
Abstract
Men who have sex with men (MSM) bear a disproportionate burden of HIV in China and are particularly vulnerable to mental health challenges. This study is phase one of a multi-phase project that aimed to identify unmet needs of MSM living with HIV to inform the development of a multi-level intervention. We interviewed 24 stakeholders through videoconferencing, including 15 MSM living with HIV, five staff from a community-based organization serving gender and sexual minority individuals, and four staff from the Centers for Disease Control and Prevention in Shanghai, China. We conducted content analysis using inductive and deductive coding and identified the following themes: 1) Navigating Turbulent Waters: multi-level stress currents; 2) Mapping Anchors: multifaceted support network; 3) Staying Afloat: Daily strategies and functioning; and 4) Charting New Courses: paths for intervention. Examining the stress and coping process among MSM living with HIV from a socio-ecological lens is especially important in the collective cultural context. The interactive nature of the stress from multiple socio-ecological levels, lack of individual coping skills, and scarcity of psychosocial services highlighted the importance of community-based, multi-level interventions to meet the needs of MSM living with HIV in China.
Globally, 1.3 million people were newly infected with HIV/AIDS in 2023 (UNAIDS, 2024). In China, men who have sex with men (MSM) bear a disproportionate burden of HIV, accounting for a quarter of the new HIV cases in 2020 (He, 2021). The prevalence of HIV continues to be on the rise from 2001 to 2018 (Dong et al., 2019). The introduction of antiretroviral therapy (ART) and increased access to it has transformed the quality of life and increased the life expectancy for people living with HIV (PWH) (Gordon et al., 2021). Nevertheless, mental health problems such as depression and anxiety are elevated among PWH compared to general populations (Nanni et al., 2015). Intense emotional reactions and extreme behaviors such as suicide attempts have also been reported among PWH (X.-P. Y. Huang et al., 2020; X.-P. Huang et al., 2024). A nationwide, population-based cohort study in China examined people diagnosed with HIV between 2012 and 2018 and reported increased suicide risk among people with HIV compared with the general population (Chen et al., 2022). The prevalence of anxiety symptoms is elevated among MSM living with HIV (21%–42%) in China, compared to HIV-negative MSM (12%–26%). The prevalence of suicidal ideation ranged from 11% to 26% among HIV-infected MSM in China (Sun et al., 2020).
The stress and coping framework (Lazarus & Folkman, 1985) is commonly used to understand elevated rates of mental health conditions among PWH and inform coping interventions. When individuals perceive a situation to exceed the currently available resources (i.e., stressful), coping efforts are activated. Coping is often defined as a cognitive or behavioral response to a perceived stressful situation (Lazarus & Folkman, 1985). Certain coping strategies (e.g., direct action, positive reappraisal) are associated with positive mental health outcomes among PWH (Moskowitz et al., 2009). PWH face stressors from multiple aspects of their lives, such as navigating and initiating HIV treatment, adherence and engagement to treatment and medical appointments, side effects from medications, HIV-related stigma and HIV-related symptoms as the disease progresses (Moskowitz et al., 2009). Qualitative studies have revealed that the stress caused by living with HIV leads to chronic emotional challenges, persistent emotional distress, and mental illnesses among PWH (Snedker & Herting, 2016; Turner & Kelly, 2000). The stress is exacerbated among MSM living with HIV due to their sexual minority identity, which is often a target of discrimination and violence in some regions of the world, including China (Altman et al., 2012; Wang et al., 2019; Yang et al., 2020) .
MSM living with HIV in China experience stress from multiple sources in the given social context (Sun et al., 2020). There remains acute stigma around having HIV in China, which has led people receiving an HIV diagnosis to experience considerable distress and elevated mental health conditions (Y. Huang et al., 2020; Yang et al., 2020). The heterosexual norm and lack of legal protection against employment discrimination of sexual minorities and PLWH in China lead to concealment as the primary coping strategy (Suen et al., 2021; Yin & Couzin, 2020). The deeply rooted value of filial piety and the collectivistic culture can also be a source of stress. The emphasis on filial piety pressures MSM to fulfill their family duty of heterosexual marriage and “procreation” (Li et al., 2015).
Addressing the cluster of stressors and improving the psychosocial well-being of MSM living with HIV in China requires multi-level services that address factors across individual, interpersonal, community, institutional, and structural levels in a socio-ecological model (Kaufman et al., 2014). The current stress and coping literature in the context of PWH has several gaps that need to be addressed to inform the development of such services. First, studies on the coping process are highly individual-focused and stripped of context in quantitative studies that used self-reported coping measures (Moskowitz et al., 2009). Coping strategies were categorized in coping measures (e.g., avoidant, active problem-focused coping) that allowed little space to take into account the interaction between coping and the existing environmental factors such as availability of family support and social services. Quantitative studies focusing on PWH in China found positive coping strategies (such as problem solving) are associated with reduced psychological distress while avoidant coping was associated with higher depression and anxiety (Chan et al., 2006; Meade et al., 2010; Zhu et al., 2020). However, whether the coping method led to desirable outcomes (e.g., increased positive affect and resolution of problems) is highly dependent on the environmental factors, even for strategies that are commonly believed as adaptive. For example, seeking social support would only lead to a decrease in negative affect when the environment responds positively to individuals’ needs while resulting in increased stress when the effort is met with social rejection (Drydakis, 2022).
Second, most qualitative studies on stress and coping processes among PWH in China focus on one or two levels in the socio-ecological framework. One such example is a study that explored means of stigma-related coping among PWH and examined both intrapersonal, interpersonal coping strategies, and interpersonal factors (Y. X. Zhang et al., 2014). However, the community services and structural level policies that shape the stress and coping process are missing in this study. No study to date engaged multiple stakeholders to identify unmet mental health needs by capturing perspectives from PWH, their social network, and staff from HIV-related community and institutional services.
Third, emotional distress was rarely the focus of attention for qualitative studies on PWH in China, despite its impact on long-term psychological wellbeing (Stewart-Brown, 1998). The multidimensional nature of stress is often reduced down to the practical aspects of HIV-related stressors, such as medication and treatment engagement (Liu et al., 2016).
To inform the development of a multi-level intervention that addresses mental health needs among MSM with HIV in China, we need to gain a comprehensive understanding of stress and coping in the social context, specifically the needs and assets across all levels in the socio-ecological framework. Stakeholder interviews guided by the socio-ecological framework are an effective method to gain a holistic picture of a community’s needs that are shaped by factors from multiple levels (Kaufman et al., 2014). Emotional distress is common among people living with other chronic illnesses as well. It is important to note that although the focus of this study is on HIV, the findings from this study could offer insight into the study of other illnesses in other global regions.
The objectives of this qualitative stakeholder interview were to: 1) describe the stress and coping among MSM living with HIV in China; 2) examine how individual coping efforts interact with existing community and institutional resources by embedding the stress and coping in a larger socio-ecological context; 3) identify service gaps and targets for multi-level interventions.
Method
Design
This descriptive qualitative study employed content analysis in this needs assessment stage of a larger study, aiming to develop a culturally appropriate digital intervention for MSM recently diagnosed with HIV using a community-based participatory approach (Doyle et al., 2020; Elo & Kyngäs, 2008; Fereday & Muir-Cochrane, 2006). We established partnerships with Shanghai CDC and Shanghai Center for Sex Workers and Men who have sex with Men (SCMC) and formed a study team comprised of one staff from Shanghai CDC, one staff from SCMC, one MSM living with HIV, and the first author. The principles of shared decision making and mutual learning were applied throughout the research process. The study team collaboratively refined study procedures, developed interview guides based on stress and coping framework, interpreted results from stakeholder interviews, and synthesized findings.
Participants
Participants in this study include multiple stakeholders whose experience and expertise informed the study design and intervention development, including MSM living with HIV, staff at community organizations and government institutions who routinely work with people recently diagnosed or living with HIV. Staff members were recruited from Shanghai CDC and SCMC. SCMC has gained trust from the community through years of serving sexual and gender minority communities.
We recruited staff from SCMC whose job responsibilities centered around providing pre- and post-diagnosis counseling for the community to initiate linkage to HIV-related care. Similarly, Shanghai CDC has staff members designated to conduct medical check-ups and phone follow-ups with people living with HIV to ensure long-term treatment engagement. We recruited staff from Shanghai CDC to gain more understanding of policies and government regulations around HIV-related services that shape the experience of MSM recently diagnosed with HIV. The inclusion criteria for staff members at Shanghai CDC and SCMC were as follows: (1) age 18 years or older; (2) work with individuals living with HIV.
The SGM population is difficult to reach in the current study context. Privacy concerns around HIV status and sexual orientation presented as significant barriers to participants recruitment. To overcome these barriers and reduce bias in the recruitment process, the study team designed the participants recruitment information sheet and informed consent with careful wording, to emphasize the protection of participants’ privacy (e.g., camera off) and that the qualitative interview data presented in research activities (e.g., publications) will not be identifiable.
SCMC has gained trust from the SGM community through years of serving the community. As part of the post-diagnosis counseling service, individuals tested positive were added to a WeChat group. In China, WeChat is a widely used mobile application that is commonly used for free chat messaging. The WeChat group serves as both a forum for HIV-positive individuals to share their experiences, ask/answer questions and a platform for SCMC to share any updates about HIV treatment such as new medications or new policies. Therefore, we decided to have SCMC staff introduce the study to members in the Wechat group and send out eligibility screening surveys to those who expressed interest in the study. The inclusion criteria for MSM living with HIV include: (1) age 18 years or older; (2) HIV positive; (3) engaged in sex with a man in their lifetime; (4) already started ART; and (5) have access to the internet to participate in interviews. Moreover, participants filled out the Patient Health Questionnaire (PHQ-9) and were included if their score was below 15, indicating none-minimal to moderate depression (Löwe et al., 2004). The reason for this was to capture people who might benefit from a low-intensity mental health intervention. Due to the disruption of the pandemic, recruitment was conducted in three rounds from April 2021 to May 2022. All study participants who met the inclusion criteria provided written consent to participate in the study.
Procedures
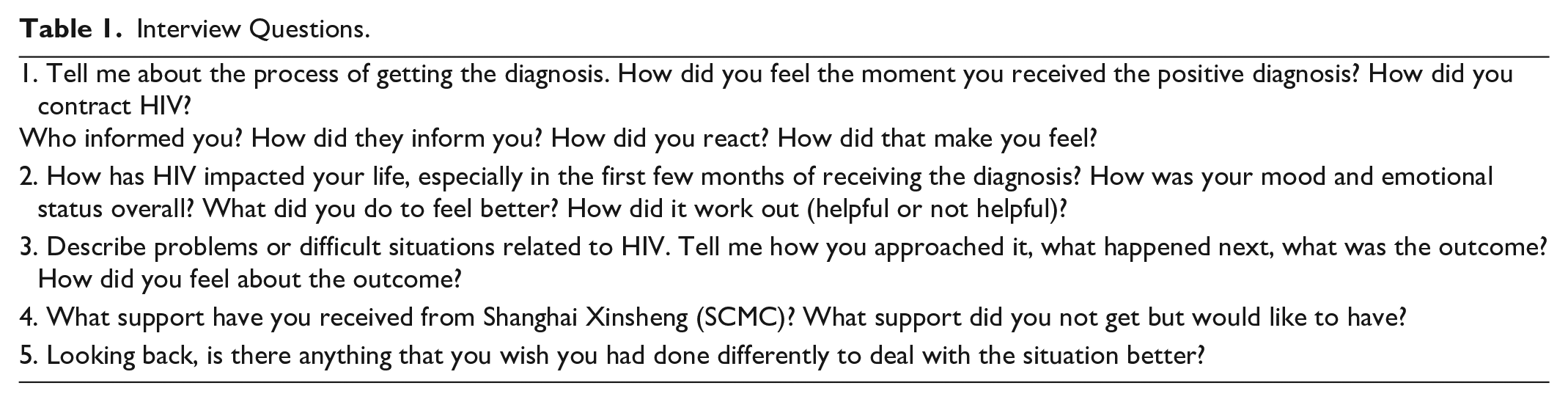
Using the participatory approach, the study team discussed and refined study procedure and semi-structured interview guidelines through biweekly online meetings (Table 1). After the interview guide was finalized, the lead author conducted online interviews using videoconferencing softwares with camera off. The interviews were conducted by the first author in Mandarin. To address participants’ privacy concerns and preferences, participants were offered options of one-on-one interviews or focus groups. All participants chose the one-on-one interview format. The online interview lasted 60 to 120 minutes. We obtained audio recordings of the interviews and collected demographic information after the interview. The recordings were transcribed using an online service (Xunfei AI transcribing service) and verified for accuracy by the first author. Each participant received $20 to compensate for their time and contribution to the study. This study was approved by the institutional review boards at the University of Washington (STUDY00011948).
Interview Questions.
Data Analysis
Interview transcripts were imported into the qualitative analysis software Atlas.ti (Version 9.1.3). Transcripts were in Mandarin and coded in English by the first author and third author who are bilingual. Data analysis was an iterative process that combined deductive and inductive coding (Table 2; Elo & Kyngäs, 2008; Fereday & Muir-Cochrane, 2006). This approach provides a clear direction for conceptualizing the data while allowing for the flexibility of incorporating unique experiences and novel information from the interviews (Nguyen et al., 2022). Specifically, we began with a deductive approach to form the initial categorization matrix based on established themes from stress and coping frameworks. Next, LW and WH conducted inductive opending coding of two transcripts, which allowed for the emergence of new codes and categories from the data. The codebook was generated after integrating the inductive codes and categories into the existing matrix. The codebook was then reviewed by the second (JM) and last author (WY) before being applied to code all transcripts. This iterative integration enabled our analysis remained both theoretically grounded and responsive to unique data insights, enhancing the robustness and depth of our findings.
Analysis Steps.

We used member checking and analysis memos to enhance the trustworthiness of the study results. The first author (LW), second author (JS), and the last author (WY) all have experience with qualitative research and working with people living with HIV or other chronic illness (Liu et al., 2016; Yuwen et al., 2017). Analysis memos involved detailed written notes of decision-making points during all stages of data analysis and interpretation. Member checking examined the accuracy of the results in relation to individuals’ experience. The analysis results were summarized and presented to participants who agreed to receive followup questions regarding the interview. Disagreements in the coding process between the first and second authors were resolved through extensive discussions and consultations with senior authors.
Results
Demographic Characteristics
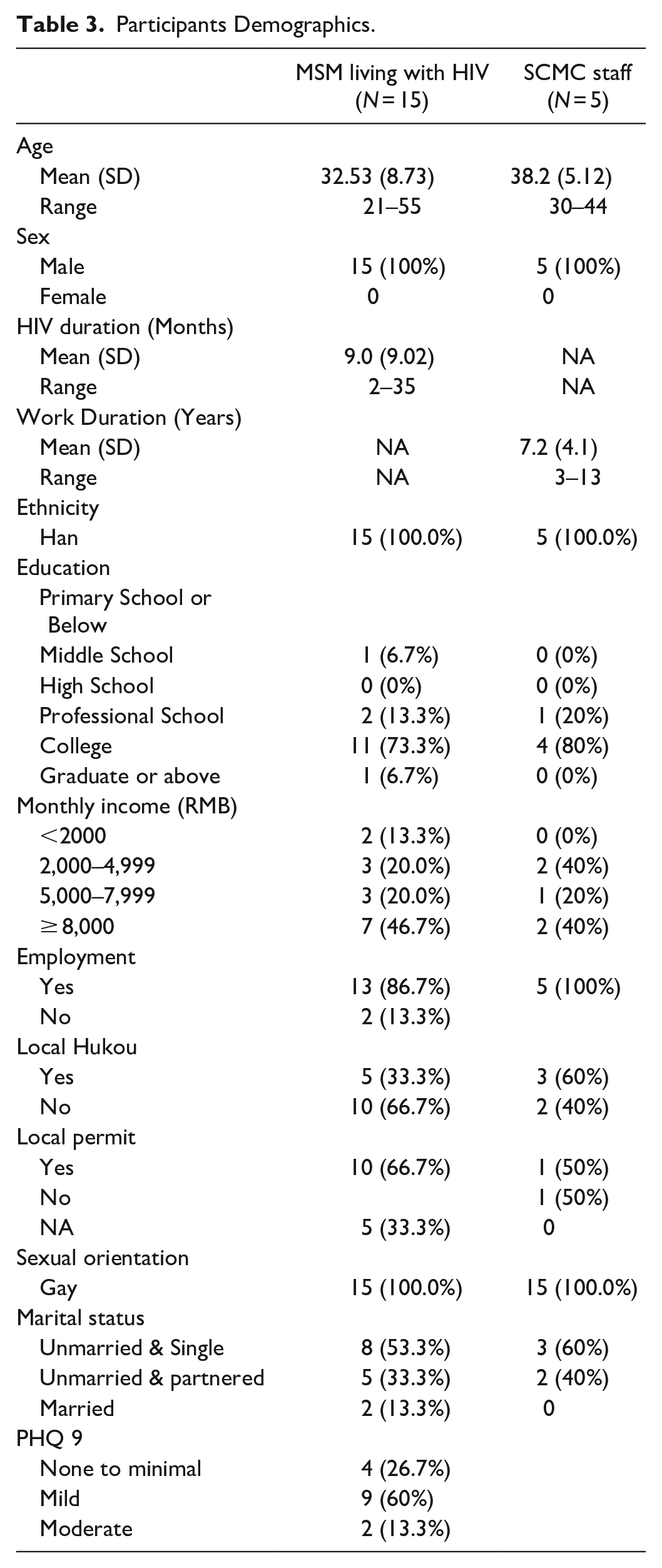
Among the 17 participants eligible for the study, one individual refused to participate due to health reasons and one participant withdrew from study 10 minutes into the interview, due to privacy concerns. Table 1 presents the demographic characteristics of the participants living with HIV (N = 15), SCMC staff (N = 5), and CDC staff (N = 4). The majority of the HIV positive individuals received college education or above (12/15, 80%), employed (13/15, 86.7%), and earned a monthly income higher than 5,000 RMB (about 685 USD, 10/15, 66.7%). About half (53.3%) of the participants received their diagnosis within the past 6 months (relative to the interview date). The average PHQ-9 score was 6.9 (SD = 3.47), indicating a mild level of depression. The majority of the HIV-positive participants (9/15, 60%) had mild depression (Table 3).
Participants Demographics.
Beyond Individual Resilience: Multi-Level Stress and Coping
Analysis of the interview data revealed that stress, coping, and outcomes were nested in a larger social context that could be conceptualized using a socio-ecological framework (Figure 1). Receiving the diagnosis was a stressful event at the individual level, while the cascade of stressors from interpersonal, community, institutional, and structural levels further contributed to emotional distress. Adjusting to the diagnosis and transitioning to living with HIV required ongoing individual coping efforts and environmental support. This study captured a snapshot of how the participants were doing (i.e., their outcomes) at this one time point along a dynamic journey of adjustment. We identified gaps where participants’ psychosocial needs were not met due to inadequate individual coping strategies and/or coping resources at multiple levels.

Multilevel stress and coping process: Stress and coping embedded in the socio-ecological framework.
Theme 1. Navigating Turbulent Waters: Multi-Level Stress Currents
Receiving an HIV diagnosis led to an initial intense emotional reaction, resembling the turbulent waves that challenge one’s sense of stability and control. Over time, individuals experienced stressors from multiple levels in the socio-ecological framework. SCMC and CDC staff recognized the complexity of multilevel factors playing into individuals’ adjustment and emotional responses (Figure 1).
The moment of diagnosis is characterized by a high level of arousal that was described by some participants as experiencing an emotional breakdown. Thoughts related to death, stigma, and future plans flooded into their mind, accompanied by a wide range of intense emotions. Participants reported a range of overwhelming emotions, including shock, intense fear, anger, guilt, shame, helplessness, and hopelessness. Some also described feeling suicidal and on the brink of despair. Emotionally overwhelmed, they were not able to process the information presented to them during the post-diagnosis consultation.
I was in shock and my brain was not working. I took notes when [a staff at CBO] explained the steps to initiate HIV treatment but did not remember anything. I couldn’t understand the notes I took at that time.
A long-term adjustment phase gradually unfolded as individuals started treatment. Parallel to this journey of adjustment, the emotional trajectory of fear, shame, and sadness revealed the compounded impact of factors from multiple levels in the socio-ecological framework (Figure 1)
At the individual level, the initial intense fear of death gradually transitioned into chronic anxiety as individuals perceived or experienced threats from multiple sources across the socio-ecological levels. The uncertainty around physical health, medication side effects, and disruptions of future plans caused worries that often spiraled into a panic state when individuals were unable to problem solve to reduce the anxiety. Stemming from internalized HIV-related stigma, shame also increased fear and anxiety. Internalized HIV-stigma surfaced as harsh and negative self-judgment, where participants reported feeling different from and inferior to those who were not infected with HIV. Some felt dirty, contaminated, and that their body was not whole/complete anymore.
I regret that I used to have a healthy body and now I have to live with this chronic illness. It’s gonna be my whole life. I also regret that I am now incomplete and dirty.
Due to the relational nature of Chinese society, individuals were particularly affected by the interpersonal implications of HIV-diagnosis. The decision-making around disclosure to family and friends was stressful on its own. Participants weighed the risks (e, g., social rejection) and benefits (e.g., social support) of disclosure, taking into account the quality and dynamics of their existing relationships. The value of family responsibility caused both sadness and shame for some participants, as they perceived decreased ability to provide for their family.
My parents are divorced. I live with my mom and my younger sister. I’m scared that I can’t take care of them in the future. I’ve been the breadwinner of this family.
Caring for others’ health and safety and perceived risk of HIV transmission caused participants to walk on eggshells, especially around their loved ones. These interpersonal implications caused individuals to feel like a burden to others. Together with insomnia, fatigue, lack of appetite, and suicidality, they formed a cluster of depression-like symptoms.
I felt like I should stop socializing with others (to not infect them with HIV), such as having dinner with them. I wanted to isolate myself. Sometimes I have thoughts like I’m inferior to other people. A lot of negative emotions towards myself.
At the community level, participants perceived the current online HIV+ and MSM community to be hostile, with discriminating comments on MSM living with HIV. Lacking a positive and supportive community, living with HIV was isolating and led to loneliness, sadness, and shame.
People online often point their fingers at people like us. They think we (PWH) should only hang out with PWH and should not harm/destroy other people’s lives.
At the institutional level, the discriminating behaviors from healthcare providers further intensified shame of being a person living with HIV and anxiety of interacting with the health system.
This is something that happened to me. I went to a tertiary hospital in Shanghai because I was having a fever. They thought I had COVID and asked if I had any chronic illness. They might have been asking about hypertension or diabetes, but I told them I had HIV. The physician at that time seemed scared. I felt discriminated against when he said people like me who did not have good immune function were more likely to get infected with COVID. He had strong reactions when I said I was HIV positive. He kept asking me questions about how I got HIV. Questions like “Did you get infected because you had sex with another man.” A lot of questions that concerned my privacy. I answered them all. But I felt extremely uncomfortable.
The structural and policy level, limited options of ART regimen and free CD4 and viral load testing, coupled with the high cost of self-paid viral load testing and medications outside of the government plan caused financial stress for participants. Additionally, lack of employment protection for persons with HIV threatened their job security and exacerbated their financial instability.
I lived constantly in fear. Because you finish one month of medication and have to pay for the cost of the next month. It was very expensive. I did not know how to cope with all of these. It was emotionally painful.
Theme 2. Mapping Anchors: Multifaceted Support Network
Participants employed coping strategies such as avoidance, problem-solving, and distraction while receiving assistance in the form of social support, community outreach, CDC services, and societal-level anti-stigma events. This multifaceted support network acts as anchors, helping individuals steady themselves against the turbulent currents of stress.
Individual Coping Efforts and Interpersonal Support
Most participants found it challenging to cope with the intense emotions in the early stage, despite the post-consultation service provided by CDC and CBO. Participants adopted denial, emotional suppression, social withdrawal, rumination, and social and career activities to distract from or block out emotions. On the extreme end, one participant quit his job to fully isolate himself. Some participants resorted to overworking or watching TV shows all day to block out and distract themselves from distressing emotions and thoughts about the diagnosis. However, attempts of blocking and suppressing emotion often backfired and did not relieve emotional pain for participants.
I was already depressed/feeling depressed (pre-HIV diagnosis). This was a huge shock. I felt so horrible that I just lied in bed the whole day watching Friends. I just kept watching until the sun went down. I’d get out of bed then and have some food and take the medication. Then I went back to bed and continued to watch the show. . . I lived constantly in fear. Because you finish one month of medication and have to pay for the cost of the next month. It was very expensive. I did not know how to cope with all of these. It was emotionally painful.
Problem-solving combined with acceptance was the main strategy participants used to regulate their anxiety and fear. They sought information from trusted sources, strategically disclosed HIV status to friends and/or family, and actively changed their lifestyle used to reduce uncertainty, maximize social support and minimize negative impact of disclosure. Through active engagement with activities hosted by CBO and CDC, individuals maintained connection to the community and cultivated a sense of belonging. Role models among peers living with HIV played a crucial role in generating hope, social learning of coping and problem-solving skills. Despite the problem solving efforts and assistance from CBO and CDC, there was still uncertainty and changes related to living with HIV that they could not resolve. Participants struggled with the anxiety around uncertainty and changes in their future while repeatedly emphasizing the importance of facing and accepting the reality. This process could be difficult and thus individuals emphasized the importance of being patient with oneself throughout this process to acceptance.
I went to an in-person gathering at SCMC. People shared their experiences living with HIV. Many of them have been taking medication for years. Some have only been taking it for 2-3 years. I haven’t started taking medication back then. I saw that people were pretty healthy and felt less worried about myself.
Generating more positive emotions was another coping strategy common among participants. Strategies used to create more positive emotions including engaging in pleasurable activities and finding meaning and value in their life going forward. Familial responsibility as an important value rooted deeply in Chinese culture kept some participants from giving up on their lives. Helping other newly diagnosed individuals by providing encouragement and emotional support was another value brought up by participants. However, they felt that their hands were tied due to lack of mental health related knowledge/training. Some were willing to but felt reluctant to share their personal story for lack of trust in and fear of negative reactions rooted in HIV-related stigma within the HIV positive MSM community.
He took us to karaoke and told me a lot of people there had HIV. I started thinking that if he disclosed others’ diagnoses to me, he probably would share my information with others as well. I did not want to socialize with him too much. . . I thought the diagnosis was people’s privacy and he did not respect that and probably would not respect mine either.
Social Services at CBO and CDC
CBO and CDC collaborate closely to provide services that assist individuals to navigate the journey post diagnosis. Services include providing post-diagnosis consultation, in-person gathering, forums, follow ups, and mental health referrals. The post-diagnosis consultation and forums provided by CBO and CDC aims to normalize the diagnosis for newly diagnosed individuals to reduce fear and anxiety. Social support was provided through in-person activities and wechat groups. During follow ups, although emotional support and mental health were not the focus of work, almost all CDC and CBO staff incorporated emotional check-ins in their work with individuals tested positive for HIV. Genuine and caring attitude from the staff members earned the trust from the individuals over time and hence they felt cared for and were more open to advice and guidance.
The work of CBO and CDC overlaps with a few differences in the focus of service. First, the emotional intensity differs between individuals receiving services from CBO and CDC. The work of CBO staff involved crisis management and intervention on the distressing moments immediately after diagnosis due to their role in post diagnosis consultation. Through long-term follow-up calls, CDC staff observed more chronic anxiety, such as anxiety about certainty around disease trajectory and long-term impacts on physical health from HIV treatment) among HIV positive individuals.
Second, the goal of service differs between CBO and CDC. CBO focused on the social aspects and specialized in targeted sub-population outreach, while CDC and CDC focused more on the clinical management such as medication adherence, treatment access, and engagement. The CBO in this study, Shanghai Xinsheng, mainly serve MSM, sex workers, and transgender individuals. CBO staff members described the organization as a “bridge to the community” for newly diagnosed individuals. For example, as part of the post-diagnosis consultation, the CBO staff invited MSM tested positive to join a WeChat group chat created by the CBO to form a connection with the MSM and HIV+ community. Many participants found the WeChat group to be a great place for obtaining the latest HIV related information, get their questions answered by peers, and stay connected to the community. This connection cultivated a sense of belonging and helped participants identify role models who inspired them to continue to live a productive life. Forums with health providers were meant to provide more information and give patients a platform to ask questions that were not perceived as very helpful.
In contrast, services provided at CDC focused on addressing issues in the clinical aspects of living with HIV, such as HIV patient management and policy-related work. Patient management involves consultation around clinical care and medical appointment follow ups to ensure engagement in medical care. For example, one staff member described an incident where she helped someone living with HIV to access care, who was refused medical service at a local hospital. The work of CDC staff informs policy development such as increasing the ART regime options into government plans and insurance coverage to reduce financial burden. CDC staff are also involved in social advocacy events such as HIV-awareness Day, which aims to educate the public about HIV-related knowledge and reduce HIV-related myths and stigma.
Theme 3. Staying Afloat: Daily Strategies and Functioning
Ongoing coping strategies played a crucial role in shaping long-term social and psychological functioning, helping individuals stay afloat. For many, the distressing emotions and thoughts that originated at the time of diagnosis persisted, creating ongoing turbulence. Individuals differed in their community connections, engagement with HIV treatment, and medication adherence, each finding their own way to navigate these challenges.
Most individuals reported resuming their daily social activities routines at some point after their diagnosis, with some adjustments made to incorporate HIV treatment in their life. Underneath this seemingly positive outcome of “back to normal life,” participants described constant struggles with the vicissitudes of emotions since the day of diagnosis, despite the overall decreased intensity of negative emotions such as fear and hopelessness. Suicidal ideation subsided as time went by but did not completely disappear. Participants described that they still had good and bad days and that sometimes the negative emotions were overwhelming.
It’s been a while. Every time I took medication, I could feel strong emotions coming up. Even right now when we are talking about this, the overwhelming emotions are like turbulent waves in the ocean. All the emotions mixed together like spices (and it’s difficult to describe them).
Participants made efforts to prioritize physical health by forming healthy habits such as a regular sleep routine and workout schedule. Nevertheless, they observed their physical health gradually declined due to HIV and medication side effects. It was still difficult for the participants to accept these changes in their physical health and the fact that they had to give up on their envisioned life trajectory due to the positive HIV diagnosis.
I had planned to study abroad. But now with HIV I had to think about how to find a physician/doctor in a new country and learn about the local policy related to HIV treatment. It is too complicated to figure out. So I gave up on going abroad. Regarding changing jobs, I also won’t do it for a while. HIV diagnosis will make it very difficult to change my job.
Individuals differed in the duration of the period of adjustment to reach the new normal, with some taking more time and detours than others. Participants who had mental health conditions prior to receiving the HIV diagnosis had more challenges adjusting to living with HIV. One such participant had depression and history of suicide attempts, coupled with chaotic family relationship and an unstable social support network, reported extended period of self-isolation, living in despair, and emotional swings.
My father always had drinking problems. He can get violent when he is drunk. I left home hoping to stay on campus, but my school refused to let me stay because of my previous suicide attempt.
At the interpersonal and community level, the outcomes differed across individuals. Some individuals reported improved quality and closeness of friends and family relationships after the disclosure of HIV-status and receiving support from them. In contrast, others were rejected by their family after disclosure of HIV-status and sexual orientation, which forced them into homelessness. While some individuals stayed connected with the HIV-positive community and utilized it as a source of support and gained a sense of belonging, others reported minimal engagement with the group activities held at CBO and CDC out of privacy concerns and lack of trust in the community. The latter group tends to heavily rely on their romantic partners or family, with some remaining isolated and deprived of the access to community support.
I stayed connected to the online community and my hope increased seeing them sharing their lives. I felt less lonely. Less depressed than before.
At the time of the interviews, all participants were on ART. Almost all participants were able to adhere to a daily medication regimen, increase their CD4 counts, and reach viral suppression. One individual reported still having difficulty accepting their HIV diagnosis till this day. According to CBO staff members, pill burden, side effects, and lifestyle (e.g., late nights and lack of regular schedule) are major reasons that were associated with poor adherence from their years of work with individuals living with HIV.
Theme 4. Charting New Courses: Paths for Intervention
Overall, the adjustment outcomes unveiled the turbulent waves of emotional experience. Participants’ voyages through these turbulent waves were complicated by dual challenges: a shortage of personal navigation skills to steer through emotional storms, and a scarcity of “safe harbors” within the social service landscape for comprehensive support.
While many participants expressed needs and interest in mental health services, very few individuals sought help from therapists due to the lack of mental health professionals, high cost, and low trust. Most relied on digital apps and self-help books to learn strategies to cope with distressing emotions and thoughts. One participant said he found someone to help him download Headspace (a meditation and mindfulness app) on his phone and has been using that to cope with anxiety, especially before sleep. Participants appreciated the attempted support from close friends and family members and pointed out that sometimes the support was provided when they were not ready to receive it. They also felt some friends and family could not exactly understand them and they would prefer to talk to a peer who was diagnosed with HIV and has lived experience.
The lack of psychological support and check-ins from staff members was a major gap identified by HIV positive individuals. Most staff from CBO and CDC recognized the need for providing psychological support to help HIV-positive individuals. However, they felt ill-equipped to provide appropriate support due to a lack of mental health training. To make up for the lack of mental health training, staff members emphasized the importance of being empathetic toward the patients. One CDC staff believed that mental health support is not necessary, and that extra support and attention will create pressure and exacerbate stigma against them.
If you just treat them like one of us, why do they need psychosocial support? Aren’t we all doing fine? If you treat them as persons living with HIV, a patient, they might feel pressured and feel the attention was unnecessary.
Other service gaps that are not related to mental health identified by patients were lack of timely response to adjustment of medication regime to address medication side effects, limited number of free viral load and CD4 count testing, and lack of timely follow up after regular physical exams. Individuals also wanted CBO to provide services to provide legal support around employment discrimination.
Member Checks
We conducted member checks with 6 participants during the followup participatory design sessions. Participants overall agreed that the summary of results was consistent with their experience. They expressed relief that they were not alone in having these struggles. A few participants emphasized that the summary about ongoing anxiety and uncertainty in their future especially resonated with them.
Discussion
To our knowledge, this is one of the few studies on MSM living with HIV in China that adopted a cultural lens by embedding stress and coping processes within the socioecological framework to assess community’s needs to inform development of a multi-level intervention. The participants portrayed their journey of adjusting to life with HIV as a long voyage through ever-changing waters, where the currents and tides of their socio-ecological environment constantly shaped their course. Four themes identified in this study were in line with stress and coping theory, including 1) Navigating Turbulent Waters: multi-level stress currents; 2) Mapping Anchors: multifaceted support network; 3) Staying Afloat: Daily strategies and functioning; and 4) Charting New Courses: paths for intervention. Although the emotional impact of the HIV diagnosis lingered into the present, HIV-related adjustment was overall positive, reflecting the resilience in individuals and their embedded support network.
Our results revealed the interactive nature of the factors from multiple socio-ecological levels, indicated by the dashed line in Figure 1. For example, the internalized stigma at the individual level interacted with and was reinforced by HIV-related stigma at the community, institutional, and structural levels. The shame and fear of disclosure drove individuals into self-isolation and were reinforced by HIV-related discriminating comments from friends and family and mitigated by receiving understanding and support. This interactive view of stress is consistent with the approach to identify behavior change factors for HIV prevention and care by (Kaufman et al., 2014). The authors mapped out the behavior change factors across socio-ecological levels and emphasized the highly interactive nature of the factors between micro and macro processes. Understanding individuals’ stress experience from the broader lens of a socio-ecological framework is especially important considering the social implications of the HIV diagnosis and the relational nature of Chinese society (Zhou, 2007). Individuals from collective cultural settings are more motivated to fit in and experience more distress when deviating from social norms (Kitayama, 2002). For example, studies on culture and stigma found PWH in collectivist societies experiencing heightened HIV-related stigma (Liamputtong, 2013). Individuals tend to interpret the diagnosis from a moral lens as bringing shame to family. Therefore, family could be a source of stress and burden depending on their reaction to the diagnosis (Ho & Mak, 2013). The interactive nature of stress in a relational culture highlights the importance of interventions that address stress from multiple socio-ecological levels.
We found that the coping process for Chinese MSM was social and embedded in the larger socio-ecological framework (Figure 1). Their individual coping process heavily relied on close relationships with friends and family, and some utilized the community resources such as activities hosted by Shanghai SCMC and CDC. Individuals’ coping with emotions was limited and community-level psychosocial support beyond the group activities was lacking. With a few exceptions such as meditation or mindful breathing, most of the individual-initiated coping efforts involved environmental resources to generate positive emotions (e.g., joy and sense of belonging, being loved and cared for) through engaging in social activities and value-oriented behaviors (e.g., helping others). Positive emotions, independent of negative emotions, are predictive of less psychological distress, increased resilience, and overall mental wellbeing (Tugade et al., 2004). It is also a form of behavioral activation, which is an evidence-supported therapeutic approach for depression, according to which pleasant activities are scheduled to counter the withdrawal tendency of depression and to increase positive emotions (Cuijpers et al., 2007). Additionally, participants used problem-solving to indirectly increase positive emotions by resourcefully utilized online platforms, services at CBO and CDC, and healthcare providers to identify role models and address their HIV-related treatment questions and challenges. Although problem-solving could be an effective strategy to reduce uncertainty, acceptance is needed, recognizing that it is unlikely to remove uncertainty completely in the case of living with HIV (Solomon et al., 2014). Accepting that an illness or injury as part of one’s life is associated with greater quality of life and lower level of depression and anxiety (Aaby et al., 2020). Individuals could benefit from balancing problem-solving and acceptance to strategically regulate emotions.
Implications for Multi-Level Intervention Development
At the individual level, participants struggled with coping with emotional distress while unable to obtain appropriate support or services. Participants could benefit from expanding the individual coping toolbox to more effectively regulate their emotions when support from others are lacking or not available. Coping interventions were developed directly targeting enhancing coping skills and demonstrated effectiveness in improving mental health outcomes, especially cognitive behavior and stress management interventions (Harding et al., 2011). Moreover, given the lack of mental health professionals in China and the concerns around privacy due to the social stigma attached to HIV (Feng et al., 2010 ; Zhao et al., 2017), peer-delivered intervention could leverage and maximize role models’ positive influence in the community to model effective coping and generate hope (Burke et al., 2022).
At the interpersonal level, disclosure interventions might also benefit PWH by increasing their social capital, relationship quality, emotional wellbeing, and access to care (Ding et al., 2011; Y. Zhang et al., 2021). Additionally, relationship-based interventions focused on communication and support skills can help close friends or family members to better understand participants living with HIV and provide appropriate support. Family support, when available, was regarded as most helpful by PWH (Yu et al., 2016). Information sessions about HIV for close family members and partners could reduce their misbeliefs around HIV and increase their ability to cope as a family, which may ease the tension in relationships after disclosure (Eustace, 2013).
The interview results revealed a lack of direct emotional support and mental health resources for individuals to cope with the emotional distress at the community and institution level. Mental health services need to be established and integrated into the current HIV care continuum. With a severe shortage of mental health professionals, training of staff at the community level is potentially an efficient solution to narrow the mental health service gap. SCMC and CDC earned trust with these community members over the years of serving the community, which would serve as a catalyst for effective intervention dissemination. Studies in resource-strained settings found the training of lay mental health workers to improve their knowledge, skills, and confidence in delivering mental health services a feasible approach to address mental health needs (Deimling Johns et al., 2018; Pallikkuth et al., 2021). Additionally, policy level changes are needed to continue to reduce the challenges for PWH by reducing medication cost, increasing free CD4 and viral load testing, and including more ART medications into the government-paid regime options. HIV stigma at the structural level could be addressed by establishing legal protection for PWH from employment discrimination, publication education of HIV, and stigma reducing training for healthcare providers.
Limitations
This study has several limitations. First, due to the convenient sampling method, individuals who volunteered to participate in this study were likely to share certain set of characteristics, such as relatively high interest in mental health, high trust in the CBO and researchers, low avoidance, and social withdrawal tendency. A few participants met the inclusion criteria but were not able to participate in the interview due to lack of trust in the researcher or severe depressive symptoms. Continuing collaboration with CBOs and integrating more research activities in CBO services might help researchers to gain more trust from HIV + MSM community. Interventions that aim to target PWH with severe mental health issues should use targeted recruitment to reach those most in need. Second, the interviews were conducted over a year, from April 2020 to May 2021, during which time COVID pandemic caused additional stress for participants. We recognize that the context of the pandemic might have made the coping process more difficult for our study participants. Nevertheless, given that this study aimed to examine the emotional distress and coping due to HIV positive diagnosis, we did not discuss the impact of COVID on individuals’ coping process in detail. Despite the aforementioned limitations, results from this study could be used to guide the timing, content, and format of a psychosocial intervention for MSM recently diagnosed with HIV.
Conclusions
Stress and coping is a social process that is better captured from a socio-ecological lens, especially in a collective Chinese culture. Receiving a positive HIV diagnosis leads to multi-level stressors that trigger individuals’ coping efforts. Environmental factors from multiple levels interacted and compounded the stress as individuals adjusted to living with HIV. Individuals coping strategies were limited and could benefit from learning skills to cope with extreme and persistent emotional distress. Mental health support at community level was lacking. Multi-level interventions are needed to integrate mental health services into the HIV care continuum to enhance individual coping skills, utilize community role models, and establish staff training on psychosocial support.
Footnotes
Acknowledgements
We are grateful for the participants that trusted the research team and received interviews. We are especially grateful for the staff at Shanghai CDC and SCMC who facilitated data collection and their commitment to improving holistic HIV care continuum for MSM and PWH in general.
Authors’ Contributions
LW designed the study, conducted interviews, analyzed data and completed manuscript writing. JS and LW conceptualized the study together, reviewed the codebook, and provided important comments and edits that shape the final draft of the manuscript. WH assisted LW with data analysis and provided comments and edits for the manuscript. LC assisted LW with IRB application, and study material preparation, and provided comments and edits for the manuscript. HZ assisted participants recruitment, provided important insight on how to best conduct the interview while protecting participants’ privacy, and reviewed the final manuscript. ZN assisted interview guideline and obtained IRB from Shanghai CDC. WY provided thoughtful guidance throughout the study, reviewed the codebook, and provided important comments and edits that shape the final draft of the manuscript.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Population Health Initiative Tier 1 Grant at University of Washington.
Ethics Approval and Informed Consent Statements
The University of Washington Human Subjects Division (STUDY00011948) approved the study. All participants provided informed consent to participate in this study.