
Abstract
In Italy, the Family and Community Nurse (FCN) was officially recognized with Legislative Decree 34/2020 and redefined by Ministerial Decree 77/2022. The introduction of the FCN has been inconsistent across the nation, leading to fragmented experiences and challenges in fully integrating the role into the healthcare system. Based on Cohen’s hermeneutic approach, this phenomenological study explores the lived experiences and meaning of being an FCN in Italy. Semi-structured interviews were conducted from December 2023 to June 2024. Interviews were transcribed, read in-depth and analyzed. Thirty-seven FCNs from four Italian regions were interviewed. Four main themes were identified: (a) Navigating elderly care complexity; (b) Education as a core function; (c) Being a node in the healthcare network; (d) Establishing the FCN identity through role differentiation. Being a FCN means managing complex needs, ensuring continuity of care, and collaborating effectively with the other primary care providers. FCNs distinguish themselves from task-oriented home care nurses by embracing a proactive approach, gaining greater organizational autonomy and actively shaping their professional identity. The implications for practice suggest the need to support FCNs in this consolidation phase through health policies that enhance their contribution to community care.
Introduction
The growing complexity of health care needs, combined with demographic pressures, has necessitated a structural rethinking of current care models, increasingly shifting towards an integrated and community-based approach (World Health Organization [WHO], 2018). Primary care (PC) represents a global approach that considers multiple factors influencing population health, including social, economic, and environmental aspects. It aims to strengthen and refocus national health systems, bringing health and well-being services closer to the community (WHO, 2022).
In 2000, the WHO outlined the role of the Family and Community Nurse (FCN) as a professional capable of supporting individuals in adapting to illness and chronic conditions and providing care within their life context, including family and community settings (WHO, 2000). FCN delivers complex nursing care, promotes health, and engages in the prevention and participatory management of individual, family, and community health processes, working within PC settings (Dellafiore et al., 2022). The value of the FCN has been widely recognized, particularly for its proactive role in care delivery (Mathews et al., 2021) and its advocacy function within interprofessional healthcare collaborations (Marcadelli et al., 2019).
This collaborative dimension is also reflected in several PC nurses’ roles that, although structurally and functionally distinct from the FCN, share a strong emphasis on interprofessional collaboration (WHO, 2022). Such collaboration develops in settings where the integration of care across both emergency and primary care services is achieved (Rasku et al., 2021), and where nurses are afforded the opportunity to assume advanced responsibilities, including diagnosis and prescription (Andrews et al., 2021). Despite differences in competencies and educational pathways compared to the FCN, the roles of PC nurses underscore a broader trend: the expanding function of nursing professionals as mediators between patients and General Practitioners (GPs), who often serve as the main gatekeepers to the healthcare system, particularly in areas such as health education, prevention, and continuity of care.
In Italy, the FCN was officially recognized with Legislative Decree 34/2020 (Italian Republic, 2020), and subsequently redefined by Ministerial Decree 77/2022 (Italian Republic, 2022), identifying it as a key component of the reorganization of PC. In support of the implementation of this role, the National Agency for Regional Health Services (AGENAS) developed guidelines to guide the Regions in integrating the FCNs into Local Health Authorities (LHAs), specifying the main functions, levels of intervention, training, and competencies required for professional practice (National Agency for Regional Health Services [AGENAS], 2023). According to an exploratory survey conducted by the AGENAS in 2021, 26 out of 38 responding LHAs (68%) reported having implemented the FCN role, for a total of 1,062 professionals employed across the country. All FCNs were attending specific training programs, including university master’s degrees, regional courses, or LHA-based training (Martini et al., 2021). Significant differences persist across regions not only in workforce numbers but also in the types of training and in the organizational models adopted, reflecting broader variability in service delivery. Despite some examples of effective adoption (Rocco et al., 2017; Taddeucci et al., 2023), the FCN role’s introduction remains uneven across different regional contexts in Italy, often accompanied by a lack of professional recognition. These challenges are not unique to Italy; similar patterns have been observed in other European countries, where the introduction of the FCN role has been uneven and hindered by systemic barriers often intensified by healthcare emergencies (Busca et al., 2021) and context-specific implementation issues (Conti et al., 2021). A recent study by Sánchez-Muñoz et al. (2024a) highlighted that FCNs integrated into PC teams in Spain face a lack of professional recognition (Sánchez-Muñoz et al., 2024a), even if the implementation of FCNs started many years before (Martínez-Riera, & Rodríguez, 2019). This issue is attributed not only to the limited awareness of their role, at both the institutional level and among other healthcare professionals, but also to the misalignment between their competencies and the actual opportunities to apply them in community care activities (Sánchez-Muñoz et al., 2024a).
The existing literature has primarily focused on the regulatory framework and the potential of the FCN role (Barisone et al., 2023; Marcadelli et al., 2019), with particular attention to nursing managers’ perspectives on the impact of the FCN on professional teams and, more broadly, on public health (Sánchez-Muñoz et al., 2024b). However, to date, there is a lack of study exploring and describing the direct field experience of FCNs implementation.
To the best of our knowledge, no studies have thoroughly explored the experience and meaning of being an FCN in Italy. Giving a voice to professionals is crucial to fully understanding their role two years after the issuance of Ministerial Decree 77/2022. Gathering experiential insights can inform about the implementation process and how the role of nursing is shaping in the community setting of the post pandemic era. Moreover, such understanding can enrich the global debate on how nursing is evolving to meet emerging needs through new community-based models and innovative roles in PC settings.
Research Objective
This study aimed to describe the experiences and meaning of being a FCN in the Italian context.
Methods
Study Design
This study was conducted using Cohen’s phenomenological methodology, which integrates both descriptive (Husserlian) and interpretative (Gadamerian) approaches (Cohen et al., 2000). This dual perspective was especially appropriate for exploring the lived experiences of FCNs and the meanings they attach to those experiences within their unique professional and cultural contexts. Cohen’s approach also informed the study design by guiding the development of open-ended, reflective questions that encouraged participants to share rich and detailed narratives. Its emphasis on meaning-making and lived experience makes it particularly well-suited to nursing research, especially in areas that are still underexplored. Aligned with the EPPiC framework (Emphasis, Purposeful sampling, Phenomenon of interest, Context) (Kalu, 2019), the phenomenon of interest was family and community nursing, with a specific emphasis on exploring the meaning of being an FCN within a context shaped by recent post-COVID investments in PC and by a nationally framed – yet regionally fragmented – healthcare system.
Participants and Recruitment
Participants were recruited between December 2023 and May 2024 using purposive and snowball sampling, whereby initial participants, identified through the Association of Family and Community Nurses (AiFeC – https://www.aifec.it/), were invited to nominate other eligible individuals (Parker et al., 2019). They were contacted by phone and/or email and provided with a detailed explanation of the study. Once informed consent had been obtained, interviews were scheduled via Voice-over Internet Protocol (VoIP) at a time and date convenient to each participant.
Given the variability of Italian contexts, participants were purposely selected using maximum variation sampling at a regional level to ensure an adequate representation of North, Central and South Italy. Emphasis was placed on information-rich cases rather than numerical representativeness, consistent with Sandelowski (1995). The geographical classification adopted, reflects well-established economic and socio-cultural distinctions (National Institute of Statistics [ISTAT], 2023). These macro-areas (North, Central and South Italy) differ in terms of population ageing rates, availability of health and social services, and socio-economic conditions, which may influence both the experiences of FCNs and the needs of the populations they serve. The participants were FCNs working in Italy who expressed a willingness to participate in an interview. Those who worked in clinical settings other than the community context were excluded.
Data Collection
Semi-structured interviews were conducted from December 2023 to June 2024. Before conducting the interviews, the research team engaged in a bracketing process, critically reflecting on and making explicit their own preconceptions, to set them aside and remain open to the meanings conveyed by participants (Cohen et al., 2000). Interviews were carried out by a nurse researcher with extensive experience in qualitative research (AD), a nurse doctoral student who was trained in qualitative research (IS) supported by a trained researcher from an external research organization with long experience in sociological studies. The involvement of professionals with different backgrounds was intended to ensure adherence to the study protocol, enhance credibility, and support researcher triangulation. All interviews were conducted in Italian, the participants’ native language, and audio-recorded via Google Meet, a video communication service developed by Google.
The research team designed the interview guide to get the experience and meaning of being a FCN. The guide proposed by Roberts (2020) was initially adopted for the interview development as a learning tool for the novice researcher (IS). The interview was subsequently refined in accordance with Cohen’s approach and intentionally designed with broad, open-ended and flexible prompts to foster a dynamic interaction between interviewer and participant (Morse, 1991). Data collection was therefore shaped by an emphasis on depth and meaning making, with the researcher actively engaging with participants’ perspectives while remaining reflexive. This approach encouraged authentic dialogue, allowing participants to freely express their perspectives.
Prior to data collection, the guide was tested by two FCNs who were not included in the final sample. The interviews started with a welcoming attitude and an initial open generic question to start the conversation, then continued with the more specific questions about the role, the experience and the scope of practice reported in the interview guide (Box 1).
Interview Guide.

Each participant was interviewed separately to prevent reciprocal influence, especially for those working in close-knit settings. Through video call interviews, field notes were taken, replicating the characteristics of classic face-to-face interviews (Janghorban et al., 2014). After the interviews, participants’ sociodemographic data were collected using an ad hoc questionnaire. Audio recording was conducted only after obtaining explicit consent from each participant.
Data Analysis
Once transcribed verbatim, the interviews were checked for accuracy by spot-checking, using a subset of the transcripts (10 of 41). Given the substantial volume of data, this approach allowed for efficient resource utilization while maintaining high-quality standards (MacLean et al., 2004). The high consistency observed between the transcripts and the original audio recordings provided sufficient confidence in the overall transcription quality, thereby rendering a full review of all transcripts unnecessary. All interviews were uploaded into NVivo® software 12.
Data analysis was conducted after data collection was completed, following Cohen et al.’s (2000) hermeneutic phenomenological methodology. In line with this interpretative approach, the adequacy of the data was assessed based on the richness, variation, and completeness of participants’ experiential accounts. Although data analysis began only after interviews had concluded, the size and composition of the sample – purposively varied geographically but sharing a common experiential grounding – allowed for the identification of conceptually dense and recurring patterns. No additional variation in the meaning of the phenomenon was observed in the final interviews, leading the research team to judge that a sufficiently deep and coherent understanding of the lived experience of FCNs had been achieved (Van Manen, 2023).
The transcripts and field notes were first read as a whole by two researchers (IS and MS) independently, in line with Cohen et al.’s (2000) hermeneutic phenomenological approach. They were then re-read in depth, line-by-line, to extract relevant contents and assign tentative theme labels to various passages. Once the whole was understood, data segments were examined at a deeper level to refine and consolidate the themes, with dialogue between researchers ensuring trustworthiness. Trustworthiness was also supported by returning to the original data in case of discrepancies.
To ensure dependability, an external expert researcher nurse (AD), not directly involved in the analysis process, assessed the adequacy of the data and the preliminary results obtained, verifying the accuracy of the findings. To address reflexivity, bracketing was undertaken as an ongoing process, particularly prior to conducting the interviews and data analysis, to acknowledge and critically reflect on preconceived notions and their potential influence (Cohen et al., 2000).
To ensure credibility, all members of the research team reached a consensus on the final organization of themes and their content justifications. During the interviews, opportunities for member checking were also incorporated, allowing participants to clarify or expand on their accounts and to ensure that their perspectives were authentically represented in the developing interpretation (Cohen et al., 2000).
Finally, two authors (IS and EB) compiled the themes into a report to present the findings, incorporating quotes (interview number, sex, and age) as exemplary evidence for each theme. One researcher (IS) translated the identified quotes into the target language (English) and another (EB) back-translated them into the source language (Italian). These two steps were repeated as necessary until the target language was acceptably equivalent to the source language. Both translators have a high understanding of both the source and target languages, and are familiar with the concepts under study (Chen & Boore, 2010).
Ethical Considerations
The study complies with the Declaration of Helsinki. Ethical approval was obtained from the Novara Ethics Committee before the study began (n°CE307/2023). The research team contacted eligible patients, informed them about the study, and asked for their verbal consent to participate, which was audio-recorded. To ensure participant anonymity, no identifiable information was included in the transcripts. Digital audio recordings were securely stored on the University of Piemonte Orientale server and deleted after transcription.
Findings
Thirty-seven participants meeting the inclusion criteria were interviewed. They were drawn from four regions: two in the North, one in the Centre, and one in the South of Italy. The majority were female (n = 33, 89%). The mean age was 42 years. All participants worked in public sector facilities. The main sociodemographic data are reported in Table 1. The interviews lasted an average of 50 min (range: 35–70 min), excluding the time for introductions and greetings.
Socio-Demographic Data of Participants.
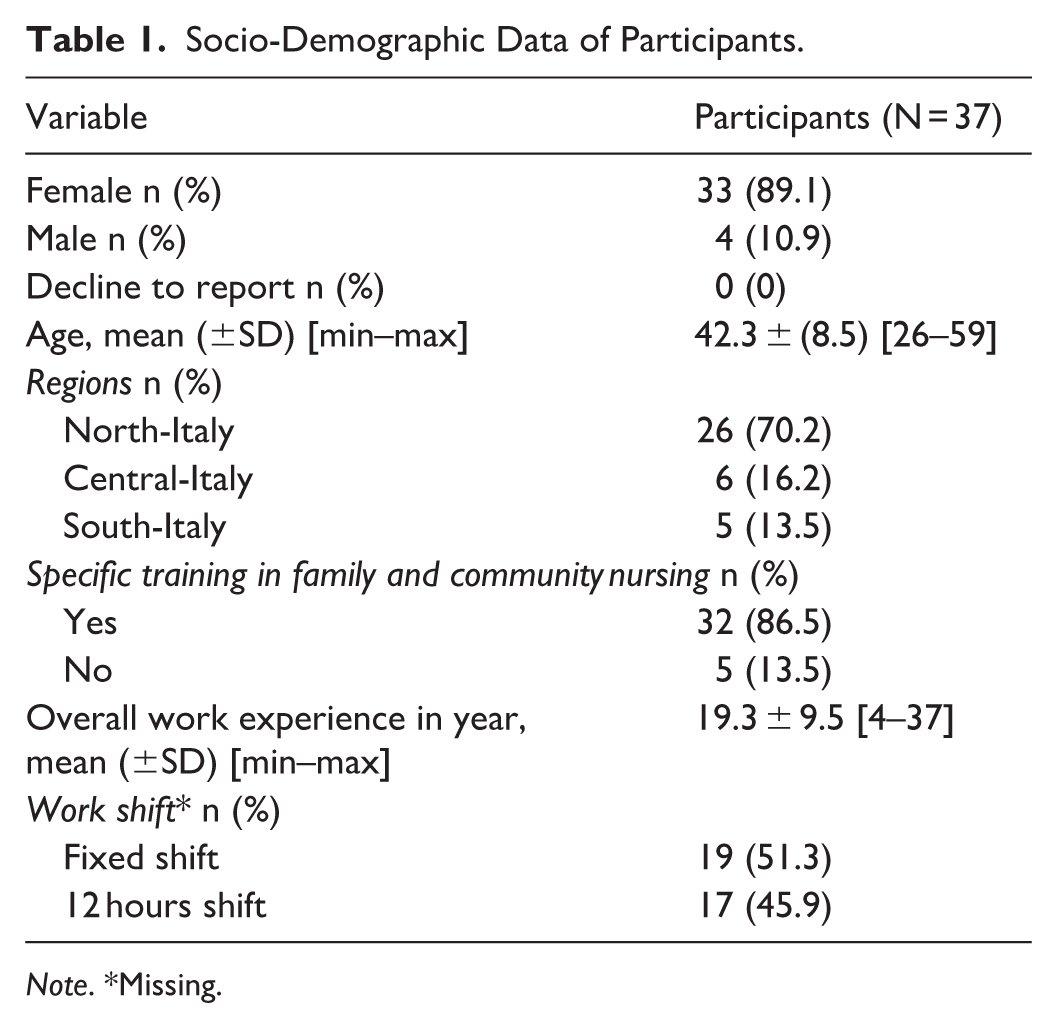
Note. *Missing.
Four main themes were identified: (a) Navigating elderly care complexity; (b) Education as a core function; (c) Being a node in the healthcare network; (d) Establishing the FCN identity through role differentiation. The themes reflect how FCNs experience and make sense of their evolving professional identity, as well as of their role within the broader national healthcare system, shaped by recent post-COVID reforms and by the challenges of a nationally framed yet regionally fragmented context.
Theme 1: Navigating Elderly Care Complexity
This theme reflects how FCNs make sense of their evolving role in the face of complex and often layered needs of older adults, intended as individuals aged 65 years and older. While participants described caring for individuals across all ages, their narratives revealed that working with an aging population was a central and demanding aspect of their practice. The care complexity emerged not only from the health conditions faced by older adults but also from the broader social and relational contexts in which care is provided. Participants recognized that working with an aging population required a deep understanding of individual’s needs, which extend beyond healthcare to include psychological, social, and economic factors, as illustrated by one participant: ‘Most of the people we care for are older adults who can no longer live independently’ (Int.39, M, 41 years).
Care delivery involved not only managing chronic illnesses and disabilities but also addressing challenges such as social isolation, loss of autonomy, changing family dynamics, and financial difficulties. The multifaceted nature of these needs necessitated an integrated approach, involving collaboration with other professionals and a strong commitment to ensuring continuity of care. This translated into regular and ongoing monitoring, aimed at ensuring that patients did not feel abandoned, particularly after nursing interventions had concluded. One participant emphasized that: ‘They are discharged in terms of services, but from the perspective of care management, many patients are never actually discharged’ (Int.25, F, 39 years).
Continuous monitoring through regularly scheduled appointments is not just a care practice; it is also perceived as a central element of the caregiver-patient relationship: ‘We schedule predetermined appointments, follow-up, exactly like a check-up visit, which we decide together with the patients, whether I need to see them or they need to see me’ (Int.10, F, 47 years). FCNs highlighted how caring for a patient with complex needs involves the timely identification of expressed and unexpressed needs and collaborative networking, as well as the active involvement of the caregiver. One participant reflected on this issue, describing a case where the caregiver’s lack of awareness affected the patient’s health: We understood that the daughter hadn’t grasped the importance of weight because the mother was usually a person who did not develop edema, so she didn’t notice it [edema], but [when this occurred] the patient would immediately experience respiratory difficulties. So, what did we do? We started from zero, retraced the entire process, and established a weight cut-off and a diuretic for emergency cases (Int.32, F, 46 years).
Theme 2: Education as Core Function
Across all interviews, FCNs reflected patient education as a fundamental aspect of their professional role, understood as a dynamic process of informing, guiding, and empowering patients to enhance their understanding and management of health conditions. Participants emphasized the importance of patient empowerment, highlighting supportive activities aimed at fostering awareness, autonomy, and the ability to recognize and utilize one’s own personal resources. In some cases, even technical procedures, such as dressing changes or blood sampling, serve as opportunities for educational interventions. During these procedures, nurses can assess the patient’s adherence to previous instructions and reinforce key educational messages. One FCN explained: ‘For example, with a patient who has diabetes but also an ulcer, we provide both education and monitoring as well as perform the dressing’ (Int.40, F, 35 years).
FCNs are pivotal in promoting prevention and supporting the patient towards greater awareness of their health status. While much of their educational work focuses on older adults, participants emphasized that health education should not be confined to a single age group. Instead, it should adopt a life-course perspective, addressing individuals at all stages of life. In fact, a small number of FCNs shared their lived experiences of engagement in school settings, describing health promotion activities, such as hand hygiene education, as meaningful extensions of their role in fostering wellbeing. As highlighted by one participant, health education plays a key role from childhood: ‘If we work on preventing unhealthy lifestyles among young people, the children of today and the youth of today will be the adults of tomorrow’ (Int. 17, F, 51 years).
The essence of educational interventions lies in empowering patients to manage their health independently. The goal is to gradually reduce dependence on healthcare professionals, allowing them to serve as a source of support and guidance rather than a constant presence. One participant stated: ‘Surely, a nurse should eventually become unnecessary, in the sense that if the job is done well, at some point, I am no longer needed’ (Int. 18, F, 31 years).
Beyond fostering patient autonomy, another key objective is facilitating behavioral change by helping patients modify lifestyle habits that could negatively impact their health. However, change is not always immediate and often requires time, as reported in the following example by an FCN where a patient, despite experiencing multiple falls, was reluctant to adjust their lifestyle habits: ‘I had to go two or three times to convince him—look, last time you fell, you hit your head, you got hurt’ (Int. 19, F, 50 years).
Theme 3: Being a Node in the Healthcare Network
This theme reflects how FCNs perceived themselves as key figures within the community-based network, acting as connectors between individuals, healthcare and social services, and local community resources. In this context, the concept of a ‘node’ represents a point of connection that links citizens’ needs with available professionals and informal resources. To effectively fulfill this role, participants emphasized the importance of developing a deep understanding of the local context and identifying informal resources – such as volunteer groups, religious organizations, and neighbors alongside existing support networks. As one participant illustrated: ‘The FCNs have this role; they are there in the community, you look at your geographical map. You must go into that area, and what do you do? You map the network’ (Int. 14, F, 46 years).
The mapping process is not merely about cataloging existing resources; it also holds a relational value, fostering strong and effective connections that support individuals throughout their health and illness journey. Participants made sense of building these connections as a fundamental aspect of their role within the network. One FCN metaphorically described this experience as ‘building bridges,’ highlighting the significance of continuity and coherence in care pathways: ‘I believe it is important [as FCN] to build bridges with social services, general practitioners, hospital services, and all the professionals who can support individuals throughout their care journey’ (Int. 20, F, 53 years).
In this perspective, the ‘network’ is seen as a dynamic and adaptable structure, designed to meet the unique needs of each individual. Being a node within this network requires a holistic approach to care, prioritizing interprofessional collaboration and recognizing the home as a key setting for care. This concept was clearly articulated by one participant, who shared: ‘A whole team of professionals was involved to ensure that this person could remain at home until the end of their life’ (Int. 03, F, 42 years).
The network is not just an organizational structure but a relational space that helps individuals feel supported and valued. As one participant explained: ‘[Patients] primarily need a network that embraces them and offers guidance for their overall health, not just for their illness or chronic condition’ (Int. 01, F, 50 years). From this perspective, the network becomes a space where diverse professionals are focused on a common goal: the well-being of the individual. The experiences shared by FCNs highlight the importance of taking a holistic view of the person and providing continuous support, not only during illness but throughout their entire life journey.
Theme 4: Establishing the FCN Identity Through Role Differentiation
This theme reveals how participants interpreted the FCN role as fundamentally distinct from that of home care nurses, emphasizing a deeper sense of professional identity and relational engagement. Whereas home care nurses were described as primarily carrying out task-oriented interventions triggered by general practitioners after identifying specific health needs manageable at home, FCNs understood their role as broader and more integrative, involving continuous presence and holistic care. At the same time, participants reported the ongoing challenge of negotiating and clarifying the boundaries of this evolving role, highlighting the ambiguity and complexity involved in defining its scope within the healthcare system. Currently, the FCN role is often defined in relation to the existing district nursing model, which is structured around home care nurses, but it lacks a clearly established framework. As one participant explained: ‘An FCN is not just someone who does what the home care nurse does’ (Int. 01, F, 50 years).
The absence of clear role boundaries often results in FCNs taking on a wide range of tasks. Some nurses describe themselves as ‘all-rounders’, expected to perform both task-oriented activities – similar to those carried out by home care nurses – and adopt a proactive approach aimed at identifying emerging health needs. As one participant illustrated: ‘The FCN is a bit of an all-rounder, handling both task-oriented activities and proactive approaches’ (Int.23, F, 55 years).
As a result, some nurses perceive family and community nursing as an integration of the task-oriented model and a proactive approach, focused on health promotion, disease prevention, and proximity to families and communities. This integration allows for greater organizational autonomy, enabling FCNs to manage their workload more flexibly within their shifts. One participant highlighted this aspect, stating: ‘You have to manage the work yourself, which can be both a pro and a con. You have the freedom to organize it the way you want and manage both time and space’ (Int. 18, F, 31 years).
Proximity to families and the community was a central dimension in FCNs’ lived experience, reflecting the ways in which they perceive and enact their role within the community. Participants described their role not merely as a physical presence within the community, but as an active engagement in building trusting relationships with citizens. The FCN was experienced as a stable and accessible point of reference for residents, embodying a sense of continuity and reliability. As one participant illustrated: ‘We are the point of reference for the citizen, for the residents of that specific area’ (Int.14, F, 46 years).
Discussion
This study explored the experiences and the meaning of being an FCN in Italy, where the role has been formally recognized as an integral part of the Italian National Health Service since the enactment of Ministerial Decree No. 77/2022. Regional health authorities have adapted and operationalized the decree by tailoring family and community nursing to the specific needs, demographic profiles, and organizational structures of local healthcare systems. Adopting a phenomenological hermeneutic approach, the study identified four main themes that capture the essence of how family and community nursing is experienced: (a) Navigating elderly care complexity; (b) Education as a core function; (c) Being a node in the healthcare network; (d) Establishing the FCN identity through role differentiation. The four themes address two key aspects of the FCN role: direct patient care and the positioning of the FCN within the healthcare system. This dual focus highlights how the professional identity of FCNs is shaped not only by their clinical responsibilities but also by their level of integration within organizational models. Findings indicate that FCNs are currently experiencing a critical phase of professional identity consolidation, characterized by efforts to gain more autonomy and a clearer definition of their role.
Due to ongoing demographic changes – most notably the rising prevalence of chronic conditions and disabilities – FCNs mainly assist populations with complex care needs. Existing literature suggests that care complexity is not solely determined by the number of chronic conditions but rather by a combination of clinical, social, and economic factors (Manning & Gagnon, 2017). Consequently, nursing practice is progressively shifting toward a holistic approach that emphasizes individualized care, health promotion, and care continuity (International Council of Nurses [ICN], 2025). Continuity of care is realized through interprofessional collaboration, where nurses act as strategic connectors among various actors and levels of the healthcare system, promoting care pathways that are centered on people and cross organizational boundaries (ICN, 2024). A key element of FCN professional identity lies in building and maintaining these connections, linking patients, families, and community-based networks. Participant interviews highlighted the role of the FCN as a ‘nurse navigator’, capable of guiding individuals through healthcare systems, frequently described by patients and caregivers as fragmented and poorly coordinated (Ploeg et al., 2017). In this role, nurses contribute significantly to improving the care experiences of individuals with complex needs (Teggart et al., 2023). However, as observed in other countries, the lack of formal recognition of nurse care coordinator roles limits their systemic impact (Brownwood & Lafortune, 2024). Without institutional legitimization and a clear operational definition, many of the activities carried out by FCNs as ‘nurse navigator’ rely heavily on the individual efforts of each professional.
The need for a clear definition aligns with broader international debates on the evolving role of the nursing profession within PC (Brownwood & Lafortune, 2024). The professional identity is not merely a matter of personal experience but the outcome of regulatory, organizational, and cultural recognition (Brzozowski et al., 2023). Interviews from this study show that many FCNs often have to negotiate their legitimacy and clarify their scope of practice within a system that still lacks standardized operational references.
This lack of structured roles contrasts with internationally established positions like the Advanced Practice Nurse (APN), which are embedded within a well-defined framework (ICN, 2020). Although FCN is not yet formally recognized as an APN role in the Italian regulatory system (Brownwood & Lafortune, 2024), efforts are underway to promote advanced education programs aligned with international standards (ICN, 2020). International experience shows that the transition to advanced nursing roles is often influenced by cultural, organizational or socio-political constraints. These include traditional perception of nurses as task-oriented practitioners rather than autonomous professionals, fragmented regulatory frameworks, and poor alignment between education, legislation, and workforce planning (Torrens et al., 2020). Furthermore, role transition represents a personal shift, involving changes in how individuals perceive themselves and how they believe they are perceived by others, with significant implications for role identity formation and its internal coherence (Kerr & Macaskill, 2020).
A central dimension in this transition is the development of both personal and professional autonomy. As Thompson and McNamara (2022) point out, autonomy is a relational and negotiated process, shaped by context, professional recognition, and interaction with other healthcare professionals. It requires both internal confidence and external validation and is often shaped through negotiation with traditional hierarchies and institutional structures (Thompson & McNamara, 2022). The lived experiences described by FCNs in this study are embedded in broader systemic structures, particularly healthcare hierarchies. These hierarchies influence both the perceived autonomy of FCNs and the degree of role recognition within PC settings. Moreover, findings from this study show that FCNs seek to define themselves as a role that is distinct yet integrated with home care nursing, establishing areas of autonomy both in patient education and in organizing their daily work. Autonomy is constructed through practice, contributing to both the empowerment of FCNs and the consolidation of their professional identity.
Strengths and Limitations
This study provides an in-depth description of the experience and meaning of being a FCN in Italy, helping to fill a gap in the literature on this professional role. However, the study has some limitations. The sample was recruited through purposive and snowball sampling, which may have resulted in the inclusion of more motivated participants sharing similar views, potentially excluding nurses with different perspectives.
Although the selection of regions from Northern, Central, and Southern Italy was intended to enhance national representativeness, this may nonetheless limit the transferability of the findings. It is important to highlight that, according to national regulations, Northern Italy and Tuscany were among the first regions to introduce the FCN. As a result, nurses in these areas may have more established experience compared to those in regions where implementation is more recent. However, this study did not explore how these regional timelines of implementation may have influenced FCNs’ experiences, limiting the ability to capture potential variations linked to the earlier or later adoption of the FCN role. Another limitation concerns the data collection method. Interviews were conducted via Google Meet, which may have influenced the quality of interactions. However, this approach facilitated participation by allowing nurses from different geographic areas to schedule interviews based on their availability. Finally, while Cohen’s method (Cohen et al., 2000) was appropriate for data analysis and techniques such as bracketing and triangulation were employed to foster reflexivity and critical awareness, the interpretation of the results may still be influenced by researcher subjectivity.
Conclusion
Working with an aging population means addressing high levels of care complexity, which requires continuity of care, the ability to build trusting relationships with both patients and caregivers, and effective collaboration with healthcare and community-based organizations. The formal recognition of the FCN role was recently established with DM 77/2022, in a context where nursing has traditionally been perceived as task oriented. Findings from the interviews indicate that FCNs seek greater role specificity and autonomy, underscoring the need for a more structured framework.
Implications for practice suggest the importance of supporting FCNs during this consolidation phase through health policies and regulations that formally recognize their specific functions and enhance their contribution to community-based care. Future research should focus on identifying and analyzing barriers and facilitators influencing the implementation of this role. These insights could be valuable for policymakers in designing effective strategies to strengthen family and community nursing integration within the healthcare system.
Footnotes
Acknowledgements
The research team would like to express our gratitude to the Association of Family and Community Nurses (AiFeC), the Directors of Nursing and to all the participants in the study for their valuable time and contribution.
Acknowledgements
This study was supported by the Italian Ministry of University and Research (MUR) program “Departments of Excellence 2023–2027”, AGING Project – Department of Translational Medicine, Università del Piemonte Orientale.
ORCID iDs
Ethical Considerations
The study was approved by the Novara Ethics Committee (n° CE307/2023) on November 9, 2023. All participants provided written and verbally informed consent prior to participating.
Consent to Participate
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article; and informed consent was also obtained verbally before participation of the interviews. The consent was audio-recorded in the presence of an independent witness.
Consent for Publication
The authors confirm that they have obtained written informed consent for publication.
Author Contributions
Conceptualization: I.S., E.B. (Erika Bassi), I.B., A.D., E.B., and A.D.M.; Investigation: I.S., A.D., and M.S.; Methodology: I.S., E.B. (Erika Bassi), E.B., A.D., and A.D.M.; Writing-original draft paper: I.S., E.B. and A.D.; Writing-review and editing: I.S., E.B., E.B. (Erika Bassi), I.B., E.A., A.D., and A.D.M.; Supervision: A.D.M.; Project administration: I.S., E.B. (Erika Bassi), E.B., and A.D.M., Funding acquisition: A.D.M. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the AGE-IT national project, which has received funding from the MUR-M4C2 1.3 of PNRR with grant agreement n. PE0000015.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.