
Abstract
BACKGROUND:
The life expectancy of patients with severe mental illness (SMI) is estimated to be 20 to 30 years shorter than in the general population due to avoidable physical illnesses. This gap is widening. Health care professionals’ performance with regard to physical health and lifestyle appears to be suboptimal.
AIMS:
The purpose of this study is to formulate recommendations to enhance physical care for patients with an SMI.
METHODS:
A generic descriptive qualitative study was conducted. Fifteen mental health nurses (MHNs) working in community mental health care in the Netherlands were interviewed. Thematic analysis of the data was performed.
RESULTS:
Most MHNs perceived physical screening and lifestyle interventions to be an important part of their professional role. However, they recognize discrepancy between their perception and actual practice. Most MHNs focus in particular on the psychiatric illness and its consequences for daily living, and they defined the provision of physical health care as a secondary concern. Participants described building a therapeutic relationship as a crucial, however, difficult part of the process of working on physical health promotion. Many MHNs tend to formulate goals and necessary behavioral changes on behalf of their patients, rather than helping them formulate their own goals and activities for themselves.
CONCLUSIONS:
Building a good therapeutic relationship with patients and supporting patients in defining their own lifestyle goals can enhance nursing physical care. Support by other team members (such as NPs) and managers is needed. In training and education for professionals, the lessons learned in this study should be included.
Introduction
People with severe mental illness (SMI) have a high prevalence of physical morbidity and a life expectancy estimated to be 20 to 30 years shorter than the general population (Walker et al., 2015). Despite the need for effective care that aims to improve their physical health, the care currently provided by mental health professionals is still suboptimal (De Hert et al., 2011; Firth et al., 2019).
Background
People with SMI such as schizophrenia, bipolar disorder, and major depression have high physical morbidity rates, poor life expectancies, and decreased health-related quality of life (Walker et al., 2015). Their life expectancy is estimated to be 20 to 30 years shorter than in the general population (De Hert et al., 2011), and this gap is widening (Hayes et al., 2017). Approximately 60% of these premature deaths are due to physical illnesses such as cardiovascular disease, diabetes, respiratory diseases, and certain types of cancer (Laursen et al., 2014). These patients’ poor physical health status is related to a complex range of factors that includes genetic factors, the symptoms of the mental illness, the side effects of psychotropic medication, an unhealthy lifestyle (smoking, sedentary lifestyle, poor nutrition, substance abuse, and unsafe sex); stigma (by health professionals); poor access to health services; and socio-economic factors such as poverty (De Hert et al., 2011; Firth et al., 2019).
Broad evidence suggests health care professionals’ performance with regard to physical health and lifestyle to be suboptimal. Accessibility as well as quality of medical care offered to patients with SMI are low (Firth et al., 2019). Stigmatization of patients with SMI by care providers is not a rare phenomenon. In a process known as diagnostic overshadowing, patients’ somatic symptoms are often attributed to the psychiatric disorder, which in turn leads to inappropriate treatment (Firth et al., 2019). To reduce morbidity rates in these patients, and to increase their life-expectancy and quality of life, health care professionals should support them in recognizing their physical problems, seeking appropriate help, and promoting multiple, effective healthy lifestyle behaviors (Firth et al., 2019).
In recent years, several guidelines have been developed, to enable health care professionals to provide adequate physical screening and lifestyle coaching for patients with SMI (Meeuwissen et al., 2015a, 2015b; NICE 2014a, 2014bb). These guidelines strongly emphasize the central role of mental health nurses (MHNs) in somatic screening and promoting healthy lifestyle behaviors. In their proximity to the patient, MHNs have the opportunity to regularly perform standardized somatic screenings, leading to early detection of physical disorders, and appropriate referral for somatic treatment. Also, as part of the screening activities, unhealthy lifestyle behaviors can be identified, which form the basis for individualized lifestyle advices and support (van Meijel et al., 2015). Happell et al. (2013) found in a qualitative study that although MHNs recognize their responsibility with respect to the physical health of patients with SMI, they see few practical possibilities for performing this. This is mainly due to factors such as staff shortages and also because they lack the knowledge to perform these screening activities properly (Happell et al., 2013). Blythe and White (2012) confirm that MHNs lack knowledge and practical skills regarding physical health promotion and that they should receive training and practical support. The same authors also stated that MHNs need a positive and more optimistic attitude toward promoting physical health in patients with SMI, in order to increase their perceived responsibility and actual activities with respect to patients’ physical health (Blythe & White, 2012).
Little is currently known about how MHNs perceive their role regarding physical health for patients with SMI and how these perceptions influence their actual practice. Profounder understanding of these issues would be likely to contribute to the development of effective training programs for MHNs, and eventually—with MHNs in a key role—to the successful implementation of physical health-promoting interventions.
Objective
The aim of this study was to establish (1) how MHNs working in community mental health care settings in the Netherlands perceive their roles with regard to physical screening and lifestyle coaching for patients with SMI and (2) how they perceive their actual performance concerning these roles.
Method
Design
For this study, we chose a generic descriptive qualitative design (Kahlke, 2014), being appropriate to our aim of describing MHNs perception of their role and role performance regarding somatic screening and lifestyle promotion in patient with SMI.
Settings
This study was performed in community mental health care teams organized as Flexible Assertive Community Treatment (FACT) teams, a Dutch variation on the internationally known Assertive Community Treatment teams (ACT teams) (Van Veldhuizen, 2007).
The original ACT teams deliver long-term high-intensive treatment to the most severely mental ill patients in the community. They provide treatment to about 20% of the patients with SMI in a given region. FACT teams, in contrast, provide treatment to all patients with SMI in a region. According to a patient’s mental health status, teams vary the intensity of ambulatory treatment. Most FACT teams consist of a psychiatrist, a psychologist, MHNs, a nurse practitioner (NP), social workers, a vocational worker, and an expert-by-experience (FACT Nederland, 2015).
Participants
We applied convenience and purposive sampling to achieve maximum variation in our sample (Kahlke, 2014). We interviewed 15 MHNs, who never received advanced training with respect to physical screening or lifestyle interventions, from four mental health organizations that covered six cities and their surrounding regions. MHNs volunteered to participate, after being invited by their manager. Maximum variation in the sample was sought with respect to work experience in mental health care, work experience in a FACT team, and level of education. To list their background characteristics, MHNs received a short questionnaire before the interview.
After 13 interviews and intermediate analyses of the data, the research group concluded that, so far, all MHNs interviewed perceived their performance regarding physical screening and lifestyle coaching to be suboptimal. To obtain a more comprehensive picture of the MHNs’ perceptions, more information was needed from MHNs who considered themselves successful in their role. We therefore used negative case analysis and selected two MHNs who had received additional training on the subject and had systematic ways of performing physical screening and lifestyle coaching.
Data Collection
All interviews were conducted by the second author (N.K.), between March and May 2016. These interviews were semistructured using a topic list based on the literature on MHNs’ perceptions of their role in screening and lifestyle interventions (Table 1). Each interview started by asking MHNs to describe their overall perception of physical screening and lifestyle coaching for patients with SMI. The topic list was used as a guide during the interviews. All interviews took place in the participants’ offices. They were audio-recorded and transcribed verbatim.
Topic List.
Note. MHNs = mental health nurses; SMI = severe mental illness.
Data Analysis
Data were analyzed using Thematic Analysis with the Nvivo 11.0 program, following the six steps described by Braun and Clarke (2006). Data analysis started by transcribing the audio files of the interviews verbatim (a). The researcher read and re-read the interview, assigning initial in vivo codes to the text (b). Three interviews were analyzed separately by three researchers. The first draft of potential themes that emerged from the initial in vivo codes was then elaborated (c). Next, after the research group had discussed the codes and emerging themes, a first draft of themes was compiled (d). To assign relevant data to the themes, all interviews were reread. When all data had been assigned to the themes, the researcher checked whether each theme consisted of enough data to support it. (e). Finally, another research meeting was conducted to discuss and reach consensus on the final themes (f).
Trustworthiness
The trustworthiness of the study was improved by applying the following criteria (Lincoln & Guba, 1985). To improve credibility, we used member-checking and negative case analysis. Member-checking consisted of asking the participants to comment on the researcher’s summary of the preliminary analyses and interpretations. To improve dependability and confirmability, an audit trail was conducted whereby the raw data and memos generated during the study were saved in a logbook. Confirmability was also improved by using reflexivity, which involved writing reflective notes after each interview and by thick description. Supervisors, co-authors, and peer-students gave the interviewer feedback on her interview techniques. Data-analysis of three interviews was performed independently by three researchers. Differences were discussed until consensus was reached.
Ethical Considerations
This study followed the ethical principles of the Declaration of Helsinki (World Medical Association, 2013). The scientific committees of the four participant mental health organizations gave their permission to conduct the study in these organizations. Before the interviews, an informed consent form was signed by the MHN and the researcher.
Results
A total of 75 MHNs were invited to participate in this study. Eighteen MHNs expressed their willingness to participate, of whom 13 eventually made an appointment with the interviewer. Later, two more MHNs were included through purposive sampling. Their characteristics are presented in Table 2.
Characteristics of Participating Nurses.
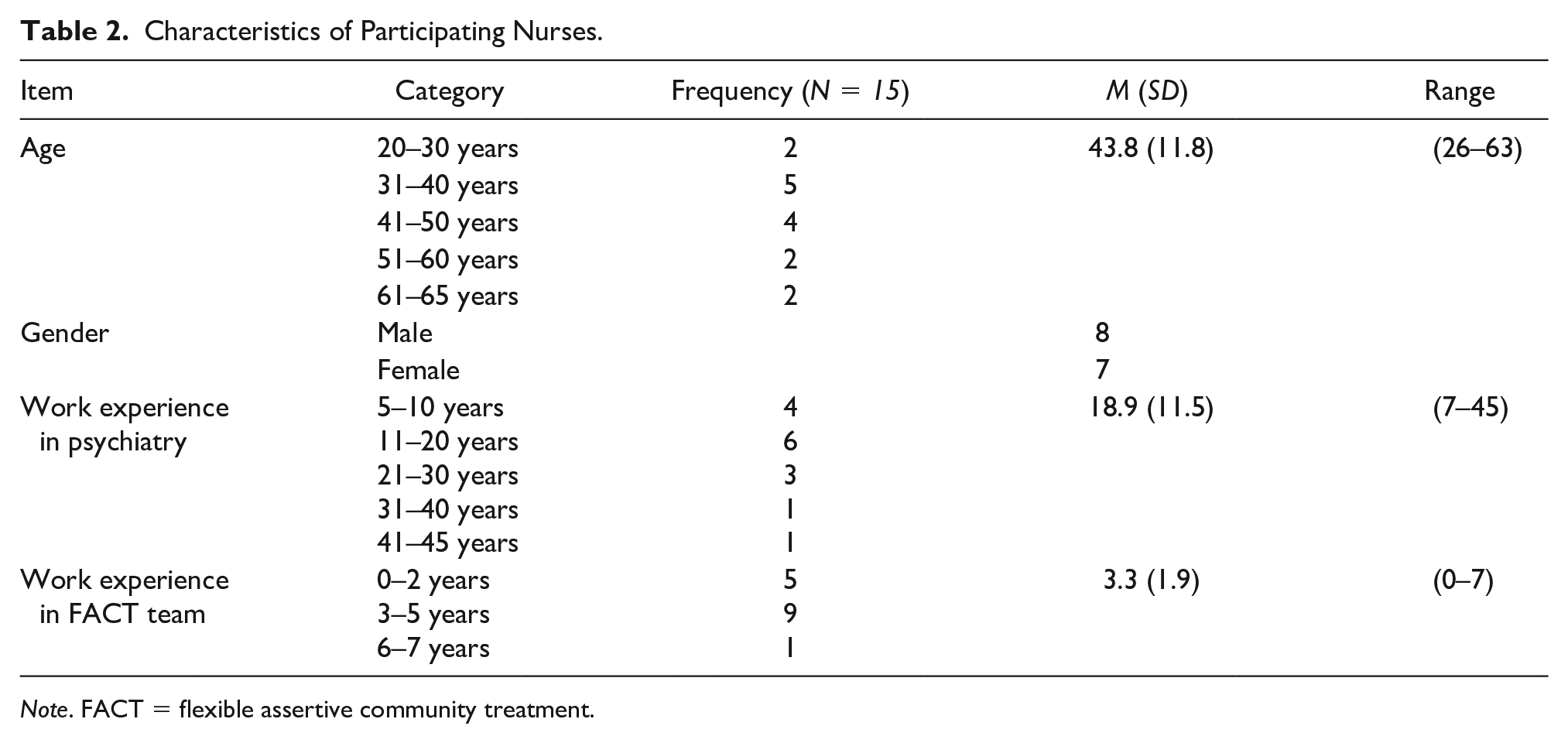
Note. FACT = flexible assertive community treatment.
Of the 13 MHNs initially interviewed, all but two perceived performing activities on physical screening and lifestyle coaching a regular part of their professional role. However, the data revealed a significant discrepancy between what MHNs thought they should do with respect to physical care for patients with SMI, and what they were actually doing. The participants named several factors that contributed to this discrepancy. In the following sections, the results of our study will be described, presenting three themes. First the MHNs’ perceptions of what should be done; second, their perceptions of what they actually did were described; and third, we elaborated on the barriers the MHNs perceived.
What MHNs Believe Should be Done
Most MHNs commented that, for optimal quality of care for patients with SMI, physical care and psychiatric care should be integrated within mental health care practice. They emphasized the leading role that MHNs could fulfill with regard to physical screening and lifestyle coaching. Two MHNs felt no responsibility for performing activities in these areas, which they felt were unimportant, and for which they stressed their lack of time and expertise. And although the majority of the participants stated lifestyle coaching was important, somatic screening was the most dominant aspect of physical health care they referred to during the interviews.
MHNs stated that organization and coordination of physical health care for patients with SMI is important and much profit can be gained here. Some interviewees felt that MHNs could fulfill a coordinating and advocacy role on patients’ behalf. For example, if patients had difficulty in keeping appointments with other health care professionals, the MHN could help them remember them, and could also accompany them to the appointments. Most MHNs in our study were willing to fulfill such a role. Regarding the organization of physical health care, one MHN described the possibility of appointing nurses to the team who were expert in physical health care and who could also coach the other MHNs: “You could make two nurses in a team responsible for the somatic screenings. They’re the ones who handle everything to do with somatic screening, and they could coach other nurses in how to do it” (Male, 26 years old). However, other MHNs preferred to perform the somatic screening themselves, due to their good relationship with patients, which provided opportunities to signal specific health risks and to monitor follow-up activities.
Current Practice
Even though most MHNs were interested in the physical health of this patient group and also in the responsibilities they believed to be involved, they emphasized that their primary focus lay on their patients’ psychiatric problems and its consequences for daily living. If there was time left in their busy daily schedules, they sometimes might undertake activities involving somatic screening and lifestyle coaching. In clear terms, most MHNs thus appeared to define the provision of physical health care as a secondary concern.
Signaling potential physical health risks for patients was one of the activities they stated to actually perform. They did so by somatic screening or by paying close attention to potential risk behaviors—such as poor dietary habits or excessive smoking—during home-visits. When risks were observed, MHNs responded mainly by giving advice, for example by telling a patient that it was healthier to drink diet soda as it contains less sugar. Some MHNs reported that they had been trained in motivational interviewing techniques, which they said to use when addressing lifestyle issues. However, due largely to their own lack of competencies to respond adequately to these physical health problems, all MHNs stated that one of their principal actions in such cases was to refer patients to other health care professionals, such as a general practitioner (GP), dietician, or physiotherapist: “What I often do—when someone is obese, for instance—is to refer him to a physiotherapist to start losing weight. If necessary, I can accompany him once or twice if that’s what he needs to get something done.” (Male, 39 years old).
Other MHNs mentioned the valuable role of the NP with respect to somatic screening and subsequent treatment. According to the interviewees, NPs have had a thorough training, and they generally have great skills in somatic screening and interpreting the results. When NPs were involved, screening tended to be followed up often. MHN also found the NPs to be easily accessible for consultation and advice. In some settings, the NP or GP was officially made responsible for the patients’ physical health care, thereby relieving the MHNs of the responsibility for it. Some MHNs approved of this, as it made matters clear for patients. In such cases, the MHNs’ responsibility was limited to promoting patients’ compliance with appointments with the NP or GP.
A few MHNs stated that they involved the patients’ informal caregiver or caregivers in physical health care, particularly with respect to motivating patients to get screened, to taking action in changing their lifestyle, and to accompanying them to appointments with other health care professionals.
A major problem in the MHNs’ view was the fact that somatic screening was often not followed up, which meant that the physical health problems assessed were not adequately treated. Similarly, MHNs stated that patients were often placed in a passive role with respect to their own physical health. For example, if lifestyle goals were formulated, they were usually formulated by the MHN, who should instead have helped patients to set their goals for themselves. Neither were the lifestyle goals generally operationalized in specific terms, which impeded the formulation of concrete activities and reduced the opportunities for evaluating them.
The two MHNs with additional training (i.e., the negative cases) stated that it was essential to support a patient in making his own goals—and that this was one of the most difficult parts of the whole process.
Yes, and that’s a real challenge. It’s not easy—you have to make the goals very specific, in accordance with the patient’s preferences. And that can be very challenging, as patients aren’t usually really specific. But you want them to set their own goals . . . (Male, 60 years old)
In their opinion, it was crucial for patients to establish their own goals and for MHNs to support them in specifying them in the form of small, clear goals that they could actually achieve within the foreseeable future.
The following description of the barriers the interviewees perceived should thus be interpreted in the light of the statements above.
Barriers Perceived by MHNs
In conjunction with the preceding statements, the MHNs described some explicit barriers to somatic screening and lifestyle interventions. A primary concern was the lack of feasible protocols and tools in the setting in which they worked. In their view, this led to suboptimal practices that were not theoretically underpinned: “No, we don’t have protocols that tell us to follow certain steps . . . you have to learn from experience what works and what doesn’t.” (Female, 53 years old).
Another barrier was related to the involvement of informal caregivers. However, some MHNs involved a patient’s informal caregivers in a more or less systematic way, others did not. Some MHNs simply “forgot” to involve them; others perceived too many barriers—such as pessimism or lack of knowledge on the part of the informal caregivers—and had therefore come to believe that these caregivers could not contribute adequately to enhancing the patients’ health: “Yes, we try to include family members . . . we try to involve them in the lifestyle changes, but usually they respond by saying, ‘We’ve told [the patient] to stop that behavior so many times before, but he just doesn’t listen.’ That’s what they’ll fob you off with” (Male, 63 years old).
Other barriers to performing somatic screening and lifestyle coaching were attributed to the patient and the illness. The negative symptoms many patients suffered also reduced their initiative—which, in the views of the MHNs, made it hard to motivate them to participate in these activities. Various other barriers were identified by the MHNs: lack of financial resources (which made it difficult for patients to buy healthy food or to pay for membership of a sport club); lack of the social contacts patients needed to work with others on their lifestyle goals; low self-esteem, which led to withdrawal; not being properly able to recognize physical symptoms; and low compliance in visiting a doctor or dentist.
Sometimes it’s very exhausting to have to drag someone out of bed and into a car for a doctor’s appointment. It’s not just as if you just knock on his door, he gets into the car, and we drive over to the doctor’s. No, I have to knock on the door, wait till he opens it, walk over to his bed (where he is in again), pull the sheets off him. . . it’s not something you can do in an hour. (Female, 34 years old)
To make any progress, such factors meant that considerable time had to be invested. MHNs frequently referred to insufficient time for fully investing in somatic screening and lifestyle coaching. Another barrier the MHNs described was the fact that patients with SMI were not always taken seriously by other professionals. This led to inadequate treatment: Then they go to the GP, who sees a lot of diagnoses but doesn’t really respond properly to what the patient says. ‘Yes well, that’s too bad,’ they say, and that’s it . . . There are many reasons our patients live 20 years shorter . . . it’s not just the pills, it’s also because health care professionals don’t take them seriously. (Male, 32 years old).
The MHNs with additional training (i.e., the negative cases) stated that more patience and endurance were required to succeed with these patients. Rather than reporting a shortage of time, they stated that it was a matter of setting the right priorities. This was confirmed by one of the other MHNs: “Yes, well, I basically just don’t make time for it . . . maybe it’s just not that important to me” (Female, 29 years old).
Further exploration of the practices of the two trained MHNs revealed that they usually perceived barriers that were similar to those perceived by the other MHNs. A key difference was that they consistently prioritized issues of health promotion and lifestyle coaching. One of them explained that she addressed physical issues during every appointment with her patients in order to make it part of their routine. Both of these MHNs gave their patients explicit opportunities to talk about what worried them about their physical health status and any wishes they had in this regard. They stated that it was crucial to establish a good connection with patients: this helped them ask the questions they needed to gain insight into the problems the patients perceived and their preferences concerning their physical health. This also enabled them to set specific goals and agree tailored interventions. They emphasized the goals to be formulated in SMART terms: Specific, Measurable, Acceptable, Realistic, and Time-bound. One of the trained MHNs stressed the importance to establish realistic goals: if a patient was unable to reach a goal in a relatively short term, its formulation had been too ambitious: In my experience, the goals you set are often too big. Then, when you want to assess whether a patient has achieved it, things get complicated, because you set multiple steps within one goal . . . Yes, I think it’s very important for a goal to be SMART—then at least you can measure whether someone has achieved it’ (Male, 60 years old).
Both of these additionally trained MHNs stressed that the inability to establish SMART goals caused patients to lose their motivation to work on their goals.
In summary, most barriers were formulated in terms of the following: insufficient tools for somatic screening and lifestyle coaching; insufficient knowledge and skills; insufficient time; no involvement in physical health promotion by members of the social network; specific patient characteristics; stigmatizing attitudes and lack of interest on the part of mental health care professionals and other health care professionals; and problems with realistic goal-setting. Some MHNs felt that these barriers could be overcome by establishing a strong relationship with the patient, by consistently setting priorities regarding physical health promotion, and by helping patients to formulate attainable goals.
Discussion
Through in-depth interviews, this study shows that a majority of MHNs acknowledged their role in performing somatic screening and lifestyle coaching for patients with SMI. But there was a clear discrepancy between what most nurses thought they should do to promote physical health in these patients, and what they perceived they actually did. These findings are consistent with previous research (Happell et al., 2013).
Our finding that MHNs experienced various barriers to performing these duties is also consistent with other studies (Blythe & White, 2012; Bradshaw & Pedley, 2012; Happell et al., 2013; Robson et al., 2013). Evidence shows (Bartlem et al., 2018) that a majority of patients with SMI are interested in improving their lifestyle and in receiving support. As a result, it is not possible to find empirical substantiation for the belief of many mental health professionals that the majority of their patients lack motivation or the capacity to comply with interventions intended to improve their lifestyle.
A striking finding of our study was that some MHNs attributed patients’ failure to achieve lifestyle goals to SMI-related factors such as negative symptoms, use of psychotropic medication, and low self-esteem. It is particularly striking that the two experienced MHNs perceived these factors to be surmountable. These MHNs experienced that, despite existing barriers, positive outcomes could be reached by realistic goal-setting, tailored support, and perseverance. In contrast, if a professional combines a stigmatizing attitude with negative perceptions of patients’ capacity for behavioral change, this is a considerable barrier to physical health improvement in patients with SMI.
One factor was experienced to be crucial to the success of somatic screening and lifestyle coaching: establishing a good therapeutic relationship with the patient, which laid the basis for open communication on physical health concerns and opportunities for lifestyle changes and health promotion. Helping patients to formulate their personal, attainable goals was perceived as essential. The participants described this as a difficult part of the process of working on physical health promotion. One factor that may particularly impede the successful achievement of health improvements is the tendency of MHNs to formulate goals and necessary behavioral changes on behalf of their patients, rather than helping them formulate their own goals and activities for themselves. This is consistent with the phenomenon called “the righting reflex” by Rollnick et al. (2008) in motivational interviewing theory—something that should be a major point of consideration when training MHNs.
While this study provides valuable insight into MHNs’ perception of their role in promoting physical health in patients with SMI, four main limitations should also be considered. First, although 15 interviews were enough to provide preliminary insights into the MHNs’ perceptions, with more interviews data saturation would have been reached. Second, the study was conducted in so-called FACT teams in The Netherlands, a specific treatment modality for outpatients with SMI. Although there is increasing international interest in this treatment model, currently such teams exist in only a minority of western countries. As the specific content and context of treatment are important factors influencing role perceptions and actual practice, our results may be less generalizable to other countries and treatment settings. However, by describing the setting in our methods section, we provided insight into the treatment context in which the data were gathered. The third limitation is the sampling bias that occurred when participants were recruited: a total of 75 MHNs were invited to participate in this study, and 15 volunteered to participate. Our sample thus overrepresents MHNs who had affinity with the research subject and acknowledged their role in improving health outcomes. The fourth limitation, as these respondents may have made “socially desirable” statements during the interviews, our results may underestimate reality. In other words, MHNs may actually perform fewer activities related to physical health than this study states. Our study also had several strengths. To enhance the trustworthiness of our data, we used strategies such as member-checking and an audit trail. The addition of negative cases to the sample produced a different perspective on the phenomenon under study, which directed to successful elements of MHNs’ support regarding physical screening and lifestyle coaching.
Implications for Nursing Practice
The physical health status of patients with SMI gives rise to serious concern and requires sustainable efforts on the part of MHNs and other professionals to improve physical health outcomes. While a majority of the MHNs in this qualitative study perceived physical health promotion and lifestyle coaching to be part of their professional responsibility, they also perceived many barriers to optimal performance in this area. Even though most of the MHNs interviewed knew what they should do, this diverged significantly from what they actually did. Three factors appear to be crucial to enhance quality of physical care for patients with SMI: establishing a good connection with patients; staying close to the patients’ preferences by tailored and attainable goal setting; and sufficient organizational and peer support for the professionals involved. For effective somatic screening and lifestyle coaching, more methodical support by team members (such as NPs) and managers could be helpful. Moreover, the barriers explored here should be taken into consideration by those who develop training for professionals and health-promotion interventions for patients.
Footnotes
Acknowledgements
The authors thank the participants for sharing their experiences and opinions. They also thank the mental health nurses for their participation in this study.
Authorship Declaration
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Authorship Statement
All authors meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors and are in agreement with the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research project was financially supported by the Research Group Mental Health Nursing Research Group of Inholland University of Applied Sciences.