
Abstract
Public representations of people who experience mental illness (PEMI) have been well documented within the stigma literature. However, studies about mental health nurses’ representations of PEMI are still scarce and characterized by contradictions. Using the theoretical concept of social representation instead of stigma, the current study aims to explore and understand mental health nurses’ social representations of PEMI. Qualitative research was conducted based on 13 semi-structured interviews with nurses from two psychiatric units in general hospitals. Data were analyzed using interpretative phenomenological analysis. Results showed that nurses’ social representations were characterized by paradoxes. They explicitly displayed positive social representations, while nuancing them from an implicit point of view. The nurses wanted to work toward a destigmatizing voice for PEMI while nuancing their assertions to sound honest and accurate, which led them to a state of cognitive dissonance.
Keywords
Introduction
In the last 70 years, people who experience mental illness (PEMI) have received increased attention within the stigma-related literature (Angermeyer & Schomerus, 2017; Hinshaw & Stier, 2008; Link & Stuart, 2017; Thornicroft et al., 2016). Originating in the work of Goffman (1963) and further developed in relation to the topic of mental illness by Link and Phelan (2001), stigma can be defined as stereotyped beliefs, prejudiced attitudes, and discriminatory behaviors toward a person due to a particular label attributed to them. Stigma directed at PEMI has essentially been studied from the general population’s point of view (Angermeyer & Schomerus, 2017; Link & Stuart, 2017), although the perspective of somatic healthcare professionals has received considerable attention in the stigma-related literature (Henderson et al., 2014). Studies have shown that both the general public and somatic healthcare professionals tend to display negative stereotypical beliefs, negative affective reactions, and discriminatory behaviors toward PEMI (de Jacq et al., 2016; Giandinoto et al., 2018).
In comparison, few studies in the stigma-related literature have been conducted specifically on mental healthcare professionals’ perspectives toward PEMI (Angermeyer & Schomerus, 2017). Mental health nurses (MHNs) are the largest group of professionals in mental health (World Health Organization, 2012), and are the mental healthcare professionals who spend the most time in direct contact with PEMI (Alexander & Link, 2003). Moreover, existing studies among MHNs present contradictory results with regard to both MHNs’ beliefs and behaviors toward PEMI (de Jacq et al., 2016). For instance, some studies have highlighted MHNs’ negative beliefs, attitudes, and behaviors that are comparable to those found among the public and somatic healthcare professionals (Dickens et al., 2022; Henderson et al., 2014; Hinshaw & Stier, 2008; Lauber et al., 2006; Ross & Goldner, 2009). In a large survey study on stereotypes, Lauber et al. (2006) found that MHNs characterize people with mental illness as being more “dangerous,” less “skilled” and more “socially disturbing” compared to other people. Other studies have identified MHNs as a source of discrimination that impacts the way they conduct patient care delivery (in terms of presenting rejecting, insensitive and disrespectful behaviors; see Henderson et al., 2014), as having a desire for social distance and displaying authoritarian attitudes, coercive and social restrictive measures toward PEMI (Henderson et al., 2014), and as demonstrating low expectations of improvement for PEMI (Dickens et al., 2022; Hinshaw & Stier, 2008; Ross & Goldner, 2009). However, other studies have depicted more positive beliefs, attitudes, and behaviors from MHNs toward PEMI. In those studies, MHNs were reported to believe that PEMI are creative, are able to work as others do, and are less unpredictable and dangerous than thought by the public (Cremonini et al., 2018; Del Olmo-Romero et al., 2019; Economou et al., 2020; Munro & Baker, 2007; J. D. Smith et al., 2017). These studies pointed out that MHNs show less fear, less anger, less authoritarian attitudes and a greater desire to help than displayed by the public (Del Olmo-Romero et al., 2019), along with diminished desire for social distance (Economou et al., 2020; J. D. Smith et al., 2017), and a lower propensity among MHNs to favor social and civil rights restrictions (Cremonini et al., 2018; Munro & Baker, 2007). These contradictory results about MHNs’ beliefs and behaviors toward PEMI raise questions about conclusions previously reached in the stigma literature. For instance, according to the stigma literature, spending time with PEMI and knowing about their illnesses are expected to improve attitudes toward them (Mehta et al., 2015; Thornicroft et al., 2016). But simultaneously, part of the stigma literature describes negative beliefs, attitudes, and behaviors among MHNs who spend extended time in direct contact with PEMI and are mental healthcare experts (Alexander & Link, 2003).
The contradictions present in the stigma-related literature about MHNs’ perspective can partially arise from the fact that much of the research carried out was based either on different populations of mental health professionals (psychiatrists, psychologists, nurses, social workers, etc.) or on nurses from different units (acute psychiatric units, chronic psychiatric units, intensive care units, community-based facilities, etc.; de Jacq et al., 2016; Dickens et al., 2022; Ross & Goldner, 2009). It is therefore not always easy to get a clear idea of the specifics with regard to MHNs, which calls for more systematic and in-depth research focused only on MHNs and considered according to their specific units (Del Olmo-Romero et al., 2019; Economou et al., 2020).
Moreover, those identified contradictions can also arise from the use of a variety of questionnaires and comparisons, generating heterogeneous results that are difficult to compare (de Jacq et al., 2016; Henderson et al., 2014). Many of the questionnaires use closed-ended responses and were initially designed from responses from the general population (Economou et al., 2020; Henderson et al., 2014). The use of these measures does not provide a coherent description of MHNs’ beliefs and behaviors toward PEMI, with whom MHNs engage in a deeper and more complex relationship than the public does. The use of an alternative method of data collection and analysis such as qualitative research would allow a complementary and more in-depth understanding of these contradictions.
Furthermore, the use of the notion of stigma directs attention toward negative beliefs, attitudes and behaviors toward PEMI, a bias that has been pointed out by some authors in the stigma literature (see Angermeyer et al., 2010 about the bias regarding prejudice and emotional reaction to PEMI). Focusing on negative beliefs could play a role in the contradictions seen in the stigma-related literature about MHNs’ perspective, as it prevents embracing the full range of beliefs, attitudes and behaviors MHNs endorse about PEMI they work with. Therefore, a shift in theoretical framework could offer another perspective on the contradictions found in the stigma-related literature so far (Angermeyer et al., 2010).
Our study aims to address these limitations and examine MHNs’ perspective about PEMI, guided by the social representation framework and using a qualitative research methodology. This shift in both theoretical and methodological approach could help to overcome the identified contradictions by offering another viewpoint on MHNs’ perspective on PEMI. Based on the insights of this study, we want to develop a more nuanced and in-depth understanding of MHNs’ perceptions toward PEMI, as well as point to directions for potential improvement of patient care delivery and wellbeing at work for MHNs (Angermeyer & Schomerus, 2017; Link & Stuart, 2017).
Theoretical Framework
Our theoretical framework is guided by the work of Moscovici (1973) on social representation theory. Social representation theory offers a social-constructionist approach for understanding how knowledge, beliefs and practices are socially constructed and mediated through interaction and discourse. Based on Moscovici’s work, a social representation can be described as the shared conception that a group of people has of a social object that has a special interest for this group (Moscovici, 1973; Wagner et al., 1999). This shared conception includes the elaboration of a series of values, ideas, metaphors, beliefs and feelings about the social object by a clearly defined community in their daily speech and actions (Moscovici, 1973; Wagner et al., 1999). Furthermore, these representations allow the group to attribute features and meanings to their social object of interest with a broad range of nuances. It allows the group to understand their social object of interest and to orient its practices and communicate about it within the complexity of the material and social world the group is dealing with (Moscovici, 1973; Wagner et al., 1999).
As social representations are the shared conception of a well-defined group of people, researchers have identified social representation theory as a suitable framework for community-based health research (Howarth et al., 2004). Howarth et al. (2004) found that social representation theory enabled them to identify how social representations influence how health professionals perceive, experience and treat health and illness. Social representations are not solely abstract ideas and concepts, but define interactions and practices, including care delivery practices, for MHNs, who renegotiate their representations in relation to the reality of every day’s work (Howarth et al., 2004; Sammut, 2016). These representations also encompass values and feelings (Moscovici, 1973; Wagner et al., 1999), giving the opportunity to consider as well emotional components of MHNs’ lived experience as care workers. Social representations allow consideration of the particular role MHNs play with PEMI, associated with specific practices, responsibilities and feelings for MHNs that are absent from the experiences of the general population.
Methods
The aim of our study is to explore and understand the social representations that MHNs have of the PEMI they encounter in their work. As social representations are not merely cognitive representations, but have also behavioral and emotional components and are built through everyday life interactions between MHNs and PEMI, we opted for a qualitative research design based on in-depth semi-structured interviews and interpretative phenomenological analysis (IPA).
IPA is an increasingly popular approach to qualitative inquiry, notably used in mental health psychology (J. A. Smith, 2011) to study illness representations, sexuality, identity, issues of stigma and the psychology of being a caregiver (Glasscoe & Smith, 2008; Hunt & Smith, 2004; J. A. Smith, 2009). IPA is interested in a person’s experiences of considerable significance and the “considerable amount of reflecting, thinking and feeling as they work through what it means” for them (J. A. Smith, 2009, p. 3).
Originating from phenomenology, hermeneutics and symbolic interactionism, IPA aims to understand participants’ social and personal experiences from their point of view, considering their experience both as a phenomenon they face and as a process they are active in (Shawn, 2019). IPA allows researchers to dig into participants’ experiences, thoughts, and beliefs, trying to grasp how they are articulated, rather than using a prior analysis grid. IPA allows researchers to approach both the meaning and the meaning-making of the participants (Antoine & Smith, 2017; Shawn, 2019). Moreover, IPA allows making interpretations about those experiences that follow the ways in which the participant depicts them. It is then considered appropriate to go beyond the participant’s own sense making and conceptualizations, while keeping them as a footing, in order to reach the closest possible understanding of the participant’s reality. An example of this could be examining subverbal cues (Shawn, 2019; J. A. Smith, 2009). However, IPA researchers are aware it is never truly possible to reach an exact understanding of the participant’s reality and that their own lenses are applied to the participant’s reality as well, creating an analytic process that is a double hermeneutic compound of the participant’s interpretation of their own reality and the researcher’s interpretation of the participant’s interpretation of their reality (Shawn, 2019; J. A. Smith, 2009). More specifically, in this study we aimed to focus on MHNs’ lived experience and address attention to what MHNs say about PEMI, how MHNs say it, and the feelings they express about PEMI (Antoine & Smith, 2017; Shawn, 2019).
Data Collection
Semi-structured interviews were conducted with 13 MHNs working in two acute psychiatric units in general hospitals. The units were selected because their similar structures allowed for a homogeneous sample. Typically, sample sizes in IPA range from a single case study to around 20 participants, with about nine interviews conducted on average (Antoine & Smith, 2017; J. A. Smith, 2009). The aim of IPA research is to delve as deeply as possible into a small body of data and carry out a detailed case-by-case analysis in order to get an in-depth understanding of rich experiential cases (Antoine & Smith, 2017; J. A. Smith, 2011). Table 1 provides a description of the sample with regard to sex and experience as mental health nurses.
Characteristics of the Participants (n = 13).

Note. Italicized names were given to participants from which quotes are transcribed in the findings section.
After the proposed research was presented during their weekly staff meeting, all the nurses present at that meeting stated their agreement to join the research or not. Two nurses declined to participate. The first author then met individually with the 13 volunteers from the two units. An interview guide with open-ended questions was used as support for conducting the interviews. The interview guide was created by the first author and tested with other qualitative researchers before being used with the participants. The interview protocol comprised five parts: (1) General introduction (to inform the participants, to introduce the topic to them, to thank them and set them at ease), (2) Exploration of how the participants describe PEMI (characteristics and features they attribute to PEMI, the conceptual framework and relevant categories they use to understand PEMI), (3) Exploration of what the participants do with PEMI as mental health professionals (clinical practices), (4) Exploration of the participants’ emotional components (what do they feel in contact with PEMI), and (5) Closing (to end the discussion and giving the opportunity to comment).The face-to-face interviews lasted between 95 and 225 min and were held outside the hospital context, at a place of choice selected by the participants.
Data Analysis
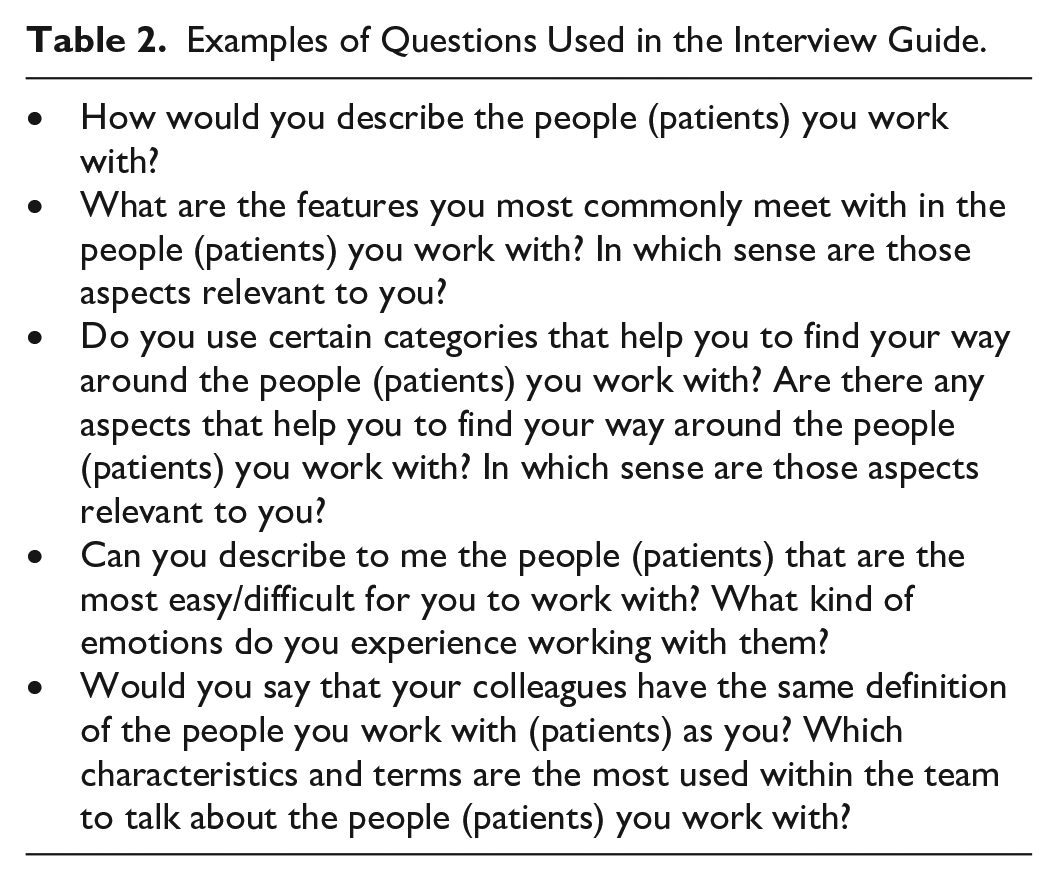
All interviews were audio-recorded with the participants’ consent and transcribed verbatim. All interviews were conducted, transcribed and analyzed in MHNs’ language (French). The examples of questions used in the interview guide in Table 2 and the verbatims quoted in this manuscript were translated to English. The interview transcripts were interpretatively coded using Nvivo 11. The analysis was carried out according to the steps recommended for IPA by the first author (J. A. Smith, 2009). The transcribed materials were read numerous times in order to generate codes of three kinds: content provided by the participant, notes on the linguistic and formal aspects of the discourse, and reflection on the content (association with theoretical concepts or topics addressed in other interviews). This was done for the different interviews in an iterative process one after the other. More specifically, the analysis of one interview and the themes emerging from it influenced the analysis of subsequent interviews, just as the analysis of an interview led to adding elements of analysis to previously coded interviews. Several support tools were then used to organize the codes generated: summaries of analyzed interviews and their coding, mind maps, and a reflexive journal kept continually throughout the analysis. Codes were clustered into superordinate themes, major themes and themes. Fragments related to the same codes were grouped to discover patterns that could be part of a particular trend. Results are presented through a description of each theme. Verbatim quotations are provided to illustrate the themes and to deepen the analysis presented.
Examples of Questions Used in the Interview Guide.
Ethical Considerations
Ethical considerations were followed during the data collection and analysis with regard to informed consent, anonymity/confidentiality, and concern for putting forward participants’ expertise (Sanjari et al., 2014). First, we obtained approval from the Saint Luc Hospital and Faculty Ethics Committee as well as of the head nurse for every unit before starting the research. Our interviews were held in other hospitals than the Saint Luc Hospital. Moreover, before starting each individual interview, the research objective was presented to the participants, ethical guidelines were stated, and a written informed consent form was signed. All participants received a document with the main elements of the research and the possibility of contacting the research team if needed. Second, special attention was devoted to guaranteeing participants’ anonymity from their colleagues in their unit, so that they could speak freely during the interviews. For reasons of confidentiality, all interview transcripts were also anonymized and safely stored on a locked device. Third, participants were encouraged to give their opinion on the research’s topic, aims and design. Their position as the primary subject-matter expert was put forward during the interviews.
Rigor
As the researcher is a psychologist and not a nurse, she presented herself and her interest in exploring this topic with the participants. They were encouraged to express their thoughts on the researcher’s motivation, the research topic itself and its relevance to their clinical practice. These reflexive comments were integrated into the analysis carried out afterward. A self-analysis was also carried out by the researcher throughout the data collection, analysis and writing process through a reflexive journal, to consider the necessary interpretation emerging from her personal position and its influence on the research. Moreover, trustworthiness of the analysis was achieved through the external view provided by several supervisors and colleagues familiar with this type of analysis, who reviewed the analysis carried out at different stages: coding, connecting and clustering themes, writing. Preliminary interpretations were shared and critically discussed among the research team (Strauss & Corbin, 1990). These different elements follow J. A. Smith’s (2009) recommendations on reflexive practice and validity in IPA research.
Findings
MHNs expressed difficulties naming their social representations of PEMI with enough nuances. They appeared uncertain and stated that they did not have a clear conceptual framework of social representations of the PEMI they work with. Our analysis did allow us to identify social representations, but they were structurally organized in paradoxes. These paradoxes were present in terms of both meaning and meaning-making. The explicit social representations MHNs expressed were positive, carrying a destigmatizing voice about PEMI. At the same time, they immediately nuanced their depictions of PEMI from an implicit point of view, as they were also eager to sound as honest and accurate as possible. These results are presented in the following section. Table 3 below summarizes the superordinate and major themes of the results.
Summary of the Superordinate and Major Themes.

PEMI and the Impossibility of Asserting a Conceptual Framework
MHNs stated that they did not have a conceptual framework giving them the vocabulary to help them understand the PEMI they met. Throughout the interviews, they expressed their difficulty in fixing and naming their social representations associated with PEMI. MHNs struggled to describe their representations in a way that satisfied them and was sufficiently nuanced for them. They presented themselves as hesitant and uncertain.
MHNs were asked about the conceptual support offered by diagnoses. They indicated using this support, but positioned considering diagnoses as not overly important. MHNs stressed how diagnoses helped them to make sense of situations encountered, but did not resolve the uncertainty they faced on a daily basis, sometimes lacked nuances and did not necessarily help them to direct care. Moreover, MHNs were wary of relying on this support, as diagnoses present risks of error and of locking PEMI into categories from which PEMI can no longer extract themselves afterward.
The diagnosis doesn’t really evoke anything to me. . . For example, when it says “manic phase,” yes, that certainly refers to [a mental health condition]. . . But look, “manic phase,” but what, what grade? If he’s better than he was two days ago, when he was completely decompensated [then what]? Is it put “observation” [to be collocated]? Is it put “manic phase,” but is he completely manageable in the unit? In any case, this diagnosis isn’t very clear, in the question of the degree. But depending on the case, there are quite few diagnoses that I find quite accurate. [But] I don’t [really] need a diagnosis. (Elliott)
As a result, MHNs lacked a shared network of social representations that they could elaborate together and on which they could explicitly rely as a team. This difficulty in naming common and structured social representations generated a particular complexity regarding working as a team.
MHNs explained their uncertainty as based on various aspects. First, MHNs emphasized the diversity of PEMI encountered in the unit: according to their experience, there were no typical profiles, but rather great eclecticism. As a result, formulating marked representations was presented as a challenge by MHNs.
For me, it could be anyone. It’s. . . it’s. . . it’s, it’s as much the mother of a family, it’s as much. . . the person who’s not in reality, it’s. . . it’s as much um. . . an 18-year-old who. . . who’s freaking out, well, it’s. . . it’s full, it’s, it’s everyone and no one at the same time, it’s. . . it could be you, it could be me. . . [Silence]. (Maddy)
Second, MHNs pointed out how the reality they faced was constantly changing. There was instability in the environment; only the experience of constant contradiction recurred. MHNs’ social representations therefore reflected these experiences marked by uncertainty, instability, and contradiction.
Psychotic patients, well, they’ll always be chronic patients. But someone who comes back several times will be a chronic patient even though he doesn’t have a pathology. . . which. . . can be chronic, so, I mean! [Silence]. Everything can be chronic, and not chronic. Because even in psychosis, for example, I think of the brief psychotic disorder. It. . . can only happen once, the brief psychotic disorder. Sometimes it’s a warning sign that there might be schizophrenia afterwards. But it can. . . just happen once because uh the person smoked a joint and it completely, uh, knocked him out and uh. . . and then it never happens again. (Maddy)
Finally, MHNs were driven by an ideal of non-judgment for and singularization of PEMI they work with. It was therefore important for MHNs to be wary of any definitive assertions and to present the most nuanced representations possible, while actively avoiding categorizing PEMI they work with. This is reflected in this exchange with Brittany:
Yes, but I could categorize them by. . . by all kinds of categories. I could put them into categories according to their pathology, according to their age, according to. . . according to their experience, I can put them into. . . into. . . into, into lots of categories, I mean it’s not easy like, uh. . . like. . . like a question [Laughing]. I wouldn’t know how to answer it.
And are there certain categories that speak to you, that are. . . that serve you, that are important to you? Categories that help you do your job?
No.
The only shared and clearly fixed representation that MHNs presented themselves as asserting was one of the suffering PEMI experienced. PEMI were described as experiencing significant suffering and needing help. PEMI’s symptoms and awareness of these could vary greatly, but were always present, sometimes to the point of being life-threatening.
The patient who comes to a, to a psychiatric service, well, in my experience, is someone who, who has a suffering which, hum, is often not recognised, who, who needs to come to this psychiatric service precisely so that there is some recognition of this suffering. For me, it’s a notion which is quite important, I think, in terms of defining what it is a, a patient in psychiatry. It’s effectively someone who has essential suffering, and when I say essential, it’s, it’s really in terms of the core, the inner core [of themselves] (Barry)
Social Representations About PEMI: A Story of Paradoxes
Although MHNs did not name a specific set of representations and stated that they did not have a conceptual framework per se, a general structure could be identified in their responses. MHNs’ social representations of the PEMI they met were characterized by paradoxes at two levels: in meanings and in meaning-making. Whether MHNs considered PEMI as a whole or individually, paradoxes emerged in their discourse. These are developed in the section below.
Considering PEMI as a Whole, Paradoxes in the Meanings
When MHNs considered PEMI as a whole, they presented two layers of representations, one explicit and asserted, the other more implicit and implied. These two layers were constructed in mirror fashion, responding to each other in a paradoxical way. We use the term paradox in the sense that a paradox results from a contradiction between two representations that diverge from each other but are nevertheless considered together as a whole. These two layers formed a paradoxical tandem, but both appeared true for MHNs.
The first layer was composed of explicitly stated representations that emphasized the positive characteristics associated with the PEMI that MHNs worked with. MHNs evoked a series of representations aimed at humanizing and individualizing PEMI, while emphasizing the environmental factors that played a role in their pathologies.
The second layer was composed of more implicitly present representations, immediately nuancing the first layer in the opposite direction. For each representation MHNs claimed explicitly, they evoked its counterpart in a more roundabout way: momentariness–chronicity, externality–internality, similarity–dissimilarity, individuality–categorization, humanization–dehumanization, agency–disability. These are developed in the section below. Although not all of the characteristics detailed below were present in every interview, this implicit/explicit double-layered structuring was present in the discourse of every participant.
Momentariness and Chronicity
MHNs insisted on the momentary aspect of the experience of people hospitalized in their unit. MHNs explained how PEMI’s experience was a difficulty that occurred at a given moment for them and characterized only this period of their lives. Their problem was not to be understood as characterizing their whole life, but rather as being situational.
What there is, it’s also, ultimately, us, we see people at a given moment in their lives, sometimes several times. At given moments in their lives. (Grace)
However, at the same time, MHNs also mentioned a certain chronicity in PEMI they met. MHNs acknowledged that a series of pathologies are cyclical or chronic. MHNs also acknowledged that the possibility of relapse exists, especially in the case of addiction. MHNs were concerned with PEMI who became inextricably entangled in their difficulties to the point of not being able to get out of them 1 day, which for MHNs was a sign of a kind of therapeutic failure.
So, when it goes on for a long time, the risk. . . is that we keep people with us for too long. And we arrive. . . Well, that, that. . . How can I put it? . . . Uh. . . If we keep them too long, they may become chronic and say to themselves that hospitalization will solve everything, and they won’t be able to leave, and the longer they stay, the more complicated it is to leave. (Janet)
Externality and Internality
MHNs emphasized the externality of the diseases. What happened to PEMI was due to a combination of circumstances—a life course, an event—more than to an inherent characteristic of their person or because of an element of their nature. This is evident in the way Anna attributes mental illness to common problems in life:
But normally there is always a problem behind it, a problem that makes one. . . be more like that [sub-vocal].
Hmhm. And the kind of problem behind it, what do you think it is?
Hm. . .. I don’t know, the problem is. . . it’s that, it’s, it’s, the problem is that. . . for me, decompensating. Or having problems in the family, or at work, or. . . Or in life, I don’t know, money too.
There are things that happen in their life story and it makes that. . .
that at some point it doesn’t go well anymore.
On the other hand, MHNs also referred to the internal aspect of mental illness. Mental illness was presented as intertwined with the internal processes of the people affected by it.
For, the layman, I say, the real fools. That it’s. . . there’s no, when I say that, there’s no. . . there’s no. . . there’s no criticism, you know. The, people are, well, they’re sick, they’re sick. That’s it, that’s. . . they’re like that. [Silence]. (Grace)
Seeing mental illness as internal led to the reasoning that PEMI sometimes have some responsibility for their disease.
Similarity and Dissimilarity
MHNs emphasized the similarity between themselves and the PEMI they encountered. MHNs’ message was that people psychiatrically hospitalized are ordinary, normal people and what happened to them could just as easily happen to anyone else, even to MHNs. The differentiation “them-us” was not relevant for MHNs because there was no qualitative difference between people who were hospitalized and those who were not. The only differences were quantitative, in the intensity of emotions or symptoms.
I mean, I could be in their place! I say people because. . . There, I tell myself at times that, yes, I, I might need this kind of help. Because. . . Because life is not, is not easy for anyone. Because sometimes we have greater fragilities at certain times. That’s the point. (Grace)
MHNs added the nuance that the similarity they emphasized between themselves and PEMI they work with corresponded for some of them, but not all of them. For MHNs, it was sometimes impossible not to notice the marked difference between themselves and some of the PEMI they work with.
Neither in the. . . in the formulations they use, nor even sometimes in the. . . in the suffering that brings them to the hospital, sometimes there are, there are things that are completely beyond us. And I, I think it’s part of my job, too, to be able to admit to myself, that it’s. . . Well. That, that what this person is going through, uh, probably I’ll, I’ll never go through it. And in a way that’s lucky for me, because it looks horrible. And, and to be able to tell me also that, no, here it is, I, I don’t understand, I don’t understand. . . the degree of suffering but that. . . well, if he’s there, it’s because he needs help. (Grace)
Individuality and Categorization
MHNs accentuated the individuality they attached to each PEMI they encountered. PEMI were seen, each time, as unique people with their own life history who had to be taken care of and considered in their singularity. It was important for MHNs to consider PEMI they met in their entirety rather than through the prism of what brought them to the hospital, and to take an interest in their history. MHNs took a stance against categorizing PEMI they worked with, for fear of locking them into a label. MHNs refused any generalizations and accentuated inter-individual differences within the same pathology.
I mean. It’s not first of all people who come with an illness, but it’s first of all, first of all people who come with. . . a history, a family, and then at some point they have problems . . . For me, it’s first of all, first of all people with whom it is, with whom it is, it’s important to, to talk, to find out, not just who brings them, not just. . . the fact that they are completely delusional, or completely suicidal but. What happened before? Where did they come from? What were their parents like? What did they do at school? Did they study? Are they married? Do they have children? Do they see their children? Do they see their parents? . . . But it’s not, it’s not a bogus question either. Because it’s, it’s really important to know that. Who are the people who come to us and, and why, and how. (Grace)
On the other hand, categorizations sometimes emerged in MHNs’ discourse. This phenomenon of categorization necessarily occurred by dint of encountering many more or less (dis)similar situations, and categories emerged according to the diagnosis, the patients’ likeability, the possible effectiveness of a therapeutic contract with them, the potential workload associated with them, their age, and so forth.
The only, hem, word that I think I hear, but more from my colleagues, or that might come up a bit, in my unit, is “it’s a shit-sit” [It’s a shitty situation], which is the word that I would use to describe patients for whom we know that care is going to be more difficult, either because care is going to be long. For example, patients who are difficult to transfer, whom their return home are going to be complicated, either because there are a lot of associated somatic pathologies, or because there’s going to be agitation and that’s going to require a lot of nursing work. (Elliott)
These categories included also people experiencing psychosis, people experiencing alcohol consumption issues, people experiencing depression, people “whose hospitalization was useless,” the discreet ones, the manipulators, and so on. These categorizations were not used explicitly as framework by MHNs to structure their understanding of the PEMI they work with, but a series of commonly used expressions and patterns were mentioned by MHNs during the interviews. Another paradox emerged here, as MHNs explicitly denied finding diagnoses useful for them, but they still used diagnoses to think about the PEMI they work with. These two opposing conceptions were simultaneously present and true for MHNs.
Humanization and Dehumanization
MHNs took a position that emphasized the human characteristics of the PEMI they work with: MHNs often talked about people and not patients, and they encouraged PEMI and others to recognize their humanity.
Yes, because. . . Well, just because they’re. . . sick doesn’t mean they’re not valuable. I mean. . . even if only in the eyes of the law, they have value. Because if they commit suicide, well, there’s an investigation, uh. . . I mean. So, they, they have. . . People have intrinsic value, after uh. . . the way they lead their lives. . . Pfff, I, I think, don’t take away this, this basic value. (Grace)
However, MHNs mentioned as well that the disease marks and sometimes dehumanizes those who are affected by it. MHNs recognized and named this phenomenon, even though they did not appreciate this fact, as presented in the quote below.
And so, yes, presenting someone as trash, that, uh. . . psychiatric patients or whatever, that, frankly, would never occur to me. [Silence]. But it’s true that there are some who have a. . . some patients who have a behavior that makes that [reaction of presenting them as trash]. That it causes that as a reaction. [Silence]. (Grace)
Agency and Disability
MHNs focused on PEMI’s remaining capacity for action and their resources. MHNs stated that everyone has skills and abilities that need to be considered: artistic sensitivity, relational skills, and the like. MHNs considered that the PEMI they work with retained their capacity for choice and remained adult and responsible, despite their suffering and the difficulties that might damage but not annihilate their free will. In addition, MHNs pointed out that PEMI have and develop a capacity to act on their illness: knowing and respecting their limits, knowing how to manage their emotions and asking for help. For MHNs, there was the possibility of progress and change in the face of the disease.
People’s ability to manage. Some people learn, huh. We’ve seen it in the course of hospitalizations in. . . in patients who return regularly. You can see that they learn. They learn to, to be able to say no, they learn to, to manage emotions, they learn to, to be able to react differently to frustration than by cutting themselves or banging into walls. Yes, it’s a learning process. (Grace)
At the same time, MHNs pointed out that the PEMI hospitalized in their wards needed help, which stemmed from the fact that their skills were affected by the disease. The disease was accompanied by a loss of agency, often through a process at the end of which people no longer knew how to do things on their own. It was because they were affected in their usual capacity to function that hospitalization became necessary. We explored this with Harriett in the following exchange:
Do some patients have a greater ability to influence their disease than others?
Yes, that’s for sure. That’s for sure. Um, well. . . Yes, but. You don’t see that a lot, because I think that once they have the ability to. . .. to, to act on their illness, as you say, we don’t see them, we don’t see them in hospital anymore. We see them when they are in crisis. And we teach them, we teach them, precisely, to be able to live with their illness. (Harriett)
Considering PEMI as a Whole, Paradoxes in the Meaning-Making
When MHNs considered PEMI as a whole, they presented paradoxes in their meaning-making, in the sense that conflicting dynamics appeared in their desire to convey their social representations about the PEMI they work with. On the one hand, MHNs had was a duty to undermine stigmatization and to normalize mental illness. They wanted to convey the message that mental illness is completely different from what people usually believe. MHNs seemed to convey the following message: “We know what it’s really like, and it has nothing to do with common representations about people experiencing mental illness.” MHNs were opposed to an essentialist conception of PEMI and in favor of an existentialist conception. They took the position of seeing mental illness as external, transitory and something that can happen to anyone, and wanted to avoid reducing to their illness the PEMI they work with. These representations were in line with MHNs’ injunctions regarding non-judgment and unconditional positive consideration as caregivers, and were at odds with the negative representations generally held by the public. It was particularly important for MHNs to transmit these representations during our interviews. MHNs wanted to convey that psychiatry is not as scary or terrible as people think. For example, Grace stated. “It’s not ‘One Flew Over the Cuckoo’s Nest’.”
Moreover, MHNs insisted on destigmatizing PEMI because they knew what it felt like to be stigmatized. When asked about the stigma they might experience themselves as MHNs, reactions were strong and immediate. They experienced stigma by association and implied: “We know what it’s like to be stigmatized, we are, too.”
On the other hand, MHNs also wanted to honestly report the reality they knew and present as many nuances as possible. MHNs knew that the positive representations on which they insisted on were not always true and were associated with counterexamples. They then expressed more nuanced representations toward PEMI as well. These nuanced representations were not explicitly claimed, as was the case for the positive representations, but were present in a more implicit way, as evoked in passing and accompanied by manifestations of discomfort. This seemed to reflect a certain reluctance on the part of MHNs to evoke more negative representations, although MHNs still evoked them in order to paint a complete and honest picture.
It was important for MHNs to convey both, positive representations and their nuanced counterparts. A necessary paradox was therefore present in their speech, as MHNs sometimes made contradictory statements in which they stated two apparently contradictory elements without seeming to realize it. MHNs also sometimes made ambivalent statements in which they stated two apparently contradictory elements while insisting both were true (e.g., PEMI being similar and dissimilar to themselves).
MHNs’ discourse was accompanied by a series of verbal tics, especially during the mention of their more nuanced and implicit representations, such as: cautionary phrasing such as the frequent use of conditional instead of present tense, multiple hesitations, multiple repetitions, self-deprecatory comments, difficulty in naming and word-finding difficulty. These verbal tics can be found in the verbatims presented throughout the results section, which have therefore been reproduced in such a way as to reflect as faithfully as possible the form of expression of the MHNs. MHNs also presented dissonant emotions such as forced laughter or asserting that they felt no fear while also reporting instances of aggression from PEMI. Where MHNs presented themselves as comfortable while conveying the first layer of positive representations, they presented themselves as less comfortable about expressing the second layer of more nuanced representations. Moreover, these language tics revealed MHNs’ permanent efforts to hold their paradoxical representations together, as MHNs were caught between two opposed positions dialectically responding to each other and experienced uneasiness while doing so.
Considering PEMI Individually, Some Paradoxes in the Meanings and the Meaning-Making
When MHNs considered PEMI they work with from an individual point of view, they described them mostly in a coherent and homogeneous way. There was no sign of paradoxical representations in their discourse. Their countertransference-based feelings displayed toward these PEMI could be positive, negative, or neutral, and MHNs did not show signs of uneasiness about it.
However, some PEMI generated paradoxical representations and feelings among MHNs. These PEMI crystallized opposed social representations: these same PEMI were simultaneously described as being capable and incapable of change; coping with their problems was simultaneously described as being both a matter of will and the converse. These shifting representations concerned more particularly the aspects of possibility of change and responsibility for change. Moreover, MHNs showed signs of uneasiness and internal conflict in relation to these PEMI. They attempted to cancel out retroactively the emotions experienced, appearing to say: “I’m not supposed to feel like this.” They also displayed tensions between their emotions felt and their prescribed emotions, as if saying: “what I should feel about this patient is not what I actually feel.” MHNs were simultaneously willing and unwilling to invest in the therapeutic relationship with these PEMI. These countertransference-based feelings were associated with psychic discomfort, as indicated through the type of verbal tics described in the previous section (e.g., cautious phrasing and expression of dissonant feelings). These contradictions in their social representations emerged from the analysis without seeming to be conscious on the part of MHNs, even though uneasiness was particularly expressed when evoking these PEMI.
These patients, they come back, often. And so it’s nice on the one hand [searching for her words] to see how they have evolved, that they have realized that when they are confronted with alcohol outside, well, in fact they are not yet strong enough, so uh. . . they come back to consolidate this, or to do an aftercare afterwards, so it takes several months uh. . . to launch this kind of project. Uh. . . But, it’s quite discouraging too. As I was saying. . . there is, well, I think of one patient in particular, it’s been at least 9, 10 times that he comes back . . . It’s, I think it’s one of the, of the pathologies that. . . where, where, yes, it’s more
Some PEMI generated a contradiction not within MHNs themselves but between them, within the team. The social representations and especially the countertransference-based feelings associated with them differed strongly between MHNs. This generated dissension in the team.
For example, with the person who cuts himself. . . well, I have a, I mean, I have colleagues who will just give band-aids to the patient, I, I’ll do the bandage myself. [Silence] . . . for example, if I feel in the interview, while doing the bandage, all that, that the patient wants to start all over again and is not at all relieved by her, by her act or what, yes, I will lead her to isolation to protect her from herself. But if what she is doing most of the time is saying “I feel much better” I will just take what is. . . harmful back from her room but I will leave her in her room. Because I don’t see the point of. . . to make an extra stress by putting her in solitary isolation, I mean, that’s it. Whereas there are some of my colleagues who would automatically put her in isolation or who, uh. . . wouldn’t even take the cutting tools because at some point there, it’s still the responsibility of. . . of what she can or cannot do, I mean. (Maddy)
When considering PEMI from an individual perspective, MHNs expressed paradoxical representations and feelings for some of them, whether this concerned the representations of a particular MHN or whether it was manifested within the team itself.
Discussion
Through inductive qualitative research guided by interpretative phenomenological analysis, we sought to explore and to understand more precisely the social representations held by MHNs through investigating their lived experience as care workers, examining what they say, how they say it and the feelings they express. We were able to highlight the uncertainty of MHNs’ representations within a shifting environment in which they emphasized non-judgment and non-categorization. In this context, it was difficult for MHNs to assert a clear and stated shared framework of representations. Paradoxical representations emerged among our participants, with explicitly positive representations, on the one hand, and more nuanced implicit representations, on the other hand, when MHNs consider PEMI as a whole. MHNs were caught between two movements. On the one hand, they wanted to deny the stigma that they knew was attached to PEMI and of which they were also the target (stigma by association; Ben Natan et al., 2015; Waddell et al., 2020). On the other hand, they supported their concern for experiential honesty, wanting to present the most accurate and nuanced possible representations of PEMI. When MHNs considered PEMI from an individual point of view, some PEMI elicited simultaneously paradoxical representations that particularly concerned PEMI’s responsibility for entering into and getting out of their difficulties. Faced with this observation of paradoxical representations that emerged from the discourse of our participants, we propose here different reflections in order to understand the presence of these representations, with the support of the literature.
First, our findings are consistent with the research conducted with PEMI and their relatives: their representations are also marked by uncertainty, and they tend not to define diagnoses as central in their conception of mental illness (Foster, 2003). Residents in community mental health centers also report complex and contradictory lived experiences and feelings (Bengtsson-Tops et al., 2014). In contrast to other fields, the representations of professionals in the field of mental health are characterized by their heterogeneity and uncertainty: there is no strong consensus among experts on the definition of mental illnesses and on the ways in which they should be treated (Morant, 2006). On the other hand, the public’s representations are marked by their certainty and homogeneity over time and across cultures (Angermeyer & Schomerus, 2017). Our results show that MHNs’ representations appear closer to those held by PEMI and their relatives than to those of the public and somatic health care professionals.
Mental health professionals then find themselves at the interface between the public and expert theorists, and are thus forced to navigate between theoretical norms that are sometimes in contradiction with each other and lay representations that are opposed to them. Situated at this crossroads, they must constantly synthesize contradictory elements. This has also been confirmed in other studies, which have shown how mental health professionals’ work involves a constant management of the ambiguity and contradictions that emerge from it (Chambers et al., 2015; Morant, 2006). In our study as well, which considers the diverse and shifting environment of the ward, the structuring of MHNs’ representations attached to their work reflects these paradoxical features. It is worth noting that the contradictions reported so far in the literature, which involve attitudes that are sometimes positive and sometimes negative attitudes, may reflect the reality: uncertainty and paradoxes are part of the lived experience generated by the context of mental illness.
Second, cognitive dissonance is a type of psychic discomfort emerging from the presence of inconsistent representations (Fointiat, 2013). In our research, we noticed several signs of psychic discomfort, including expressions of uneasiness, uncertainty, verbal tics and conflicted feelings toward some PEMI that MHNs work with. Our study identified inconsistent representations in the form of MHNs’ paradoxical representations in implicit and explicit layers. Moreover, there was dissonance between MHNs’ non-judgmental standards as care workers and their concern to depict a genuine representation of reality. Researches show that cognitive dissonance is accompanied by attempts to reduce it (Fointiat, 2013). In our research, we observed that MHNs displayed verbal tics, contradictory statements and ambivalent statements. These showed MHNs’ persistent efforts to hold their paradoxical representations together and to keep their more nuanced representations implicit. These different elements found in our research argue for the presence of cognitive dissonance in the MHNs we met. Schulze’s (2007) work highlighted that mental health professionals are simultaneously stigmatizing, stigmatized and destigmatizing agents. This triad highlighted by Schulze’s work is also reflected in our results: MHNs are keen to play an active role in denying stigma (destigmatizing), particularly as they are also targets of the stigma experienced by PEMI (stigmatized by association) (Ben Natan et al., 2015; Waddell et al., 2020), while themselves holding representations that are not always conducive to destigmatizing (stigmatizing). The simultaneous presence of these different roles is a driver of cognitive dissonance. These different observations lead us to suggest that MHNs are in a state of cognitive dissonance. It is a lens that would explain the presence of the contradictory findings found so far in the literature.
It is noteworthy that the most marked moments of dissonance concerned some PEMI for whom paradoxical representations were evoked at an individual level. These PEMI generated particular discomfort that was expressed with more pronounced verbal tics. These paradoxical representations were particularly concerned with issues regarding these PEMI’s responsibility for the appearance and disappearance of their difficulties. A parallel can be drawn with the beliefs held by the public about PEMI’s responsibility for the appearance of their illness (onset responsibility) and for overcoming their illness or having it continue (offset responsibility). These beliefs are pointed to as the main and most investigated dimensions accounting for stigma toward PEMI in the literature (Corrigan et al., 2003; Johnson-Kwochka et al., 2021; Schomerus et al., 2014). While for the majority of PEMI, MHNs’ representations appear close to those of PEMI and their relatives, MHNs’ representations share greater similarities to those of the public with regard to some specific PEMI, to whom the most paradoxical representations are attached and who generate the greatest discomfort for MHNs.
Third, we suggest the following reasoning for the building up of such paradoxical representations as those presented by MHNs. It should be remembered that people develop a representation of mental illness early in their social life (Henderson et al., 2014; Link & Stuart, 2017). MHNs have necessarily forged attitudes as members of the public before their professional careers begin (Henderson et al., 2014). We are wondering if the implicit representations found in our results, some of which share similarities with those of the public or of somatic care workers, may be traces of the first representations MHNs forged. In addition to the representations of illness forged as lay people, training as mental health professionals and prolonged contact with patients leads to the formation of different representations, marked by the values of non-judgment and non-categorization (Rogers, 2001). We are wondering if the paradoxes in MHNs’ representations could emerge from the tension between the representations they forged as members of the public and the new ones emerging from their professional identity. This could be another way of understanding the presence of paradoxical representations and could be further documented through longitudinal studies.
Strengths and Limitations of the Study
The use of qualitative methods and of social representations framework allowed in-depth analysis that complemented the existing studies in the stigma literature. It allowed us to reach a better understanding of the already identified contradictions in earlier research. Our research shows that the contradictions emerging thus far in MHNs’ representations from one study to another appear so because paradoxes are at the heart of those representations. Paradoxes are intrinsically part of MHNs’ lived experience, with regard to both their representations of PEMI and the principles they have internalized, as MHNs are keen to be simultaneously non-judgmental and particularly honest.
A first limitation of our study is that it relied on a broad interview guide. The literature questioning the reason for the contradiction in the stigma literature is very limited. To address the issue of contradiction, we opted for an inductive approach with broad questioning, without knowing that one of the main paths toward understanding was this double-layered implicit and explicit structure. Another limitation of our study is that some MHNs declined to participate in our study without saying why they declined, who could have presented a different tone in response to our research question, and whose responses could have generated divergent themes.
Relevance to Clinical Practice and Research
Understanding the content of social representations, their structuring and their meaning-making is a necessary step to support adaptation of MHNs’ clinical training and to improve clinical practice and well-being at work. It holds up a mirror to MHNs that reflects their representations, which may help with acknowledging their position while at work. It also points to directions for future studies.
First, MHNs’ representations of PEMI have a necessary impact on the way MHNs care for them. MHNs’ positive representations and destigmatizing position shown in our findings contribute to their effective patient care delivery. Actively considering PEMI as not responsible for what happened to them, but in the meantime considering PEMI as capable of changes and viewing each PEMI as individual and fundamentally human is essential as care-givers. It facilitates providing benevolent, non-judgmental, and empathetic care (Rogers, 2001). Moreover, it helps PEMI who usually present high self-stigma to consider themselves in the same positive manner (see, e.g., Martinez, 2014). Otherwise, the literature shows that endorsing essentialist beliefs (i.e., beliefs that the attributed characteristics are so by essence and are immutable) enhances the perception of differentness and the display of stigmatizing attitudes, while diminishing optimism about recovery and perceived personal responsibility for the onset of illness (Howell et al., 2011). In our findings, MHNs supporting an existentialist view of PEMI (i.e., beliefs that the attributed characteristics are so by experience and are mutable) should then operate within a destigmatizing and optimistic dynamic, but could also perceive greater personal responsibility. And research among the public shows that believing in PEMI’s responsibility for their difficulties leads to anger, decreased pity and lowered propensity to help (Corrigan et al., 2003). MHNs’ paradoxical representations may then well have a paradoxical impact on clinical practices. Further research is needed to understand the paradoxical representations MHNs work within, to investigate their impact on clinical practices and to help MHNs deal with the complexity that arises from them.
Second, thanks to our qualitative approach, we have hints of the existence of implicit representations that could affect interactions and interventions by MHNs. Studies on implicit representations have highlighted that they are more likely to be negative representations, which is similar to the dynamics we find in our data. Implicit representations are also found to be more predictive of behavioral responses compared to explicit ones (Brener et al., 2013; Stull et al., 2013) or to be predictive of involuntary or automatic actions (Asendorpf et al., 2002). Some studies have found that the relation between implicit and explicit representations is weak, suggesting that they are supported by unconnected paths (Kopera et al., 2015; Monteith & Pettit, 2011; Peris et al., 2008; Teachman et al., 2006). Future research should allocate resources to better understand the implicit representations held by MHNs.
Third, our findings raise attention to the uncertainty, dissonant positions and inner conflict experienced by MHNs. Dissonances in positions and emotions felt was shown to be related to burnout and compassion fatigue (Andela et al., 2016; Barnett et al., 2022). In order to promote wellbeing at work for MHNs, the awareness raised by our research calls for the development of targeted interventions addressing the management of the dissonances MHNs experience in their workplace.
Fourth, our results raise questions about how MHNs’ representations may evolve during their training, when their representations pass from lay to mental health professionals’ representations. This could be another entry point for understanding the presence of paradoxical representations among MHNs, especially by means of longitudinal studies.
Conclusion
Our study examined MHNs’ perspective about PEMI, using the social representation framework and qualitative methods rather than the stigma framework and quantitative methods. Our analysis allowed us to ascertain that MHNs’ social representations of the PEMI they encountered were characterized by paradoxes at two levels. In terms of the meaning of their representations, MHNs associated positive representations with PEMI from an explicit point of view, while nuancing them in the opposite direction from an implicit point of view. In terms of the meaning-making of their representations, MHNs presented conflicting dynamics, on the one hand displaying non-judgment and normalization of mental illness, and on the other hand offering contradictory counterexamples to paint the most honest and complete picture possible. MHNs’ speech was peppered with verbal tics conveying their uneasiness while doing so, and displayed the effort involved in trying to maintain these paradoxical representations and dynamics together. We propose the concept of cognitive dissonance as a lens for making sense of these results.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The first author benefited from a Faculty Assistant Mandate from the UCLouvain.