academy of Medical Sciences (grant no. SAMS PC 21/17).