
Abstract
Underutilization of sexual and reproductive health services among young people is associated with many adverse sexual and reproductive health-related outcomes and morbidity. Guided by the socioecological model, this study undertook a qualitative exploration of the barriers limiting young peoples’ uptake of sexual and reproductive health services in Osun State, Nigeria. Fifty-eight young people (aged 15–24 years) from two universities and one community in Osun State were selected and involved in six focus group discussions. A thematic analysis was performed using NVivo software version 12. Intrapersonal, interpersonal, institutional, and community-level barriers were identified from the focus group discussions, aligning with the socioecological model framework. The study identified various interwoven barriers to the utilization of sexual and reproductive health information and services. The interrelatedness of the factors at different levels underscores the need to design and implement multifaceted policies and interventions aimed at improving young people’s access to and utilization of sexual and reproductive health services.
Keywords
Introduction
Young people experience several psychological, physiological, and social changes that may expose them to risky sexual practices including early sexual debut, unsafe sex, and multiple sexual partners among others, which can eventually lead to sexual and reproductive health (SRH) problems (Ninsiima et al., 2021). High morbidity and mortality rates among young people are mostly a result of SRH problems (Thongmixay et al., 2019). Previous studies have shown that young people are faced with SRH challenges such as unintended pregnancies, unsafe abortions, and sexually transmitted infections, due to underutilization of SRH services (Ninsiima et al., 2021; Nmadu et al., 2020; Utaka et al., 2023).
Sexual and reproductive health services are crucial for mitigating SRH issues and promoting healthy outcomes among young people. This aligns with the objective of Sustainable Development Goal three (Odo et al., 2021). However, in Nigeria, it has been documented that there is under-utilization of SRH services among young people (Odo et al., 2018). The major barriers to accessing and utilizing SRH services among youth include lack of knowledge and awareness of SRH services, shame/stigma as a result of cultural unacceptability of the use of SRH by young people, poor attitude of healthcare providers and lack of privacy and confidentiality (Braeken & Rondinelli, 2012). Underutilization of SRH services is associated with numerous adverse outcomes, including unintended pregnancies, unsafe abortion complications, sexually transmitted infections and gender-based violence (Odo et al., 2021).
Sexual and reproductive health services involve various components which include family planning information and services, safe motherhood and child survival, prevention and management of complications of abortion, provision of safe abortion services where the law permits, and prevention and management of STIs, including Human Immunodeficiency Virus (HIV)/Acquired Immunodeficiency Syndrome (AIDS) (Utaka et al., 2023). Universal access to SRH services is central to attaining the 2030 Sustainable Development Goals (SDGs) relating to good health, well-being, and gender equality. To empower young people to make informed choices about their sexual health, comprehensive SRH services must be accessible, affordable, and tailored to their unique needs (Zepro et al., 2023).
Young people are vulnerable to SRH problems due to increased unhealthy sexual behavior among them (Odo et al., 2021). The persistent high prevalence of these problems may suggest that current policies and programs are limited in promoting access to SRH services among this age group. As time evolves, so do the barriers to SRH service utilization. Given the widespread use of technology among young people, mHealth interventions have the potential to play a significant role in promoting SRH issues.
This study is a part of the sexual health literacy (SHELTER) project (described in the method section) which seeks to design a mobile health intervention to improve the utilization of SRH services among young people. Developing and implementing effective interventions to enhance SRH utilization among young people necessitates a comprehensive grasp of the complex barriers they encounter. This requires continuous exploration of their opinions, perceptions, and experiences in this regard (Tilahun et al., 2021). Hence, this study aimed to explore the challenges and barriers encountered by young people in accessing SRH information and services in Osun State, Nigeria.
Conceptual Framework
The Socioecological Model (SEM) was adopted as the conceptual framework underpinning this study (McLeroy et al., 1988). The SEM framework demonstrates that diverse factors and barriers affect health behaviors at various interconnected domains, including the communal, institutional, interpersonal, and intrapersonal levels (Sidamo et al., 2023). By integrating these diverse influences, SEM provides a comprehensive understanding of the complex interplay between various determinants of behavior. This multi-level approach allows researchers to capture insights into how different factors interact and contribute to overall behavioral outcomes (McLeroy et al., 1988, Sidamo et al., 2023).
The SEM has been previously utilized in the identification of barriers to the utilization of SRH services (Ezenwaka et al., 2020, Sidamo et al., 2023). At the core of the SEM is the individual, whose actions are impacted not only by personal knowledge, beliefs, and attitudes but also by concentric layers of multiple external variables (Ezenwaka et al., 2020; McLeroy et al., 1988). The second layer of the framework is the interpersonal level which describes individuals’ familial and social networks that may influence health-seeking behavior and utilization of healthcare resources (Sidamo et al., 2023).
The institutional level of the SEM describes the factors related to healthcare facilities and workers and the role they play in influencing the determinants of health. The community-level variables represent the physical environment and the societal norms and customs that govern individual beliefs and behavior, while the outermost layer of the framework indicates the various local and national policies and guidelines. This study applied the SEM to qualitatively explore the perspectives and experiences of young adults regarding the barriers hindering their access to and utilization of SRH services.
While the socio-ecological model offers a comprehensive framework for understanding health behaviors, it is not without its limitations (Partelow, 2018; Schölmerich & Kawachi, 2016). One significant drawback is its complexity. The model's multi-level approach can be challenging to apply. Similarly, interventions that address multiple levels require a lot of resources and substantial coordination and collaboration among various stakeholders. Achieving this in practice can be difficult, particularly in settings with limited resources (Fleury & Lee, 2006; Schölmerich & Kawachi, 2016).
Furthermore, there is the potential for overlooking relevant factors. Although the SEM encourages a comprehensive approach, there is always a risk that some determinants may be missed, especially if they do not fit neatly into one of the model’s predefined levels. This can result in an incomplete understanding of the factors influencing health behaviors (Partelow, 2018). However, despite these potential constraints, the socio-ecological model provides a valuable framework for considering the multiple influences on health determinants.
Methods
Study Design, Setting & Selection of Participants
A descriptive qualitative design was adopted in this study to explore the challenges and barriers faced by young people in accessing and utilizing SRH services in Osun State, Southwest Nigeria. Qualitative description design, also known as descriptive qualitative design, is appropriate in situations when time and resources are limited and personal information from individuals experiencing the phenomenon being studied is needed (Bradshaw et al., 2017). It is used in this study to investigate the barriers associated with the utilization of SRH services among young people in Osun State, Nigeria.
The presentation of this study report was guided by the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Tong et al., 2007). This study is the qualitative arm of the SHELTER project conducted in Osun State, Southwestern Nigeria. The SHELTER project was designed to bridge the significant gap in SRH care services, characterized by low SRH literacy and limited access to essential information and services. Using the design thinking approach, the project was carefully designed to provide effective solutions that address the specific challenges and requirements of young people seeking SRH care. The study comprised three distinct phases: inspiration, ideation, and implementation. The initial inspiration phase aimed to gain a deep understanding of the needs and challenges faced by young people in utilizing SRH services, through mixed-methods approach. The subsequent ideation phase focused on prioritizing and developing ideas for content and design of the SHELTER application, leveraging the insights gathered in phase one and expert-prepared SRH modules to inform the development of the application. Finally, the implementation phase involved pilot-testing the mHealth application among participants from Osun State University to assess its effectiveness.
The SHELTER project was conducted among in-school and out-of-school young people (aged 15–24 years) selected through a multistage cluster sampling technique. Osun State was selected randomly out of the six states in Southwestern Nigeria. Osun State is located in Southwestern Nigeria with Osogbo as its capital. The State is divided into three senatorial districts and thirty Local Government Areas. Osun State has twelve universities (four public and eight private) out of which one public (Osun State University, Osogbo) and one private (Redeemer’s University, Ede) were selected. There are nine major towns in the state (Osogbo, Iwo, Ikirun, Ila-Orangun, Ile-Ife, Ikire, Ilesa, Ejigbo, and Ede) (Osun State, 2023) out of which Ilesa was randomly selected for the study. The authors recruited participants for the focus group discussions using purposive sampling. In-school young people between the ages of 15 & 24 years and willing to provide consent to participate were drawn from the two selected universities. Also, in the community, out-of-school young people were selected using the same criteria. The out-of-school participants were residents of the selected community who had not completed tertiary education and were not students of any formal educational institution at the time of the study.
Ethical Consideration
Ethical approval to conduct the study was obtained from the Health Research Ethic Committee of the author’s institution. Approval to conduct the study was obtained from the directorate of research and innovation management of the University where the study was conducted and the Chairman of Local Government in the community. The participants received detailed information about the study, after which they gave informed consent to participate. They were assured of confidentiality and that their data would only be used for research purposes. Participants were reminded to maintain confidentiality and respect the privacy of their peers by keeping the conversations and shared information within the group, thereby ensuring a safe and trustworthy environment for open dialogue.
Data Collection
A total of six focus group discussions (FGDs) were conducted among the young people, two in each of the three study sites. In each site, there was one FGD among males and females respectively. Each group had between 8 to 11 participants with a total of 58, two of those invited for the FGD in one setting could not participate due to logistic reasons. The breakdown of the FGD groups and total number of participants by sites of data collection are as follows: Osun State University (Groups 1 and 2; n = 17), Redeemer’s University (Groups 3 and 4; n = 21), and Ilesa community (Groups 5 and 6; n = 20).
The FGDs explored participants’ perceptions and experiences about individual, interpersonal, institutional, societal, and other barriers hindering access to and use of SRH information and services. The FGD guide was developed after a detailed review of relevant literature. Although the discussion guide was prepared in both English and Yoruba languages, all participants were able to speak English language, hence, the focus group discussions were conducted in English language.
Two questions that were focused on in this article are highlighted below;
(i). What challenges do young people have in accessing SRH information and services?
(ii). What are the barriers to using SRH Services among young people?
The focus group sessions were conducted separately for males and females, to foster open and honest discussions. The questions were designed to explore barriers to the utilization of SRH services without compulsorily asking for personal stories or experiences, they were encouraged to share other people’s stories that they are aware of and this enabled participants to provide insightful and thoughtful responses while maintaining their privacy and comfort level. The FGDs were conducted by the authors, who have been trained and are experienced in conducting qualitative research. Field notes were taken during the data collection by three research assistants who were also trained and given adequate information about the specific objectives and the protocol of the study. Each FGD lasted between 60 and 90 minutes and was audio-recorded with the consent of the participants. The FGDs were conducted between October and December 2022.
Data Analysis
The audio recordings from the FGDs were transcribed verbatim and imported into NVivo 12 for coding and analysis. The data was deductively analyzed using the SEM as the theoretical framework. There are two main approaches to thematic analysis: an inductive (bottom-up) approach and a theoretical, or deductive (top-down) approach. Inductive thematic analysis generates themes and codes data spontaneously, without attempting to fit it into a pre-existing framework. In contrast, a deductive analysis is guided by the researcher's theoretical or analytical focus, data is examined, and themes are identified using a pre-established theoretical framework (Braun & Clarke, 2006). In this study, the SEM was adopted as the framework for the deductive analysis of the data.
At various stages of analysis, the transcribed texts were revisited and reviewed to ensure that the inductively derived codes and themes accurately represented participants’ perspectives. The report was structured according to the SEM framework, encompassing intrapersonal, interpersonal, institutional, and community levels. Relevant participant quotes illustrated key themes, and no additional themes emerged beyond the SEM framework.
Qualitative Rigor
A rigorous effort was made to ensure the trustworthiness of the qualitative process employed in this study. Participants were asked to provide objective responses supported by specific examples. Probing questions were also asked to ensure clarity of the information provided by the participant. Data saturation was ensured by giving sufficient time for discussion.
To ensure dependability and confirmability, an inquiry audit was conducted, where researchers reviewed the research process and data analysis to verify the consistency and reliability of the findings. The research methodology was extensively documented. The professional transcription yielded high-quality text data, subsequently reviewed and validated by two expert qualitative researchers.
Throughout the research process, a reflexive journal was kept to take notes and record useful and pertinent information, which helped to ensure the degree of objectivity in the findings. Additionally, the researchers continually examined their prejudices, beliefs, and personal preferences to distinguish them from the information that the participants supplied. These procedures were utilized to establish credibility and trustworthiness, along with those previously discussed under data analysis.
Results
Sociodemographic Characteristics
Fifty-eight participants (28 females and 30 males) took part in this study, aged between 15 and 24 years. All the participants were single and had at least a secondary level of education. The majority (n = 50, 86.2%) were Christians. Each participant was identified with a code number as G1 = group 1, P1 = participant 1, hence G1/P1 means group 1 participant 1, G6/P2 means group 6 participant 2, and so on.
Following the SEM framework, themes from the discussions were grouped into four broad categories as follows; intrapersonal/individual, interpersonal, institutional, and community factors. The factors are however interrelated (Figure 1).
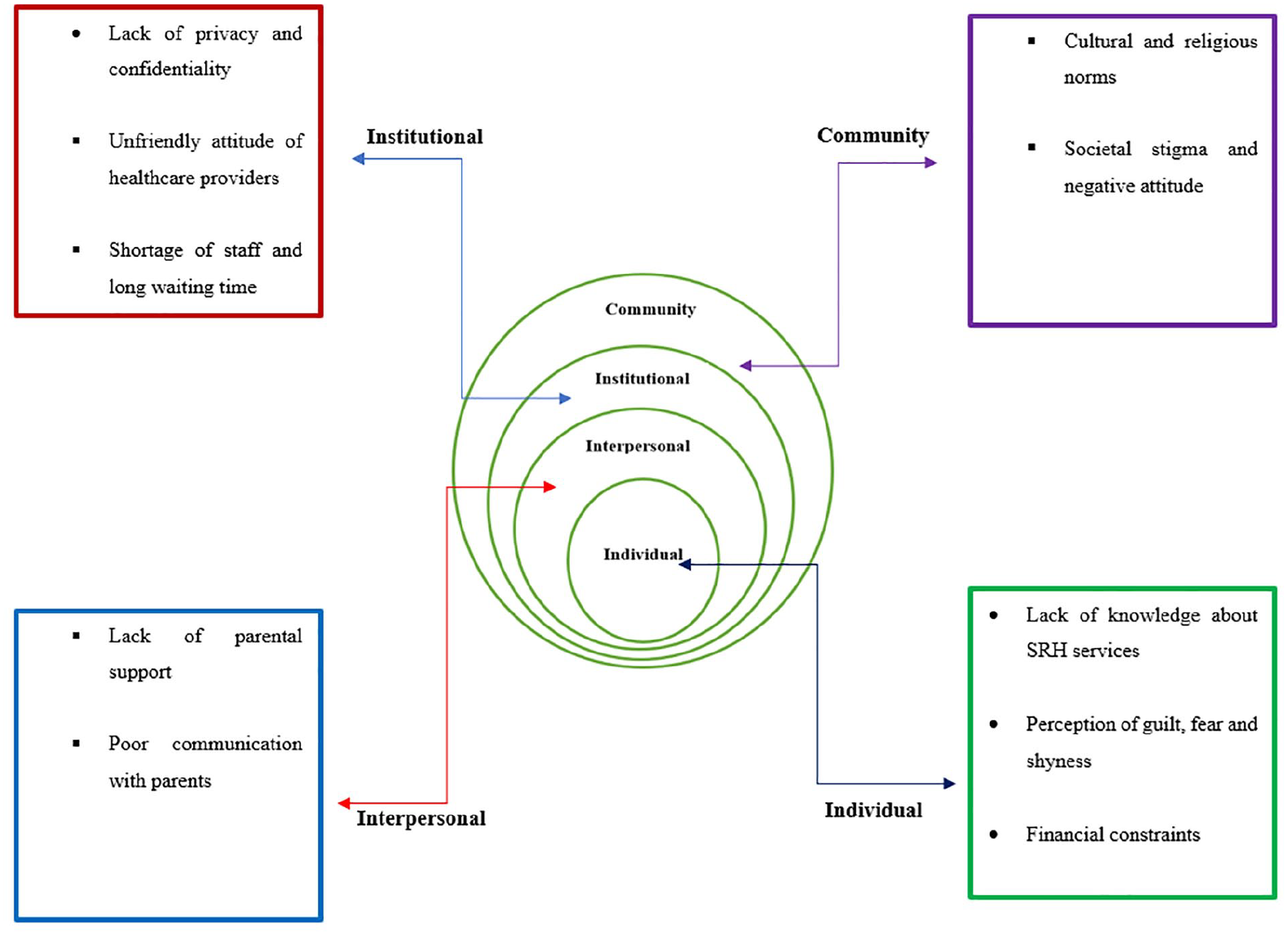
Barriers influencing sexual and reproductive health service utilization using the Socio-ecological Model.
Barriers at the Individual Level
Lack of Knowledge About SRH Services
One of the key barriers to participants’ utilization of SRH services was the lack of information on accessible SRH-related resources, counseling, and available services. This knowledge gap was highlighted by a participant, who expressed a shared concern in the group when she said the following; . . .so, most of us are ignorant of many things because we are not aware of anywhere to ask for information on such matters. There is no place where one can get information unless health workers can come to schools to give them the information. (G6P9, 22-year-old male) I feel that we need to be educated about the conditions we might have as females and how to get help when we have any problems. Some people are more enlightened than others, but the information is not widespread. (G3P2, 18-year-old female)
Individual Perception of Guilt, Fear, and Shyness
Some of the participants experience feelings of fear and guilt when discussing their SRH needs or seeking related information and services. This feeling can stem from individual personality traits or concerns about being judged or embarrassed by others, including SRH service providers. This barrier can discourage young people from seeking formal SRH services, causing them to internalize their SRH needs or problems or only confide in close friends. Examples of such feelings are captured in the excerpts below: Individual perception is a major hindrance. . .some people feel guilty talking about sexual matters, they feel guilty and afraid of what other people may think about them. (G3P8, 16-year-old female) One of the challenges we face is that many of us are too shy to open up and seek information or help when needed. Like me. . ., I sometimes feel like. . .how will people look at me? (G4P8, 23-year-old male)
Financial Constraints
Participants identified the inability to afford the cost of some of the services as one of the barriers they encountered. One of the participants put it as follows: Your finances as a teenager are limited. . . Let’s say you have an infection from sexual activity and you want to go for treatment. . .. if you need to pay for tests. . .or get drugs. . .and you do not have the money. . .it’s a barrier, a big one. (G3P8, 16-year-old female)
Another participant in the same group shared her experience: It is even more costly to access treatment when you have female conditions like fibroid or polycystic ovarian syndrome. I remember my experience in the hospital when I went for some tests, it cost me a lot of money. One test cost ₦22,000 (approximately $30 at the time of the study), and it was extremely challenging for me to secure the funds. (G3P6, 19-year-old female).
Interpersonal Factors
Lack of Parental Support
The participants highlighted the fact that many parents restrict their children from accessing SRH information or services, and some parents do not provide adequate financial support to their young adults seeking SRH services. Furthermore, parents' overreaction and overprotective attitudes on issues related to SRH create barriers for young people. This is illustrated by the personal experience shared by a female in-school participant: And you know how parents too. . .are not helping in that aspect. . . Like my dad will tell me: ‘If you like, go and have sex and get pregnant, once that happens, your schooling is finished.’ How will I then let him know if I need the type of information or service related to what we are talking about? So, parents have a long way to go about this. (G1P8, 21-year-old female)
Also, a male out-of-school participant said; We have been made to believe that young people are not meant to be discussing sexual matters, I am often excluded from conversations about sex and told to leave the place where such discussion is taking place. . . When I attempt to ask my parents or older brothers about sexual matters, they usually respond with disapproval, questioning whether I should be thinking about such things. (G6P7, 24-year-old male)
Poor Communication with Parents
Some participants believed their parents should be their first contact for information on SRH, however, the majority do not have good and open communication with their parents on matters relating to SRH. Hence, if and when they need SRH information or services, they are unable to seek such openly because of the fear of their parents.
Communication (with parents) is not good. I think this communication is the priority barrier to address. (G1P5, 23-year-old female)
A male participant revealed that many young people prefer to confide in their friends than their parents: Most times, young people are unable to confide in their parents. . . Many parents are not so open that they (the children) can speak about what they are going through. . .So parents should be more open to their children, and get closer to them so they can confide in them when they get to such a stage. (G4P11, 18-year-old male)
Institutional Factors
Lack of Privacy and Confidentiality
One of the major institutional or health-system level barriers mentioned by the participants is the lack of privacy young people experience whenever they go to clinic/healthcare facilities for SRH services. They were also significantly concerned about the confidentiality of the information they gave healthcare workers. Young people seeking SRH services in health facilities feel uncomfortable sharing their health history with health workers because of a lack of confidentiality. Participants reported instances where health workers inappropriately shared a client's SRH information with others, sometimes even in the client’s presence.
I remember a day when a health provider was teaching his students who were on internship and he used me as an example without my consent. I felt humiliated and disrespected because he didn’t ask if I was willing or comfortable to be presented as a case for his teaching. (G3P6, 19-year-old female)
A male participant also expressed a shared concern; As for me. . . I do not find it easy to go to a health facility because I am concerned about my privacy and whether my personal information will be handled with confidentiality, and I know many of my friends who feel the same way. (G4P6, 18-year-old male)
Unfriendly Attitude of Healthcare Providers
The participants were almost unanimous in their complaints about the disposition and unfriendly attitude of many healthcare workers. It was also noted that some health workers display subtle or obvious judgemental attitudes toward adolescents and young people when they seek SRH care and services.
Some are not friendly, especially to young girls, and some are too harsh. Like me, when I was 16 years old. . .I wanted to do a test. Someone told me about the test but when I got there. . . If you see the way the woman there shouted at me, and asked me very embarrassing questions in a very aggressive way. (G1P8, 21-year-female) . . .if I need anything, I will not go to those health centres. My friends told me that the staff there have a way of looking at their clients with a judgemental attitude when they seek sexual-related services. If I need any information or treatment, I would prefer to go online. (G1P5 17-year-old male)
This unfriendly attitude of some health workers restricts young people from seeking SRH services. According to one of the participants, the attitude of the clinic staff hindered her from seeking certain SRH-related information regarding her genotype.
I could remember when I did genotype, I wanted to ask a question about it, but I could not ask again when I saw their attitude. I just kept it to myself and I checked online. (G5P9, 22-year-old female)
Shortage of Staff and Long Waiting Time
Another factor identified by the participants as a barrier to the use of public health facilities for SRH services is the long waiting time in the clinic. According to them, it is mainly caused by inadequate medical staff to attend promptly to all the clients. As a result, patients face long queues and spend many productive hours waiting to see healthcare providers.
I think nurses and doctors are few. They are short-staffed than to be asking for history. They also have limited time because they have a lot of patients to attend to. So, I know they are short-staffed, so they will not have time for the clients to express themselves. (G5P2, 21-year-old female)
Community-Level Factors
Cultural and Religious Norms
It was found that young people lack the freedom to discuss issues affecting their SRH with their peers and older adults, including their parents because of the cultural and religious norms in the community. According to the participants, it was generally believed that SRH issues are reserved for married people and it is morally wrong to involve young unmarried people, especially adolescents, in such discussions. Such norms were rooted in the belief that restricting access to SRH-related information would promote chastity, moral uprightness, and avoidance of culturally unacceptable practices like premarital sex.
One of the major barriers is that we have been made to believe that sexual topic is not meant for young unmarried people. . . because they will say you have not gotten to the stage to know about it. So, we are meant to believe that when we are talking about sexual matters, it’s like we are sinning. (G6P7, 24-year-old male) In our culture, it is like a taboo to have sex before marriage, especially at such a young age. So, when we do it (sexual act), we don’t want our parents or the older ones to know. . . and when we have any problem, we are afraid to go to the hospital. . . someone who knows me may see me and ask why I came. (G3P8, 16-year-old female).
Societal Stigma and Negative Attitude
Many of the participants identified the stigma and name-calling in the community as a constraint to accessing SRH services. According to the participants, when a young person attempts to visit a health clinic for SRH counseling or services, he or she is at risk of being stigmatized by some of their peers and other members of society.
Given that SRH services are usually provided within the confines of regular general health care centers/services, some young persons who require SRH-related care prefer to stay away from such clinics because of the fear of being seen by someone who knows them and who might inquire why they came to the clinic.
Let’s say you want to go to the clinic to seek care or ask for information. . . Then you are like. . .what if I get there and meet someone, maybe an adult who knows my family, and the person starts to look at me suspiciously and ask ‘Why are you here.’ Or if they hear me asking some questions, they may react discouragingly. (G3P9, 17-year-old female)
A male participant expressed his displeasure about the experience he had with a salesgirl; In certain stores, they do not sell condoms to young people, and they go as far as asking for your age. . .. As for me, I always want to get a good condom at a stable supermarket so that I will not buy all these perforated ones at the roadside. On getting there (the supermarket), the salesgirl said to me, “You too have started using condoms. . ..” To me, this is embarrassing and it is a kind of a barrier. (G4P1, 16-year-old male)
Participants indicated that the fear of stigmatization is one main reason why some victims of sexual assault do not bother to report or seek appropriate health care.
For people that are assaulted or raped, most times, the reason why they do not go to seek help or care is because they are afraid of the way society will begin to look at them if the information gets out. (G3P2, 18-year-old female)
Discussion
This study identified a web of interrelated barriers that prevent young people from accessing and using SRH services, highlighting the need for a comprehensive approach to address these challenges. At the individual level, findings from this study revealed that lack of information on where to obtain SRH-related information and counseling was one of the barriers to the utilization of SRH services among young people. This aligns with existing studies (Eremutha & Gabriel, 2019; Nmadu et al., 2020; Wakjira & Habedi, 2022), highlighting the persistent challenge of inadequate information about SRH services, which hindered the uptake of these essential services. The poor information about SRH services among the participants can be attributed to several reasons such as limited sex education, stigma, and cultural taboos surrounding SRH-related topics (Adione et al., 2023). To mitigate this, it is important to implement comprehensive sex education programs, promote open and non-judgmental discussions, and ensure the availability of easily accessible SRH information resources.
Another key factor influencing the use of SRH-related services is individual perceptions of shame, fear, and shyness, this finding is in agreement with previous studies (Abuosi & Anaba, 2019; Ezenwaka et al., 2020). These perceptions and feelings of shame and fear can be deeply ingrained in cultural, societal, and personal beliefs. It is also worth noting that young people’s fear of stigmatization can be a powerful deterrent, preventing individuals from seeking the help or information they need (Nmadu et al., 2020). The tendency to discuss SRH issues only with close friends is common among young people. While peer support might be beneficial, it does not always offer reliable information or access to professional services.
Financial constraints were another barrier to the utilization of SRH services, which aligns with some earlier studies conducted in developed and developing countries, including Nigeria (Abuosi & Anaba 2019; Ezenwaka et al., 2020; Sidamo et al., 2023; Wakjira & Habedi 2022). This finding could result from the fact that most of these young people are still dependent on their parents and families as their major source of income, making it challenging to allocate funds for healthcare expenses and difficult to request such financial assistance from their parents. This is compounded by the fact that many SRH services in the country are not free. Patients are expected to pay out of pocket if they do not have health insurance for services such as registration for consultation, diagnostic tests for sexually transmitted infections, family planning services, and abortion or post-abortion care. Even in settings where some of the services are free or subsidized, the transportation fee to these facilities could still be a challenge.
At the interpersonal level, lack of parental support was another barrier to the use of SRH services by young people. This finding is consistent with previously documented studies (Munea et al., 2022; Sidamo et al., 2023; Wakjira & Habedi 2022), most of which were conducted in Sub-Saharan Africa. Many parents restrict their children's access to SRH information or services due to the belief that they are too young to be involved in matters related to SRH. Additionally, cultural or religious beliefs held by parents may limit open discussions or access to SRH services (Adione et al., 2023). Parents’ concerns about encouraging sexual activity among young people may lead them to withhold SRH-related information and restrict access to SRH services. While these overprotective measures may stem from a desire to safeguard their children, they can ultimately undermine young people's ability to make informed decisions about their own sexual and reproductive health, compromising their autonomy, and ultimately putting them at a disadvantage.
As previously reported, poor communication with parents was also presented as one of the barriers to accessing SRH services among young people (Ezenwaka et al., 2020; Sidamo et al., 2023). Many parents mistakenly assume that talking to their children about SRH will promote promiscuity, causing them to shy away from these important conversations. However, young people expressed a desire for their parents to be their initial point of contact for SRH information, highlighting a significant gap between parental perceptions and the SRH needs of young people (Ezenwaka et al., 2020). Additionally, some parents may lack the requisite knowledge and understanding of SRH to provide effective guidance and support to their children. To address this barrier, it is essential to empower parents and caregivers to offer comprehensive support for young people in accessing SRH services and making informed decisions about their sexual and reproductive health (Sidamo et al., 2023).
At the institutional level, lack of privacy was a major factor highlighted by the participants which agrees with some earlier studies (Nmadu et al., 2020; Mutea et al., 2020; Onokerhoraye et al., 2017). Limited privacy for patients in healthcare facilities, often due to insufficient rooms for private consultations, limited resources, and overcrowding, can deter young people from seeking SRH services. The embarrassment and discomfort of discussing personal SRH concerns in a public setting, coupled with the fear of judgment from healthcare providers and peers, can prevent young people from accessing essential care and openly addressing their SRH needs. Healthcare institutions should create private and inclusive spaces for young people to access SRH services without fear or judgment (Nmadu et al., 2020). This can be achieved by designating separate waiting areas and consulting rooms, educating them about their privacy rights, and offering alternative options like telehealth and online consultations (Mutea et al., 2020).
Findings from this study also revealed that young people seeking SRH services in health facilities felt uncomfortable sharing their health history with health workers because of concerns about confidentiality. This finding corroborates previously documented studies (Mutea et al., 2020; Nmadu et al., 2020; Onokerhoraye et al., 2017). Confidentiality concerns, including the potential for information misuse or unauthorized sharing, can prevent young people from accessing SRH services. Additionally, they may be unaware of healthcare providers' confidentiality responsibilities. To address this, healthcare providers and institutions should prioritize confidentiality through training and clear policies to maintain patient trust (Eremutha & Gabriel, 2019).
The negative attitude of healthcare providers, characterized by unfriendliness and judgment, remains a significant barrier to the utilization of SRH services among young people (Nmadu et al., 2020; Wakjira & Habedi, 2022). Personal biases and stigmatizing attitudes among healthcare providers can create barriers for young people seeking SRH services (Hailemariam et al., 2021). Moreover, inadequate communication skills can lead to unintentional harshness when discussing sensitive SRH topics. Training healthcare workers to be empathetic, culturally sensitive, and youth-friendliness can help overcome these barriers and encourage more young people to seek SRH services without fear of being judged or mistreated.
The long waiting times at public health facilities for SRH services is a recurrent challenge in many developing countries attributable mainly to inadequate personnel and infrastructure (Landa and Fushai, 2018; Mutea et al., 2020). The pervasive use of mobile phones among young people presents an opportunity to leverage virtual consultations and scheduled appointments, thereby reducing wait times and improving access to SRH service.
The impact of cultural and religious norms on SRH utilization cannot be overemphasized, in line with previous studies (Dioubaté et al., 2019; Hailemariam et al., 2021; Nmadu et al., 2020; Sidamo et al., 2023; Thongmixay et al., 2019). Sociocultural and religious norms that discourage open discussions about SRH among young people can pose substantial barriers to accessing essential information and services. These norms often prioritize modesty and chastity, leading to a reluctance to engage in open conversations about SRH. Additionally, many religious traditions have moral guidelines that implicitly prohibit discussions about SRH outside of marriage.
The constraints associated with societal stigma and negative attitudes toward young people seeking SRH services have been consistently reported in many studies (Dioubaté et al., 2021; Mutea et al., 2020; Nmadu et al., 2020; Sidamo et al., 2023; Wakjira & Habedi, 2022). Most African societies hold conservative views about SRH-related matters leading to judgmental and negative reactions toward young unmarried persons who seek SRH information or services. There is a need for culturally sensitive approaches that respect these norms while still providing young people with accurate age-appropriate SRH information and support (Sidamo et al., 2023). The following measures might be helpful: community-based education, involving religious or community leaders in awareness campaigns, and creating safe spaces for young people to discuss SRH topics without fear of judgment or moral condemnation (Eremutha & Gabriel, 2019).
A previous study (Ezenwaka et al., 2020) explored the challenges adolescents faced in accessing contraceptives among stakeholders such as policymakers, community leaders, health service providers, and parents using the SEM framework. The perspectives of stakeholders largely aligned with the views of the young persons in the current study on the majority of individual, interpersonal, institutional, and societal barriers. One notable difference was in the area of gender norms. Ezenwaka and colleagues identified this as a significant barrier, noting that adolescent girls seeking contraceptive information and services are often viewed as wayward, whereas boys rarely face such gender-based bias. A systematic review by Sidamo et al., (2023) also underscored the barrier of gender norms. However, in the present study, respondents did not recognize gender norms as a barrier and they did not report gender differences in the impact of the various levels of barriers they experienced in accessing SRH services. The discrepancy in findings may be attributed to the fact that this study focused on the experiences and viewpoints of the young people directly impacted by these barriers. As the primary stakeholders, they are better positioned to indicate whether they perceive gender bias in accessing these services.
Strengths and Limitations
The cultural norms and secrecy surrounding the topic of sexual and reproductive health in the study setting might serve as limitations for providing detailed information by the participants. However, they were assured of confidentiality while seeking consent for the study and the result showed that participants offered useful information. Nevertheless, it should be noted that the cultural and religious context in Nigeria strongly disapproves of homosexuality and transgender identities, and legislation criminalizes alternative sexuality (Ojoniyi, 2018). Although stigmatization, discrimination, and limited access to public health resources experienced by sexual minorities in Nigeria have been recognized (Ibigbami et al., 2023; Makanjuola et al., 2018; Sekoni, 2020), because of these censures and to protect participants from legal and social consequences of any disclosures, we did not explore the influence of gender identity and sexual orientation on access to sexual health services in this study. Furthermore, individual interviews might have given the participants more freedom to speak, however, FGD was used to allow for robust discussion where participants could validate or relate with the experience of others in the group. Nevertheless, to mitigate any concerns, the authors utilized their expertise to create a secure and confidential environment for the participants. The participants were assured that all information shared would be strictly used for research purposes only and encouraged to express themselves freely. Additionally, they were encouraged to share others’ examples or experiences, to help facilitate open and truthful discussions. Furthermore, before the discussion began, the authors used ice-breakers to create a relaxed atmosphere for free expression and participants were informed that there was no wrong or right answer, hence everyone was free to express themselves.
This study drew strengths from applying the socioecological model to identify and explain barriers hindering young people's access to SRH services. It also captured diverse perspectives from both in-school and out-of-school young people.
Implication for Practice
This study highlights the need for healthcare providers, particularly nurses, to adapt their approach to better serve young people seeking SRH services. Nurses should be specially trained in providing youth-friendly care, and act as mentors or facilitate peer support groups for young people to discuss SRH concerns in a safe and supportive environment. Healthcare facilities should create private spaces for consultations and reinforce the importance of maintaining the confidentiality of SRH information. To address the knowledge gap at the individual level, it is crucial to implement comprehensive sex education programs and ensure that accurate and reliable SRH information resources are readily accessible. Empowering parents/guardians is important to ensure they can provide appropriate support and guidance to young people, enabling them to access SRH services and make informed decisions about their sexual and reproductive health.
Conclusion
The study identified various interwoven barriers to SRH uptake across the different levels of the SEM framework, including individual, interpersonal, institutional, and community factors. The interrelatedness of the various factors underscores the need for multifaceted strategies and interventions to improve access to and the use of SRH information and services among young people in the study setting. Also, this study shows that some of these barriers have been identified previously, the fact that they still exist may indicate that the effectiveness of existing SRH policies and interventions needs to be reviewed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No. G-19-57145), Sida (Grant No:54100113), Uppsala Monitoring Center, Norwegian Agency for Development Cooperation (Norad), and by the Wellcome Trust [reference no. 107768/Z/15/Z] and the UK Foreign, Commonwealth & Development Office, with support from the Developing Excellence in Leadership, Training, and Science in Africa (DELTAS Africa) program. The statements made and views expressed are solely the responsibility of the Fellow.