
Abstract
Workplace bullying impacts at least half of the nurses worldwide. Despite the link to increased nurse turnover, few intervention studies have addressed bullying in the workplace. Since most studies report cross-sectional designs that provide little insight into the complexities of this phenomenon, the purpose of this descriptive phenomenology was to describe the lived experiences of nurses as they were actively being bullied in the workplace. Semi-structured interviews were conducted through Skype until data adequacy was realized with 12 participant interviews. Giorgi’s six-step method was used to analyze the data in Atlas.ti. A central theme, “The whole culture of nursing needs to change” described an organizational culture where managers were unable to identify or unwilling to respond to workplace bullying. The four themes identified from the data included “going to work can be really hard,” “not good for patient care,” “learning to live with bullying,” and “changing the culture.” Leaders of organizations should implement comprehensive anti-bullying programs to assess bullying in their workplace and to provide bullied nurses with reporting options. Nurse managers need to prevent workplace bullying by intervening when aware of bullying and cultivating a culture of mutual respect.
Introduction
Bullying is a social interaction between a person of low power, called the victim, and another person with perceived higher power, called the bully (Agervold, 2007). Scandinavian researchers first introduced bullying from schoolyard aggression studies in the early 1970s (Smith, 1997). Bullying manifests as repeated psychological aggression toward a person or a group of people (Bishop et al., 2006; Dellasega, 2009; van Heugten, 2013). Over the years, bullying expanded from a playground problem into a global workplace crisis for healthcare organizations (Donegan, 2012; Granstra, 2015; Zych et al., 2015).
Workplace bullying in healthcare contributes to the long-standing nursing shortage (Edmonson & Zelonka, 2019) that will grow by 2030 to 1 million in the United States (Juraschek et al., 2012, 2019), 2.5 million in Organization for Economic Co-operation and Development member countries (Scheffler & Arnold, 2019), and nearly 6 million globally (World Health Organization, 2020). Workplace bullying for nurses occurs at a rate of 10% to 50% but has been reported to be as high as 90% in hospital settings (Ceravolo et al., 2012; Cheung & Yip, 2017; Esfahani & Shahbazi, 2014). Women are bullied more often than their male counterparts (Gillespie et al., 2015; Lee et al., 2014); however, older experienced nurses are less likely to encounter workplace bullying than younger, less experienced nurses (Ovayolu et al., 2014).
Bullying in nursing creates a toxic workplace (Berry et al., 2016; Karatza et al., 2016) that harms victims, bystanders, and organizations (Emdad et al., 2013; Esfahani & Shahbazi, 2014). In addition, bullying negatively impacts teamwork in nursing units (Trépanier et al., 2016), a critical attribute for maintaining patient safety. Patients and family members are also at risk for harm (Altuntaş et al., 2014; Ariza-Montes et al., 2013; Chipps et al., 2013; Snavely, 2016) because bullied nurses are distracted from providing safe care and unable to build positive interpersonal relationships with patients (Karatza et al., 2016). Bullying negatively impacts the work of victims through decreased job attachment, increased stress, absenteeism, and intention to leave nursing (Ariza-Montes et al., 2013; Li et al., 2015). Cliques often facilitate bullying in the workplace (Barton et al., 2011) as they seek to maintain power or remain dominant (Anusiewicz et al., 2020). Behaviors associated with bullying include gossiping, name-calling, spreading rumors, and telling jokes but can also include humiliation, unsupportiveness, and vindictiveness (Anusiewicz et al., 2019; Arnetz et al., 2019; Fry & Schmer, 2021). As such, the nursing profession can be its own worst enemy (Edmonson & Zelonka, 2019), and nurses are vulnerable to these behaviors (Szutenbach & Stechschulte, 2008; Van Fleet & Van Fleet, 2012).
Workplace bullying adversely impacts less experienced nurses and new graduates entering the workforce (D'Ambra & Andrews, 2014; Granstra, 2015). Despite nursing being a well-established discipline with professional integrity (Epstein & Turner, 2015), nurses “eat their young” (Dellasega, 2009) as seasoned nurses often mistreat newer and less experienced nurses (Etienne, 2013; Granstra, 2015; Townsend, 2015). Although nursing students expected to “save the world” before graduation, they reported feeling like the “odd-one-out” 3 months after graduation (Barton et al., 2011). Because they felt alienated and experienced abuse from workplace bullying, nearly 60% of new nurses left their positions within 6 months (Edmonson & Zelonka, 2019). For these reasons, bullying is a different experience for novice and early career nurses than experienced and established nurses.
Victims of bullying experience psychological, emotional, and physical effects (Lee et al., 2014; Ovayolu et al., 2014). Adverse psychological problems that correlate with workplace bullying include anxiety, avoidance, depression, hyperarousal, low self-esteem, and stress (Berry et al., 2016). Bullied nurses report physical consequences, such as cardiac issues, headaches, hypertension, exhaustion, gastric discomfort, sleeplessness, and weight loss (Dellasega, 2009; Lever et al., 2019; Yildirim, 2009). If workplace bullying persists for any length of time, the protection from coping mechanisms decreases, which, in turn, increases the potential for post-traumatic stress disorder and suicidal ideation (Harrington et al., 2015; Li et al., 2015; Rodwell et al., 2013; Vessey et al., 2010). In one study, nearly half of nurses who reported workplace bullying were diagnosed with post-traumatic stress disorder (Tehrani, 2004).
Most workplace bullying research reported in nursing are observational studies using measurement instruments for data collection (Goh et al., 2022; Jang et al., 2022; Johnson, 2009; Lever et al., 2019; Liu et al., 2019; Rittenmeyer et al., 2013). A meta-synthesis and a cross-cultural scoping review of bullying among nurses revealed that the complexities of the phenomenon have not been adequately captured through the lived experience of nurses while being bullied in the workplace (Karatuna et al., 2020; Lee et al., 2022). Although researchers continue to call for nurse leaders to address bullying (Anthony & Brett, 2020), few interventions to address bullying are reported in the literature (Hartin et al., 2020; Jang et al., 2022). Only one study addressed intervention effectiveness, with findings lacking statistical significance (Hawkins et al., 2023; Rittenmeyer et al., 2013). Thus, a clearer connection is necessary between bullying as a nursing phenomenon and the development of interventions to address the experiences of bullied nurses. As such, the purpose of the current study was to describe the lived experiences of nurses actively being bullied in the workplace to inform the development of interventions and organizational policies.
Methods
Study Design
This qualitative study used a phenomenological descriptive design (Giorgi, 1985, 2021; Husserl, 1982) with an empirical (Giorgi, 1970, 2009) rather than transcendental (Colaizzi, 1973; Moustakas, 1994) approach. Descriptive phenomenology moves from describing the lived experience of participants being bullied to describing the structural essence (core structure) of bullying in the workplace as it appears to those who experience this phenomenon (Englander & Morley, 2023; Leigh-Osroosh, 2021). This approach was congruent with “nursing ideals where humanistic knowledge is valued” (Rose et al., 1995, p. 1123) to describe a phenomenon embedded in the individual consciousness of nurses (Neubauer et al., 2019). As such, the collective nursing experience was described with salient attributes and defining characteristics (Levitt et al., 2017) of workplace bullying to capture the lived experience (Willis et al., 2016).
Setting and Sample
Purposive sampling (Gentles et al., 2015) was used to recruit registered nurses currently being bullied who worked in health care organizations and educational settings in different areas of the United States. Facebook was the primary source for participant recruitment, and a purchased advertisement was used to target working nurses. The inclusion criteria for the study were nurses with at least 1 year of work experience who had been at their current position for at least 6 months, were working while being bullied, and were able to converse in English.
Data Collection
Data were collected between September 2017 and January 2018 through semi-structured interviews, with open-ended questions to encourage full responses (Phillippi & Lauderdale, 2018). As the data collection should “fit the phenomenon instead of the phenomenon being forced to fit the design” (Englander & Morley, 2023, p. 30), interview questions were created from a comprehensive literature review with feedback from clinical nurses practicing at a large health system. Two pilot interviews were completed to verify the questions would capture the experience of being bullied. No questions were changed based on the data collected during the pilot interviews. The pilot interviews were not included in the analysis.
The semi-structured interviews were conducted conversationally (Rubin & Rubin, 2012) and digitally recorded. The interviews began with demographic questions and continued with an opening question, “Tell me about your experience with bullying at work,” followed by probing questions grouped into three areas derived from a literature review. The three areas for probing questions included current experience with bullying, caring for patients while being bullied, and managing bullying (Table 1). The lead researcher conducted all interviews using Skype, a widely used technology to support research across countries (Krouwel et al., 2019), at a time selected by the participant. The interviews averaged 40 min (ranging from 30 to 70 min).
Semi-Structured Interview Guide.

According to Giorgi (2009), “research based upon depth strategies should not be confused with research based upon sampling strategies” (pp. 198–199). For phenomenology, strategies that gain a depth of information can achieve a sample with information power (Malterud et al., 2016). Recognizing that logical empiricism of data saturation is a “thorny concept” (Varpio et al., 2017) incongruent with thematic analysis (Braun & Clarke, 2021) we took direction from Giorgi (1988) who argues the goal of phenomenology is to collect the “proper evidence for knowledge claims” (p. 167). Guided by this approach, we determined that data adequacy was achieved when 12 participant interviews captured the depth, complexity, and range of experiences to address the aims of this study.
Data Analysis
Interview transcripts were analyzed in ATLAS.ti Scientific Software Development GmbH (2021), version 9.1.7, using Giorgi’s (1970, 1985) method for descriptive phenomenology (Figure 1). The six-step method used for the current study included (1) preparing for phenomenology by assuming the correct attitude, (2) reading the transcripts for data familiarity, (3) delineating meaning units from the whole data, (4) transforming meaning units into meaning structures, (5) synthesizing the essential structure identified to describe the phenomenon, and (6) applying the essential structure to empirical data to understand variations (Giorgi, 1985; Giorgi et al., 2017; Giorgi, 2006, 2009, 2012). To prepare for data analysis, the research team reviewed the philosophical paradigm and empirical process for descriptive phenomenology (Giorgi, 2009) and assumed the correct attitude for phenomenological reduction (Giorgi et al., 2017). This preparation is described in the method and illustrated as the first step for this research. The process for this research is illustrated in Figure 1.
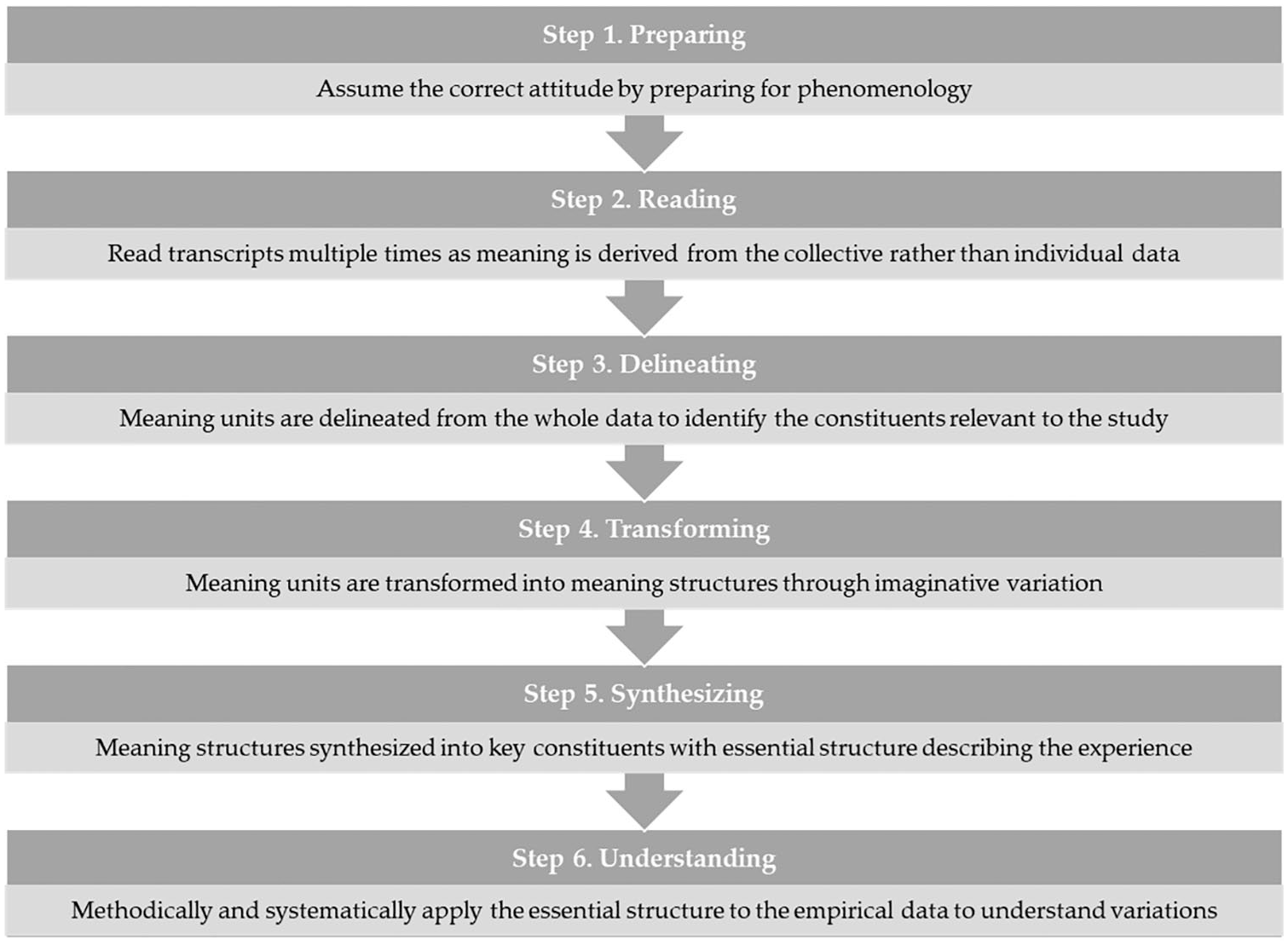
Six steps for data analysis using Giorgi’s descriptive phenomenology.
As the interviews were completed and transcribed, each transcript was read multiple times to understand the participant’s experience in the context of the phenomenon (familiarity with the data). Next, meaning units were delineated from the participant’s perspective relevant to the phenomenon (coding the data). The meaning units were then transformed into meaning structures that form the phenomenon (grouping the codes into subthemes). Then, the meaning structures were synthesized into an essential structure to make a cohesive statement that described the phenomenon (consolidating subthemes into themes). Finally, the essential structure was applied to the empirical data to understand variations in a methodological and systematic way. This important final step, called post-structural analysis, was described (Giorgi & Giorgi, 2003) but not previously illustrated as the final step (Giorgi et al., 2017). The analysis resulted in constituent subthemes and themes to describe the phenomenon of workplace bullying in nursing.
Trustworthiness and Rigor
The trustworthiness of qualitative data ensures credibility, transferability, dependability, and confirmability (Lincoln & Guba, 1985). Establishing trustworthiness requires a rigorous method with clearly described procedures (Guba & Lincoln, 1994). Credibility means the analysis is believable, confirmability means the data support the results, transferability implies the information applies to other contexts, and dependability indicates the findings are reproducible (Noble & Smith, 2015). The sampling strategy provided coherence through the epistemological congruency with the study design (Robinson, 2014). The primary investigator compared the transcripts to the digital recording for accuracy. Although all study participants reviewed the accuracy of their transcripts to capture their lived experience, none of the participants requested amendment or correction.
The researchers used phenomenological reduction (Giorgi, 1988) to bracket past knowledge and previous experiences from being imposed on the phenomenon (Beck et al., 1994). Reduction is a critical process for researchers to realize the epoché or the “pure mode of apperception” (Bernet et al., 1993, p. 62) essential for imaginative variation (Giorgi, 1985). This robust approach for data analysis, using multiple researchers, and our audit process ensured credibility and confirmability (Birt et al., 2016; Whittemore et al., 2001). An audit trail was maintained to document the processes with decisions and to ensure the credibility and dependability of findings (Akkerman et al., 2008; Koch, 2006). The audit trail is summarized in Supplemental File 1. Professional transcription from digital audio recordings was completed within 48 hours after each interview. Consistent with the data analysis for Giorgi’s (1985) approach, the researchers did not seek participant feedback about the findings as recommended in other approaches (Colaizzi, 1978). Additional methodological strategies were implemented to ensure the trustworthiness of the data, including coding checks, constant feedback, team meetings, and peer debriefing with an external researcher (Morse et al., 2002). Two team members participated in the coding process, and another additional team member performed an independent review to determine the accuracy of the coding process.
The current study was reported according to the quality criteria for qualitative research recommended by the Standards for Reporting Qualitative Research (O’Brien et al., 2014) and the Consolidated Criteria for Reporting Qualitative Research (Tong et al., 2007). However, these reporting criteria were tailored to align with Giorgi (1988) seldomly cited guidance for establishing reliability and validity in the context of a descriptive phenomenology with an empirical design, noting differences with the other approaches (Beck et al., 1994). The complementary but overlapping reporting recommendations address important details in justifying and describing the methodology and methods, researcher role and reflectivity, and data collection and analysis. Applying quality criteria tailored to reporting a phenomenological study results in a more “thorough, transparent, and trustworthy account of the data collection process, analysis, and the relationship to the findings” (Pardell-Dominguez et al., 2021, p. 4).
Ethical Considerations
The current study was approved by the Institutional Review Board at Walden University (protocol #: 08-29-17-0418151) and conducted according to the guidelines of the Declaration of Helsinki (World Medical Association, 2024). Informed consent was obtained from each participant and documented in the digital recording before beginning the interview. The original audio recordings were destroyed at the end of the study because the transcripts documented the interviews. All personal identifiers were removed from the transcripts before data analysis by the research team. The results are presented with pseudonyms for individual level data (quotes).
Results
The 12 participants were female, with 2 to 39 years of nursing experience. The participants were from different states, and all but one participant worked in the hospital setting. The complete sociodemographic data are provided in Table 2. Four themes and 11 subthemes described a central theme, “The whole culture of nursing needs to change” (Table 3). These themes described an organizational culture with workplace bullying. Participants expressed frustration, as they perceived managers struggled to recognize workplace bullying, were reluctant to intervene, or were involved in the bullying. For this reason, participants felt trapped, describing how they had to endure bullying or ultimately made the difficult decision to leave the workplace.
Participant Sociodemographic Information.

Themes and Subthemes.

Despite bullying being visible to most people in the workplace, participants shared feelings of abandonment and helplessness, as they perceived managers neither identified nor addressed bullying behaviors. Whether teaching in a classroom or providing patient care on a hospital unit, the participants frequently described bullies as holding either formal or informal power, which they believed contributed to the persistence of the bullying behaviors. One participant working in a university provided a short story that illustrates the pervasive nature of bullying with the direct involvement of a manager as the bully.
While I was in class, I was doing a lecture, and she [Dean] came to the door and she knocked and stuck her head in, and she said, ‘Would it be okay if I addressed the class for a moment? Because we need to talk about their election of class officers.’ And I said, Sure, come on in. So, I sat down on the opposite side of the room from the door. And the students were between me and the door. So, I was sitting there, and she talked about choosing officers, and they voted right then and there, and they selected their class officers. And then she says, ‘Now, I understand that some of you have some complaints about your nursing teacher.’ That was me. She said, ‘We’re going to talk about those while she’s here.’ She let them, 45 minutes of bashing me. From my voice, the way I walk, everything. Everything. And someone asked me later why I didn’t leave, and I said because I couldn’t get out of the room. They were between me and the door. I couldn’t get out. And I had to sit there and listen to them for 45 minutes. And when they were done, she said, ‘Now, don’t you feel better? Don’t you worry. I will fix this.’ And she walked out of the room. She walked out of the building down to her car and left for a vacation for two weeks. And the only thing that I could say, all the students looked at me, and the room was really quiet, they all looked at me, and I said, why don’t you go to lunch? And they all got up and left, and I picked up my things, and I was headed back down to my office, and one of the students stopped me in the hall, and she said, ‘Did you know that she was coming up to talk to us?’ And I said, No. And she said, ‘I didn’t think so because when I looked at you all the blood had drained out of your face.’ She said, ‘You had turned white.’ And I went into my room into my office, and I just put my head down and I just cried. (Janet)
Theme 1: Going to Work Can Be Really Hard
The participants described the negative feelings associated with their experience of going to work and being bullied. As the participants prepared for work in the morning, they began thinking about being bullied again. Robin described the experience as “It’s really hard to get out of the house and go to work when I’m probably going to get yelled at first thing in the morning. I hate that. I hate that.” Also, the participants hoped the bully would not be at work when they arrived. Most participants stated they preferred to stay home but realized this was not a viable option. Ruminating about the bullying that could begin when they arrived at work made the participants nervous and they felt sick. Anna shared “If the person who bullies me is around me, I would not want to go to work. I don’t feel like I want to go to work. I feel sick. I feel like I cannot face the day.”
Being Present for the Patient
All the participants reported a more stressful day at work when the bully was present. Despite the bully being on the unit, the participants tried to be present for the patient. For example, despite recognizing it was “a much more stressful environment” when the bully was present, Sheila was adamant that she remained “there for the patient.” While working, all the participants tried to manage the bully by standing up for themselves with self-encouragement. They wanted to provide good patient care while struggling to make it through the shift. For example, Natalie described learning “to develop a thick skin.. . .I go in, I put on a smile, and I just do what I need to do.”
Some participants explained how they focused on the patient’s needs when dealing with the bully. The participants often felt their work was not valued until they began delivering care to their patients. Anna stated, “I think being bullied has made me feel like you’re not contributing, you’re not valued [sic], you’re not respected, and really, you’re not wanted.” As the participants were delivering patient care, they ruminated about the bully. They all reported working hard to maintain their composure for the benefit of their patients.
Many participants engaged in “mental encouragement” to stay motivated and focused on providing good patient care. Wanda described her situation as “Inside work, I’m pretty much, no this isn’t gonna happen, we’re not going to do this. I know what you are doing so stop playing games.” In the end, all the participants described how they focused their attention on the patient in the foreground while trying to manage the bullying in the background. For example, Shiela stated “It’s just ultimately remembering that we’re there for the patient. That’s what it comes down to.”
Love Being a Nurse
All the participants stayed in their current positions because they loved being a nurse. Some nurses also reported they needed their position for financial reasons, and some feared being unable to find another position if they left. However, they were enthusiastic about being a nurse, and they loved their role in caring for patients. All the participants share Shiela’s sentiment, “I love my job. I absolutely could not dream of doing anything else [other than working as a nurse].” Most participants were adamant that they would not be bullied out of their job or from their profession. Anna stated she would not leave the profession “because I love what I do . . . and I wouldn’t have someone just bully me out of my position.”
Some participants believed the bullies would leave the workplace before they did because the bully did not have the same love for the profession.
[Nursing] it was kind of like a dream job. Knowing what I know about people who are bullying and rude in my workplace, I know they’re going to be out of there faster than I would because I really love what I do. (Gabriella)
Similarly, Janet was not working in a hospital setting and enjoyed teaching at the university. She loved working with students and mentoring them as they developed as young nurses.
I love working with my [nursing] students. I have lots to offer to each of them. I love to continue being in contact with them after they graduate and become part of the workforce. It gives me great pride when they still call me. (Janet)
Although some participants admitted they wanted to leave nursing when the bullying made work difficult to endure, they were unable to let go of their love for the profession.
I always tell my husband, I’ve been saying it a lot lately, that I think I need to get out of nursing. But I just I can’t let it go. I love nursing, and I’ve been in it forever. There’s really nothing else I want to do . . . even with all the bullying. (Wanda).
Theme 2: Not Good for Patient Care
Across the interviews, all the participants described the negative impact of bullying on patient care. Although participants responded to the bullying with intentional strategies to provide good patient care while trying to appear “normal,” they always worried about the possible impact of the bullying on patient care.
Most days, just trying to be a duck that looks calm and paddling like hell underneath because I’m spending 90% of my day paddling underneath, making sure that I’m walking a fine line of taking care of everybody and getting everybody’s needs in order. (Vanessa)
Because of the emotional consequences from bullying, some nurses noted their relationship with the patient was altered, such as being more abrupt and less patient. For example, Robin recognized the bullying as “an ordeal that made me less patient with my patients and that’s not okay.”
Constantly Feeling Nervous
The bullying experience resulted in all the participants describing a continual state of nervousness about the perceived quality of their work. When the bully was at work, Shiela recalled “I needed to be on my toes, but to be fearful and wary, I guess to an extreme, is not always good.” Some participants were also concerned about not feeling as confident in their work. The participants believed they performed better when the bully was not at work because they “make you nervous, and it makes you question yourself” (Anna).
Losing Confidence
The participants reflected that the bullying made them constantly confront their self-confidence. They were often worried about their diminished self-confidence being noticed by the patient. As such, the participants always tried to exhibit confidence to maintain a good relationship with their patients.
When you’re not confident in something, it can definitely have an effect on patient care because patients pick up on that kind of stuff, especially with new nurses. See, I’ve had patients tell me, “I could tell this nurse was a little hesitant,” when they were doing something. (Kimberly)
Secondary to concerns about the patient relationship, many participants were worried about the bully eroding the confidence of colleagues regarding their ability to care for patients.
And people just don’t have confidence in you or value your opinion or contributions. And when you feel that way and going into the workplace where that person is around, it makes you feel all those things. (Anna)
Paranoia Results in Hypervigilance
When the bully was at work, all the participants felt paranoid as they feared interactions with the bully. They were anxious about the bully sabotaging their patient care. The participants felt stressed under the bully’s watchful eye as they were convinced, they were being scrutinized. Gabriela described this as walking into work “and as soon as I see them [bully], I’m like oh, it’s going to be a great night [sarcasm]. I can just tell. It’s definitely not a good feeling.” Most participants reported paranoia when the bully invasively monitored their work. At some point, many participants noted their work was slower because they were constantly checking to make sure the bully would not find any errors. When the bully was the charge nurse for the day, Anna noted, “If you do encounter a challenge during the day, you have to call that person as a resource. Then, you’re nervous because you’re worried about being attacked.”
Being careful was described by the participants as an automatic response to preventing the bully from having a reason to bring a complaint against them or to instigate a negative performance evaluation.
Janet worried about making mistakes, explaining that the bully is “going to be angry with you. That he’s going to report you.” Others like Patty worried about being evaluated by the bully commenting, “I kind of dread it, to be honest.” Many participants were concerned about the bully conspiring with colleagues to watch them, describing how the bully recruited colleagues to monitor them, especially when the bully was not working.
I was not trusting of the people around me. I was very, very leery of my coworkers because I didn’t know who was going to her or who was watching. Because she does have people, [I wasn’t] sure who I could trust. (Brandy)
Learning to work more efficiently and effectively to deal with the bullying resulted in most participants describing a state of hypervigilance. All the participants reported trying to be extra careful to avoid mistakes. Vanessa noted that she can’t “make any mistakes whatsoever. [I need to manage] the challenge of hypervigilance and the challenge of just making sure that I’m doing everything up to par.”
Becoming the Problem
A universal concern of the participants was becoming labeled as “the problem” if the bullying remained in the background. All participants continually worried about the next episode of bullying. Because of their experiences with bullying, they began to understand the bully could use some situations to turn them into a problem. Anna explained she was worried about the bully “undermining” her as a “valued employee.” Most participants reported the bullies were clinical experts or managers with many years of experience. Some participants described how the bullies used this profile to turn the bullying, inappropriate workplace behaviors, and confrontational interactions into clinical practice or professional competency problems. Janet explained “She [the bully] told me, ‘I’ve been doing this[nursing] for a long time without a problem. So, if you have a problem with my practice as a critical-care nurse, that’s your problem, not mine.” As a result, all the participants were worried about being terminated from employment or transferred to another area of the organization because of the bullying. Natalie believed the bully “is going to turn me in for something to either try to get me fired or moved from the unit.”
Several participants believed they would have problems seeking employment at another organization. A couple of the participants ruminated about their fear of external retribution. When the bully was a manager, the participants felt trapped in their job.
A lot of nursing is word of mouth. If you stand up to a bully, especially if it’s a boss, they tend to tell others, and then finding another job can become very challenging.. . . They [the bully] dub you as a problem, and it can become very difficult.. . . You can be stuck in your job even if you don’t want to be surrounded by bullying. (Wanda)
Theme 3: Learning to Live With Bullying
Almost all the participants described learning to live with the bully. They used different strategies to limit confrontations. Patty worked weekends, noting “I’d kind of hoped I didn’t run into her [the bully].” Several other participants reported the bullying became so severe at times that colleagues began helping them avoid the bully.
His behavior toward me got to the extent that when the other nurses on the unit saw him coming, they would come and tell me, ‘John’s coming. John’s coming.’ And I would go hide. I would hide in the patient’s bathroom, or I would hide behind the curtains or hide in the hopper room. I would hide anywhere, so that John wouldn’t see me, so that he wouldn’t look so angry at me. So, he wouldn’t speak to me in such a hateful way, I would just hide from him. (Kimberly)
Dealing With Bullying at Work
Some participants recounted using assertive communication to set boundaries with the bully during moments when they could confidently stand up for themselves. For example, Shiela described maintaining her composure and strength during a shift change by firmly stating “If you want to manage the patient and keep her, then I will give you [the bully] report and you can stay here at bedside.” The participants also confronted the bully in front of other colleagues by demanding respectful behavior and professional conduct. Robin addressed the bully by saying “Being spoken to in a harsh tone of voice, there is no excuse for that. Talk to me like I’m an adult. Don’t talk to me like I am eight, and I forgot my homework.” Most participants reported finding safe spaces as the most important strategy to briefly escape the bully. The safe spaces were important to detoxify situations and to cleanse their mind of the bullying. Michelle explained, “A lot of times [at work], we have a courtyard where we take the patients.. . .Going outside in that fresh air, I can take deep breaths and it’s like cleansing.”
Several participants described the safe places as essential for dealing with emotional consequences of bullying, such as anger, frustration, and pain. In addition to being the places to regain composure, the participants emphasized the importance of not gratifying the bully by displaying their lack of composure.
If I feel on the inside like I can’t keep it together, then I’ll go to the bathroom or whatever and I won’t scream out loud, but I’ll make the motion. You know, in the bathroom like I’m screaming or jumping up and down. [If] I feel like I need to cry a few minutes, I’ll cry and get myself together. Then I’ll go back and go to work. I never try to let, as that commercial used to say, never let them see you sweat! (Michelle)
None of the participants spoke about bullies following them to their safe place. Bullying was described as local confrontations, episodes, or incidents rather than continual assaults across the workplace.
Leaving the Bullying at Work
All the participants noted a continual effort to leave the bullying at work, keeping it away from home. In this regard, Vanessa noted “Me at home is not the same as the me at work.” Most participants described how they purposely transitioned from work to home. Some participants explained how they needed to compose themselves before going into their homes. In the case of Michelle, she shared that “I’ll desensitize myself by sitting in my car before I come home so I don’t bring my work stress home.” Other participants spoke about ways of venting anger or engaging in physical activities to relieve stress at home. The goal was to release bullying thoughts from their mind and body. For example, Wanda shared “When I go home, I’ll vent like crazy, and when I’m done, I’ll go ziplining.”
Resilience Emerges From Coping
All the participants spoke about different ways of coping with bullying. Many participants explained their religion and commitment to caring for people helped them learn to cope with the bully.
Christian faith was number one. Number two, my oath that I took the day that I stood before my family members and along with my classmates when I graduated as a nurse to do the best that I could do and do no harm to my patients and respect them and provide for them at all times no matter what. (Michelle)
Other participants spoke about their professionalism and ethical duty as key reasons for learning how to cope with bullying. For example, Janet shared “I have a strong sense of professionalism and ethics and community, and I think more than anything, I wanted to make sure that I fulfilled the duty that they expected of me.” The participants discussed how coping resulted in resilience to the bullying over time with experience. Most participants described an inner strength that emerged to minimize the impact of bullying and reduce the threat of bullying to their professional wellbeing.
It’s so challenging emotionally and physically that you develop some kind of strength inside you to deal with the challenging things. And also, other things that doesn’t [sic] seem life threatening seem to kind of be easier to cope with. . .. You develop a sense of strength, and that helps you to be more resilient, I think. And it makes you stronger. (Anna)
Over time, many participants noted a stronger sense of self and a rejuvenated passion for nursing despite the ongoing bullying. They saw the bully as trying to take away their passion for caring and their joy of nursing. Brandy commented that “I have a great amount of strength, and I love my job with passion, and I would never let her take that from me because I have a lot to give to those patients.” With the experience from working through the bullying, all the participants spoke about becoming resilient to the bullying. They learned how to cope with bullying as a daily problem in the bigger picture of life. Shiela described the coping as “It’s like anything else in life. I make a conscious choice every day to get up and go to work. It’s a matter of pushing through. . . and looking at the bigger picture.”
In the end, the bullying experience was incorporated into the participant role as caregiver for patients on the nursing unit or students in the classroom. However, each participant’s self-care for their well-being was noticeably missing from all descriptions.
I just try to do the best that I know to make sure that this ward is a proficient and competent ward. Make sure that our patients are receiving the best possible care, and they are reaching their goals and they are being discharged from the hospital back into [the] community and able to function on the outside. (Michelle)
Theme 4: Changing the Culture
The participants described ways to reduce bullying in the workplace, particularly for future nurses. While they learned how to cope with bullying as part of their daily work, they also expressed frustration with the persistent nature of the problem. Like Anna, all the participants recognized “Bullying is something that’s very common in nursing” and not fully addressed by organizational interventions or prevented by professional norms. However, the situation was not viewed as hopeless. Most participants described strategies to cultivate more supportive work environments.
Organizational Culture
Participants believed inexperienced nurses need to be better prepared to manage interpersonal conflict when they initially enter the workplace. The orientation process should develop their confidence and facilitate new relationships through mentoring.
I know it’s definitely hard when you’re so new, and you’re new to policies and procedures, but kind of finding a mentor, whether it be someone they’re orienting with or another friend on the unit, just to kind of re-affirm their abilities. That kind of stuff. (Kimberly)
Also, participants stated experienced nurses need to be more supportive and less critical of inexperienced nurses and more collegial with other nurses in their unit.
We just need to try to educate our nurses, our older nurses, that when those new nurses come out don’t say, ‘Okay, I’m going to see what they’re made of.’ We need to take them, and we need to, like a mother bird would do with her baby, put that nurse under our wings and care for them and lead and guide them and help them grow. (Michelle)
Finally, some participants provided similar advice about addressing bullying in the workplace by being strong and reporting the bullying.
I would tell [nurses being bullied] to stand up for themselves. Obviously, you should be professional. . . don’t be scared. . . move up the chain. If your manager is kind of bullying you or not helping your career. . . you can talk to a director. You can talk to somebody further up. Because you’re probably not the only one [being bullied].” (Patty)
Professional Culture
Recognizing that many nurses without bullying experience view bullying as “isolated situations” or “not getting along” rather than systemic violence in the workplace, the nurses were adamant that bullying was a widespread problem in nursing that needed to be addressed, as illustrated in this quote: “I feel that nurses need to be better about protecting each other and standing up for each other and not throwing each other under the bus” (Anna). For this reason, participants noted change needs to begin in nursing school and extend into the workplace. They emphasized leadership, professionalism, human caring, collegiality, and mutual respect to were essential to change the nursing culture. Wanda stated “The whole culture of nursing needs to change. . . to stop bullying . . .. [so] that your coworkers are not your enemy.”
Discussion
To the best of our knowledge, this was one of the first studies to describe the lived experiences of nurses actively being bullied in the workplace. The nurses in this study were living the experience of bullying at the time of the interviews. As such, bullying as a nursing phenomenon was described by a central theme, “The whole culture of nursing needs to change.” Unlike previous research in nursing, this study describes how bullying was visible to colleagues and supervisors, without organizational intervention.
The central theme was constructed from the four major themes of “going to work can be really hard,” “not good for patient care,” “learning to live with bullying,” and “changing the culture.” The nurses in the current study recognized the nursing profession is grounded in caring (Watson, 1979, 1999, 2012) and nurses unconditionally care for people requiring health care (Turkel et al., 2018) while keeping them safe from harm (Tønnessen et al., 2020). Similar to other studies (Arnetz et al., 2019; Vessey et al., 2010), including Magnet recognized hospitals (Bolandian-Bafghi et al., 2022; Hickson, 2013, 2015), bullying in the current study was facilitated by workplace factors that hindered identification and prevented intervention. As such, our results contribute to an important gap in the literature (Goh et al., 2022; Jang et al., 2022; Lever et al., 2019; Liu et al., 2019; Shorey & Wong, 2021) by describing how management inaction resulted in bullied nurses developing their own strategies to deliver good patient care.
Regardless of the context of the work or the conditions of the workplace, nurses recognize their ethical responsibility to provide quality patient care as part of the philosophy of nursing (Danaci & Koç, 2020). As previously reported in the literature (Shorey & Wong, 2021), nurses in the current study had struggled to respond to the bully because there were hidden drivers rather than organizational interventions. The bullies were described by our participating nurses as informal leaders with many years of clinical experience or supervisors with formal positions. This finding is important because management studies report abusive supervision influences paranoid arousal (anxiety and fear) and paranoid cognition (hypervigilance and rumination), resulting in changes in employee behavior (Chan & McAllister, 2014).
The nurses in our study described working through bullying as an “emotional rollercoaster” until they gained enough experience to manage their emotions. The nurses described feeling angry, distracted, frustrated, nervous, stressed, and worried while providing patient care. The negative emotions inflicted by the bully overshadowed the patient-centeredness of their nursing practice (Shorey & Wong, 2021). However, the love of caring (Yoo & Ahn, 2020) and the need to advocate for patients (Houck & Colbert, 2017) helped them develop strategies to minimize the pain and lessen the emotional burden. Similar to previous studies, the nurses in our study responded to the bullying through avoidance (Karatuna et al., 2020), ignoring (Hampton et al., 2019), silence (MacMahon et al., 2018), and emotion suppression (Berry et al., 2016). In addition, several participants reported confronting the bully either during shift change to show strength before the bully left the workplace or in front of colleagues when the bully used patronizing language or made critical remarks (Autrey et al., 2013; Berry et al., 2016; Hampton et al., 2019). However, these strategies were reported to be largely ineffective in addressing the problem. When bullying situations became too difficult to manage, the nurses in our study reported retreating to a “safe place” removed from the patient care area to emotionally decompress and professionally recompose themselves. The identification of a “safe place,” where nurses could temporarily remove themselves from the bullying, has not been previously reported in the literature, but researchers have recommended organizations develop “no bullying zones” (Edmonson & Allard, 2013).
Throughout the current study, the nurses described how being bullied made them feel inadequate and alienated. As reported by other researchers, (Berry et al., 2016; Karatuna, 2015), the nurses in our study lost self-confidence and felt increasingly anxious at work. In response, they became hypervigilant, a strategy to protect their decision-making and to limit criticisms from impacting their performance. In response to the bullying, the nurses in our study also described working harder (Johnson, 2019) rather than disengaging from work (Pickering et al., 2017). However, they worked harder because they were paranoid about what the bully, who was constantly watching them in the workplace, might find to use against them. They ruminated about what mistakes and errors the bully might observe to question their competency or report their work to management, leading to a state of hypervigilance. While hypervigilance may be a protective mechanism, it can contribute to delays in care due to the additional time needed to perform tasks or detract from the quality of care provided to patients (Ham et al., 2022). Additionally, bullying can result in medication errors, a significant enough concern to be recognized during hospital accreditation visits (Wright & Khatri, 2015). Workplace bullying negatively impacts nurse well-being and patient safety.
Despite the bullying, the nurses in our study continued working because of their selfless concern for the well-being of their patients (Ciezar-Andersen & King-Shier, 2021). Although nurses often make personal sacrifices for the benefit of other people (Slettmyr et al., 2023), the nurses in our study realized they were being harmed by the psychological and physical burden of bullying, resulting in anxiety, depression, stress, and insomnia (Yoo & Ahn, 2020). Unlike a previous study (Vessey et al., 2010), the nurses in our study did not seek emotional support from friends and family. Instead, they described self-care strategies of leaving the bullying at work so they could live their personal life. These strategies included decompression time in the car before leaving work or entering their home, venting with close family members for a brief time after arriving home, and engaging in physical activities to alleviate anxiety and reduce stress. Despite participants feeling emotionally drained and physically tired at the end of the workday, they recovered by leaving the bullying at work.
When encountering daily professional challenges and emotional harm in the workplace (Buheji & Buhaid, 2020), resilience is the most important protective factor (Cooper et al., 2020) for nurses to thrive during the crisis (Jo et al., 2021), such as bullying. Nurses described drawing on their experience and inner strength to cope with the bullying. Because of their profound love for nursing (Bolandian-Bafghi et al., 2022), the nurses refused to let the bully take away their profession or drive them from their workplace. This finding contradicts previous studies reporting nurses often transferred to other units or left the organization in response to bullying (Berry et al., 2016; Hampton et al., 2019; Johnson, 2019). Since the nurses in our study were determined to outlast the bully at work, their eventual resilience shifted the emotional pain from bullying to the background and the joy of caring for patients in the workplace to the foreground.
In the current study, the lack of management interventions for bullying suggested anti-bullying policies were not a high priority for the organization (Fox & Cowan, 2015). Even when antibullying policies are present in an organization, reports of bullying are hindered by fear of retribution from managers (Harrington et al., 2015). In the current study, the organizational cultures seemed to tolerate bullying, and managers preferred to avoid recognizing the bully. Similarly, in a cross-cultural scoping review of workplace bullying in nursing, Karatuna et al. (2020) reported that organizational tolerance for bullying was a commonly observed problem in performance-oriented cultures in Anglo countries, such as the United States. For this reason, managers need to understand antibullying policies and be better prepared to fulfill their role in preventing, identifying, and managing bullying (Granstra, 2015).
Policy Implications
The findings of this study highlight critical gaps in workplace support structures, particularly in addressing bullying in hospital work environments. To mitigate the impact of bullying and to promote healthier work environments, policy changes should focus on creating a formal program to educate nurses about the impact of bullying on workplace wellness, to establish a reporting system for bullying situations, and to provide managers with the tools to identify and to respond to bullying behaviors. The introduction of designated “safe spaces” and the reinforcement of a no tolerance for bullying behaviors workplace represent essential steps in this direction, reflecting the urgent need for institutional commitment to nurse well-being and professional sustainability.
Similar to the professional culture in most countries, American nurses are obligated to “create an ethical environment and culture of civility and kindness, treating colleagues, coworkers, employees, students, and others with dignity and respect” (American Nurses Association, 2015, p. 4), and employers are legally required to provide safe and healthy workplaces for their employees (Michaels & Barab, 2020). In this regard, nurses can report bullying situations to the Occupational Safety and Health Administration under the General Duty Clause, section 5(a)(1), that requires employers to provide a workplace free from conditions that cause, or are likely to cause, death or serious physical harm to employees.
When considering government regulations, professional ethics, licensing requirements, and accreditation standards, organizations employing nurses must begin fulfilling their obligation to provide a safe workplace that is free from bullying. Since bullying is unethical professional conduct, possibly involving illegal acts, nurses should be encouraged to report bullying to their organization ethics hotline, if it is not properly addressed by management. In addition, licensing boards for nursing need to make nurses aware of the process to report nurse bullies because these boards have the power to investigate and adjudicate cases of workplace bullying. Finally, accreditation agencies should develop an external process for nurses to report bullying cases not addressed by management so that the workplace can be identified as unsafe.
Accreditation entities for healthcare organizations and universities with schools of nursing must develop evidence-based standards with robust assessment criteria aimed at preventing workplace bullying. Despite an early accreditation alert detailing the behaviors that undermine a culture of safety in hospitals (The Joint Commission, 2008) and the substantial body of evidence reporting the negative impact of bullying on nurses and the patient care they provide (Goh et al., 2022; Jang et al., 2022; Johnson, 2009; Karatuna et al., 2020; Lever et al., 2019; Liu et al., 2019; Martin & Zadinsky, 2022; Rittenmeyer et al., 2013; Shorey & Wong, 2021), a decade was required for an alert that focused on physical and verbal abuse, including bullying (The Joint Commission, 2018). After this alert, The Joint Commission (2021) published new violence prevention standards specific to environment of care, human resources, and leadership. Effective at the beginning of 2022, the four standards include five performance elements requiring worksite analysis, data collection and continuous monitoring, identification of risks, hospital staff education and training, and workplace violence prevention programs (Arnetz, 2022). Although the standards are too broadly focused on workplace violence rather than specifically addressing the bullying epidemic, leaders should finally be compelled to formally recognize workplace violence in their organizations.
Accreditation standards for schools of nursing (Commission on Collegiate Nursing Education, 2018) seem to be silent about addressing workplace violence, including bullying by administrators, faculty, and students. However, the core competencies guiding curriculum development for professional nursing education (American Association of Colleges of Nursing, 2021) briefly recognize three sub-competencies related to violence in domain 5 (quality and safety), including preventing workplace violence and injury (entry-level), promoting policies to prevent violence and mitigate risk (entry-level), and fostering a just culture reflecting civility and respect (advanced-level). Two additional subcompetencies related to culture in domain 9 (professionalism) include adhering to a culture of civility (entry-level) and fostering strategies that promote a culture of civility across settings (advanced level). Importantly, accreditation entities are critical intermediaries with schools of nursing to advance evidence-based standards for developing organizational cultures and guiding professional conduct to prevent bullying.
Future Research
Bullying has not been reduced despite extensive research and multiple systematic reviews of the evidence (Goh et al., 2022; Jang et al., 2022; Lever et al., 2019; Liu et al., 2019; Rittenmeyer et al., 2013; Shorey & Wong, 2021). There are few intervention studies (Jang et al., 2022; Rutherford et al., 2019), and many studies only report incidence, prevalence, and risk factors. Furthermore, too much research seems to be focused on bullying at the individual level, such as nurses and managers, without robust assessments of the culture and management at the organization level (Castronovo et al., 2016; Goh et al., 2022; Hartin et al., 2020; Rittenmeyer et al., 2013; Vessey et al., 2010). Future research may be needed to understand experienced, witnessed, and instigated bullying, as previously reported in the organizational behavior literature (Schilpzand et al., 2016). Although the nurse’s experience of bullying is well described in the observational research literature, the literature is almost silent about witnessed bullying by colleagues and managers. The nurses in the current study identified the organization as a bystander who supported the bullying because of management inaction. There does seem to be limited research focused on understanding, from the perspective of bullied nurses and their bullies, what instigates workplace bullying and how to stop the bullying. The organizational behavior, development, and theory literatures may provide useful knowledge to advance research with new perspectives to inform interventions with novel strategies.
Limitations and Strengths
There are at least five limitations to disclose for the current study. First, although the sampling evolved to focus on identifying male participants, the study had only female participants. Second, the sampling strategy targeted early career nurses, but few were recruited for the study. These sampling limitations mean our findings may not be transferable to men or early career nurses. However, this is also a strength due to the homogeneity of the sample. In this regard, previous researchers reported the experience of women being bullied differs from men (Emdad et al., 2013; Rosander et al., 2020). Third, response bias can contribute to participants being more likely to recall or emphasize certain aspects of their bullying experiences. As the participants were actively being bullied at the time of their interviews, they might recall the most recent experiences rather than the general experience. Fourth, the experiences of the participants in this study aligned with the structural description resulting from Giorgi’s (2006, 2009) approach to phenomenology. However, the structural description resulting from this approach may not resonate for other people at different times, with other contexts, or across spaces (Leigh-Osroosh, 2021). Finally, there was less workplace variation than intended, with more participants working in a clinical practice setting than educational. However, the participant characteristics varied by academic preparation, workplace location, type of setting, and professional role. Across all participants, data from the single educational workplace was consistent with the other settings.
Conclusions
While most nursing workplace bullying research has focused on cross-sectional survey designs, the current study is one of a few studies to report the phenomenon of nurses being actively bullied in the workplace. The bullying was not acknowledged by managers, and colleagues avoided involvement in bullying situations. The lack of management intervention is an area requiring focused research. Despite unresolved bullying in the workplace, nurses continue going to work because they love nursing and caring for patients. Some participants decided to stay at work and endure the bullying as they were concerned about finding another job. As the nurses gained experience coping with bullying, they began enjoying nursing because they were more resilient. Developing resilience to workplace bullying is another area requiring research to understand the process and to propose effective strategies.
To address bullying in the workplace, leaders must assess their organization for bullying, provide processes for nurses to report bullying, and teach managers how to intervene when bullying is identified. Since early career nurses need better preparation to confront bullying, nursing education programs should implement curricular strategies to encourage teamwork, develop healthy relationships, cultivate mutual respect, and facilitate effective communication. Researchers need to recommend evidence-based strategies and to evaluate programs for effectiveness in preventing workplace bullying. Finally, accreditation organizations should develop robust standards focused on preventing workplace bullying in healthcare organizations and universities with schools of nursing.
Supplemental Material
sj-docx-1-gqn-10.1177_23333936251319783 – Supplemental material for “The Whole Culture of Nursing Needs to Change”: A Descriptive Phenomenology of Nurses Being Bullied
Supplemental material, sj-docx-1-gqn-10.1177_23333936251319783 for “The Whole Culture of Nursing Needs to Change”: A Descriptive Phenomenology of Nurses Being Bullied by Dawn R. White, Patrick A. Palmieri, Sara R. Huaman-Morillo, Timothy A. White and Eric W. Hickey in Global Qualitative Nursing Research
Footnotes
Acknowledgements
The authors acknowledge Deborah Goggin, scientific writer from the Department of Research Support at A.T. Still University, for her comprehensive editorial review of this manuscript. We also appreciate the continued technical support provided by Dr. Neringa Kalpokas and the Atlas.ti team.
Author Contributions
Conceptualization, D.R.W.; methodology, D.R.W. and E.W.H.; validation, P.A.P. and E.W.H.; formal analysis, D.R.W., P.A.P., S.R.H.M., and T.A.W.; investigation, D.R.W.; resources, D.R.W. and E.W.H.; data curation, D.R.W.; writing—original draft preparation, D.R.W., P.A.P.; writing—review and editing, D.R.W., E.W.H., P.A.P., S.R.H.M., and T.A.W.; supervision, E.W.H.; project administration, D.R.W.; funding acquisition, P.A.P. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
Data are contained within the article. Since our qualitative data resulted from confidential participant interviews, the complete transcripts of each interview cannot be released without the written consent of each participant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board at Walden University (protocol no. 8-29-17-0418151).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study. The data published in this study is deidentified.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.