
Abstract
The purpose of this study was to describe the nursing praxis of nurses and midwives on intercultural care in Poland with refugees from Ukraine. A qualitative descriptive study was conducted by an international, inter-professional research team, co-led by nurse scientists in the USA and Poland. In-depth interviews were completed in 2023 with 15 Polish nurses and midwives who cared for refugees from Ukraine. Nursing praxis was identified in four themes: Mobilizing resources, Clarifying health services, (In)visibility of trauma, and Discerning cultural nuances. Nurses were at the forefront of professional and volunteer efforts to assist refugees. Nursing praxis focused on building trust and creating a “sense of security” among refugees. There was a systemic lack of trauma-informed care and language access for nurses, hindering intercultural care. The study suggests nurses advocate for institutional support of qualified interpreters on health care teams where language differences persist. Nursing education should include intercultural care for war-affected refugees who are likely to experience long term psychological trauma. Ukrainian leaders could partner with investigators on research and program development for sustainable solutions in refugee communities.
Introduction
The people of Poland opened their country to millions of refugees from Ukraine in response to the humanitarian crises caused by the Russian invasion of February 2022. Poland reported over 17 million border crossings since the beginning of the war and nearly one million refugees now reside in Poland (United Nations High Commissioner for Refugees [UNHCR], 2024). Over the past 2 years, Poland has hosted more refugees from Ukraine than any other nation and has offered the greatest financial assistance with the help of the European Union (United Nations Office for the Coordination of Humanitarian Affairs [UNOCHA], 2024). Still, 40% of the Ukrainian population remain in need of humanitarian assistance (UNHCR, 2024).
The World Health Organization (WHO, 2021) established standards of care for refugees and immigrants although the degree of implementation and effectiveness of these standards is unknown. More recently the WHO Regional Office of Europe (WHORO, 2023) created an action plan for refugee and migrant health that calls for inclusive environments that promote public health, social justice, and well-being. We undertook this study to contribute to the WHO action plan by expanding the nursing research on refugee health. Thus, the purpose of this study was to develop intercultural care guidelines for nurses caring for refugees and to promote the health of refugees from Ukraine.
Background
Historical Context
While the history between Poland and Ukraine is deep and complex, a brief description of several historical events helps elucidate the complicated relationship between the two countries. In 1943 Ukrainian nationalist partisans massacred thousands of Polish villagers in Volhynia followed by more murders of Poles in Eastern Galicia. In retalitation, the Polish resistance movement killed thousands of Ukrainian community leaders and villagers (Mick, 2022). For some people, these historical events are still unresolved.
The two countries also had a common enemy in the Soviet Union who engaged in extreme victimization of Ukrainian and Polish people during the reign of communism. Joseph Stalin’s man-made famine in Ukraine between 1932 and 1933 killed 4 to 5 million Ukrainians from starvation. The Soviet security forces killed more than 100,000 Poles living in the Soviet Union and deported many more to Siberia in what became known as the “Polish operation” during the years 1937 to 1938 (Mick, 2022).
After the fall of communism in 1991, independent Poland and Ukraine entered into better relations. Poland, as a member of NATO and the European Union, has advocated for Ukraine’s membership in both organizations. Over the past 30 years, an estimated 1.5 million Ukrainians have emigrated to Poland, primarily for economic reasons. This Ukrainian diaspora has played an essential role in the reception and integration efforts of the current refugee crises (Kohlenberger et al., 2023). The residents of the Polish-Ukrainian border region speak both languages and have mixed ancestry (Mick, 2022). This is the historical context in which the study took place.
Current Health Status of Refugees from Ukraine
The vast majority of refugees from Ukraine are women and children. A recent study conducted with over 700 adult Ukrainians who crossed the borders of Poland and Hungary found PTSD symptoms were high in both locations (45.4% in Hungary and 44.8% in Poland), and higher among women than men (Kovács et. al., 2023). According to the latest WHO Emergency Appeal, 26% of women and girls in Ukraine experience violence by an intimate partner (WHO, 2024). Pregnant women and recent mothers have been identified as being particularly vulnerable to mental health problems (Rodríguez-Muñoz et al., 2023). Oviedo et al. (2022) interviewed 94 refugees on their coping strategies following resettlement in Poland, Spain, and Italy. Strategies that promoted resilience were having a reliable method of communication to stay in touch with loved ones, and prayer took on a heightened sense of importance (Oviedo et al., 2022).
Several recent studies have reported on the psychological needs of refugee children. Using a parent-reported Child and Adolescent Trauma Screen, Redican et al. (2024) surveyed over 2,000 Ukrainian parents who remained in Ukraine. The most commonly reported concern was low general happiness for both pre-school age (66%) and older children (77%) (Redican et al., 2024). Two qualitative studies, one in Estonia and the other in Germany, foregrounded the voices of children who fled the war. Toros et al. (2024) reported that refugee children in Estonia struggled with socialization and fear of rejection and emphasized the need for psychological support. In Germany, Chabursky et al. (2024) reported on the concept of double schooling, where older refugee children study both in their host country and in their Ukrainian school online. While double schooling provided a multifaceted learning environment, the academic burden was great and refugees’ psychological needs were unmet (Chabursky et al., 2024). A range of mental health difficulties among refugee children have been reported, including PTSD, depression, and behavioral problems (Glazer, 2023; Hodes, 2023). Yet, refugee youth and families do not readily seek preventive or primary care for behavioral health problems (Yeo et al., 2024)
Increased risk for infectious diseases has been related to the overcrowding and poor housing conditions refugees endure (Saleh et al., 2022). Vaccination coverage in Ukraine was already among the lowest in the WHO European Region even before the onset of the war (Rzymski et al., 2022). A campaign to increase vaccination coverage in Ukraine was interrupted by the Russian invasion, which caused further disruption to health care services in Ukraine, including vaccine availability (Hill et al., 2022). Still, a recent epidemiological study reported that Ukrainian war refugees in Poland did not have a negative health effect on the country (Korzeniewski et al., 2024).
Crucial health risks for adults fleeing Ukraine and the major challenges for health care systems in host countries include fragmented care of chronic conditions, such as cancer, cardiovascular, respiratory and endocrine diseases (Health Cluster Ukraine, 2023). Relocated Ukrainian older adults require regular care coordination to manage co-morbidities and chronic conditions (Zimba & Gasparyan, 2023). Fragmentation in health care has led to higher mortality and morbidity among refugees compared to the general population (Püsküllüoğlu et al., 2023).
With health and social systems in host countries facing ongoing challenges (Biesiada et al., 2023), adoption and implementation of evidence-based practice is essential to provide high-quality care (UNOCHA, 2024). In one of the only studies of Ukrainian refugee resettlement in the US, investigators reported on adaptation challenges in the area of mental health and stressors from displacement and separation (Childress et al., 2025). This is noteworthy, as nurses in the Canary Islands working with refugees from Ukraine reported a high number of psychosocial problems related to war (Martín-Dorta et al., 2025). Three other recent nursing studies, reporting on care of refugees’ from Somalia, Syria, and Ukraine, highlighted the need for better trauma assessment and psychosocial care regarding incidents of gender-based violence (GBV) (Capasso et al., 2022; Olukotun et al., 2025; Öztürk et al., 2023). As members of professional organizations, nurses and midwives need to take the lead globally to advance the UN Sustainable Development Goals, such as gender equality (Hawkins et al., 2025). For this to occur nurses and midwives need better institutional support and preparation to implement person-centered approaches using effective intercultural care strategies.
Theoretical Assumptions
We use the term nursing praxis to illustrate the process by which a theory or skill is applied or put into practice to address real-world problems (Freire, 2009; Mayo, 2020). A vital component of nursing praxis is intercultural competence. At the individual and contextual levels, intercultural competence includes self and other awareness, shared goals, and sensitivity to equality and human agency (Arasaratnam, 2016). At the macro-level, intercultural competence is the ability of systems to accept and adapt to a wide range of values, beliefs and behaviors, and to tailor programs to meet social, cultural, and linguistic needs (Bennett, 2008). This study is also informed by Campinha-Bacote’s (2002) five interrelated constructs necessary for effective intercultural care: building cultural awareness; acquiring cultural knowledge; applying cultural skills; experiencing cultural encounters; and nurturing cultural desire.
While intercultural and cultural competence have been used interchangeably, in this study we use intercultural competence as it encompasses a systems approach (Arasaratnam, 2016). When nurses are fully engaged in the praxis of intercultural care the expected outcomes are reduced health disparities and improved health equity (Leyva-Moral et al., 2023; Velasco et al., 2022). Worldwide, nurses and midwives are often the first point of contact for refugees and play a key role in assisting in refugee integration to a new country (Lau & Rodgers, 2021). Identifying refugees’ needs and providing adequate care largely depends on nurses’ intercultural competence. Interculturally prepared nurses and midwives understand that values, beliefs and practices are shaped by socioeconomic, political and historical viewpoints. Political and historical factors are strongly linked to the current Ukrainian refugee crisis. Armed conflict and the need to flee the country affect social and economic factors.
Method
An international, inter-professional team conducted a qualitative descriptive study in Fall 2023 as the second part of a three-part initiative to develop an evidence-based practice model of intercultural nursing care for war-affected refugees. Qualitative description was used to answer questions of clinical importance, generate findings that remain close to the data, and communicate results in a coherent and useful manner (Sandelowski, 2010). Two nurse investigators (KLL and LPZ) co-led the study: one from North Carolina with expertise in migrant and refugee health and the other from Poland with expertise in adult health. Both had taught transcultural content in their respective nursing programs for over 20 years. The research team included a Ukrainian-American professor (NS) with expertise in human development and family science and a cultural anthropologist (JL) who is the Associate Director in the university Office of Global Affairs. Research approval was granted by East Carolina University Medical Center IRB [#23-000343] and Jagiellonian University Medical College [#118.6120.84.2023].
The first part of the three-part initiative described nursing student perceptions about the health needs of refugees from Ukraine through a global health international virtual exchange (IVE) course (Larson et al., 2024). Eighteen nursing students from North Carolina and Poland completed the global health IVE course in Spring 2023. Recommendations for intercultural nursing care were to (a) improve language access, (b) strengthen a trauma-informed care approach, and (c) engage Ukrainian community leaders in health promotion and disease prevention efforts (Larson et al., 2024).
The current study reports on the second part of the initiative, which elicited the perspectives of Polish nurses caring for refugees from Ukraine who had resettled in Poland. The nurse scientist from North Carolina (KLL) received a US Fulbright Scholar award to live in Poland from August to December 2023 and collaborate with the Polish nurse investigator (LPZ). This time allowed for a deeper understanding of Poland-Ukraine relations, and nursing education and practice in Poland. Data were collected from Polish nurses and midwives by KLL and LPZ in Fall 2023. The third part of the initiative, building consensus on the intercultural care guidelines by an expert panel of Polish nurses, is underway.
Sample and Setting
The nurse investigators recruited Polish nurses and midwives in-person during two professional development workshops held at a well-known nursing school. Approximately 50 to 60 nurses were in attendance from specialty fields of adult and maternal-child health. We explained the study, answered questions in English and Polish, and provided our email addresses to contact us if interested in participating. Inclusion criteria were Polish nurses and midwives who had cared for refugees from Ukraine since the February 2022 Russian invasion, currently working in the Małopolska region of Poland, and were Polish and/or English-speakers. We used maximum variation sampling to recruit participants who varied in age, marital status, gender, years of experience, and from different clinical settings. Gift cards were given to participants following each interview.
The Małopolska region of Poland borders Slovakia and is approximately 250 km from the western border of Ukraine. The district has numerous public hospitals (general and specialty) and primary care clinics, as well as private health care facilities. The National Health Service provides health care coverage to all working Poles and their family members. Poles may seek health care services from the private sector for a fee. Public transportation via bus, train, and tram is safe, efficient, economic, and accessible to public services, such as hospitals, clinics, and social welfare.
Data Collection
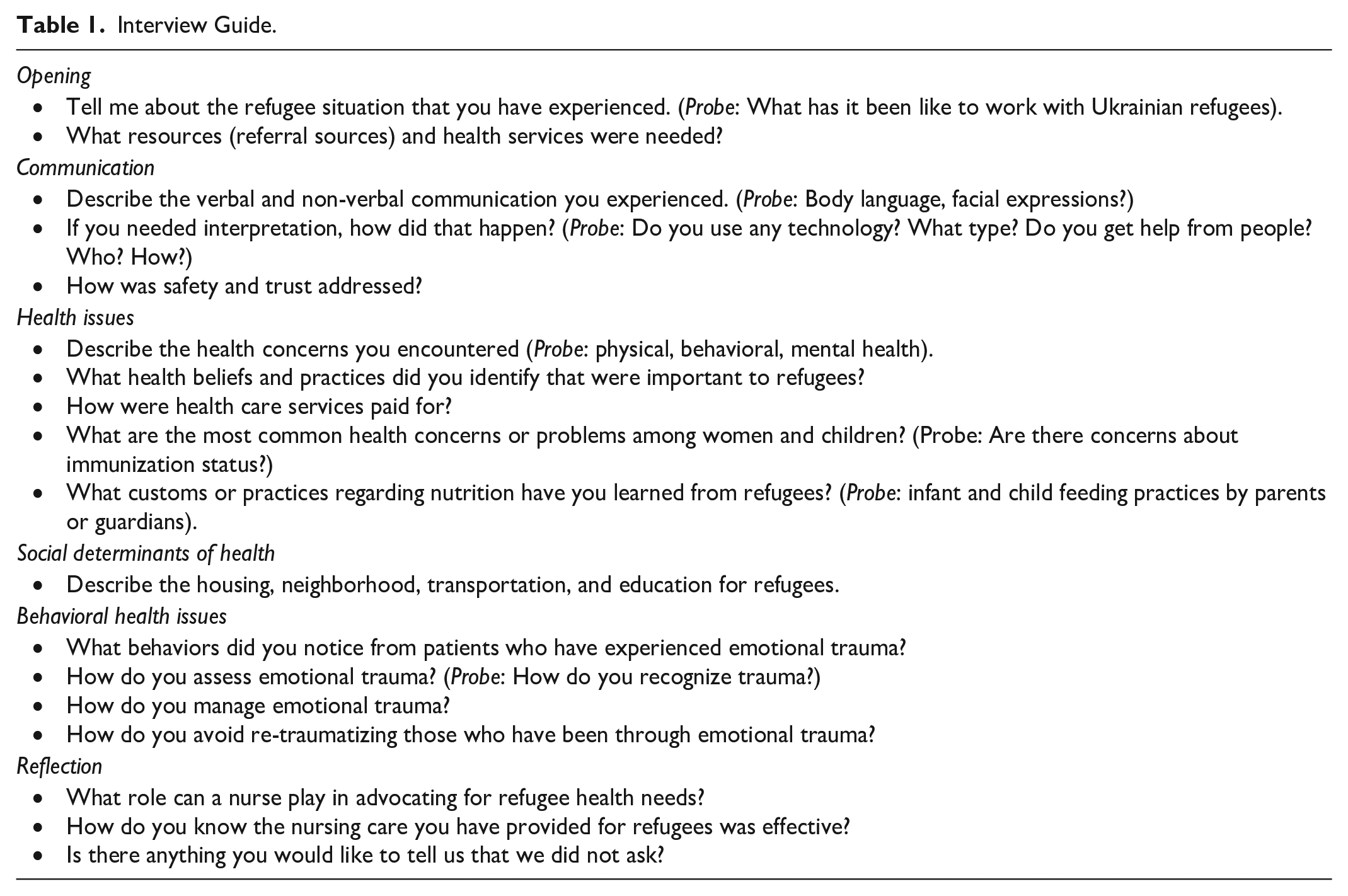
The two nurse investigators conducted interviews over a 10-week period using a semi-structured interview guide based on refugee health literature and developed by the international research team (see Table 1). Questions and prompts were designed to elicit opinions on the nurses’ responsiveness to the health, sociocultural and linguistic needs of refugees. For example, when asked about housing, transportation, and education for refugees, we prompted nurses to describe their involvement within and outside of clinical settings. Participants chose to be interviewed in either Polish or English. The lead nurses interviewed all participants in-person at the participant’s preferred location and time of day, for example, an office in the school of nursing or a private area in a coffee shop. Interviews lasted between 30 and 60 min, with an average of 40 min.
Interview Guide.
Data Management and Analysis
All interviews were recorded and transcribed. Interviews conducted in English were transcribed by the lead nurse from North Carolina and verified by the bilingual lead nurse from Poland. Polish interviews were transcribed by the Polish nurse investigator, then translated into English using the DeepL translation application, and were verified using the back translation method. Transcripts totaled 163 single-spaced typed pages. Next, both lead nurses read each transcript separately multiple times to understand each case on its own terms, writing memos, and highlighting key words. A codebook was created by identifying In Vivo and descriptive code words that were commonly used and those that offered unique or divergent viewpoints. Code words were given definitions and beginning with the first transcript both nurses independently applied the code words noting frequency of use and context. This process was followed iteratively to inductively code each successive transcript. Using the key words in context approach we merged similar code words producing coded segments. Following codebook revision, we proceeded with a cross-case analysis using a replication strategy where one case is studied in-depth and successive cases are examined for patterns, similarities, and differences (Miles et al., 2020). We displayed patterns, based on the coded segments, in various combinations of data matrices that captured references to nursing praxis and intercultural care (Sandelowski, 1995). Thematic content analysis (Patton, 2015) was used by organizing patterns to inductively derive subthemes and themes (see Table 2). Based on the sample recruited, we were able to attain a reasonable range of perspectives to address the purpose of the study (Thorne, 2020).
Thematic Analysis.

Ethical Considerations
We met with each eligible participant in a private location, described the study, allowed time for questions, and explained that they could leave the interview at any time. All participants signed informed consent. At the end of the interview, participants were invited to elaborate on content already discussed or add new information. Transcripts were de-identified, and pseudonyms were given to participants to be used in reporting aggregate findings.
Rigor
To promote transparency and improve trustworthiness we maintained an audit trail that included interview transcripts, field notes, codebook, and detailed records of analytic discussions among team members. An international, inter-professional research team provided analyst triangulation and contributed to analysis and interpretation of findings. The two lead nurses met weekly in-person during the Fulbright award period (August–December 2023) followed by weekly virtual meetings to reflexively question biases and assumptions. Where applicable (Braun & Clarke, 2024) we addressed the COREQ reporting criteria according to Tong et al. (2007).
Results
Fifteen participants, 13 nurses and 2 midwives, took part in the study. They were young or middle-aged adult women who worked in a range of clinical settings (see Table 3). We use the term nursing praxis to illustrate the process by which a theory or skill is applied or put into practice to solve real-world problems (Freire, 2009). Nursing praxis was represented by four themes: Mobilizing resources, Clarifying health services, (In)visibility of trauma, and Discerning cultural nuances. Exemplary quotes that support the findings are noted by pseudonyms assigned to each participant.
Demographic Profile of Polish Nurses (N = 15).
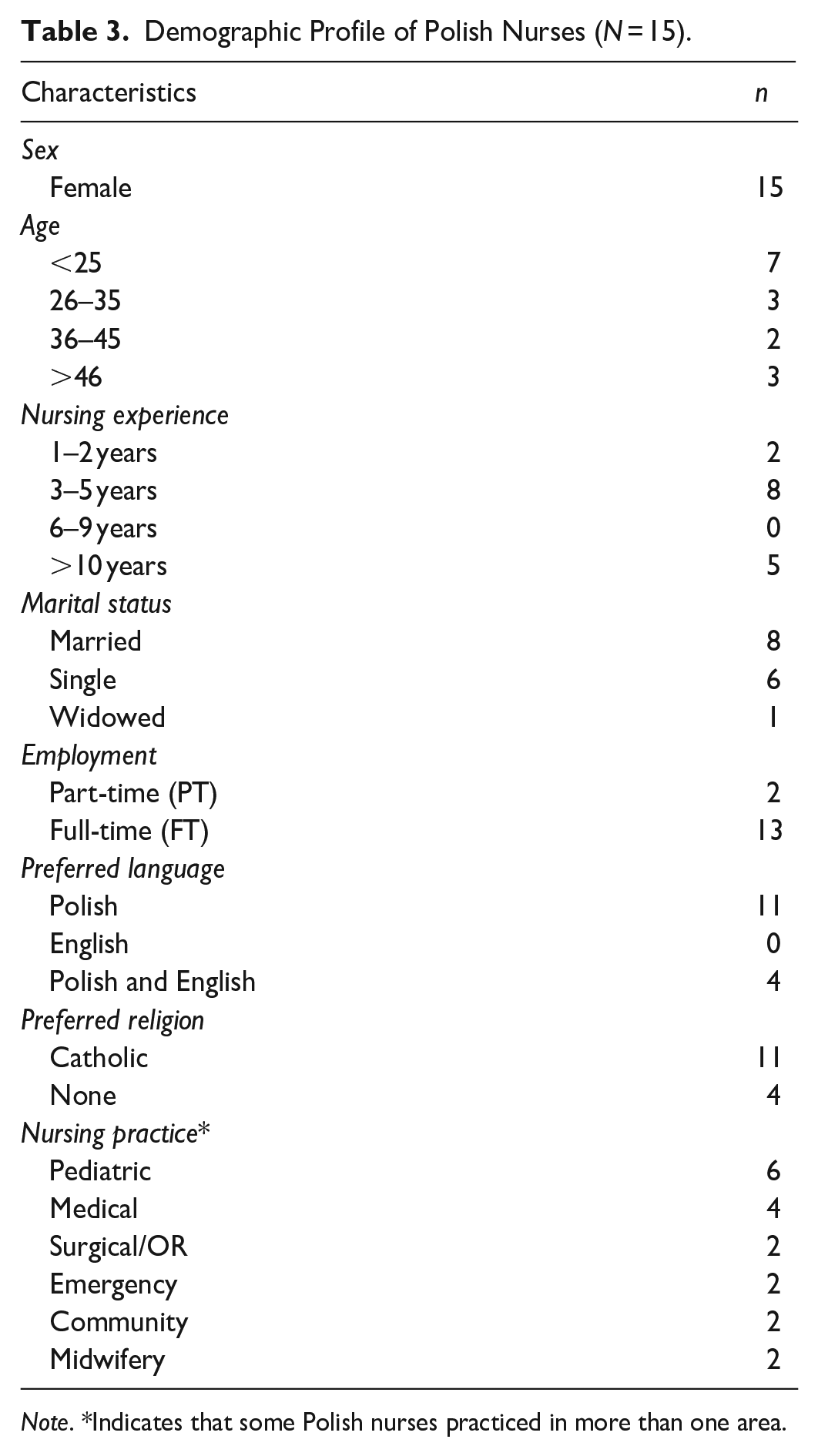
Note. *Indicates that some Polish nurses practiced in more than one area.
Theme I: Mobilizing Resources
Mobilizing resources was characterized by the actions Polish nurses and midwives took on behalf of refugees from Ukraine in managing public and private resources during a wartime crisis. These participants were aware that refugees who crossed the Ukraine-Poland border after the start of the Russian invasion would be given a Polish PESEL number (Powszechny Elektroniczny System Ewidencji Ludności/Universal Electronic Population Registration System), a requirement for access to health care. One midwife explained, Pretty much straight away there was a law on assistance for refugees, so they had health care provided from the National Health Service, so they were automatically insured. As soon as these people were given a PESEL number, it was already displayed to us in the system [computer] that this person was a refugee from Ukraine (Maria, midwife).
While receipt of a PESEL number was a requirement for health care, at the beginning of the war not all refugees received one when they crossed the border. One nurse described the problems, “but some didn’t register, some were waiting for hours or days, the queues were so long, at some point they [border patrol] were just letting people go without even stamping the passport, some came without documents” (Aneta, pediatric nurse). Yet, nurses ensured that care “was arranged without a PESEL. . .there was an option in the system. . .that it means there’s no PESEL and why [not] and there were options to choose from. . .” (Kaja, community nurse).
The mobilization of resources was also expressed by nurses in their support of Poland’s financial contribution and their own commitment to democracy, Poland made a huge effort to help refugees, and that is what we should do, nobody regrets that. We know that is how it should be. In my opinion, it’s a big burden to take on, but this is something worthwhile. It’s helping our neighbors, our brothers, and we don’t know in which case it could be the same situation for us and our families (Agata, ED nurse).
While nurses gave credit to their country for providing refugees with what they needed, they were at the forefront of organizing and distributing these resources. Participants ensured access to care even when documentation was not available. They distributed donations from private companies, such as lactation equipment, clothes, and food to refugees in need. Participants related how aid coalesed, I think that many Polish citizens offered to help, they bought some medical equipment, they offered people a house, a place to live, food, clothes, etc. A very big, a large amount of things, like resources, we gave to them (Wanessa, OR nurse).
In addition to providing clinical care for refugees, nurses and midwives purchased items, provided housing, and volunteered at refugee centers. One nurse disclosed, “I went there [refugee center] to help like because there was, you know, volunteers day and night. So, anyone with medical training could go there just to be there to help” (Karen, surgical nurse). Another nurse shared, “we were asked to help a family [a mother and her two daughters] from Ukraine. So we went to Slovakia to pick them up. The family stayed here [an apartment owned by her family]” (Aneta, pediatric nurse).
These nurses and midwives embodied Polish consciousness in their expression of nursing praxis through the mobilization of resources. They ensured that refugees received health care and basic necessities, and engaged in numerous resettlement activities, all while fulfilling their own personal and professional obligations.
Theme II: Clarifying Health Services
Clarifying health services was characterized by ensuring that refugees knew how and where to access primary and secondary care services. Nurses knew it was essential to have a General Practitioner (GP), yet first a PESEL was required, followed by selection from a slate of available GPs. Karen explained the importance of having a GP, “in Poland like you have to first go to your GP doctor and then you can go to [a] cardiologist, surgeon or whatever doctor you need. . .this is the first step and I think they did not understand.” The midwife working in the community related a situation where a Ukrainian family came in to select their GP and at the time there was a physician shortage, which limited access to primary care even for Poles.
Since not all refugees had a PESEL number immediately after arrival, a pre-requisite to selecting a GP, many of them used the Emergency Department [ED] for primary care, A lot of people, for example, went to the ED because they just didn’t know where they were supposed to go. And they also didn’t have a PESEL assigned to them at the beginning, so they didn’t have their family doctor to whom they could go, in fact, with an illness that didn’t qualify for the ED in our country (Klara, ED/pediatric nurse).
Nurses stressed the importance of support and information in navigating the Polish healthcare system. If refugees had not received a PESEL, nurses explained where in the city they could register. One midwife placed information about where to receive antenatal services on social media that aided both Ukrainian women and Polish clinicians working with refugees. Klara, a pediatric ED nurse remarked, “So, they mainly needed information - how it works in our country, because it’s extremely different from how it works in their country.” Agnieszka understood the logic of refugees, “If you live in Poland, you know where your family doctor is and know where to look for help, but if you are a refugee you need to go where the doctor is and in emergency [dept] you will find a doctor.”
Nurses and midwives endeavored to alleviate the confusion refugees experienced with the Polish healthcare system and improve health literacy, It was very difficult at the very beginning because the hospital did not yet have its procedures in place, it was not fully prepared for the influx of refugees. Various facilities were created later, there were also phone cards for Ukrainian refugees, but it was also our job to send them [to certain agencies] . . . so we had to create different maps . . . a lot of instructions in Polish, Ukrainian and translators were employed in the ED (Paulina, pediatric nurse).
While hospital care was paid for by the National Health Service, prescriptions were not routinely covered. Alicja noted, “I don’t know how it was with prescription drugs. I think they. . .had to go to the pharmacy and buy it.” This was especially true if a refugee did not have a GP. One nurse cared for a child with Type 1 diabetes who had left Ukraine without insulin. She explained, But here in Poland they had to have a PESEL, they had to go to the GP. . .so there was no support for Type 1 diabetes. How do you dispense insulin here in our country, which is on prescription and which is very expensive, if it is not reimbursed? And this is where such problems arose and often these people also came to the hospital simply for. . .obtaining this insulin (Paulina, pediatric nurse).
Uncertainty about fees for services and prescriptions, waiting periods, and not being understood caused confusion and frustration among refugees. Several nurses remarked, “they [Ukrainians] are just like us” and did their best to treat refugees from Ukraine the same as Polish citizens. Yet, one surgical nurse knew of cases where refugees received special treatment, Patients from Ukraine got the special treatment because, for example, patients in Poland to replace. . .the knee joint. . .they have to wait a year, two years. . .and Ukrainians [had to wait] like a week, two weeks. Pretty nice, [to have a] new knee or hip replacement. . .and we kind of didn’t like it (Katarzyna, surgical nurse).
In addition to organizing and distributing resources and assisting refugees with resettlement, nurses and midwives helped refugees navigate a complicated healthcare system. Still the on-going war was a strain on the nursing workforce and the Polish healthcare system and nurses observed, “they needed and demanded more from us than we could give them.”
Theme III: (In)visibility of Trauma
The (in)visibility of trauma was represented by two subthemes, manifestation of trauma among refugees and secondary trauma among nurses. Some nurses admitted to learning about war-related emotional trauma on-the-job. One nurse reflected, “in general I learned about trauma, this was the first time I met people who have experienced the war” (Justyna, ED nurse). This sentiment was echoed by several nurses, “For us, of course, I’m not talking about World War II, but for a long time we have not had these problems” (Agata, ED nurse). A third nurse reflected on behaviors she observed which might be associated with war-related trauma, I am not sure if it’s correct, if someone is very closed, even if you take a few minutes to connect with this person, and it doesn’t work, you see that it won’t work. Something causes that situation. It’s not normal for someone to not open themselves in medical situations. . .they don’t want to take the blood test. . .they don’t want us to touch their hand. . .I don’t know if this is trauma, but I think that it may be (Wanessa, OR nurse).
A midwife who helped hundreds of refugee women receive antenatal care services reiterated that refugee women “are afraid of touch, that the examination is frightening.” Most participants perceived that trauma was present and ongoing. One nurse vividly recounted caring for an older woman, It was the beginning of the armed conflict. . . She lost her husband straight away during the bombing, so we felt very sorry for her. . .I know that [she] called her family and then after each phone call she cried, she even screamed at times. . . so I think that this fear, this anxiety is still there (Beata, medical nurse).
Others observed behaviors suggestive of trauma, such as crying, anger, or fear, and knew that refugees needed mental health care. This nurse explained, We have so little time and I’m not sure if there was even a possibility for them to go anywhere because OK, I can refer them but what next, right? Where? To whom? You know so sometimes it’s you wanted to do more, but it’s . . . impossible (Karen, surgical nurse).
The nurses also recognized the possibility that their nursing care and hospitalization might contribute to re-traumatization. While nurses were cognizant of the trauma experienced by refugees, they were not prepared or trained to assess psychological trauma and psychological support was scarce. One nurse admitted, “I think it was quite neglected. . .and I think there was no time to deal with mental health.”
Considering that some participants learned about or experienced war-related trauma for the first time, the visibility of trauma varied widely. A few nurses noted that emotional trauma had subsided with time, “They don’t show as much trauma as they did at the beginning of the war. . .and then, more than a year, in my opinion, these features of trauma. . . calmed down a bit” (Alicja, medical/pediatric nurse). Since nurses did not have the skills to assess or recognize emotional trauma among refugees, they may not have been aware of secondary trauma among themselves. While several nurses reported they had cried when they heard stories of war from refugees, only one midwife shared a personal account of secondary trauma, I developed the syndrome [PTSD] by being around traumatized people. When I think that I very often didn’t have that thought, that I had a traumatized person around me, because too much and too fast was happening and too much these people were strolling around and that was it. Whereas I myself didn’t know that I had trauma, so it’s hard to determine that someone has trauma (Angelika, midwife).
This midwife was unique in her self-awareness of secondary trauma because of the frequent exposure she had with women who had experienced war-related violence. Yet, knowing the limitations of other participants in the assessment of trauma it is likely that they were unaware of secondary trauma to themselves. Whether nurses and midwives admitted to seeing trauma, most shared how trust, safety and a sense of security was integral in their work with refugees. One midwife understood that “once they felt safe, they knew how to do a lot by themselves. They know how to give birth, they know how to [breast]feed, they just needed a sense of security.” Klara echoed the importance of a safe place, We knew they were traumatized, we knew they were shocked and as much as possible we tried to talk to them, reassure them that they were safe here. And tried to build trust in a way that somehow we could work together, because as you know - collaboration is important in therapy.
Taking care of basic needs, treating refugees fairly, not asking about the war, and speaking calmly were ways these nurses and midwives handled trauma. Ultimately, in the absence of trauma-informed care training, nursing praxis focused on building trust and creating a sense of security.
Theme IV: Discerning Cultural Nuances
Discerning cultural nuances was represented by two subthemes, communication work and vaccination work. Nursing actions related to communication work and vaccination work were new to the nurses and midwives in this study, who were until now accustomed to caring for a homogeneous Polish population. Communication work entailed managing language differences between nurses and refugees and limited translation services. Thus, in order to deliver quality care they took action in various ways. One nurse approached hospital leadership, We asked the Director of the hospital if we could have a translator in-person, who is a professional translator, but they said it was impossible because of the money that they don’t have for such things. So we just went on (Justyna, ED nurse).
Another way was to call on Ukrainian hospital staff who spoke Polish to help with communication, but complicated procedures and instructions over-extended their Polish language capabilities. A surgical nurse recalled an emergency situation with a 6-year-old Ukrainian refugee. The nurse was in the operating room and was ordered to take a health history from the child, For example, are they allergic or when did they [last] eat something? He didn’t know what I was saying in Polish or English. . .I took out my phone and he used google translator but it didn’t work. . .so um we took a risk and just did the operation (Wanessa, OR nurse).
Finding an interpreter was essentially left up to the nurses, a job they were not prepared or trained for in nursing. Klara, an ED nurse, described working with a paramedic and a young doctor, both Ukrainian, who sometimes helped her communicate with refugees. Another nurse described, “the possibility that an interpreter could come to the ward. . .and in other situations we had to manage on our own. Some of us had some fundamentals of Russian, so that somehow combined with gestures enabled us to communicate” (Monika, medical nurse). Agata worked in an ED where there were no interpreters, she said, “if they came with a translator, it was a big help. But if they didn’t, we tried to use the phones.”
Nurses attempted to communicate with the help of a translation app on their personal cellphones. But numerous problems arose that made this channel of communication ineffective especially for persons with visual or hearing impairment; the very old or very young; and those with complicated medical conditions. Paulina recounted her concerns, “the problem with the keyboard, we have our Latin one, they have a Ukrainian one [Cyrillic script]. I wrote something to one mum, she wanted to reply to me, but she looks at my keyboard and is not able to write.”
Some participants would first discern the refugees’ language of preference before attempting translation. Angelika, a midwife, explained how the language of refugees varied by geographic origin. If they were from an urban area like Kiev or Lviv (on the western border of Ukraine), refugees could communicate in Polish or English. If they came from the eastern or rural regions of Ukraine they spoke Ukrainian or Russian. This midwife had connections with the medical school and solicited volunteers from among Ukrainian medical students.
Vaccination work involved discerning the immunization status of a refugee child based on the mother’s verbal confirmation. Nurses recalled how Ukrainian parents “escaped without documents of these children, so we could only believe what they said – that they were vaccinated or not” (Paulina, pediatric nurse). Discerning whether or not to accept a Ukrainian mother’s verbal confirmation of vaccination status was further complicated by the language barrier.
In the region where this study was conducted, unvaccinated children are not admitted to state childcare centers. Some Ukrainian children were not allowed to enroll in public daycare centers because they lacked documentation of immunization status. One pediatric nurse met with city officials about this situation to negotiate a change in the rule for Ukrainian children, As a result of his [city official] actions it was voted a few years ago that only vaccinated children should be admitted to local govenment nurseries and kindergartens. So I consulted him. . .and he said ‘No’ despite his sympathy for refugees because he goes there [to Ukraine] all the time with transports, ‘we only accept children who have confirmed vaccinations’ (Jolanta, pediatric nurse).
Low vaccination rates among Ukrainian children were documented in major health reports at the time and attributed mainly to the disruption in primary care services in Ukraine, but also to mistrust in vaccine quality, resulting in vaccine refusal or hesitency. Still, a few nurses believed that the low vaccination rates among refugees was a result of vaccines not being required in Ukraine. This nurse described her concern, “in Ukraine, vaccines are not obligatory. Here in Poland, vaccines are required. And now we have taken in many people who have not been vaccinated” (Agata, ED nurse).
Environmental adversity, with mass transportation at the border and crowding in the refugee aid centers, was noted by some participants that contributed to potential refugee contagion. Thus, environmental safeguards were taken by these nurses. Pediatric nurses in particular were more familiar with immunization schedules in both countries and acting out of precaution tried to mitigate transmission of infectious disease in the community, During that time, mostly kids were coming in already with infections and diseases because they had a different vaccination program as a nation. So they were kind of separated from the rest. They don’t have all the vaccinations that could protect them, so they were separated because of these infections. In addition to what they had to be treated for (Aneta, pediatric nurse).
Similarities in cultural beliefs about vaccinations were also noted. One nurse knew of parents from both Poland and Ukraine who believed that Down’s Syndrome was linked to certain vaccines. Other nurses knew of parents from both countries who had similar attitudes toward vaccination, It is known that there are parents [from Ukraine] who somehow think like Polish society . . .parents who have a normal, full vaccination calendar [immunization card]. Well, there are also people who think it’s unnecessary and it’s hard to convince them to do it (Gaja, neonatal ICU nurse).
One nurse called the conversation with parents about vaccinations “difficult.” While nurses heard of refugee children with communicable diseases, such as, tetanus, measles, and chickenpox, none had cared for children with any of these diseases. Importantly, over half of the study sample worked with adults and were unlikely to know of childhood infectious diseases.
Discussion
This qualitative descriptive study with Polish nurses and midwives suggests new information related to intercultural care and nursing praxis with refugees. The large and unexpected influx of refugees from Ukraine meant that the health care system did not immediately function smoothly. Still, nurses moved into action without systemic guidance or support. Praxis is the on-going process of applying theory to action, while reflecting on whether the actions address social justice and health equity (Sridhar et al., 2023). In this study, nurses and midwives engaged in nursing praxis by ensuring access to health and social services and recognizing their inability to address emotional trauma and language access. While institutional support in trauma-informed care and language access was limited, participants reflected on these limitations and determined to find solutions.
Emotional trauma and the manifestations of trauma symptoms among refugee children and adults was expected by these nurses. Despite major resources (i.e., health insurance, food, shelter) offered by public and private entities to refugees, psychological support was overlooked, and nurses were inadequately prepared in trauma-informed care practices. Lack of access to or inadequate psychological services are common problems not only in Poland, but also throughout the EU, which is exacerbated by stigma, waiting times and user fees (Bernardo et al., 2021). While several non-governmental organizations, such as the Polish-Ukrainian Zustricz Foundation (https://zustricz.pl), offered free psychological services to refugees, the nurses in this study were unaware of them. Poland recently launched the WHO Mental Health Gap Action Program (mhGAP) – an evidence-based approach to increasing capacity and services for mental health care under the National Health Service. Ukrainian refugees are also covered under this program (WHO Europe, 2023).
Historically, refugees experience tremendous pre-migration and post-migration stress and trauma, which can be ongoing for decades, and who may or may not be aware of it (Lor et al., 2022; Sangalang et al., 2019). In recent years, there has been increasing demand to incorporate trauma-informed care into nursing curriculum which can lead to improvements in trauma-informed knowledge, skills, and attitudes (Cannon et al., 2020; Holod et al., 2025). Polish nurses and midwives were not alone in their lack of preparation. Undergraduate and graduate nursing education across the USA has fallen behind other helping professions in trauma-informed care training (Li et al., 2019). A recent study at a Midwestern University integrated competency-based trauma-informed care in the nursing curriculum using a combined didactic- and simulation-based approach (Holod et al., 2025). The study assessed competency in implementing the seven trauma-informed care principles (safety, trustworthiness, peer support, collaboration, empowerment, communication, and sociocultural issues) and found that most students, after training, were at the novice or advanced beginner competency level (Holod et al., 2025). Despite lack of training, nurses and midwives in this study practiced two of the seven principles, ensuring a safe environment and providing trustworthy information.
A recent scoping review examined the application of trauma-informed care principles within sexual and reproductive healthcare among resettled refugee women who experienced GBV (Mathis et al., 2024). Investigators highlighted The Refugee Women’s Health Clinic in Phoenix, Arizona as a national model that was built with the goal of providing trauma-informed care in collaboration with women from the community affected by violence (Mathis et al., 2024). Intentional organizational structure and training in trauma-informed care could help prevent re-traumatization among refugees and avoid secondary trauma in nurses. It is also a first step in keeping refugee needs at the forefront of psychological support services to further extend this care.
Additional effort must be made toward the preparation of nurses and midwives around the world to meet the intercultural care needs of refugees. Ideally this training should involve a continuous learning process that integrates Campinha-Bacote’s five interrelated constructs: cultural awareness; cultural knowledge; cultural skills; cultural encounters; and cultural desire (Campinha-Bacote, 2002). While these constructs were evident through the interview data, findings allude to where more support and training for nurses were needed. For example, the lack of experience working with non-Polish speaking populations (cultural encounters) compounded many of the challenges faced by the nurses and midwives in this study. In mobilizing resources, they demonstrated a strong cultural desire, going beyond the scope of their jobs to help however they could. They also applied cultural skills in finding creative solutions to meet refugees’ needs. While participants developed strategies to navigate language barriers and address differences in vaccination practices, the challenges faced also highlighted insufficient cultural knowledge and cultural skill. The World Bank ranks Poland among the high-income countries with access to quality health care and education (The World Bank, 2023). Yet, after 2 years into the war, there is minimal infrastructure in place to integrate essential intercultural care practices. These findings suggest a lack of cultural awareness at the institutional level by not having the necessary support in place to care for a refugee population and emphasizes the need for supplemental nursing education for those providing refugee care.
Nurse-client communication is a facilitator of praxis (Rafii et al., 2022). Nurses in this study advocated for qualified interpreters after determining the refugees’ language of preference. These actions could be extremely time-consuming and in many cases the telephone or an untrained volunteer was insufficient. In the case of an emergency operation, when no interpreters were available, medically necessary steps/risks were taken. The language barrier impeded intercultural care notably, which is congruent with findings from another study where participants described “troubled communication” between refugees from Ukraine and nurses in Poland (Larson et al., 2024). While the EU has a Migrant-Friendly Hospital Initiative, competence in intercultural communication remains lacking (Bischoff et al., 2009).
In a review of literature, investigators found that utilizing professional interpreters rather than volunteers was essential to providing psychological care (Kirmayer et al., 2011). In Canada, precise guidelines exist for clinicians collaborating with interpreters that specify meeting with the interpreter before the encounter with the patient to establish ground rules and after the encounter to assess the interpreters’ emotional reactions or concerns (Kirmayer et al., 2011). The use of simple technology, such as smartphones, allows for fast translation to meet basic needs (shelter/food/maps) which may reduce the initial stress level of some refugees. But this technology is insufficient for complicated and complex health care needs. Many large hospitals in the US (serving persons who do not speak English) use virtual live certified interpreters and technology where clients are engaged in exchange of health information with clinicians using a virtual interpreter. This technology is expensive and was not available for these Polish nurses at the time of the study.
The most explicit description of nursing praxis was in the mobilization of resources for refugees. Without hesitation, nurses were on the front lines of organizing and distributing donations, offering shelter, and volunteering in refugee centers. Nurses and midwives engaged in nursing praxis in the community in additional ways – using social media to help locate antenatal resources and promoting vaccinations in community clinics. Potential next steps may be to gain support from health care organizations and institutions of higher education dedicated to health equity for a praxis-orientation to intercultural care (Hawkins et al., 2025; Sridhar et al., 2023).
Strengths/Limitations
Nursing research with refugees from Ukraine has been minimal to date. This is the first study that we know of to describe nursing praxis on intercultural care with refugees from Ukraine 2 years into the Russian invasion. Another strength of this study was in the international research team, including a member from Ukraine. Despite efforts to recruit male nurses, all participants were female, as most nurses in Poland are women. While the sample size has limitations, with only female nurses working in one region of Poland, the participants varied in age, years of experience, and clinical settings. They also shared rich description of their experiences and deep concern for refugees from Ukraine.
Implications for Policy and Practice
While this research focused on the care of Ukrainian war refugees in Poland, it has policy and practice implications for the intercultural care of refugees more broadly. Sinclair et al. (2023) report that host country reception is positive when war-affected refugees are culturally similar. Thus, European countries have welcomed refugees from Ukraine because of cultural similarity, but nurses all over the world must ensure health equity for culturally diverse refugees as well.
It must be recognized that refugees migrating from areas of conflict will likely experience on-going psychological trauma. Yet, nurses may not be equipped to evaluate and support individuals with war-related trauma. Care of refugees is further complicated by linguistic and cultural differences. Institutional support for nurses in the form of employing qualified interpreters and culture brokers as well as professional development seminars in trauma-informed care and intercultural competence could be especially useful. Methods that increase intercultural competence include combinations of study abroad, international virtual exchange, simulation, and reflection (Červený et al., 2022). Securing institutional funding for these opportunities, as well as language access services, will ensure that nurses can provide more effective intercultural care.
Public health outreach may be able to help bridge the gap between health care providers and refugees in terms of understanding each other’s health care systems, cultural contexts, and refugees’ health seeking patterns. An evidence-based approach to achieve health equity is to engage community members as equal partners in research and program development. The Refugee Dialogic Co-Creation Process is a community-based project to address mental health and psychological well-being of refugee and migrant youth recently implemented in six European countries (Sordé-Martí et al., 2023). Olukotun et al. (2025) delineate a framework for examining GBV in women with refugee status that calls for engaging affected women in the design and implementation of practical and sustainable interventions. In these projects, refugees provide local knowledge and social reality, while researchers provide knowledge from the scientific community. These projects have the potential to educate clinicians on refugees’ health-seeking behaviors in their home countries and provide nurses with important cultural context that can enhance care. Gepshstein et al. (2024) suggest that meeting the needs of refugees involves considering the adaptive skills and help-seeking behaviors of refugees, as well as the power dynamics that exist between refugees, clinicians, and health care systems in host countries. When these concepts are considered, clinicians can develop an intercultural approach to care by recognizing refugees’ knowledge, skills, and autonomy (Gepshstein et al., 2024).
Conclusion
While it is impossible to be prepared for all crisis situations, the experience and the response offered by Poland, to include a major national health service response, should be used as an example for other crises around the world. Providing additional resources and essential training to nurses specifically on trauma-informed and intercultural care for refugee populations, anticipating the need for linguistic support, and bridging the cultural gap are all critical for providing refugees quality and effective care to meet their health needs.
Footnotes
Acknowledgements
We would like to thank the participants who gave their time to this study. We appreciate the work of Marianne Choufani, graduate research assistant, in formatting references.
Ethical Considerations
The study received IRB approval.
Informed Consent Statement
All participants signed informed consent.
Author Contributions
KLL was responsible for methodology, project administration and supervision. KLL and LPZ were responsible for conceptualization, data curation, investigation, validation and writing. All authors were responsible for analysis, visualization, and reviewing and editing the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted during a Fulbright US Scholar award to Poland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are not available to the public. Individual requests will be considered.