
Abstract
This study aimed to explore the interests and expectations of people living with Parkinson’s disease (PD), family carers, health and social care professionals, and key stakeholders regarding relevant systems of support and community resources for PD management. As part of the OPTIM-PARK project (Optimisation of Community Resources and Systems of Support to Enhance the Process of Living with PD), an exploratory qualitative study was conducted in Spain. Forty-one participants completed a GENIE concentric circles mapping exercise to identify existing support systems and community resources. These maps informed subsequent semi-structured interviews. All interviews were digitally recorded and transcribed verbatim for thematic analysis. Participants identified several barriers to effective collaboration across healthcare and social care systems, including poor understanding of PD, limited financial resources, and insufficient communication among professionals and sectors. Facilitators for improved community-based PD management included personalised care pathways, shared decision-making, improved access to professional services and local resources, and the strategic use of Information and Communication Technologies (ICTs). Participants emphasised the need for long-term investment and strong institutional commitment to reinforce community-based support networks for individuals living with PD.
Introduction
Parkinson’s disease (PD) is the second most common neurodegenerative disease, with global estimates in 2019 showing over 8.5 million people living with PD (PwPD) (WHO, 2022). This prevalence has increased in the last 30 years more than 2.5 times and will double by 2030 (Tolosa et al., 2021). The Global Burden of Disease shows a pronounced increasing trend in the PD burden, between 1990 and 2019, in high-income countries, probably related to the increase in disability in later life, as age is the most important risk factor to developing PD (GBD 2016 Neurology Collaborators, 2019). Longer disease duration in early onset PD, and other complications like stroke, dementia, dysphagia, or depression and anxiety, could prolong the course of disability. PD is an increasing challenge to global health (Ou et al., 2021; Tolosa et al., 2021).
The lack of ability to fulfil social roles and the restriction of normal social activities, due to motor (bradykinesia, rigidity, resting tremor, and postural instability) and non-motor symptoms (constipation, urine incontinence, cognitive impairment, fatigue, mood disturbances, and sleep), also affect the burden on people living with PD and their families (Li et al., 2023). Different authors (Li et al., 2023; Ou et al., 2021) have highlighted the importance of more effective strategies and person-centred treatments to decrease disability while maximizing the person’s quality of life and well-being.
Recent studies show that multidisciplinary or interdisciplinary teams may improve PD management (Bloem et al., 2020; Qamar et al., 2017). Although there are no tested clinical pathways in people living with PD and family carers (FC), experts have proposed key recommendations and considerations for optimal multidisciplinary care for PwPD, including care organised in a person-centred way; access to a core multidisciplinary team for newly diagnosed people; reducing health inequalities; the involvement of PD associations, other local community and voluntary organisations; networks of interdisciplinary expertise; the need to ensure high-quality services within and across agencies; and the importance of a community approach (Nielsen et al., 2022; Radder et al., 2020).
The diagnosis and treatment of Parkinson’s disease in Spain is performed in hospital movement disorder clinics, and standard follow-up is conducted by the neurologist at these clinics every 6 months. The role of primary care in this process is to detect symptoms and support treatment. Neurologists often offer advice on accessing other specialists (speech therapists, physical therapists, nutritionists) or participating in activities organised by associations to maintain optimal quality of life. The complexity of PD management, which encompasses cross-sectoral collaboration, coordination with community services and non-clinical interventions with a multisectoral or intersectoral approach, 1 can pose significant challenges throughout the PD journey. The compared perceptions of PwPD, their family carers and health and social care professionals in finding, navigating, and making use of the complex systems of support have not previously stated in the literature. Therefore, the aim of this study was to explore the interests and expectations of PwPD, family carers, health and social care professionals and stakeholders (SH) regarding the use, collaboration and impact of different organisations and sectors to enhance the management of PD in the community.
Specifically, the research questions were:
What systems of support and community resources are identified by people living with Parkinson’s, family carers, health and social care professionals and stakeholders for the daily management of Parkinson’s, and how accessible are they?
What unmet needs or difficulties exist in the management of Parkinson’s disease in the community setting?
Methods
This study employed an exploratory-descriptive qualitative design (Hunter et al., 2019), a suitable theoretical framework to study a healthcare practice topic, the management of PD in the community, which has received little attention. This study is part of the OPTIM-PARK project, a wider mixed-methods study with a sequential design to establish the feasibility and acceptability of an intervention that will enhance the process of living with PD for patients and family-carers by building multisectoral care pathways. This intervention had a special focus on how to optimise the use of resources and systems of support in the community in four European countries: Denmark, Norway, Spain and the United Kingdom. In the OPTIM-PARK research project, cross-national analyses have been conducted and published reporting on the strengths and challenges for multisectoral collaboration in the management of Parkinson’s disease in the community setting (Navarta-Sánchez et al., 2023; Soilemezi et al., 2023).
This paper reports on the perceptions of people living with PD, family carers, health and social care professionals and stakeholders, to understand the particularities of PD management in the community in Spain. Specifically, we explored what support systems and community resources were relevant to PD management according to the four key participant groups involved in this issue and what challenges they identify in managing PD in the community setting. Data for this paper were collected through semi-structured individual interviews and analysed using a thematic analysis (Braun & Clarke, 2006). The reporting in this study adheres to consolidated criteria for reporting qualitative (COREQ) research (Tong et al., 2007).
Participants and Setting
Eligible participants were people living with PD, their family carers, health and social care professionals and stakeholders (H&SCP), purposively sampled, in a large city and its metropolitan area, to achieve a diverse sample, including PwPD living in less advantaged areas or individuals from different sectors stakeholders and disciplines (Table 1).
Characteristics of the Participants in the Individual Interviews.

The inclusion criteria for participants were as follows:
People with PD living at home, Hoehn & Yahr stage 1 to 4, cognitively able to participate based on nurses/neurologists’ assessment; able to communicate well in the language of their country; at different stages (early, mid, later by years of diagnosis) and ages (younger and older); who had not been hospitalised in the last year.
Family carers of people leaving with PD at different stages (early, mid, late) involved in the care process. Family carers of people leaving with PD with cognitive impairment were also included.
Professionals from different disciplines (physicians, neurologists, general practitioners, nurses and specialist nurses, social workers, occupational therapists, physiotherapists, pharmacists, speech therapists), with at least 1 year of experience providing support directly or indirectly to people living with PD and family carers.
Stakeholders involved in policy making or working or collaborating in voluntary organisations or from different sectors—private health care, social services, voluntary sector, employment, food, pharmaceutical, education, political—which impact directly or indirectly on PD management and the development of care pathways for PD or other long-term conditions.
For the recruitment process, a nurse and a neurologist from a tertiary hospital identified the participants in the PwPD and family care group who met the inclusion criteria and informed them about the study. Information on the project was sent by email to various patients’ associations, research groups, and professional networks to achieve a diverse sample with representation from different sectors (health, social, research, pharmaceutical industry, voluntary organisations, etc.). Snowball sampling was also used to identify potential participants from different areas.
Data Collection
We planned semi-structured face-to-face interviews, however due to the Covid-19 pandemic these were held mainly by phone or videoconference and supported by an interview guide. The main topics covered in the interview guides were PwPD and family carers’ experiences and perceptions, different professional and voluntary organisations’ roles in PD management, available resources/services/organisations for PD management, and collaboration between agencies to improve PD management in the community (for more details see Appendix 1). Interviews lasted between 23 and 118 min and were digitally recorded and transcribed verbatim for analysis.
After agreeing to take part (with written consent sent by email or postal mail), all participants were asked to complete the socio-demographic questionnaire. Participants then took part in a semi-structured interview, using a concentric circles diagram. Permission from the original authors was obtained to use the concentric circles diagram from the GENIE intervention tool website (GENIE® is a registered trademark of the University of Southampton) as a reference (Figure 1). These diagrams helped create a visual map of the participants’ support network, and importance and roles of support in their daily lives (Kennedy et al., 2015). This also offered the opportunity to initiate a dialogue about the participants’ support needs. People living with Parkinson’s disease and family carers were asked to write the names of every personal network of support, access to resources and availability (or lack) of support, indicating the perceived degree of closeness by their proximity to the centre of the GENIE circles. Health and social care professionals and stakeholders were asked to do the same with their professional networks of support and information, access to resources and communication with other people and groups within their professional role. The use of GENIE enabled the identification and discussion of existing community resources and systems of support and allowed for a point of reflection and focus on the themes to be explored which helped to deepen and articulate the subsequent interview.
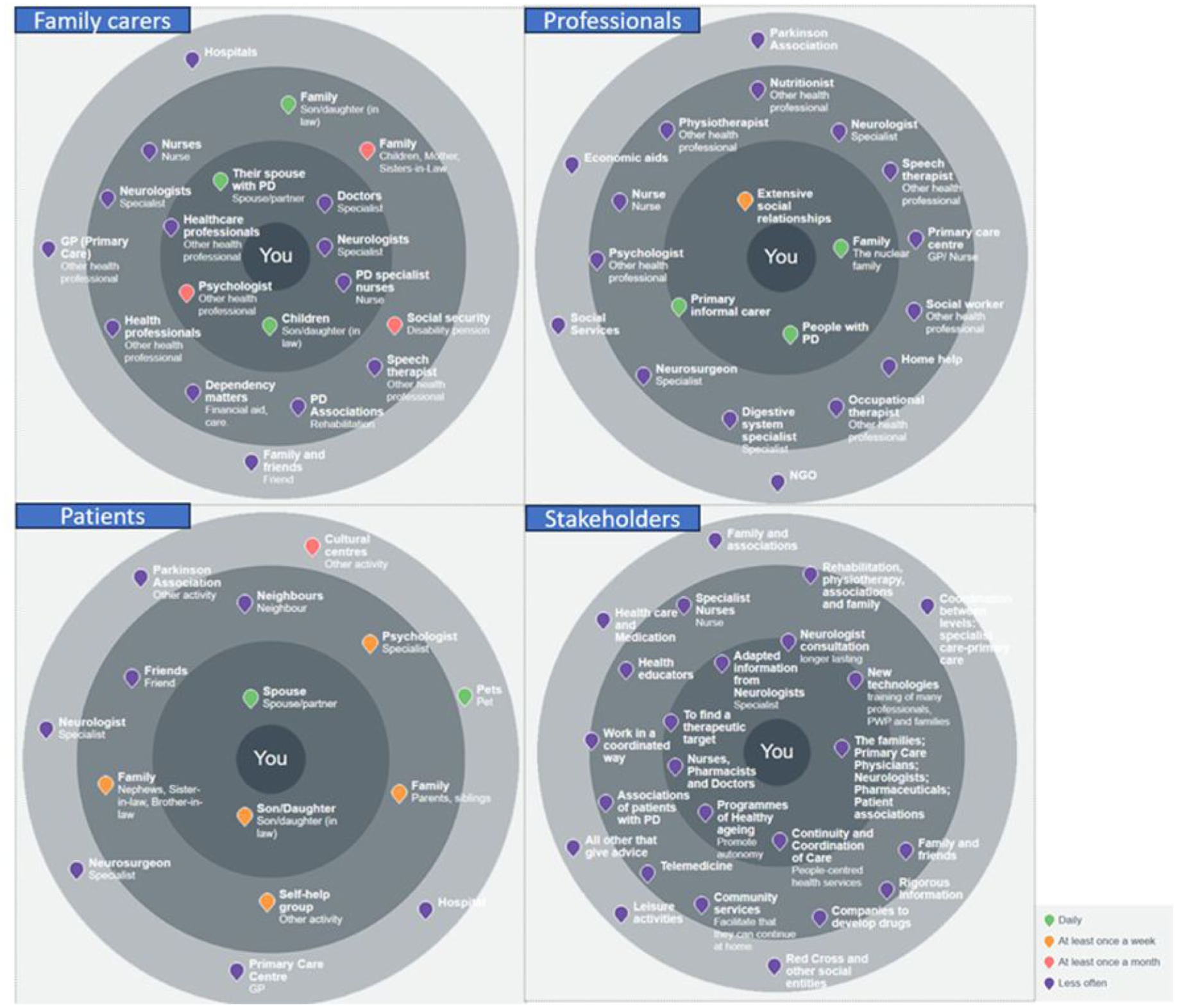
Systems of support and community resources identified by the different groups of participants for the daily management of Parkinson’s, using the GENIE® intervention tool.
Analysis
We conducted a thematic analysis (Braun & Clarke, 2006, 2021) of the interviews, to explore and describe the experiences of participants in relation to phenomena under study (Hunter et al., 2019), with an inductive approach (Braun & Clarke, 2023). In this analysis, the observational data in the GENIE tool was of assistance in gaining a better understanding of the support networks perceived by participants as a precursor to thematic analysis (Kennedy et al., 2015).
The analysis began after the first interviews with an inductive approach and was run in parallel to data collection. Meaning units were identified and labelled with a code by the research team over several sessions. The document containing codes for the analysis pathways enabled the categorisation of ideas generated from the transcripts. Following an iterative process, researchers reviewed the research goals several times, refining the codes established and reorganising them into broader categories. A thematic map was prepared, grouping labels in themes and subthemes that were illustrated with relevant verbatim quotations. All authors participated in all phases of the analysis to ensure a nuanced analysis.
Ethics
The Ethics Committee at Hospital Universitario La Princesa (Reference 3995, CEIm 02/20) approved this study. Interview data were anonymised, and transcriptions were stored in a protected file in the university cloud storage with a strong authentication method. An information sheet was co-designed with expert people from the Patient and Public Involvement group (Zeissler et al., 2024). Participants received the information sheet and could ask questions before accepting to participate. All participants signed an informed consent document.
Rigour
To enhance the rigour of this study, trustworthiness was ensured through different approaches based on the framework of Lincoln and Guba (1985). To enhance the credibility of the analysis, verbatim participant quotes were used to support the authors’ interpretations and to illustrate the richness of the data. To facilitate transferability, we worked to provide thick descriptions of the context, the sample and the perspectives of the participants. As a check on dependability, the researchers kept a running account diary of the process. Finally, the researchers themselves used reflexivity about their own position on the topic, to ensure the confirmability of the data (Lincoln and Guba, 1985).
Results
In this study, 41 semi-structured individual interviews were carried out. The characteristics of participants are detailed in Table 1. In the analysis of the interviews, a total of 2 themes and 6 subthemes were identified, which can be seen in Table 2 and are described below in this section.
Themes and Subthemes.
Integrated Care to Improve PD Management
Integrated care provides a strategic response to the complexity of Parkinson’s disease (PD), ensuring support beyond clinical treatment. Key priorities include mobilising valuable resources within communities, strengthening multidisciplinary coordination among healthcare professionals, and advancing intersectoral collaboration to overcome service fragmentation. Together, these elements guide the design of integrated and sustainable models that improve quality of life for people living with PD and their carers.
Valuable Resources
The community resources identified in the GENIE diagram by the various groups of participants illustrated how family carers and people living with PD perceived their network members, and who they deemed valuable within their support and resources network. Stakeholders, health and social care professionals identified services, organisations and key elements they perceived to be useful for people living with PD and for family carers (see Figure 1).
People living with PD specifically identified their spouse as the person who gave them their main support, both at an emotional and instrumental level. Each of the people living with PD identified their spouse as the most important resource supporting them to live with PD. Depending on the degree of PD, patients’ spouses helped in more or fewer everyday activities. In general, people living with PD perceived this help as a significant and constant support to face the disease.
I feel well taken care of. I have an unbeatable family atmosphere. My husband and I are very close, and we understand each other very well. I have a son who still lives with me and a daughter who is 20 years old. Then we have an older girl who is 30 years old, but she already lives away from home. The thing is that, I’m going to be honest, the children are by my side, but who I can count on is my husband. (PwPD-009).
However, family carers saw the health and social services, together with their spouse with PD and children, as the most valuable resources for them to manage the disease in the community. Along the same lines, H&SCP focused on the nuclear family, other people living with PD and their extensive social relationships as the key resources for people living with PD. On the other hand, stakeholders put at the centre of the GENIE an array of resources, other than the family: adapted information from neurologists, new technologies, finding a therapeutic target, healthy ageing programmes, nurses, pharmacists and doctors, or continued and coordinated care.
The doctors, social workers, therapists (. . .), people in charge of associations and foundations that I connect with the therapists as well and then the family and caregivers. For me they are a whole, it is a circle that has to be united, because in the end each gear by itself does not make sense, they are temporary solutions. It will not be solved. In other words, it will not be given good support. (H&SCP-011)
Multidisciplinary Coordination
In relation to the accessibility and type of care received by healthcare professionals (identified as important resources for the management of PD in the GENIE diagrams), it is important to note that most of the participants in the four groups interviewed found difficulties in multidisciplinary coordination. In particular, PwPD perceived a lack of coordination between Primary Care and Specialised Care. They pointed out that Primary Care was not a place of reference for their PD related needs. Moreover, they explained that their contact with Primary Care was occasional.
The first doctor who treated me did not even know what Parkinson’s was (. . .) when I went to the health centre for something and the doctor told me, “Come in, come in”, and he didn’t realize that I couldn’t [easy access from the waiting room to the consulting room]. And then he realized and apologized, but I felt bad because I said, “not even the doctor knows”. (PwPD-002)
Health and social care professionals and stakeholders underlined this lack of coordination that affects the continuity of care between healthcare levels. But they also called for the creation of multidisciplinary teams including professionals from different disciplines and levels of care. However, they rarely spoke about coordinated interventions, only when asked directly. It seems that there was not a culture of multilevel thinking.
I do not see that there is anyone who is coordinating, at least they have not asked us [Primary Care professionals] (. . .) That is, to do something in common in a coordinated way (. . .) to work in common. That is why I find it a bit difficult due to the different areas. And then the social aspect, which clearly comes into play here, with the healthcare aspect, with which we already have two different areas (social and health). [. . .] And then the associations that do everything they can, sometimes even try to do something in common, but they also often get lost in our institutional bureaucracy. (H&SCP-005)
Intersectoral Collaboration
Consistent the GENIE diagrams, where stakeholders identified coordinated care as a valuable resource for PD management, participants emphasised in their interviews that cross-sector coordination remains an important but unmet goal. Despite the differences between multisectoral or intersectoral coordination, health care professionals and stakeholders interviewed in our study used both terms as synonymous. Notwithstanding, participants agreed on the need to build a network of resources that fosters collaborative support in managing PD. They noted that learning from others and showcasing successful examples could serve as a foundation for initiating multisectoral efforts tailored to the specific needs of each community.
There is a company, a start-up, which was founded by engineers from (name of the University) in collaboration with a medical doctor and they have developed a motion sensor (. . .) they already have it ready for the market. (. . .) There are already people who have tried it and are delighted because the sensor puts in front of them what they need to know, which is when the patient is unwell during the day and . . . and then, with a quick glance, they can make better medication adjustments. (SH-001)
Intersectoral collaboration unites diverse sectors to tackle complex issues, such as PD management, by integrating expertise and resources from multiple areas to achieve effective and sustainable solutions. Knowing and incorporating accessible community resources in the environment of the person with PD can contribute to expanding this network of resources, which incorporates health resources, but also goes beyond the limitations of a biomedical approach to the disease.
Well, I think it’s very important when people tell you ‘I’ve always lived here and I feel like part of this neighbourhood, and . . .’, right? Neighbourhoods change a lot, others are transformed. But they still have their friends there, their parish where they go, I don’t know (. . .). The health centre itself and their nurse. They are like references there, they are key, right? To sustain chronic processes. (SH-002)
Nevertheless, family carers and PwPD identified several barriers to the implementation of effective intersectoral initiatives—most notably, a lack of understanding of PD and limited funding. Concerns about the affordability of necessary resources and services were also raised, as one participant explained.
Not more available, but at least more affordable (refers to therapies in a PD association). It is an economic question . . . for people who have a pension of eight hundred, nine hundred euros, where do they go? There are many people who may be a widow, or a widower, who have a small pension, indeed, the association is expensive. (FC-002)
Optimising Resources and Support Systems
Participants emphasised the importance of improving access to resources and ensuring a more effective use of existing support systems in the management of PD. They identified several strategies to address current gaps and strengthen care delivery, particularly through approaches tailored to individual needs and local contexts. Four interrelated sub-themes reflect these findings: the development of a personalised pathway to care, the central role of family support, the importance of accessibility, and the potential of information and communication technology to enhance coordination and connection.
A Personalised Pathway
While stakeholders were the only group to identify information as a key resource for managing PD in the GENIE diagrams, participants from the other three groups also emphasised the importance of information during their interviews. People living with PD wanted to have more access to accurate information regarding their individual needs. They wished for personalised information about disease, treatment options and available community services and resources. However, depending on sociodemographic and contextual factors, participants perceived greater or fewer difficulties when entering a PD pathway. Age was identified as one of the key elements that influence participants’ experience. PD in younger people was generally experienced as a more serious biographical disruption. Younger participants did not feel represented in the “chronic patient” label, because this was usually linked to advanced ages, when the coping and acceptance of limitations became more complex.
I was thinking of Parkinson’s, when you were already old, at eighty-something years . . . The older you are, the neurologist told me that the medication had an effect on you for 8-10 years, the medication has an effect on you and more or less you have a normal life. Then the problem is with young people, what do we do when those ten years are up. (PwPD-002)
Family carers explained that they have used the internet and other sources to gain knowledge about PD. An opportunity was lost for professionals to provide key and necessary information and training to PwPD and carers. Availing of certain resources or managing certain aspects of disease monitoring was not usually mediated or facilitated by the health professionals. The hospital and specialists were also providers of information, but this was occasional (only in the context of the appointment) and not adapted to the particular needs of people living with PD and caregivers. Relatives explained that they did not have access to any professional to answer their questions and doubts.
More or less, I have studied a little online, read books that I have had, and I use the internet a lot (. . .) Maybe you have a question, and you don’t know what to do, you don’t know where to call. Well, so that they can solve any doubts, well look now he is blocked, he needs this pill, can I give it to him? (. . .) Every time this happens to him, what do I do? (FC-005) I have many doubts that I have already learned to live with. You have many doubts, but they will not solve anything or solve anything for you. (FC-006)
This contrasted with the professionals’ discourse, who in the interviews emphasised the importance of providing information specific to the individual person’s needs and situation. They explained that PD was a complex disease with different symptoms and that the trajectory of the disease in each person could vary. Most professionals regularly carried out global patient assessments and asked them what they wanted to know about Parkinson’s and their concerns. In this way, professionals could adapt the information about PD or resources to the patient.
Before he came, I phoned to ask him what he was doing, whether he was active or not, his family situation, his education level, and I asked him how he wanted, that is, what he wanted to know, that we would have the opportunity to see each other over a long time and that we could organize an education programme according to how he felt at the time, his needs and his psychological state. (. . .) And that, in the end, what you achieve is that your patient’s satisfaction will increase and everything that surrounds it, such as resistance, adherence, disease management, etc., will also improve. (H&SCP-001)
Professionals pointed out that people living with PD could benefit from shared decision-making in treatment management. This collaboration involved both shared management that could be established between patient, family carer and professional, as well as shared management among the different professionals involved in treating the person.
When a patient is diagnosed with a disease, he goes to the doctor, or the nurse and the doctor proposes the different therapies that exist. The logical thing is that a choice of therapy is made, let’s say among everything else (. . .) you have to take into account all the parties involved, including the family member or the main carer, so that there is good adherence to the treatment, a good persistence and the patient is happy and knows how to handle their situation well. (H&SCP-001)
Family Support
All four groups of participants identified on the GENIE diagrams that the family is an important resource for people living with Parkinson’s disease in their daily lives. Many participants mentioned that family carers could be quite resourceful and asked for help from H&SCPs or other stakeholders they were in contact with and that they trusted. Family carers would proactively go and look for help in any way that they could, asking about how to access information or resources that was relevant to their need and might support their management of living with or caring for someone with PD. This was most evident at the time of diagnosis when there could be a need to seek information about how best to support their family member with PD. Family carers were clearly involved in the care process and this could mean important indirect costs the system was saving. It is important to me that my opinion is taken into account. Not because it is more or less important than anyone else’s, simply because I also have doubts, maybe I also have something to contribute, or give ideas about what we are talking about right now, that help that we as caregivers also need sometimes. (FC-004) There are families that organize themselves and distribute it (the care) among all members. There is usually one who is the main one, a person who takes the lead. But often there are more people in a family that share caregiving. And it is an important job, and it is a job that moves a lot of money. In other words, if that were not done (by the family), it would mean a lot of money. (SH-009)
Caregivers, both family and other informal caregivers, needed recognition and support. This was how participants perceived it, although they were aware that the formal services could not always provide or deliver this type of assistance.
At the [name of a voluntary organization] we work with mutual support groups, we work with the respite part, where, for example, a volunteer will stay with the dependent person, while the caregiver . . . so that the caregiver can have a free space, either for leisure, or for. . . Which is sometimes simply to do other business, okay? Many times, it is to go to the pharmacy to buy. I don’t know what. But hey, between going to the pharmacy, he goes for a walk and quiets his mind a little. But hey, out there. And psychological support, guidance. . . . All this is part of the project of care for caregivers. (SH-009)
Supporting Access to Care
The theme of supporting access to care encompasses strategies such as facilitating connections to community resources and services, providing transportation options, expanding the use of Information and Communication Technologies (ICTs) like telehealth, and ensuring the availability of home help.
Access to community resources and services was identified as a challenge for people living with PD. In many cases, public transportation was not a viable option, and participants noted that subsidies for taxi use were not consistently available. As a result, families members often had to provide the person with PD a lift; however, this was not always feasible due to limited availability or the absence of a valid driver’s license.
You need a family member to take you to the pool, pick you up, take you to the association, and then pick you up again . . . That is a big problem because you screw your son, you screw . . . the people, your family, because they always have to be looking out for you. (PwPD-002)
Information and Communication Technologies (ICTs) were identified in the GENIE diagrams by stakeholders as a resource that could increase accessibility to care in some cases. Some professionals specifically suggested that incorporating telehealth consultations and improving appointment scheduling could help ease the burden on caregivers while also saving time for healthcare providers as well as caregivers and patients.
I believe that without replacing the face-to-face consultation, because I do not believe that it can be substituted at all in our case, but perhaps if a telephone consultation can be inserted that needs less duration than the face-to-face appointment, we can shorten those times. (. . .) If it were conducted through a video call, it could even improve the time spent on the medical check. (H&SCP-002)
The lack of economic resources to support daily living with PD was another big issue commented on, not only by the people living with PD and family carers, but also by stakeholders and H&SCP. In the Spanish context, the Dependency Law creates a dependency autonomy and care system through a set of public and private services and benefits, ranging from prevention to residential care, including other services such as telecare or home help.
We should have more help with that, because with the help they give you today you can do nothing! (. . .) You need a lot of things and with two hundred euros, nothing! (FC-005) I see patients and relatives when they are in a non-incipient state of the disease, and especially in advanced stages, when they begin to request some type of resource related to dependency, because the disease progresses and caregivers require support (. . .) So there is a great dysfunction regarding the impressive delay inherent to the Dependency Law. (H&SCP-006)
Discussion
This is the first study which provides a wider understanding of PD management and systems of support from the perspective of people with PD, family carers, professionals and stakeholders. By triangulating the perspectives of all actors involved, the visualisation of support presented in this paper offers a comprehensive understanding of a unique reality, capturing the interests and expectations of both PD service providers and users.
In this study, family stood out as the primary source of support for people living with PD. The idiosyncrasy of the Mediterranean basin, where family members are the cornerstone of care for people living with chronic conditions, providing essential support that is both culturally expected and practically necessary, has been pointed out in various studies (Porcel-Gálvez et al., 2024). However, all participants emphasised the need for additional resources to ensure access to specialised professionals—such as physiotherapists, speech therapists, and occupational therapists—as well as to community services that assist both individuals with PD and their family carers in managing the condition. This finding is consistent with previous research studies that identify multidisciplinary teams as essential to enhancing PD management at the Primary Care level (Bloem et al., 2020; Navarta-Sánchez et al., 2020).
People living with Parkinson’s disease (PD) and their family members in our study highlighted the need for personalised, local care, to assist them in managing PD within their own environment. Health professionals and stakeholders considered it necessary to establish a comprehensive, integrated multilevel system for treating these persons, whose care needs increase as the disease progresses and at different stages in their lives. In specific terms, they pointed out the importance of sharing objectives in the care given to people living with PD across the levels of care (Primary Health Care, clinics and hospital) and other sectors (town council, PD organisations). These findings match the proposal by the WHO (2021) and previous research (Bartolomeu Pires et al., 2024) on the need to provide long-term, personalised and comprehensive care to people living with neurodegenerative diseases such as PD. This approach requires the different services offering support to PwPD to respond to the changing needs as their disease progresses.
Multisectoral collaboration has been shown to be key to managing chronic health problems, in which different needs require the participation of different care and support resources to enable the person with PD and family members, to have the best quality of life possible (Portillo et al., 2017; WHO, 2018). Vester et al. (2023), in a recent scoping review, identified peer support and a personal, coordinated plan as one of the most beneficial strategies for raising the quality of life for PwPD. They propose that multisectoral initiatives ought to accompany the development of the condition, as well as a Parkinson’s care-coordinator whose mission is to uphold communication among the agents involved and to provide individualised information regarding the available resources for managing Parkinson’s Disease (Vester et al., 2023). Such initiatives were also discussed by participants in our study, although PwPD and family carers were more focused on access to resources from the perspectives of economy, proximity and information. Health professionals called for coordination among the different levels of care and services, but they viewed this as desirable or necessary rather than part of their role. Stakeholders, however, held the clearest notion of how this network should be set up, involving professionals and administrators alike.
In the era of increasingly personalised care, our findings align with other research (Tuijt et al., 2020) in the need to tailor the information given, especially in the initial stages of the condition, as well as in the coping strategies relevant to people living with PD. Person-centred care approach to clinical practice is relevant to the findings of this study as it respects and empowers patients as “moral agents and collaborative partners whose own perspectives on their lives and how they live them, matter” (Entwistle et al., 2018). Hence, PD services need to meet the expectations of people living with PD, taking into account the stage they are undergoing, their personal characteristics and their social context. Considering this approach, H&SCP encounter limitations, fundamentally, related to the biomedical approach toward patients, as described in the study by Armstrong et al. (2021), the lack of coordination with other levels of care, and the time dedicated to each consultation, as well as the pace at which the latter are conducted. As Bloem et al. (2020) pointed, PD current care is fragmented across different health-care providers and organisations. They proposed nurses specialised in PD care as the first point of access for patient queries. But they also feel that nurses acting as a personal care manager might be based in the community. In our study, primary care was barely mentioned as a resource in the discourses of PwPD and their family carers. Nevertheless, the primary health care seems the best setting to manage the daily needs of the disease in close collaboration with other levels of care and resources.
Information and Communication Technologies were offered as a useful tool for enhancing communication with PwPD and family carers, rendering it more efficient and reducing the burden on the healthcare system, as seen in the study by Jiménez et al. (2023), which proposes incorporating end users both in the design of these technological solutions and in their operation procedures. Among other uses, IC Technologies can be applied to clinical monitoring procedures, enabling more accessible information and resources, and the use of technology in rehabilitation and speech therapy (Bloem et al., 2020; Fabbri et al., 2020).
The growing prevalence of Parkinson’s disease and, therefore, rising costs to the health system, detracts from the efficiency of a care system based on monitoring through sparse in-clinic visits. Proposals entailing a community approach are deemed more effective, but further evidence is still needed to understand how to bring together professionals and resources in a pragmatic and flexible approach that adapts to the needs arising as the condition progresses (Fabbri et al., 2020). Among the most pressing needs highlighted in our study, access to resources and support systems, recourse to reliable information that is relevant to the needs of those living with PD and to family caregivers, were referred to as closely interconnected aspects. Economic resources and family support enable access to certain resources, while provision of personalised information facilitates the selection of the resources best suited to each situation. According to the most recent NICE (2017) guide to PD management, an appropriate communication and information channel should be guaranteed for people living with PD and family carers, allowing them to participate in making decisions regarding their health and living with PD, and thus address their own individual needs. Patient and public involvement and engagement must be a reality at all levels of care, research and management and the incorporation of Parkinson’s associations can be a key element in advocating for the needs of people living with PD and their families.
The need for information on how to find community resources or apply for financial aid is also one of the main needs highlighted by PwPD in the study by Lee et al. (2019). Family caregivers in the local environment are key to managing Parkinson’s disease, and require resources for training, information and support to provide this care. We have found few studies that specify the type of community resources PwPD and their family carers might benefit from. Numerous studies point out the importance of a care coordinator (Bartolomeu Pires et al., 2024; Bloem et al., 2020; Vester et al., 2023). In contrast, although our participants repeatedly identified the need for coordination across all levels of care, this was not framed as a specific care coordination role.
Conclusion
In this study, participants identified the family carer as the most valuable and accessible resource for the management of Parkinson’s in the community. Therefore, clinical pathways should be integrated in the nursing practice to support family carers’ needs. Besides, healthcare professionals reflect on the need for personalised care that addresses people living with PD’s needs in a multidisciplinary collaborative context with the focus on prevention and follow-up. On the other hand, family carers and PwPD, who agree with the individualised pathway, long for recognition of their illness trajectory and their role in it. All participants in this study felt that it was necessary to strengthen the community network of resources with long-term investment and the implication of all the health and social care organisations.
Although participants rarely singled out specific health professionals other than neurologists, this lack of distinction may reflect the organisation of care in Spain, where specialised Parkinson’s disease (PD) nurses are not yet integrated into routine clinical practice. Nevertheless, nurses in primary health care settings play a crucial role in supporting people with PD, particularly in preventing complications, promoting self-management, and encouraging healthy lifestyles through interventions such as social prescribing. These findings underscore the potential for expanding the nursing role within multidisciplinary teams to improve the quality of care for people living with PD. They also highlight the need for greater visibility and recognition of nursing contributions in chronic disease management, both in Spain and in other contexts with similar health care structures
GENIE has been primarily implemented as a self-management support tool to empower individuals with long-term conditions. As far as we know it has not been used as a research tool, but its use in this study has been an asset to map and discuss the importance of the resources identified by PwPD, family carers, HSCP and stakeholders and the absence of those not pointed out, and reflect on the way they could be brought together in an integrated way.
Footnotes
Appendix
Interview Guide for the Individual Interviews with People with Parkinsons’s, Family Carers, Health and Social Care Professionals and Stakeholders.*

| Topic fields | Questions |
|---|---|
| The roles of the different professional and voluntary organisations in PD management | • What role do you think different organisations have in the management and everyday experience of Parkinson’s Disease (PD) and in caring for people with PD? (Professional organisations, voluntary organisations, the government, the national healthcare system.) |
| Available resources/services/organisations for PD management | • What community resources/systems of support are you aware of for people with PD and family carers? • What kind of support do they provide? How can they contribute to more positive living with PD? |
| Collaboration between agencies to improve PD management in the community | Specific for people with PD and family carers: • Have you experienced any problems accessing resources or services? What might have improved this access? • What aspects of PD management do you find most difficult? • Are there any relationships that would need to be focused on or strengthened in order for a new pathway to be helpful? • Specific for health and social care professionals and stakeholders: • Who is responsible in your organization for liaising with other organisations, professionals, policymakers? • Is there an official pathway within your service to signpost or refer to? • What kind of relationship do you have with the various PD organisations? • What kind of intervention would you find most useful in your current practice/role? |
Source. *An extended version of the interview guide can be found in the articles of Soilemezi et al. (2023) and Navarta-Sánchez et al. (2023) which show cross-country findings of the OPTIM-PARK project.
Acknowledgements
We want to thank Dr. Lydia Lopez Manzanares and Beatriz Gonzalez (Hospital Universitario de La Princesa) for their assistance in recruiting informants. We would also like to acknowledge the PPI representatives for their contribution to the study. This work was supported by the EU Joint Programme—Neurodegenerative Disease Research (JPND). The Autonomous University of Madrid and the Ministry of Universities of the Spanish Government (Recovery, Transformation and Resilience Plan) were the financing entities of the researcher M. V. Navarta-Sánchez (Grant number: CA2/RSUE/2021-00854). The Language Support Office of the Autonomous University of Madrid (OAL-UAM) provided edition assistance in English.
We would also like to thank Dr Ivaylo Vassilev and Prof Anne Rogers for granting permission to use the concentric circles of GENIE® (registered trademark of the University of Southampton) as a reference
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained by the required ethics committees: University of Southampton—IRAS number: 265184; Research Ethics Committee in Hospital Universitario La Princesa Number: 3995, CEIm 02/20; Norwegian Centre for Research Data Reference Number: 986940.
Consent to Participate
Participants received an information sheet and could ask questions before accepting to participate. All participants signed an informed consent document.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was has received funding by the EU Joint Programme—Neurodegenerative Disease Research (JPND), the Research Council of Norway (Grant Number: 299762) and the DAM foundation (Project Number FO296567), the Innovation Fund Denmark, and the Alzheimer’s Society (Grant Number: 470). The Autonomous University of Madrid and the Ministry of Universities of the Spanish Government (Recovery, Transformation and Resilience Plan) were the financing entities of the researcher Dr M Victoria Navarta-Sánchez (Grant Number: CA2/RSUE/2021-00854).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.