
Abstract
The early integration of palliative care (PC) alongside standard cancer care is associated with decreased symptom burden, better adherence to cancer treatment, and enhanced quality of life for individuals living with cancer. The purpose of this mixed methods systematic review was to answer the following research questions (1) What are the characteristics of PC access in non-hospital settings in the US for individuals living with cancer?, and (2) What factors facilitate or deter whether PC is integrated early alongside standard cancer care? The study followed the Joanna Briggs Institute methodology for mixed methods systematic review and a convergent integrated data analysis design. The Conceptual Framework of Access to Healthcare and its five dimensions of access (approachability, acceptability, availability, affordability, appropriateness) guided the categorization and organization of the review’s findings. Fifty-one studies were included and findings illuminated facilitators and challenges of PC access and early integration. While findings supported the use of traditional PC approaches for early integration, embedded PC clinics, lay navigation, and telehealth were found to be promising alternatives, especially for historically minoritized and rural populations. The results of this review led to the development of the Conceptual Framework for Early PC Access and Integration for Individuals Living with Cancer.
Background
In 2025, there will be over 2 million newly diagnosed cancer cases in the United States (US); and nearly 700,000 individuals will be living with metastatic cancer (American Cancer Society, 2024; Gallicchio et al., 2022). Individuals living with cancer and their care partners can endure significant physical and psychological distress. To support these individuals living with cancer and their care partners, palliative care (PC) offers interdisciplinary, person-centered care aimed at anticipating, preventing, and reducing suffering, and supporting the best quality of life (QOL) (Dans et al., 2021).
Early integration of PC alongside standard cancer care has been associated with decreased symptom burden, better adherence to cancer treatment, and enhanced QOL for individuals living with cancer; and care partners have reported improved QOL and satisfaction with the care provided to their loved ones (Cheville et al., 2015; Hoerger et al., 2019; Kwon et al., 2013). The American Society of Clinical Oncology and PC experts recommend integration of PC as early as 8 weeks from a cancer diagnosis that is locally advanced or deemed metastatic (Kamal et al., 2013; Meier et al., 2017). Early PC integration can also be beneficial for individuals experiencing complex symptoms or psychosocial distress even when their cancer is not metastatic or locally advanced, supporting a need-based, rather than prognosis-based approach to PC integration. Meghani (2004) conceptualized early integration not solely in terms of timing, but as concurrently delivered with disease-directed treatment. Similarly, Sawatzky et al. (2016) emphasize moving further upstream towards meeting the PC needs of individuals who have a life limiting condition including the development of PC competency and delivery in non-specialty PC settings, and the need to integrate PC principles across various healthcare settings.
While 95% of National Cancer Institute (NCI) Comprehensive Cancer Centers and 40% of all other cancer programs in the US have established outpatient PC (Hui, Anderson, et al., 2020), early integration of PC alongside standard cancer care outside the hospital setting remains suboptimal. It is estimated that up to 75% of individuals living with serious illnesses including cancer could benefit from PC (Morin et al., 2017). Yet, the rates of PC use are much lower than the percentage of those who could benefit. More than one-third of individuals living with cancer receiving PC do so in the last week of life (Roeland et al., 2016). There is also evidence that health determinants influence PC access and use. PC access and rates of use are lower for individuals of minority race or ethnicity, lower socioeconomic status, and those in rural dwellings (Belcher et al., 2023; Islam et al., 2021; Lee et al., 2021; Rubens et al., 2020).
These challenges are further complicated by structural and regulatory barriers present in the US healthcare system. Barriers include fragmented healthcare services, inadequate and antiquated documentation standards for outpatient and interdisciplinary PC reimbursement (Esch & Jones, 2024), and limited PC resources. State level regulatory constraints and variation in telehealth coverage policies inhibit flexible PC delivery models. Cultural misconceptions in equating PC with hospice or limiting PC to end of life care persist among many in the US, including healthcare systems (Slusser et al., 2024). The US healthcare system operates as a mix of public and private entities, leading to variability in access depending on individual insurance status, health care providers and payor contracts, and geographic region (Dir 2640 US, 2025).
The purpose of this mixed methods systematic review (MMSR) was to critically appraise and synthesize quantitative and qualitative data to answer the following research questions: (1) What are the characteristics of PC access in non-hospital settings in the US for individuals living with cancer and their care partners?, and (2) What factors facilitate or deter whether PC is integrated early alongside standard cancer care?
Methods
This study was conducted in accordance with Joanna Briggs Institute (JBI) methodology for MMSRs which included the following steps: formulation of review questions; evaluation of existent knowledge; establishing eligibility criteria; development of a search strategy; searching and retrieval of relevant studies; critical appraisal of included studies; and data extraction, transformation, integration, and synthesis (Aromataris et al., 2024). A convergent integrated design was used for data transformation, integration, and synthesis (Sandelowski et al., 2006). This approach required transformation of the quantitative findings into qualitative descriptions. These qualitative descriptions were integrated with the findings from the included qualitative studies before data synthesis. This design approach allows for deep interpretation of this study’s phenomenon (Stern et al., 2020). The study’s review team (K.S., M.M., A.L.B., F.L., H.C.) has a wide range of clinical and research experience in PC, health care systems, and cancer care. To reduce bias and identify the influence of the study team members’ subjectivity, personal reflexivity using memo-taking and journaling during the study’s iterative processes was used. Personal reflexivity is an approach acknowledging that bias cannot be eliminated and adds rigor to how the researchers’ unique perspectives influence a study (Olmos-Vega et al., 2023). Throughout the systematic review, reflexivity was used to minimize bias while interpreting results. Rather than ignoring lived experience and perspectives, the study team actively acknowledged these experiences, ensuring they informed rather than distorted the study’s analysis. Evolving thoughts and potential biases were documented—both on paper and within Covidence—to maintain transparency and self-awareness. Regular discussions of the study team further helped refine interpretations and enhance objectivity. Institutional ethical review and approval was not required for this study since all data were retrieved from publicly available sources and the study did not involve direct interaction with participants or collection of identifiable personal information.
The conceptual framework of healthcare access guided our study approach (Levesque et al., 2013). Recognizing the complexity and varied interpretations of healthcare access, Levesque et al. (2013) identified five multilevel dimensions of access: approachability, acceptability, availability, affordability, and appropriateness (Table 1). The synthesized data were categorized into these five dimensions.
Five Dimensions of Access.

Source. Levesque, J.-F., Harris, M. F., & Russell, G. (2013). Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. International Journal for Equity in Health, 12(1), 1–18 (pp. 5–6). https://doi.org/10.1186/1475-9276-12-18.
Evaluation of Existent Knowledge
An initial search in PubMed, Cochrane, and PROSPERO was conducted to confirm a gap in existent reviews examining PC access and early integration in the non-hospital setting for individuals living with cancer and their care partners. This gap was confirmed after examining 77 publications about PC, inclusive of systematic, scoping, and integrated reviews. The 77 reviews focused on (1) patient outcomes such as QOL and mortality; (2) broad patient populations not specific to cancer or populations with a specific cancer diagnosis; (3) settings not limited to non-hospital locations, and (4) a singular PC delivery model such as telehealth or home care.
Inclusion and Exclusion Criteria
Population
The inclusion criteria were intended to capture a diverse population based on gender, race and ethnicity, socioeconomic factors, and cancer type. Studies were considered if they included individuals living with cancer, care partners to those with cancer, or oncology and PC clinicians providing care to individuals living with cancer in the outpatient setting. Individuals living with cancer were defined as adults with solid tumors or hematologic malignancies being treated for their cancer in the outpatient setting. Care partners were defined as unpaid caregivers or family members. Clinicians included healthcare professionals providing care to those with cancer. Individuals identified as near the end of life (EOL) and under 18 years old were excluded.
Phenomena of Interest
Studies investigating and exploring PC integration alongside standard cancer care in the non-hospital setting were considered. The definition of early PC integration is inconsistent in the literature (Hui et al., 2022); therefore, studies were broadly considered if the intervention or phenomena involved PC. For this study, early integration of PC refers to the provision of PC concurrently with anti-cancer treatments, regardless of prognosis. PC descriptions that described study population as EOL or described PC interventions focusing on EOL or hospice care were excluded.
Context
Studies in the non-hospital setting were included. The non-hospital setting was defined as stand-alone PC clinics, embedded PC clinics or teams within cancer clinics; home- and community-based PC; and telehealth PC. Exclusion criteria included studies examining PC access and use in nursing homes, extended care facilities, and inpatient units. All studies were conducted in the US.
Types of Studies
Quantitative, qualitative, and mixed methods studies were considered for inclusion. Quantitative studies included randomized clinical trials (RCTs), cohort studies, quasi-experimental studies, and cross-sectional studies. All types of qualitative studies were considered. Mixed methods studies where data from the quantitative or qualitative results could be extracted were also considered. Review studies, protocols, quality improvement (QI), gray literature, and published abstracts were excluded. Protocols, QI studies, and abstracts were excluded as they do not align with this MMSR’s intent to follow a standardized process for quality appraisal and synthesis of results.
Search Strategy
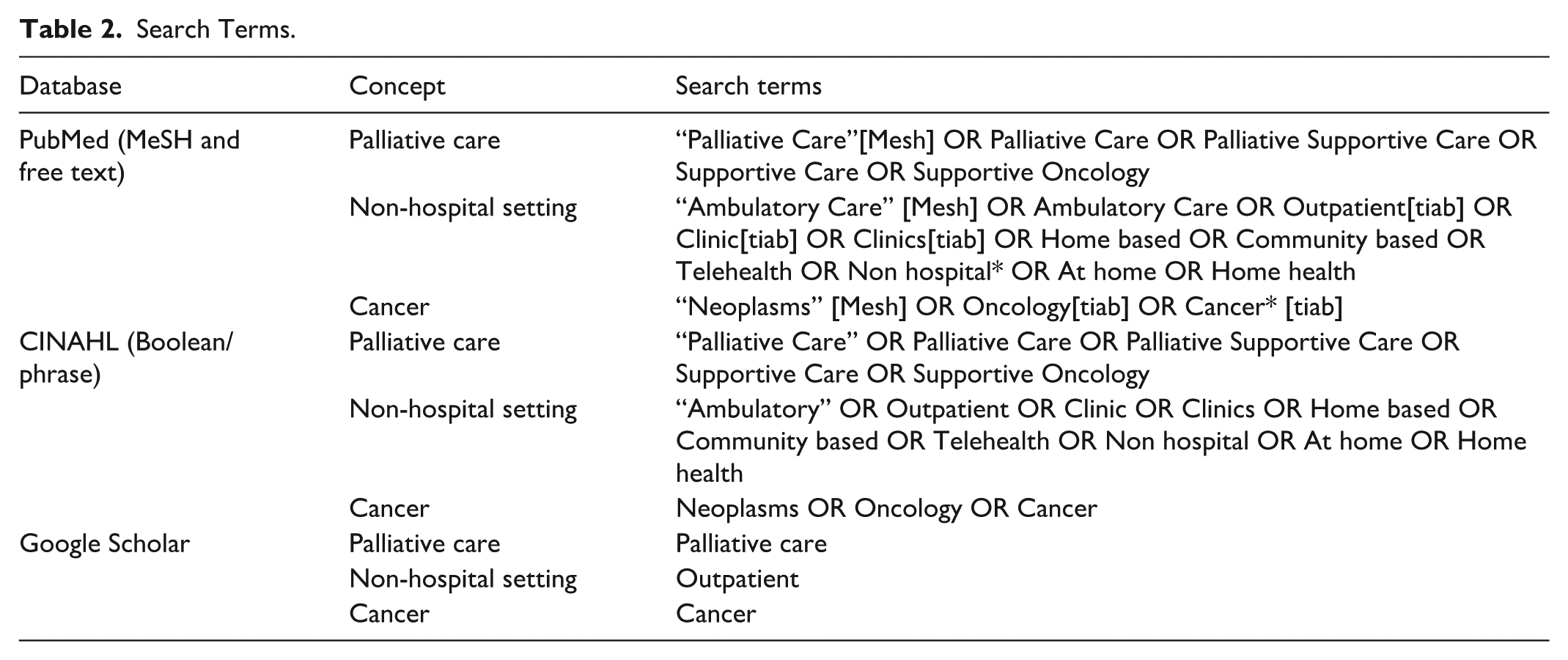
Aligning with JBI methodology, the search strategy followed the Preferred Reporting Items for systematic review and Meta-Analysis Protocols (PRISMA-P) standards (Moher et al., 2015). After consultation with a university librarian and preliminary trial searches, search terms were determined (Table 2). Searches were conducted by K.S. in PubMed and CINAHL databases. Manual review of Google Scholar, and hand searches from email alerts and related articles’ references were completed. Studies were limited to publications in English from January 2013 through January 2024. A 10-year timeframe was used to capture consistent components of early PC over time and identify emerging new approaches. Searches were performed from January 23, 2024 through February 12, 2024.
Search Terms.
Study Selection
Identified citations were uploaded into the citation management system, EndNoteTM (The EndNote Team, 2013). The references were exported for screening, full text review, data abstraction, and critical appraisal to Covidence, a web-based collaboration software platform that supports the production of systematic reviews (Covidence Systematic Review Software, 2024). K.S. screened titles and abstracts based on inclusion and exclusion criteria. Studies meeting inclusion criteria were retrieved for full text review. K.S. and A.L.B independently reviewed and compared results. Studies that did not meet criteria were excluded. Results were reported using the 2020 PRISMA flow diagram (Page et al., 2021).
Assessment of Methodological Quality
The selected studies were independently assessed for methodological quality by study team members K.S. and F.L. using JBI’s qualitative and quantitative critical appraisal checklists (Aromataris et al., 2024, Barker et al., 2023; Lockwood et al., 2015). The appraisal checklists allow for answers of “yes,” “no,” “unclear, or “N/A.” In accordance with JBI Manual for Evidence Synthesis, all selected studies were included regardless of methodological quality (Aromataris et al., 2024). Appraisal results were summarized, and a score was assigned based on the percentage of criterion met for each study. Studies were determined to be high quality if they met most (80% or more) of all appraisal criteria and moderate if 50% to 79% of criteria were met. Less than 50% of criteria met were considered low quality. Qualitative data were assigned a level of credibility by K.S. of unequivocal, credible, or not supported (Aromataris et al., 2024).
Data Abstraction
A data abstraction form was created in Covidence to correspond with JBI guidelines (Aromataris et al., 2024). The data were abstracted into Covidence by K.S. and verified by A.L.B. Data abstracted included authors, location, population, study methods, aim, model and description of PC if provided, and primary findings. Authors were not contacted about missing information or additional data.
Data Transformation, Integration, and Synthesis
Thematic analysis was conducted using a convergent integrated design (Aromataris et al., 2024). The efficacy, effectiveness, and narrative descriptive findings from the quantitative data were manually transformed into qualitative textual descriptions (Hong et al., 2017). As quantitative data was abstracted, data transformation occurred in parallel. Then, the transformed quantitative data were integrated with the qualitative data based on similarity in meaning. After data integration, the data were organized and synthesized within the conceptual framework for healthcare access’ five dimensions of access (Levesque et al., 2013). The initial data categorization and organization was conducted by K.S. After initial data categorization, study team members (K.S., M.M., A.L.B., F.L., H.C.) reviewed the findings, providing feedback and insights until consensus was reached.
Results
Study Inclusion
The initial literature search yielded 5,092 citations. After removal of duplicates and title and abstract screening, 484 articles were identified for full text review. Three studies were unable to be retrieved. After full text review, 51 articles were selected for extraction (see Figure 1). A summary of the extracted data was created including author, aim, study design, location, number of participants, population description, inclusion and exclusion criteria, key findings, and relevant notes (see Supplemental File 1).

PRISMA for study selection.
Methodological Quality
All studies were appraised for methodological quality. Quality scores were moderate to high quality, scoring 62% to 85% for RCT studies (n = 9), 89% to 100% for cohort studies (n = 8), 63% to 100% for quasi-experimental studies (n = 4), 70% for the case series study (n = 1), 60% to 100% for qualitative studies (n = 11) and 56% to 83% for mixed methods studies (n = 6). Cross sectional studies had a larger range from low to high quality with scores of 50% to 100% (n = 12). Of the qualitative studies, seven of the studies’ findings were ranked unequivocable (Dionne-Odom et al., 2018; Formagini et al., 2022; Hay, Lefkowits, Crowley-Matoka, Bakitas, Clark, Duska, Urban, Chen, et al., 2017; Hay, Lefkowits, Crowley-Matoka, Bakitas, Clark, Duska, Urban, Creasy, et al., 2017; Schenker et al., 2014; Siler et al., 2018; Yoong et al., 2013) and four studies’ findings were ranked credible (Back et al., 2014; Bergman et al., 2016; Fink et al., 2020; Keim-Malpass et al., 2015). Of the six mixed methods studies, the rankings for the qualitative data findings included two unequivocable (Dillon et al., 2021; Schenker et al., 2018) and four credible (Bagcivan et al., 2018; Larson et al., 2023; McLouth et al., 2023; Sadang et al., 2023).
Certain findings from the quality appraisals are worth noting. The quality scores for the RCTs reflected that the studies were not blinded to those delivering the treatment, which is understandable in PC intervention studies. Lower scoring qualitative studies lacked description of the philosophical perspective, limiting the ability to determine congruency with the research methodology. Lastly, a notable pattern with the mixed methods studies was the absence of researchers stating how their influence on the study was addressed.
Characteristics of Included Studies
The studies were conducted in all regions of the US (United States Census Bureau, 2024). Most of the studies were conducted in the South (n = 18) with 61% (n = 11) of the South region studies conducted in Texas. The South was followed by the Northeast region (n = 10), West (n = 7), Midwest (n = 6), and multiple states representing all regions (n = 6). Four studies did not disclose the state(s) where the study was conducted. Seventy-five percent of the studies included sites at NCI Cancer Centers and Comprehensive Cancer Centers or Academic Medical Centers. Twenty-five percent of the studies were conducted in rural and other community-based locations.
Individuals living with cancer were the participants in most studies (n = 29), followed by clinicians (n = 11) and care partners (n = 4). One study included patients and care partners, three included patients and clinicians, and three included patients, care partners, and clinicians. Most individuals living with cancer were identified as White race or Caucasian. Smaller percentages of participants were of Black race, Hispanic ethnicity, and Asian ethnicity. Three studies specifically focused on historically minoritized populations (Dionne-Odom et al., 2022; Fink et al., 2020; Larson et al., 2023) and seven studies focused on patients living in rural regions (Bagcivan et al., 2018; Bakitas et al., 2015; Dionne-Odom et al., 2018; Fink et al., 2020; Keim-Malpass et al., 2015; Larson et al., 2023; Orsak et al., 2019). Many of the studies did not include the education level of the participants, but when provided, most individuals living with cancer had a high school diploma or higher level of education. Most had stage III and IV solid tumor cancer diagnoses. Care partners were often family members living with the patient. Clinicians included physicians, advanced practice nurses, nurses, and clinical and lay navigators.
The definition and timing of early PC integration varied. Many of the studies described the delivery of PC as a standalone clinic within a cancer center or in close proximity to a cancer clinic. Yet, several of the studies described PC as embedded within the cancer clinic. The embedded PC services consisted of primary and specialty PC approaches. Other studies examined and compared standalone and embedded PC clinics. There were a few studies that solely examined the use of PC telehealth. One study examined a PC home-based program (Fink et al., 2020). PC delivery was most often described as provided by an interdisciplinary team (IDT) consisting of physicians, nurse practitioners, registered nurses, social work, chaplain, and other healthcare professionals. Embedded PC clinics varied whether they had a full complement of an IDT; and embedded PC clinics had fewer days and hours of operations than standalone PC clinics (see Supplemental File 2).
Data Synthesis Describing PC Access and Early Integration
The synthesized findings of PC access and early integration are provided in Table 3. Themes emerged in all five dimensions of access. This section provides a summary of the synthesized data in each dimension as well as descriptions of overlapping themes across multiple dimensions.
Synthesized Data Within the Levesque and Colleagues’ Five Domains of Access (2013).

Approachability
Individual and care partner lack of knowledge and misconceptions of PC were identified as a limiter to approachability. Provider decisions regarding information and explanations about PC they provide to individuals living with cancer and their care partners influenced individual and care partner PC knowledge and transparency of available PC services. Misconceptions of PC most often included equating PC with EOL (McLouth et al., 2023; Schlichte et al., 2024). Moreover, the ability to identify an individual that could benefit from PC was limited due to clinician uncertainty of when to integrate PC and unclear pathways for referral to specialty PC (Anderson et al., 2022; Dillon et al., 2021; Keim-Malpass et al., 2015). Yet, to facilitate accurate information and expectations of PC, it was suggested that oncology clinicians directly confront PC misconceptions of individuals living with cancer and their care partners (Formagini et al., 2022; Hay, Lefkowits, Crowley-Matoka, Bakitas, Clark, Duska, Urban, Creasy, et al., 2017).
The findings also highlighted the significance of outreach in enhancing or hindering approachability. While PC telehealth was found to be a successful strategy for outreach in rural and underserved populations, there was also evidence that the ability of PC telehealth to reach underserved populations was compromised due to limited technology literacy and access to the internet and devices (Dionne-Odom et al., 2018; Sadang et al., 2023). Individuals receiving cancer care at academic medical centers and NCI cancer centers and comprehensive cancer centers demonstrated higher awareness of PC, but this was tempered by individuals still experiencing anxiety when referred to PC (Schlichte et al., 2024). Oncology clinicians facilitating goals of care conversations was recommended to increase early PC (Reddy et al., 2023). Cancer clinics with embedded PC services were effective in providing early PC integration. Additionally, PC education provided to oncology clinicians prior to the implementation of embedded PC clinics further contributed to early PC integration (Bergman et al., 2016; Hui et al., 2018).
Acceptability
Several key factors were identified as influencing the acceptability of early PC integration, irrespective of the type of outpatient setting and whether the services were provided in rural or urban areas. Acceptability of early integration of PC hinges on whether individuals and clinicians view PC as desirable and compatible with their values, expectations, and needs. The preferences of individuals living with cancer and their care partners informed clinicians’ decision to refer to or discuss PC. Early PC integration was more readily accepted when individuals living with cancer were experiencing distressing pain (Saravia et al., 2022) or were diagnosed with later stages of cancer (Schlichte et al., 2024). While some oncology clinicians reported feeling a sense of failure when referring individuals to PC, it was noted that PC programs valuing the long-term relationship oncology clinicians have with their patients (Hay, Lefkowits, Crowley-Matoka, Bakitas, Clark, Duska, Urban, Creasy, et al., 2017) and a commitment to communication and coordination of care from the PC team can facilitate PC referrals and clinician acceptability (Anderson et al., 2022; Bergman et al., 2016; Hay, Lefkowits, Crowley-Matoka, Bakitas, Clark, Duska, Urban, Chen, et al., 2017; Keim-Malpass et al., 2015; Rosenblum et al., 2023).
Availability
The availability of PC and early PC integration were influenced by PC proximity to the clinics. IDT and PC services coupled with proactive, intentional follow up supported early PC integration. However, PC IDT models were often limited to standalone PC clinics. This segregation from the cancer clinics posed a barrier to early PC integration compared to cancer clinics with embedded PC (Agne et al., 2021; Guay et al., 2014). Individuals living with cancer may live far from the PC clinic, especially in areas with underserved populations where longer wait times for PC were more common (Cervantez et al., 2018; Guay et al., 2014). To address availability issues for the underserved, elderly, rural and less resourced populations, strategies such as lay navigation (Fink et al., 2020) and embedded PC telehealth were implemented (Dionne-Odom et al., 2018; Sadang et al., 2023).
Affordability
Affordability of early PC integration was either facilitated or hindered due to personal time requirements, socioeconomic factors, and policy considerations. Although some clinicians feared that PC would be too time-consuming or costly, evidence suggest that offering PC referral in the oncology clinic did not consume more clinician time (Bergman et al., 2016). However, the broader cost landscape remains complex. Individuals often face non-monetary costs such as travel time and inconvenience of location, and long clinic days, as well as the added cost of PC appointments which deter early PC integration (Agne et al., 2021; Schenker et al., 2018). The economic capacity in rural areas was a limiting factor for telehealth PC due to the lack of internet services and access to mobile devices (Dionne-Odom et al., 2018; Sadang et al., 2023). From healthcare systems and policy perspectives, issues such as insurance coverage and interstate licensure regulations limited PC access, particularly PC telehealth capabilities (Sadang et al., 2023). Furthermore, organizational constraints, such as lack of PC specialty trained providers and competing staffing demands, can limit the affordability of PC in the US (Siler et al., 2018).
Appropriateness
Studies consistently demonstrated that nurse driven assessments employing validated instruments to inform the PC plan of care were commonly regarded as a means to ensure appropriateness. Some of the most commonly validated instruments used were discussed in the ENABLE (Educate, Nurture, Advise, Before Life Ends) studies (Bagcivan et al., 2018; Bakitas et al., 2015; Dionne-Odom et al., 2015). Furthermore, lay navigation, including in diverse populations, facilitated a more comprehensive understanding of the concerns of individuals living with cancer and their care partners, enabling the provision of appropriate and tailored PC services (Dionne-Odom et al., 2022; Ferrell et al., 2015; Fink et al., 2020). While IDT PC programs have a long record of benefiting individuals living with cancer and their care partners, the emergence of non-traditional PC programs without a full IDT complement also demonstrated positive outcomes. Early PC integration supported oncologists’ communication with individuals living with cancer are provided essential time to assist with interpreting information about cancer treatment and prognosis (Back et al., 2014; Yoong et al., 2013). However, Wong et al. (2019) noted that patients with less symptom burden may feel like referrals to PC were too early, underscoring the importance of timing and education.
Overlap Between the Access Dimensions
Overlap and intersecting relationships between the five dimensions of access emerged. For example, the relationship between approachability and acceptability was highlighted by the significance of the role oncology clinicians have in facilitating PC access and early PC integration. Individuals living with cancer rely on their oncology clinician to be the gateway for information, guidance, and navigation of care which can influence approachability and acceptability. Furthermore, acceptability and availability of PC access and early integration were enhanced by implementation of embedded clinics and telehealth services, even if the traditional PC IDT model could not be realized. Affordability and accessibility considerations highlighted the challenges with cost of care in the US, especially for underserved populations, and the time cost to individuals who may have to travel or spend long days at clinician visits.
Based on the conceptual framework for healthcare access (Levesque et al., 2013) and findings from this study, a conceptual framework for early PC access for individuals living with cancer was developed (Figure 2). This new conceptual framework illustrates the facilitators and barriers to early PC access, considering the overlap between these factors among the five dimensions of access and the reciprocal relationships between the dimensions within all levels (individual, clinic, and healthcare systems).

Conceptual framework for early palliative care access and integration for individuals living with cancer.
Discussion
Using the conceptual framework of healthcare access (Levesque et al., 2013), this MMSR aimed to evaluate the characteristics of PC access and early PC integration alongside standard cancer care in the non-hospital setting for individuals living with cancer and their care partners. The synthesized results for PC access and early integration alongside cancer care illuminated multifaceted challenges and opportunities, providing a unique understanding of PC access and early integration in care of individuals living with cancer in the US.
The screening process yielded a substantial body of literature, underscoring the significance of the focus on PC. Methodological quality assessment revealed a range of scores across different study designs with most studies being of moderate to high quality. The geographic distribution of the included studies was across all regions of the US; however, a sizable number of studies were conducted in the South, reflecting potential regional disparities in research conducted in other parts of the country. A gap in the literature critically reviewed also highlighted the lack of research of individuals with hematologic malignancies compared to those with solid tumors. One study indicated that the evidence of attitudes of hematology oncologists towards PC was a reason for study exclusion of individuals with hematologic malignancies (Yu et al., 2019). This is concerning considering an intervention study of hospitalized individuals with acute myeloid leukemia found that individuals receiving PC alongside their cancer treatment reported better QOL and improvement in other symptoms as early as week 2 of admission and lasting throughout 24 weeks (El-Jawahri et al., 2021).
Nevertheless, many studies were conducted in urban academic medical centers or NCI cancer centers and comprehensive cancer centers with a majority of the population representing participants of White race and high education level. Previous studies found regions in the US with historically higher income and education levels to have greater access to access and use of PC (Osagiede et al., 2018; Rubens et al., 2020). Nadolny et al. (2023) found that historically minoritized and rural populations have limited access to PC resources. The findings of this MMSR found comparable results suggesting a need for improved access for this at-risk population and geographic regions in the US. Furthermore, results from this study suggest elements of availability and affordability may adversely influence PC access and early integration in rural and historically minoritized populations.
Approachability emerged as a critical concept influenced by factors such as clinical pathways, clinician uncertainty, and individual and care partner misconceptions. The challenges identified in this MMSR resonate with findings from international literature that emphasize the complexity of integrating PC early in cancer care outside of specialized PC settings (Öhlén et al., 2022; Sawatzky et al., 2016). Acceptability was influenced by individual and care partner preferences, stage of cancer, and clinician dependent referral processes. Proactive outreach such as lay navigation, routine, scheduled phone calls, and telehealth were found to be promising approaches to address availability challenges. The appropriateness of PC services was contingent upon the individualized alignment of services with the individual living with cancer and their care partner. Nurse-driven evidence-based needs assessment instruments and navigation models were effective strategies to tailor PC services to meet individual needs. The demonstrated effectiveness of nurse-led care delivery and embedded PC clinics in the US aligns with findings from a study in Canada examining nurse-led navigation to facilitate early PC in rural areas (Pesut et al., 2017). Due to the complex healthcare system in the US and available resources, affordability rose to be one of the most significant challenges in achieving PC access and early integration. These results highlight the need to advocate for change, consistent with international sentiment for capacity building, workforce training, and education to promote PC access and early integration (World Health Organization, 2022).
Recommendations for Practice
There are several implications for practice based on the findings from this study. Embedding PC within existing cancer clinics facilitates access in multiple ways. It provides PC access to individuals living with cancer and their caregivers, inclusive of opportunities for informal education and collaboration between oncology and PC clinicians. Optimizing telehealth and community outreach should be considered to address the unique challenges of both the patient/partner and proximity to a non-hospital-based clinic in which care is being delivered. Our current US healthcare financial model and varied state-to-state regulations affecting availability and reimbursement of PC needs to continue to be an area of clinician and healthcare system advocacy for policy and reimbursement structure changes. Strategies need to continue to address equity and inclusivity in PC regardless of background or socioeconomic status of individuals living with cancer. There are signals of positive change in regulatory and policy in the US that may facilitate PC access and early integration. Examples include a bill to expand access to PC which is currently being reviewed in Congress, and in January of 2024, Medicare policy changes now allow for reimbursement for navigation services (American Cancer Society Cancer Action Network, 2023; Expanding Access to Palliative Care Act, 2023).
Unfortunately, this MMSR did not provide further consensus regarding the definition of early integration of PC which was a similar finding as Hui et al. (2022). Hui et al. (2022) suggests focusing on timely PC vs early PC and using a standardized referral criteria and process for screening to improve PC services as part of cancer care.
Study Strengths and Limitations
There are several strengths of this MMSR. The review was conducted using a comprehensive theory-driven design guided by Levesque et al.’s (2013) Conceptual Framework of Healthcare Access. The framework enabled the evaluation of multilevel factors influencing PC access and early integration within the five dimensions of access. Rigour was added by having independent study team member validation of studies selected for inclusion and quality appraisal of the included studies. Furthermore, by including both qualitative and quantitative studies and synthesizing results using a convergent integrated approach, this MMSR captured the complex nature of PC access and early integration, allowing for a deeper understanding than would be possible through a single-method review.
It is also important to note the limitations of this study. While multiple study members were involved in independent review for inclusion and quality appraisal of the included studies, only one study member conducted the abstract and title screening which could increase risk of bias in elimination of relevant studies. Also, due to the vast number of studies, this review did not include other types of literature such as quality improvement and grey material which can increase the risk of publication bias as studies may be overrepresented with positive findings since studies with neutral or negative findings are less likely to be published. The thematic analysis was also limited to synthesizing results into the five dimensions of access which may have limited the discovery of new themes or concepts to be considered when evaluating PC access and early integration.
Conclusion
In conclusion, this MMSR led to the development of a new conceptual framework and offers a comprehensive understanding of the factors influencing access and early integration of PC in non-hospital settings in the United States for individuals living with cancer. As healthcare policy and reimbursement landscapes evolve, there is an opportunity to reimagine how PC is integrated alongside cancer care. This MMSR contributes meaningful insights to inform practice, policy, and future research aimed at improving person-centered, timely, and equitable PC for all individuals affected by cancer.
Supplemental Material
sj-docx-1-gqn-10.1177_23333936251375184 – Supplemental material for Access and Early Integration of Palliative Care in the Non-Hospital Setting for Individuals Living with Cancer in the United States: A Mixed Methods Systematic Review
Supplemental material, sj-docx-1-gqn-10.1177_23333936251375184 for Access and Early Integration of Palliative Care in the Non-Hospital Setting for Individuals Living with Cancer in the United States: A Mixed Methods Systematic Review by Kim Slusser, Mary Beth Flynn Makic, Figaro Loresto, Ashley Leak Bryant and Health Coats in Global Qualitative Nursing Research
Supplemental Material
sj-docx-2-gqn-10.1177_23333936251375184 – Supplemental material for Access and Early Integration of Palliative Care in the Non-Hospital Setting for Individuals Living with Cancer in the United States: A Mixed Methods Systematic Review
Supplemental material, sj-docx-2-gqn-10.1177_23333936251375184 for Access and Early Integration of Palliative Care in the Non-Hospital Setting for Individuals Living with Cancer in the United States: A Mixed Methods Systematic Review by Kim Slusser, Mary Beth Flynn Makic, Figaro Loresto, Ashley Leak Bryant and Health Coats in Global Qualitative Nursing Research
Footnotes
Ethical Considerations
This was a review study and did not require informed consent or institutional review board approvals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.