
Abstract
Hospital clowns are widely used in pediatric settings. However, the field of pain and pain experience in children is complex and multifaceted. Therefore, the aim of this study was to expand knowledge on the impact and influence of hospital clowns on 4 to 15-year-old children’s experiences of managing painful procedures and conditions. A convergent mixed method study was conducted integrating findings from three individual studies: a prospective non-blinded study and two focused ethnographic studies. The findings illuminated a child—clown interaction characterized by a close relationship evolving during a continuous, mutually focused attention, conceptualized as WE. This WE represent a responsive interaction between child and clown, which supported the child during the procedures, and generated three integrated findings: an age-differentiated approach; understanding the child’s condition; and previous experiences as a part of the child’s history. The WE approach strengthened the child’s competences and ability to manage during painful procedures.
Introduction
Hospitalized children of all ages experience a variety of potentially painful procedures and conditions during examinations, treatment, and care (Birnie et al., 2018). In particular needle related procedures (e.g., venipunctures) are found to be among the most painful procedures during hospitalization (Friedrichsdorf et al., 2015; Walther-Larsen et al., 2017). Literature reveals that children continually report undermanaged procedure related pain during hospitalization (Birnie et al., 2014; Friedrichsdorf et al., 2015; Walther-Larsen et al., 2017). Moreover, children experiencing repeated painful procedures and conditions are at special risk since memories of previous experiences play a crucial role in managing future painful events. Whereby children with previous experiences of under or untreated pain have increased risk of experiencing psychological negative consequences and lower pain threshold (McMurtry et al., 2015; Noel, Chambers, McGrath, et al., 2012; Noel, Chambers, Petter, et al., 2012), that might affect the child’s response of pain negatively and influence their future health related help seeking behavior and health (Birnie et al., 2018). Hence, in managing procedural treatment and care-related pain in hospitalized children, there is an urgent need to reduce the experiences of pain and distress. In order to address this complexity, pain management and assessment require equal multidisciplinary approaches. Therefore, the patient’s voice needs to be heard from the very beginning of an encounter and maintained during the hospitalization, thus establishing a relationship by the nurses or other health care professionals seems fundamental (A. Kitson et al., 2013).
Non-pharmacological strategies (e.g., distraction, hypnosis, breathing) can positively influence how children manage a painful or distressing procedure (Birnie et al., 2018; J. Stinson et al., 2008). Integrating non-pharmacological strategies is recommended to optimize and ensure adequate pain management (Pediatric Anesthesia, 2012). Best practice in the choice of non-pharmacological approach is found through knowledge of the individual child with an identification of the child’s previous experiences and preferences (Alotaibi et al., 2018; Karlsson et al., 2016; Koller & Goldman, 2012). As such, any intervention should ideally match the individual child in a specific context (Birnie et al., 2018; Thompson, 2018).
The hospital clown (hereafter clown) is characterized as a non-pharmacological strategy. The clown operates by inviting children in an imaginative, safe an individually tailored relationship, to support the child in potentially stressful situations (Koller & Gryski, 2008; Linge, 2012, 2013). Clowns have a formalized education. They are trained with a special focus on understanding medical knowledge. Intervention research with clowns using self-reported pain scales, have shown conflicting results concerning the alleviative effect during potential painful medical procedures or conditions (Sridharan & Sivaramakrishnan, 2016). Recently a review, including 24 studies (Lopes-Júnior et al., 2020), showed that children reported significantly less anxiety during different medical procedures with the presence of clowns, furthermore, there was an improved psychological wellbeing in both children with acute and chronic conditions. Nevertheless, the field of children’s pain is characterized by complexity as pain is a subjective and contextually shaped experience which can be managed by various strategies and remain difficult to assess and evaluate. To date, no studies have combined qualitative and quantitative data of the child-clown interactions during specific painful procedures and conditions. The field of pain and pain experience in children is complex and multifaceted. Therefore, there is a need to use multiple approaches to gain unique insight into the topic. In contribution to the existing literature, this study integrates quantitative and qualitative data to expand knowledge of the impact and influence of the clown.
Aim
To expand knowledge on the impact and influence of hospital clowns on 4 to 15-year-old children’s experience of managing painful procedures and conditions during acute and recurrent hospitalizations.
Methods
Mixed Methods Research Design
The present study is a convergent mixed methods design (Creswell et al., 2018) focusing on presenting the integrated findings of three already published studies (Kristensen et al., 2018 2019a, 2019b). The use of mixed methods is founded on the research questions in which several data sources are required for the purpose of comparing, expanding, or contrasting the results and findings.
The mixed methods study involved two distinct stages of data collection within a sequential approach (Figure 1). Stage one consisted of a quantitative study (study 1) and a qualitative (study 2). Stage two consisted of a qualitative study (study 3). Study 1 was a prospective non-blinded study in a parallel design, that aimed to investigate pain intensity of acutely hospitalized children, receiving venipuncture. Assessment of pain intensity using self-report is the recommended source in health care for children as young as 3 years of age, thereby children’s self-reporting of pain intensity is a valuable source of information on pain. Study 2 was an ethnographic study, that aimed to explore (a) the interaction between the acutely hospitalized child and the clown during the venipuncture and (b) how this interaction influenced the children’s experience of pain and ability to manage. Study 1 and 2 took place concurrently by collecting both quantitative and qualitative data at the same time and then analyzing data separately (Creswell et al., 2018). Study 3 was an ethnographic study, that aimed to explore the interaction between the child, and the clown during recurrent hospitalizations, comprising repeated painful procedures and conditions.

A convergent mixed methods design (Kristensen, 2019).
To ensure validity and transparency in the three individual studies (Kristensen et al., 2018, 2019a, 2019b) a precise focus on the methodology for each study was recognized and as such the three studies were conducted in stages between 2016 and 2019. To minimize the threats of validity and transparency and thereby improve the quality, a convergent design was chosen (Creswell et al., 2018). Specifically, parallel questions addressed the same concept. As such, the quantitative variables (pain scores) in study 1 and the qualitative phenomena (experience of pain and ability to manage) in study 2 and 3 were parallel.
Inclusion Criteria for All Studies
Children aged 4 to 15, undergoing painful procedures (e.g., venipuncture, intramuscular injections, nasogastric tube, port-a-cath access) and/or suffering from painful conditions (e.g., mobilization, eating) in the acute pediatric admission unit (study 1 and 2) or in a ward treating children with cancer and rheumatological diseases (study 3) were included in the study. All children were followed by at least one parent (Table 1).
Inclusion Criteria Study 1, 2 and 3.
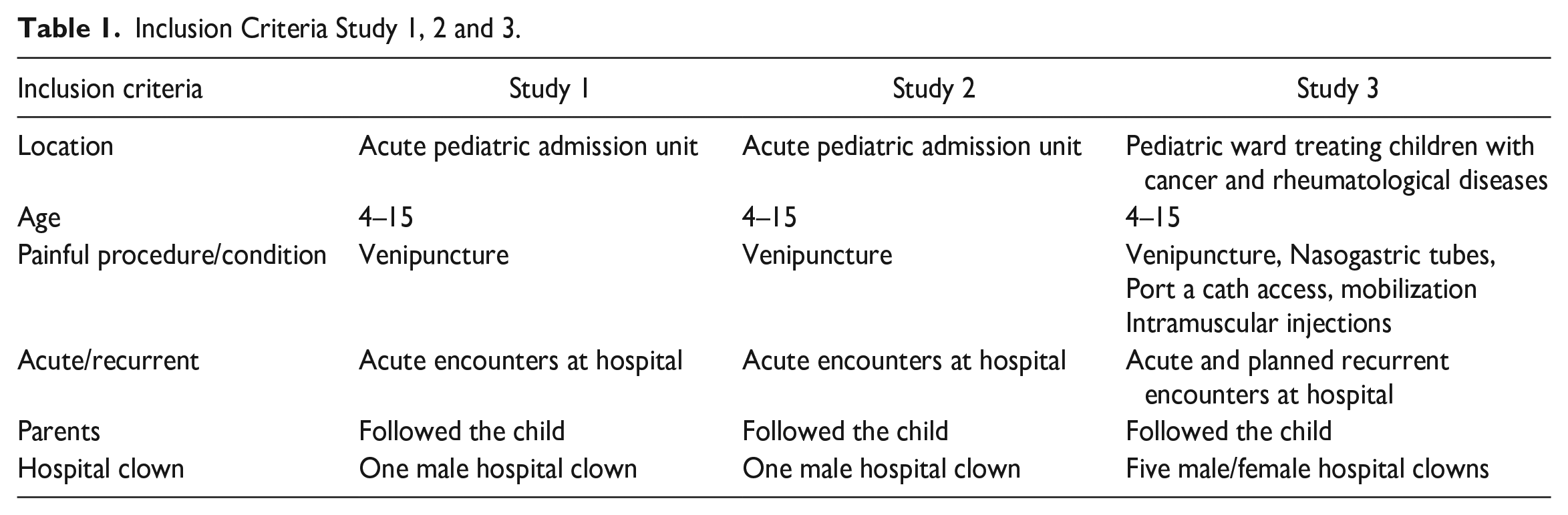
The clowns were connected to the pediatric wards before this study was undertaken. They had a formalized education as hospital clown. In study 1 and 2, one male clown was used for all the included children to secure minimal variation in the approach. In study 3, five clowns participated.
Study Population, Data Collection Procedures and Data Analysis
Study 1: Prospective Non-Blinded Study
One hundred sixteen children were admitted consecutively from April 2016 to January 2017. Children were randomly assigned to either a clown intervention or standard care during acute venipuncture procedure. After allocation to either the clown intervention or standard care, 111 children were included in the analysis. The clown followed the child before, during and after the procedure. Strategies as music, making temporary tattoos, holding hands and guiding were used by the clown. Children in the standard care group collaborated with the nurses before the procedure as they verbally explained the procedure. Parents were involved in collaboration with the nurses and with the clown. Baseline information was collected (Table 2). Primary outcome measure was self-reported pain on two age-appropriate scales (Numerical Rating Scale and Wong-Baker Faces Pain Scale) (J. N. Stinson et al., 2006). Descriptive statistic was used for homogeneity of general characteristics. Pain score and other characteristics was compared using 2-sample t-test. Adjusted analysis was performed to capture the effect of potential intermediate variables. Supplementary analyses were performed, stratified by age (4–6 and 7–15), sex, present pain condition and previous experiences, by using multivariable linear regression. The cut off for age groups was based on literature addressing the challenges in self-report on pain in younger children. For further details see (Kristensen et al., 2018).
Characteristics of Participants.

Note. NRS = Numerical Rating Scale; FPS = Faces Pain Scale.
Study 2: Focused Ethnography
Focused ethnography (Cruz & Higginbottom, 2013) was used to understand more specific aspects of participants’ experiences of a defined element. Hence, focused ethnography was appropriate for the aim of exploring the interactions between the child and clown during acute venipuncture procedures. Thirty-eight children were included (study 2). The fieldwork was undertaken at two public general university hospitals from April 2016 to January 2017. The data collection comprised participant observation, informal interviews, and video recording. The participant observation was performed by following and observing the interactions between the child and the clown from their first encounter until the procedure was completed. The analysis comprised thematic analyses (Braun & Clarke, 2018) in an iterative and non-linear process becoming familiar with the data, generating initial codes, searching for relationships between the codes and developing patterns, reviewing and refinement of the potential themes by rereading data for ascertaining that the themes fit the data material and further identify and label subthemes. The analysis was undertaken in a continuous dialog with all research members. For further details, see Kristensen et al. (2019a).
Study 3: Focused Ethnography
Focused ethnography was used to explore the interaction between child and clown during recurrent hospitalizations (Cruz & Higginbottom, 2013). Thirteen children were included. Inclusion required the child to have recurrent interactions to ensure the possibility to follow the child over time. In total 61 encounters were observed. The fieldwork was undertaken at a public general university hospital from October to December 2017. The data collection comprised participant observation and informal interviews. Typically, it was not known in advance if and when the children were admitted and prescribed a specific procedure. Though the children and the clown did not know, when they would meet again. The researcher followed the clowns on their scheduled days, observing and interviewing children that met the inclusion criteria. The analysis comprised thematic analyses (Braun & Clarke, 2018) and followed the phases described in Study 2. For further details see Kristensen et al. (2019b).
Mixed Methods Integration
The study design is based on a dynamic approach (Creswell et al., 2018), combining both fixed and emergent elements (Creswell, 2014; Creswell et al., 2018). The preliminary results of study 1 and 2 added focus and planning to study 3. Data were integrated at the design, methods and interpretation/reporting level (Creswell, 2014; Creswell et al., 2018) to create the synergy brought about the research questions (Fetters & Freshwater, 2015).
The themes were generated through an interactive back and forth process by a simultaneous frame for merging the quantitative results and the qualitative findings. The mixed methods analyses were an analytical and selective process, in which we examined how both the quantitative results, and the qualitative findings influenced the child’s experience of managing pain in the interaction with the clown during painful procedures and conditions.
Integration at the design level was accomplished by using a convergent design with a concurrent data collection of quantitative and qualitative data for study 1 and 2. The convergent design in this study is further developed by connecting a study 3 (Figure 1). Connecting occurred by linking of the qualitative data from study 2 and 3 concerning two identical assessments of children’s experiences of managing pain-related procedures and conditions in acute and recurrent hospitalizations during clown interactions.
Integration at the methods level was accomplished by linking the quantitative phase (study 1) with the qualitative phases (study 2 and 3) in order to compare the three strands (Fetters et al., 2013). The data collection took place through a parallel and sequential strategy and was followed by separate analyses. The experiences of managing pain during the procedures from the qualitative observations were tightly linked with the pain scores from the quantitative data.
Integration at the interpretation and reporting level was performed. The data from study 1, 2, and 3 were initially reported individually in three papers (Kristensen et al., 2018, 2019a, 2019b). The quantitative and qualitative data were then integrated in a mixed methods analysis to add value to the existing individual studies and expand knowledge of the impact and influence of the clown (Fetters & Freshwater, 2015). First, the quantitative constructs and the qualitative themes was brought together by seeking common concepts (Creswell et al., 2018). Second, the merging is outlined via a narrative approach (Fetters & Molina-Azorin, 2017; Fetters et al., 2013), identifying similarities and differences within the three datasets. Joint displays were applied with the purpose of directly comparing the data through a visual means (Creswell et al., 2018; Fetters et al., 2013). The mixed methods analysis was conducted within a bidirectional perspective, including the merging of the data with both quantitative and qualitative lenses simultaneously in an interactive back and forth process (Moseholm & Fetters, 2017). The fit of integration of Studies 1, 2, and 3 were facilitated using joint displays resulting in either confirmation, complementarity, expansion, or discordance (Fetters & Molina-Azorin, 2017; Fetters et al., 2013). As each of the studies were reported in separate papers, the overall integration and mixed methods interpretation were conducted during a staged approach with cross-referencing to the individual related papers (Fetters & Molina-Azorin, 2017).
Ethical Considerations
The study was approved by the pediatric administration and permission was given by the Danish Data Protection Agency (Journal no. 2008-58-0028; id: 2016-5). All procedures complied with the Helsinki Declaration (World Medical Association, 2000). The children, parents and clowns were provided written and oral information to assure anonymity. Written informed consent was obtained from parents and clowns. All children, parents and clowns agreed to participate. Healthcare professionals were informed during the study period.
Results
Study 1: Prospective Non-Blinded Study
Data from 111 children were included in the analysis. The results showed no demographic differences between the group of children assigned to intervention with the clown or standard care (Table 2). Table 2 presents an extract of the participants’ homogeneous general characteristics from the paper by Kristensen et al. (2018). Furthermore, the results (Table 3) showed that there were no differences in pain intensity, notwithstanding the presence of the clown, even when adjusted for potentially influencing variables (see Table 3) (p = .920). Stratified analysis showed a differing effect between age groups (p = .018). Children aged 4 and 6 were found to have a higher pain intensity score with the presence of the clown (p = .054). Whereas children aged 7 to 15 reported lower scores (p = .025). Stratified analysis showed a nonsignificant difference relating to prior experiences (p = .054). The results showed an estimated positive effect of the clown (p = .085) concerning the group of children with no previous venipunctures. In contrast, for children with previous venipuncture experiences, an estimated negative effect was found (p = .248). Table 3 presents an extract of Table 2 in the paper by Kristensen et al. (2018).
Crude and Adjusted Analysis.

Note. Cl = confidence interval; Diff. = difference (Kristensen et al., 2018).
Adjusted for baseline variables related to the VP procedure: local anesthetic, nitrous oxide, time per procedure, number of punctures.
Study 2: Focused Ethnography
The data analysis resulted in an overarching theme: Hospital clown tailoring strategies to individual child creating a WE. This WE represents a responsive interaction between child and clown, described as a close relationship which evolved during a mutually focused and continuous attention. This WE was observed initially when the clown expressed: “I think we can talk about, how WE manage this venipuncture,” and was further evidenced by children’s expressions: “WE can do this together.” The WE included verbal and non-verbal gestures that manifested an interactive and close relationship between child and clown. The strategies tailored by the clown focused on the child’s response, behavior and expression and were intended to create this WE, that gradually evolved during the establishment of a relational alliance between child and clown from the first encounter until the child left the hospital. The overarching theme was based on three themes: (1) How do WE do this together? covering the first encounter, before venipuncture, illustrated by a familiar atmosphere, creating a mutual understanding and a clear game plan. (2) WE are together, during venipuncture, covering the time the lab tech entered the examination room until the venipuncture was completed. It includes articulation, implementation and modifying the game plan, facilitated by the clown. (3) WE did it! covering the period after, illustrated with a mutual evaluation, which manifested the importance of remaining in the interaction after the venipuncture (Kristensen et al., 2019a).
Study 3: Focused Ethnography
The data analysis resulted in an overarching theme: An ongoing WE, based on two identified themes: (1) Stronger in a WE, which covers Maybe today. . .? demonstrating how the clown initially showed a cautious approach to the child and You are my friend referring to involvement and closeness, expressed verbally and physically by the child and clown. (2) Hope in a WE related to the current and the future painful procedures and covers WE did it your way and see you again, related to the child’s and parents’ expectations of help from the clowns in managing current pain-related situations and future meetings. The WE was characterized by a strong and close relationship developed during recurrent hospitalizations (Kristensen et al., 2019b).
Integrated Mixed Methods Findings
In response to the overall aim, integrating the findings from study 1, 2, and 3 led to three mixed methods findings: (1) An age-differentiated approach, (2) Understanding the child’s condition, and (3) Previous experiences as a part of the child’s history. The mixed methods findings will be presented in the following sections through narrative weaving and joint displays (Guetterman et al., 2015) (Figures 2–4). Specifically, in Figure 2 we added an example of the specific data.
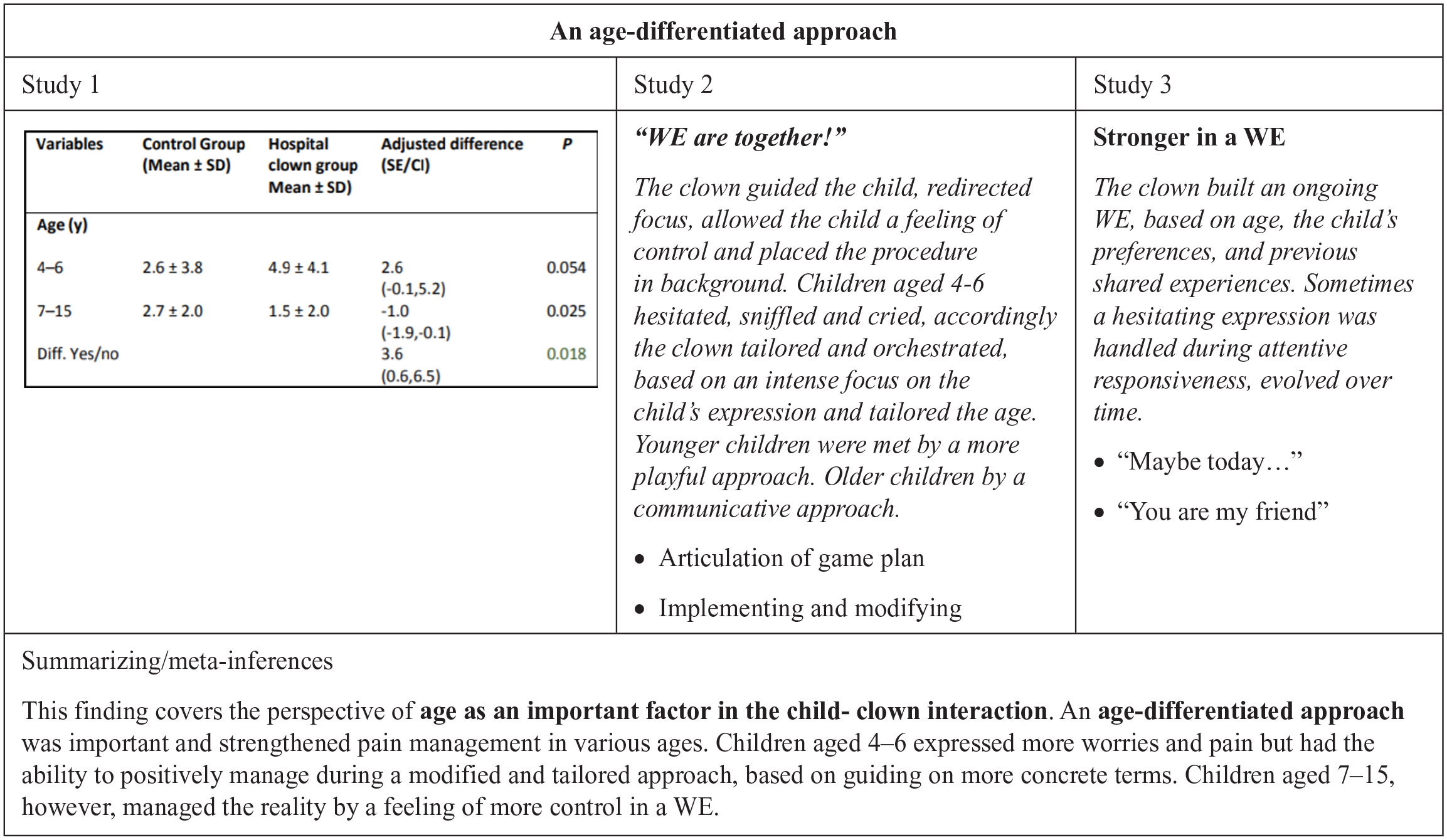
MM Finding 1: An age-differentiated approach.

MM Finding 2: Understanding the child’s condition.

MM Finding 3: Previous experiences as a part of the child’s history.
An Age-Differentiated Approach
This integrated finding covers that an age-differentiated approach in the child-clown interaction was important for the child’s ability to manage painful procedures and conditions. Study 1 showed a higher pain intensity score for children aged 4 to 6 years when interacting with the clown (2.6 [−0.1, 5.2], p = .054). In contrast study 2 and 3 found an established WE tailored to the age of the child, that positively influenced the children’s ability to manage during painful procedures or conditions. Thus, the pain intensity scores were somewhat inconsistent with study 2, as this age group were found to have a higher pain intensity score with the presence of the clown and at the same time the interaction with the clown in a WE relationship positively influenced the child’s ability to manage. The results were also somewhat consistent, as some of the youngest children more than the older group of children were hesitating, sniffling, or crying. These findings can both be related to the actual painful procedure and/or to the whole situation and context of being sick, the unknown staff etc. However, the findings highlight, that the clown tailored and modified the strategies to the children’s age and various expressions, as demonstrated by the clown keeping an intense focus with the child, stressing WE are together. Thereby the children (aged 4–6) mostly cooperated keeping their arms straight without moving, even when a worried facial expression was observed. Study 2 and 3 showed how closely the children (aged 4–6) paid attention, while the clown guided them, tailoring the strategies to the age of the child by using more concrete terms (e.g., tattoos, toys) and taking the whole situation in consideration. These findings illustrate an expanded understanding of the assessment of pain (using pain scales) in younger children, pointing at a positive influence of the clown, although the pain intensity score was higher (Diff. 4–6/7–15 p = .018) in the group of 4 to 6 aged children with clown.
Study 2 and 3 expanded the understanding of the reduced pain intensity scores (−1.0 [−1.9, −0.1], p = .025) (study 1) in children aged 7 to 15. The age-differentiated approach was shown during a focus on the child’s expressions, which supported the children in maintaining a sense of control, expressed by the children as a feeling of being a part of a WE. The redirecting of the focus of attention during the procedure, suggests that the engagement with the clown allowed the older children to distract themselves, resulting in a lower pain intensity score.
Understanding the Child’s Condition
This integrated finding covers that clown’s attentive focus on understanding the children’s condition was essential for the children’s experience of managing painful procedures and conditions. Some of the children complained about a double challenging situation, as they had to deal with both an overall feeling of pain and an insecure situation, relating to the procedure. The pain intensity scores (study 1) demonstrated that children, to a limited extent, benefited from the clown intervention. Findings from study 2 and 3 complemented that, among different aspects, a painful current condition could affect the children in a way that they would not have the mental or physical capacity to interact with the clown. Study 3 revealed how the clown assessed and respected the current state of the child’s condition, which therefore sometimes caused the encounter to be postponed to another day (“Maybe today”). Though the recurrent hospitalized children were certain that the clown would be there in future situations (“See you again”), in contrast to the acute children. Thus, findings from study 3 to some degree, expand Study 1; for example, the clown asked for permission and acknowledged the state of the child by giving time, and promising the children to come again (“Maybe today”) to share as friends (“You are my friend”). On the other hand, the clown’s cautious approach led the children to push pain, bad mood, etc. to the background of their attention, with a feeling of being stronger in a WE. This suggests a positive influence on the children’s ability to manage, which is contradictory to the pain intensity scores. Moreover, the evaluation (“WE did it your way”) involved a focus on hope in the WE, expressed as an expectation from the children for the clown to help despite the current situation (Study 3).
The findings from study 2 suggest how the clown used a conscious-focused approach when integrating the children in “How do WE do this together?,” taking small steps in the initial meeting to provide a familiar atmosphere and the following preparation of the children, which led to an intuitively uncovering of their condition and formed the basis for a clear game plan. Thus, the articulation, implementation, and modification of this game plan (“WE do/are together”) in contrast to Study 1 (children aged 4–6; p = .054) suggests a positive influence of the clown, even when they were suffering from a painful condition. For example, the children acted and collaborated with relief and smile in their responsive interactions with the clown. The alliance in the acute encounter was maintained through continuity before, during, and after venipuncture. Continuity during recurrent encounters were complemented by findings from Study 2, revealing how the children challenged their current pain, given the benefits of the clown creating a WE, when the interaction was maintained according to the children’s terms.
Previous Experiences as a Part of the Child’s History
This integrated finding covers that the clown’s strategy based on the child’s history of previous experiences and related feelings were essential for managing the current pain related situation. Previous experiences seemed to either strengthen or diminish the children’s expectations of ability to manage as they were forced to navigate multiple and diverse feelings (e.g., worries, anxiety, fear of restraint, pain, relief). Although the clown was present, the children managed differently during the procedure with either a relieving attitude or a hesitating and anxious one. The results from the pain intensity scores (study 1) to some degree complemented the impact of previous experiences by affecting the pain intensity. Results showed a tendency to increased pain intensity scores with the presence of the clown (SE/CI −0.9 [−2.4, 0.5]), even the findings in study 2 showed how the clown used a conscious strategy for verbalizing the previous experiences and building up the current situation based on these. In contrast, the results from the children with no previous venipunctures showed the benefit of the intervention with the clown given the lower pain intensity scores (SE/CI 2.0 [−0.0, 4.0], p = .053). However, contrasting experiences were revealed (study 2) as worries connected to both the acute situation and previous experiences were positively managed during the interaction with the clown “How do WE do this together.” In addition, the children in a mutual evaluation managed to share the strategies for the next procedure with the clown based on the current situation. These findings were confirmed in study 3, describing how the visualization and repetition of the children’s individual strategies in the responsive interaction were present during the recurrent encounters and strengthened their hope for a less painful experience in the future (“Hope in the WE”). However, a few cases (Study 2) demonstrated that previous experiences based on restraining and threats affected the children in a way that the interaction with the clown did not help, pointing at a negative effect, as shown in the pain intensity scores.
Finally, findings from the recurrent hospitalization (“WE did it your way”) expanded the findings from the acute (“We did it”) as illustrating how the clown continuously helped the children navigate their contrasting feelings, building a strategy, specifically based on their common previous experiences. The importance of conducting an evaluation was shown in study 2, as a part of the procedure to modify memories, reduce the anticipatory fear for subsequent procedures, and providing the children with competencies in pain management. Study 3 showed that the individually tailored approach included perspectives of the histories of the children, which seems to provide the children with the feeling of being remembered and received as a friend. Thereby a feeling of hope and safety was facilitated in a WE, which positively influenced the child’s experience of pain management.
Discussion
With the aim to expand knowledge on the impact and influence of the clown on 4 to 15-year-old children’s experience of managing painful procedures and conditions during acute and recurrent hospitalizations, this study reveals a relationship in a WE, representing a responsive interaction between the child and clown. A uniquely tailored and modified clown approach, responding to the individual child’s expression and needs, characterized the WE. Despite differences in pain intensity scores, this WE was found to strengthen the children’s competencies for managing procedure-related pain by giving the child a feeling of not being alone.
An Age-Differentiated Approach
Providing an age-specific approach suggests a positive influence on managing pain related procedures or conditions. In line with the present study, child life literature (Thompson, 2018) mention age as one of the most critical variables to affect a child’s emotional response to hospitalization and medical procedures. Further, the results of Linge (2012) report that age play a pivotal role in the child-clown interactions. In contrary to evaluate specific procedures, Linge (2012) evaluated children being hospitalized for various lengths of time. Nevertheless, the results show some similarities, in that the hesitating and cautious attitude, expressed by younger children, suggest that more time is needed when establishing the relationship. Therefore, the findings emphasize the importance of applying a tailored and age-differentiated approach in a WE, which may strengthen the children’s experience of managing painful procedures and conditions during acute and recurrent hospitalizations. Age-related differences can be explained by cognitive, emotional and psychosocial development (Sommer et al., 2010). As such the age 4 to 6 is a vulnerable period in terms of procedures and hospitalization, as they have limited abilities to do abstract thinking (Thompson, 2018), whereas children from 6 years of age master more complex thinking, (Kaakinen et al., 2015, Chapter 13; Thompson, 2018 ). Accordingly, the present findings imply how an interaction with the clown using more concrete terms increased feelings of control for the younger children, which seemed vital to this age group (Linge, 2012; Thompson, 2018). The strategies for older children include more cognitive interactions with the clown that involves choices and self-expression and thereby allows them to apply the concepts from one situation to another and evaluate their thinking and experiences.
Understanding the Child’s Condition
The finding of maintaining a special and continuous focus on the individual child’s condition from the outset and during all phases of the process represent a key aspect in establishing a relationship based on trust. This relation in a WE seemed to support the child in managing experiences of pain during painful procedures and conditions. Different circumstances, for example, lack of time, can affect the interaction, thus implying that the presented strategies should be tailored to the individual child to enhance the children’s ability to manage these painful situations. A child’s effort to manage may be considered either emotion-focused or problem-focused (Biggs et al., 2017; Lazarus & Folkman, 1984; Thompson, 2018). According to the findings of this study the individually tailored approach is linked to an understanding of WE to both accommodating the children’s feelings (mutual understanding, “You are my friend”) and the more specific plan for managing the procedures (game plan). Therefore, understanding and respecting the children’s condition may form the basis for enhancing the children’s feeling of managing. The trustful relationship was represented in the child as a feeling of being seen and met from the first encounter. Thus, the present findings indicate that the clown (as the professional) established a relationship as an ongoing WE, which seems to support the child in managing painful procedures. This professional child-clown relationship might be comparable with the relational dimensions between patient and nurse, described in the Fundamentals of Care (FoC) framework (A. L. Kitson, 2018), as the core in nursing practice. In this framework five relational aspects (trust, focus, anticipate, know, and evaluate) are conceptualized as fundamental for nurse’s to establish a relationship (Feo & Kitson, 2016; A. Kitson et al., 2013) that can support the individually tailored care (A. Kitson et al., 2013). This study illustrates that the clown mediated the psychosocial dimensions using the relational aspects as enhancing the children’s understanding and facilitating their managing creating this relationship. It can, therefore, be assumed that the responsive interaction in a WE during procedures and related conditions implicate that support for a child’s managing pain might be handled as a special task in the room. The complexity of this task may therefore be taken care of besides the specific procedure.
The present findings have raised important questions about how the focus on the psychosocial dimensions, shown in a WE, can be perceived as important as the physical and practical issues and thereby provide the children with an integrated experience of care in painful procedures and related conditions.
Previous Experiences as a Part of the Child’s History
In the present study, a tendency to increased pain intensity and worried expressions and attitudes were found for children with previous experiences, even when the clown was present. Children often describe needle-related procedures as the worst pain (Friedrichsdorf et al., 2015; Walther-Larsen et al., 2017). Furthermore previous negative experiences may affect the child’s response of pain in the current situation (McMurtry et al., 2015; Noel, Chambers, Petter, et al., 2012; Noel, Chambers, McGrath, et al., 2012; Noel et al., 2018; Thompson, 2018). This study shows how the clown accommodates the children’s previous experiences by asking the children how they felt during previous experiences, subsequently embracing the children’s expression in the WE. Consequently, it is possible that negative previous experiences require special attention and approaches.
Research on the risk of negative pain memories and the influence on children’s experience of managing pain during recurrent procedures accounts for the importance of drawing attention to unmanaged pain (McMurtry et al., 2015; Noel, Chambers, McGrath, et al., 2012). Accordingly, the strategies provided in the present findings, encompassing the previous experiences, explain how the clown established an evaluation focusing on successful strategies, which supported the children in a feeling of “I/WE did it” or “WE did it your way.” Noel et al. (2018) showed that interventions of reframing may modify a child’s memory of needle-related procedures and thereby positively influence the child’s anticipatory fear of pain related to future procedures. An evaluation should therefore be an integrated part of managing the painful procedure or condition. The present findings expanded previous research on language-based memory reframing (Noel et al., 2018) by illustrating how a tailored and trustful interaction in a WE can offer an accurate and positive reframing of children’s memories by maintaining a close alliance during an evaluation important for the future. Thus, making the first potential painful experience a positive one and taking the memory into account for the next situation seems critical.
Strengths and Limitations
Complexity characterizes the research field of pain as a subjective, emotional, and individual experience and moreover a phenomenon that can be moderated by various strategies and difficult to assess and evaluate. Therefore, the added value from conducting this mixed methods study is based on the strengths of both quantitative and qualitative methods which led to new insights and nuanced perspectives on 4 to15 aged children’s experiences of managing painful procedures and conditions, specifically of the impact and influence of clowns.
Especially integrating the findings of the three studies provided nuances and lead to new findings which could not be captured in one of the single studies. To state the importance of an integration, an example illustrated, that the higher pain score found in study 1 for children aged 4 to 6 year when interacting with the hospital clown were expanded in study 2 by the qualitative observations, where the established WE tailored the age of the child positively influenced the children’s ability to manage during painful procedures or conditions.
The use of mixed methods is founded on the research question in which several data sources are required for the purpose of comparing, expanding, or contrasting the results and findings (Creswell et al., 2018). In addition, the mixed methods approach provides knowledge that cannot be captured by either a quantitative or qualitative approach alone. Therefore the integrated findings in this study added nuances to the three individual papers.
The important point of discussion in mixed methods is the integration (Fetters & Freshwater, 2015; Fetters et al., 2013; Schoonenboom & Johnson, 2017). Moreover, efforts should be made to acknowledge the research tradition related to the individual studies. The limitations and strengths of each individual study are presented in the individual papers.
The convergent design chosen in this study is both concurrent (Study 1 and 2) and sequential (study 3), which allows the focus to emerge and added nuances to the observations (Creswell, 2014; Creswell et al., 2018; Schoonenboom & Johnson, 2017). To improve the quality and minimize validity threats, the convergent design requires parallel questions addressing the same concept (Creswell et al., 2018). As such, the quantitative variables and the qualitative phenomena were parallel. Nevertheless, for some of the quantitative constructs and qualitative themes linking was not possible (Creswell et al., 2018; Fetters et al., 2013), which may potentially exclude some nuances (e.g., duration of procedures, gender, parent’s role).
The label connecting was revised several times and finally based on referring to two assessments of the clown interactions. Ideally, a plan developed for data collection is conducive to merging different datasets by choosing similar instruments and thereby looking for common concepts (Creswell et al., 2018; Fetters et al., 2013). However, the integration at the methods level in this study represents some limitations, such as the use of self-reported pain, which was not chosen as a data collection method in Study 3, due to the type of interactions, where sometimes no procedure was included.
Conclusion
This research has shown that the child’s age, physical and psychological condition and previous experiences influenced the child–clown interactions. Specifically, the findings demonstrate how a WE, characterized by a continuous responsive interaction between child and clown has an impact and positively influenced 4 to 15-year-old children’s experiences of managing painful procedures and conditions in both acute and recurrent hospitalizations. The uniquely tailored and modified clown approach, responding to the individual child’s age, physical and psychological condition, and previous experiences, was expressed in the WE. The WE, initially established by the clown from the first encounter, maintained and further tailored during the process in a mutual close and trustful individual relationship, illustrates the importance of getting to know the individual child from the very first encounter. Thereby, the findings demonstrate how the WE approach strengthened the child’s competences in managing painful procedures and conditions.
Relevance to Clinical Practice
The findings can be transferred to nursing practice, as the relational dimensions is an integrated part of nursing practice. Healthcare professionals could benefit from adapting some of the presented strategies to establish a trustful relationship in a WE atmosphere, tailored to the individual child from the first encounter and continuously throughout hospitalization. This requires an active involvement of the child, with recognizing the age of the child as a key to choose strategies in planning and ensuring the best individual health care. Furthermore, the relationship in a WE should encompass the uniqueness of the child’s history, based on cognitive abilities, previous experiences, levels of distress, pain, and actual condition. It is pivotal to acknowledge the importance of a WE as a distinct psychosocial and relational caring practice to be taken into consideration. Thus, an important point for further research and discussion is if supporting the children in a WE atmosphere might require an extra person in the room besides the health care professionals handling the procedures.
Footnotes
Acknowledgements
The authors acknowledge Professor Erik Elgaard Soerensen for his contribution to make this research possible. To our sorry, Erik Elgaard Soerensen passed away in 2019.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Danish Child Cancer Foundation, Copenhagen; the North Denmark Region Health Science Foundation; and the Clinical Nursing Research Unit, Aalborg University Hospital, Denmark.