
Abstract
This study aimed to explore the lived experiences of patients receiving maintenance hemodialysis in Pakistan. Purposive sampling was used to recruit 24 patients and six healthcare professionals, each participated in a semi-structured interview. Interpretive Phenomenological Analysis was used to analyze interviews’ data. Two superordinate themes, “The experience of hemodialysis” and “The conceptualizations of hemodialysis” as well as six sub-themes were identified. The experience of hemodialysis was related to, the implications of HD procedure on everyday life, social, cognitive, emotional, financial, and occupational influences. While all participants recognized the importance of hemodialysis for their survival, their conceptualizations of the treatment varied. Despite facing multiple challenges, optimism and independence were observed among participants. Stigma related to hemodialysis, and role adaptation, which appear unique to the Pakistani context, highlight a need for tailored interventions designed to enhance and maintain the mental health of patients receiving hemodialysis in Pakistan.
Introduction
Chronic kidney failure leading to End-Stage Renal Disease (ESRD) is currently a challenge faced by more than 2 million people worldwide, a number that is increasing by 5% to 7% annually (USRDS, 2018). In Pakistan, it has been estimated that there are about 16,000 new patients with ESRD every year (Hamid et al., 2019; Naqvi, 2009). Patients with ESRD require ongoing renal replacement therapy to survive, which can be either in the form of peritoneal or maintenance hemodialysis (Himmelfarb & Ikizler, 2019). ESRD may also be treated successfully with a kidney transplant (Chiaranai, 2016; Lee, 2017) from a living or deceased donor. The majority of end stage renal disease patients in Pakistan, usually, cannot get a kidney transplant due to a lack of funds and limited number of kidney donors (Jha, 2013). Due to problems such as infections and expenses associated with peritoneal dialysis (Aldukhayel, 2015; Crowley, 2013; Iyasere et al., 2016; Yeates et al., 2012) patients usually have to undergo maintenance hemodialysis (HD) for the rest of their lives (Argyropoulos & Unruh, 2014). Around 99% of all patients with ESRD in Pakistan receive maintenance HD as the preferred treatment method (Sinha & Bagga, 2015).
HD is commonly performed in standalone dialysis centers or hospitals (Weinhandl et al., 2012). During HD, a patient’s blood is continuously filtered through a dialyzer, which acts as an artificial kidney and a filter, and then pumped back into the patient’s body (Kara et al., 2007) using an extracorporeal circuit. During maintenance hemodialysis, end stage renal disease patients are connected to an hemodialysis machine for 3 to 5 hours per session, usually three times per week (Moran et al., 2009). These HD sessions, while vital for patients’ survival, are often experienced as disabling, and frequently pose a major challenge for patients with ESRD (Castro et al., 2003). Other challenges associated with HD include traveling, time commitment, dependence, social challenges, emotional difficulties, and changed lifestyle, all of which can render the HD experience a negative one (Dziubek et al., 2016; Najafi et al., 2016; Weisbord, 2016).
In addition to the issues experienced by patients receiving HD globally, providing HD in Pakistan is associated with particular challenges. In Pakistan, dialysis is difficult and expensive, with only 40% of patients with ESRD having access to dialysis, and most of these patients are under dialyzed; they are dialyzed twice, instead of the recommended thrice weekly (Prasad & Jha, 2015). Limited medical resources in government hospitals as well as the high cost of medical treatment in private dialysis centers and related financial problems are burdens associated with hemodialysis in Pakistan (Jha, 2013). Socio-economic factors associated with HD, such as loss of income, lack of employment, and disruptions to education, have significant impacts on the quality of life of patients receiving hemodialysis in Pakistan (Anees et al., 2018). Subsequently, the majority of patients receiving hemodialysis in Pakistan suffer from depression (Bhatti et al., 2014), which may see patients terminating their HD treatment prematurely (Reid et al., 2016). Such termination subsequently results in an increased premature mortality rate among patients with ESRD (Farrokhi et al., 2014). Hence, ESRD and the associated HD affect patients’ quality of life more adversely than other potential pre-existing chronic comorbidities such as diabetes, heart failure, arthritis, and chronic lung disease. A study by Anees et al. (2011) revealed that several patients receiving HD in Pakistan decided to withdraw from maintenance HD as they experienced a reduced quality of life associated with the treatment. The complexities around delivering effective HD in Pakistan point to a need for thorough investigations into the lived experiences of Pakistani patients receiving HD. These patients face a lifelong dependency on a dialysis machine for their survival, with most also facing limited medical and financial resources in this developing country.
Further, as emphasized by Engel (1977), cultural influences, the experience of illness, and adaptation to chronic conditions (Pomaki et al., 2011), it is important to understand the experience of patients receiving hemodialysis in their individual cultural context, and in this case, this may also apply in the cultural context of Pakistan. Moreover, the existing literature on patients receiving HD in Pakistan is predominantly based on quantitative data (Anees et al., 2018; Bhatti et al., 2014; Hamid et al., 2019; Shafi et al., 2018; Zohair Nomani et al., 2016), highlighting a need for in-depth qualitative investigations in order to gain further understanding of the subjective lived experiences of patients receiving HD in Pakistan.
To address the gap in the body of knowledge in relation to the lived experience of patients receiving HD in Pakistan, the current study, which was part of a larger project concerning the wellbeing of HD patients in Pakistan, engaged an in-depth qualitative investigation. The focus of this investigation was to generate a nuanced picture of psychological aspects of the lives of patients receiving HD to inform interventions aimed at improving important objective and subjective aspects in the lives of patients receiving HD in Pakistan. The research question posed in the current study was: “What is the lived experience of patients with ESRD undergoing maintenance HD in Pakistan?.”
Method
Methodological Approach
An interpretive phenomenology was adopted as the methodological approach in this study. Interpretive phenomenology is both phenomenological and hermeneutic in its approach (Shaw et al., 2014; Smith, 2004). In the context of our study, phenomenology relates to the notion that the world is shaped and experienced through awareness (Willig & Rogers, 2017); hence, the analysis of the experience is performed “by the one who is experiencing it” (Bacon et al., 2020; Smith, 2004). Interpretive phenomenological analysis (IPA), which was used to analyze the data in the current study, evaluates the cognitive and emotional reactions of participants toward their experiences (Smith, 2011). Moreover, interpretive phenomenological analysis is hermeneutic, which means it intends to make meaning intelligible (Willig & Rogers, 2017). According to Smith (2011), interpretive phenomenological analysis is “double hermeneutic,” as firstly participants analyze their own experiences, making sense of them, and the researcher then interprets those interpretations participants share with her/him. Therefore, in interpretive phenomenological analysis, the perspective of the researcher is equally as important as the experience of participants (Smith, 2004). Interpretive phenomenological analysis is also idiosyncratic, so it is important to analyze every case individually to evaluate how each participant makes sense of his/her own experience.
Participants
Participants were recruited from a variety of clinical settings including a government hospital, one private HD center, and a non-government organization based HD center in Pakistan. Patients were included if they were diagnosed with ESRD in Pakistan and had been on maintenance HD for at least 6 months prior to commencement of the study. Exclusion criteria included severe physical health conditions, cognitive impairments, hallucinations, delusions, and/or suicidal risks. A total of 24 patients (19 males and 5 females) volunteered and consented to participate in the study. They ranged in age from 21 to 60 years and had been receiving HD for 1 to 9 years. We also recruited healthcare professionals in these clinical settings because they are in regular contact with patients with ESRD and observe patients receiving HD on a daily basis. We reasoned that their observations would enrich the data and our understanding of the context of HD. Two nephrologists, two HD nurses, and two HD technicians, who have been working with patients receiving HD for more than a year, participated in the study. The study received ethics approval from the Edith Cowan University, Human Research Ethics Committee (2019-00613-SHOUKET). All participants provided informed consent and received a written information letter and a consent form in Urdu.
Data Collection
Semi-structured, in-depth individual interviews were conducted with patients and healthcare professionals. Two semi-structured interview schedules guided the interviews: one for patients receiving HD and one for healthcare professionals (see Supplemental File for interview schedules). Patients were asked about their perceptions and experiences of HD. Health professionals were asked what they observed about patient experiences based on their professional practice in working with patients undergoing HD. Interviews were conducted in dialysis centers, either during dialysis sessions or while patients were waiting for their treatment. Interviews were between 20 and 40 minutes in duration. The interviews were conducted in Urdu, and to enhance accuracy and rigor, the translations, performed by the first author, were validated by another Urdu and English bilingual researcher. In the verbatim transcripts participants’ names were replaced by pseudonyms.
Data Analysis
Transcribed interview data were analyzed using IPA. The step-by-step guide for IPA suggested by Smith et al. (2008) was followed. Initially, the interview transcripts were read, and recordings of the interviews were listened to several times to allow the chief investigator to become immersed in the data. The second step involved writing comments made on observations. In the third step, themes were developed by connecting and observing patterns between various comments. The fourth step of analysis was to observe connections between identified themes. The fifth step was to repeat the same process in full for another interview. The sixth and final step was to identify patterns across all interview transcripts. This involved higher-order analysis by organizing themes in the form of a data matrix, reflecting comparability and shared meanings across all participant discourses, and identified themes.
Rigor
Rigor was enhanced by transcribing the audio interviews verbatim and then reading each transcript several times to become immersed in the data (Burhans & Alligood, 2010; Yardley, 2000). Moreover, data were collected from multiple sources including patients receiving HD and healthcare staff (nephrologists, HD nurses, and HD technicians); therefore, the information was enriched and cross-checked. Additionally, journaling and triangulation enhanced rigor (Barusch et al., 2011).
Reflexivity
Researchers’ interpretations were extremely important in our study. The first author is a native Pakistani who is well aware of cultural issues that are relevant to HD and, further, has had firsthand experience with a significant other who received HD as a patient diagnosed with ESRD. During the study, a reflective diary (Galea, 2018) was kept by the first author, to note observations, feelings, and perceptions about the experience of HD in Pakistan. Moreover, to minimize bias, the researcher’s evaluation of the HD experience for patients in Pakistan was discussed with the research team and the audiotapes, transcripts, and analysis were returned to repeatedly to ensure that the findings and conclusions were grounded in the data
Results and Interpretation
Two superordinate themes and six sub-themes (see Table 1) were identified in the data. The superordinate themes and subthemes are discussed below along with illustrative quotes from participants.
Superordinate Themes and Subthemes.
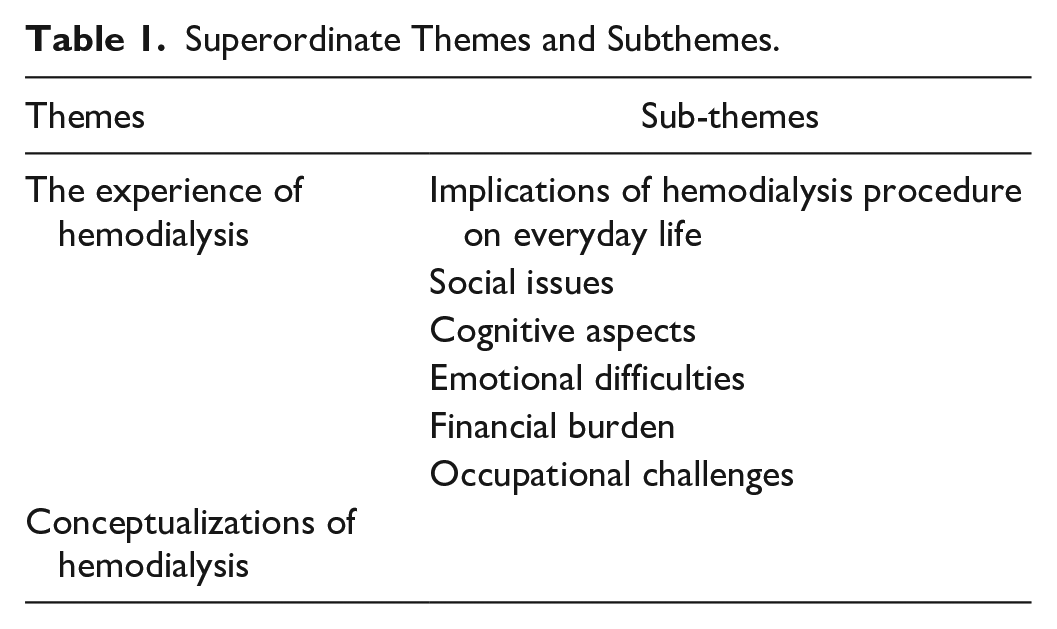
The Experience of HD
The superordinate theme “The experience of the HD” relates to multiple aspects of the implications of HD procedure on everyday life, as well as social, cognitive, emotional, financial, and occupational challenges related to undergoing HD as reported by participants.
Implications of HD procedures on everyday life
All implications that were related to the procedure of HD itself, were characterized as subthemes in the experience of HD. The implications were: HD being time-consuming and repetitive; lifestyle limitations; dependence; age and distance; frequently experienced symptoms; HD changes life overall and kidney transplant, and are described below:
HD’s time-consuming and repetitive regimen
Participants experienced the time-consuming nature of HD to be frustrating as they found it challenging to pass the time during treatment. Moreover, the entire experience of attending a HD session is not limited to the 3 to 4 hours of treatment but further requires additional time to travel to and from the HD center before and after every session and waiting for the preparation and attachment to the HD machine, which takes an extra 15 to 30 minutes in addition to patients’ treatment and travel time. Further, HD treatment sessions are repetitive, and are usually needed to continue for the rest of a patient’s life or until a kidney transplant becomes available, making the overall HD experience difficult to endure for patients. As Hassan (27yo, male) shared:
Firstly, it is troublesome when you must travel for 50 kilometres on public transport to get to the dialysis unit. Secondly, you must lie down here for long hours of treatment, after which, you must travel back home. You must repeat this process twice a week. All of this is extremely hard.
In Pakistan, the lack of quality public transport along with financial difficulties make a time-consuming and repetitive HD experience even harder for patients receiving HD to endure, which was apparent in the participants’ discourses.
Lifestyle limitations
Amongst all the lifestyle limitations, such as a renal specific diet, and travel requirements associated with HD, the participants in our study cited their general dietary and fluid intake restrictions among the most significant challenges they face, Zahid (55yo, male), patient receiving HD, has described: “Dialysis has taken away the biggest blessing of life from me, that is water. Water is a blessing of God, isn’t it? One on dialysis cannot drink water anymore.” A participant in our study, Asif (50yo, male), described his efforts to follow several “strict [dietary] preventive measures” by re-counting how he avoids having lunch or dinner with his family, preferring instead to eat in a different room. In Pakistan, food is a paramount aspect of social gatherings, and many patients receiving HD, due to their restricted food intake and specific dietary requirements, often avoid social gatherings. Indeed, Aslam (55yo, male) related that he avoids attending family gatherings as he cannot eat much of the food.
Another lifestyle restriction experienced by patients receiving HD, which was highlighted in our study, related to personal travel and/or leisure. Since dialysis routines require the availability of a HD machine at regular intervals, patients could not go too far from a dialysis center; thereby significantly impacting the lifestyle many enjoyed prior to becoming dependent on HD. One participant, Hassan (27yo, male), stated that: “It is difficult for me to travel, I cannot go anywhere.” Additionally, traveling limitations generally influence socializing where travel would be needed to meet family and friends. Komal (32yo, female) stated: “It’s disadvantage is, that one is detached, belonged just to this thing [HD]. Now for almost two years, I haven’t been to Karachi” [city of the maternal family]. However, in cases where patients receiving HD do plan to travel, they must prearrange their HD treatment at their destination and liaise with the relevant centers before departure. Badar (59yo, male) has been on HD for seven consecutive years and has managed to travel abroad by arranging his HD sessions elsewhere in advance. He expressed his experience as: “I had dialysis in Saudi Arabia. I went there for Umrah [pilgrimage] and had two dialysis sessions there.” However, for patients receiving HD, traveling was complicated by a number of factors, such as physical health, fitting in requirements for HD during travel, having sufficient financial resources, and most importantly, patients’ attitudes. It appeared that among the patients receiving HD who participated in the current study, positive outlook encouraged travel whereas negative outlook discouraged it.
Frequently experienced HD-related symptoms
Participants reported that they experience general weakness, fluctuations in blood pressure, and headaches as common side effects during and after HD sessions. Sakina (50yo, female) described her experience in this way: “I feel exhausted, once I reach home after my dialysis.” Moreover, another patient participant named Aslam (male, 55yo), described that “Dialysis leaves me with headaches and low blood sugar level. I also experience fluctuations in blood pressure during and after dialysis.” Contrary to this, some participants in our study did not report any such symptoms and some who did have symptoms, noted they sometimes lasted for only a few minutes during the day of HD.
According to the doctors who participated, physical weakness following a HD session could be due to the lower frequency of HD treatment in Pakistan when compared to international standards for maintenance HD, where patients receive HD more frequently and with longer treatment hours consequently show fewer side-effects caused by the infrequency of treatment. A nephrologist interviewed for this study also pointed to the lower quality of HD in Pakistan as a possible cause for patients feeling weak after treatment and adversely affecting their quality of life, he noted: “There is lack of high-quality dialysis which adversely affects the patients’ quality of life.”
Dependence
Some patients learned to accept the lifestyle change of being dependent on others to attend their HD sessions, while others were able to maintain their independence. For example, Usman explained his dependency on others:
“One becomes dependent upon someone else. As my brother must come with me. He will stay with me for four hours. I cannot come alone, as on the dialysis day, usually, I cannot walk.”
However, other patient participants in our study reported that they have managed to live their lives and engage HD while maintaining their independence. As participant Saleem (60yo, male) explains, “I drive my bike by myself to and from [dialysis centre].” This finding reveals an optimistic positive aspect of HD that has rarely been reported. Notably, when patients did not experience debilitating side effects from the treatment, some could maintain the agency they were accustomed to by traveling alone.
Age and distance
The participants’ age and their residential distance from HD centers were reported as having a significant impact on patient experiences of and with HD. Generally, younger patients with ESRD coped better with the daily challenges of undergoing HD, while elderly patients viewed their own struggle as useless and overwhelming. As stated by a patient Amjad (39yo, male): “Age is a huge factor. I have observed that young patients have tolerated the dialysis impact well. . . .However, the ones who are aged do not strive hard.” The distance of an HD center from a patient’s residence is another relevant factor that influences the experience of patients receiving HD. This is especially the case for those living in remote or rural areas of Pakistan, where health facilities such as HD centers are not readily available. For example, participant Ishak (24yo, male) traveled more than 250 km in total to and from his HD sessions. Similarly, participant Khalid (45yo, male) lived in a village about 100 km away from his HD center. Both participants were using public transport to get to sessions, which—given the paucity of reliable public transport in Pakistan—prolonged traveling time substantially. Khalid described his experience:
Dialysis is an extremely hard experience for me since I come from afar. I must come for dialysis every third day of the week. . . . . I live so far away that I will reach home after sunset. What day is today? Isn’t it Thursday? There are only two days in between that is Friday and Saturday. On Sunday, I must again leave home to come to the city and might stay at someone’s place to make it for Monday’s dialysis.
Khalid’s quote illustrates how living further away from a HD center impacts on the experience of patients with ESRD. The experience is significantly less taxing for patients living closer to an HD center., for example, Zahid (55 years, male), who lives close to an HD center, states that “I am fortunate enough, it [dialysis centre] is close to my home.”
HD changes life overall
HD affects a patients’ lives overall, involving drastic lifestyle changes that disrupt daily living. Some patients who were working abroad when diagnosed with ESRD, had to leave their jobs, and return to Pakistan as they were not eligible to receive HD treatments in the countries, they worked in. Amir (31yo, male) explained how his life has drastically changed due to the need for maintenance HD:
I was a tanker driver. I used to live in Jeddah, Saudi Arabia where I owned an oil tanker. I drove that throughout Saudi Arabia. . . . .I had my vehicle; however, when I came back, I sold everything. Earlier, I could travel anywhere, but these days, due to my illness I cannot go anywhere. Most of the time, I stay at home.
Similarly, Asif (50yo, male) was part of a management team in a Dubai-based company and was leading what he considered to be a normal life. When he was diagnosed with ESRD, he needed to return to Pakistan as he could not continue his job and was unable to afford any medical expenses in Dubai. Undergoing maintenance HD subsequently drastically changed his life. Prior to the ongoing HD treatment, he had been financially independent and now he was dependent on his family for living and support. Another participant, Usman (21yo, male), had been studying engineering but had to leave his studies when it became impossible for him to manage the regular HD routine with daily classes scheduled at university. Even if someone manages to work along with undertaking HD, overall life conditions change.
The lives of family members of patients receiving HD are also significantly affected. Ijaz (52yo, male), another HD patient, described how families of patients with ESRD can face certain problems noting that, “There are three types of effects [on the family]. Firstly, they are bound to follow a patient’s schedule, then they must take care of the patient, and lastly, they must face financial stress as well.” Families of patients are impacted in multiple ways, where some participants thought that they themselves were a common source of stress for their families. Participant Salman (31yo, male) stated: “If we look closely, I am the major tension my family has right now. My pain affects the whole family environment.”
Kidney transplant
Only a few patients receiving HD in our study were waiting for a potential kidney transplant and were expecting to then be able to cease the ongoing HD treatments. Amir (31yo, male), who had a graft rejection after a first kidney transplant and was waiting for another kidney transplant, stated: “I was ready for transplant. . ., but doctors found an infection in my kidneys. A transplant can’t be done again until the infection is cured . . . . . .after transplant I’ll be free from dialysis.” Additionally, the long-term success of kidney transplantation cannot be guaranteed. Amir’s graft failure occured 3 years after a successful kidney transplant. However, there were several patients who noted that they cannot receive kidney transplants due to multiple reasons, thus they were relying on HD as the only ongoing treatment option for the rest of their lives. Adnan (52yo, male) has been on HD for 2 years and deliberately chose not to pursue a kidney transplant option. He stated: “Unfortunately, I could not find a living donor [of kidney] in my family, and I do not want to take the risk in the black market.” In Pakistan, the vast majority of potential kidney donors are underprivileged villagers who sell one of their kidneys, rather than donors from patients’ families (Moazam, 2013). Therefore, most Pakistani patients receiving HD cannot afford the expense of a kidney transplant and the post operational treatment associated with it. According to one estimation, in Pakistan, less than 5% of patients with ESRD had a kidney transplantation (Rizvi et al., 2013) that is 5 to 15 patients (per million population, pmp), unlike any other developed countries (USA > 55 patients pmp), where more patients with ESRD consider kidney transplant an option (Herlin & Wann-Hansson, 2010).
Social issues
Several social issues related to HD were also highlighted by the participants in our study. These issues included social support, negative social influence of HD, and the social stigma of HD. These subtheme categories of social aspects of HD are discussed below:
Social support
Participants highlighted the importance of social support from their family, friends, fellow patients receiving HD, and staff at the HD center. The role of the family is especially crucial in the lives of Pakistani patients receiving HD, where it can substantially alter and improve the HD experience. One patient, Nadia (35yo, female) expressed: “If your family does not support you, it gets very hard. However, if you have someone who supports you, encourages you, takes care of you, in that case, it [dialysis] does not remain that hard.” Further, patients receiving HD in our study described that their friends’ support played an important role in their lives. Ishak (24yo, male), a HD patient, noted the emotionally supportive role of his friends in his life: “Whenever I feel agitated at home or I am unwell, I visit my friend. He knows that I can come to him when I am upset, so he talks to me and sets me free of my worries.” In addition to providing emotional support, in some cases, patients receiving HD in our study were also financially supported by their friends. Khalid (45yo, male) stated that: “It becomes hard to bear the expenses. I survived these 15 months on HD because of my friends. . .they send me money.”
Our study highlighted that the HD center was also viewed as an important social support system for patients. Patients with ESRD who regularly attended the same HD center were identified in our study as having a shared social support network. Amjad (39yo, male) described the experience of HD sessions in HD centers with his fellow patients by noting: “Now we have a good connection with each other [in dialysis centres]. The patient beside me is now like my mother. . . . . . We have found a new way of living, a new life, new relatives, new friends [in dialysis centres].” Additionally, the staff within HD centers also play an important role in patient experiences of HD. Nadia (35yo, female), a HD patient, describes the role of HD staff: “The care of the staff here helps us to have a good time.” Hence, staff often form significant interpersonal bonds with patients, to the extent that patients develop an attachment to particular staff members and centers. Nadia stated: “If we go to a new place [HD centre], the fear of unfamiliarity might give us stress.”
Negative social influence of HD in life
Participants also reported adverse effects of HD on their social lives. Some patients lost contact with friends who could not manage the limitations related to living with ESRD and HD. Amjad (39yo, male), a participating HD patient, described: “There used to be friends who would call me ten times a day. But nowadays, I often text them myself to remind them that I am still alive.” Further, patient Asif reported that his wife had abandoned him as she could not bear to live with his lifelong chronic illness. Contrary to this, some participants reported that their families were overprotective and restricted patients’ independence, regardless of a patient wishes and/or their individual abilities. For example, sometimes family members disregarded patients’ wishes for independence and insisted on escorting them to treatment. Hassan (27yo, male) an HD patient, stated: “I can come by myself [to dialysis Centre], but my mother doesn’t agree. They don’t let me go on my own anywhere.” Such behavior often restricts patients who strive for living independently with their lifelong survival treatment. This indicates that an adequate level of social support is required for patients receiving HD; either too little or too much support can significantly affect the lived experience of patients receiving HD.
The social stigma of HD
In Pakistan, the social stigma of dialysis is of impending death, and this stigma is injurious to patients’ well-being. This negative attitude and belief about HD in Pakistan was explained by Hakim (35yo, male) experience:
My doctor suggested that my family potentially would discourage me from attending dialysis, it would be better not to tell them. I went ahead with dialysis without informing my family. Afterwards, my family thought I tortured myself by going through this. I told them, not doing this, would have killed me; dialysis helped me to continue living. If I would have told them before [HD] they wouldn’t have let me do dialysis at all. Our village people rarely choose to do dialysis.
Similarly, one physician stated: “Patients have a mindset, that if you go for dialysis, you will die. They [patients receiving HD] get the message [from society] that don’t go for dialysis [it’s not good for you].” These findings suggest that the social stigma related to HD may be a common experience in Pakistan, and specific to the context in this country.
Cognitive aspects
Cognition or thinking pattern of patients receiving HD in Pakistan were also found to be influenced by HD in several ways during our study. These cognitive aspects related to HD as reported by participants of the study are discussed below.
Social comparison
It is humans’ innate drive to think and evaluate themselves by comparing to others (Festinger, 1954). Sometimes, patients receiving HD may use downward social comparison. Such thinking patterns help them to feel better about their own state of health. As Adnan (52yo, male) noted: “Look around, some patients are in worse health than mine.” Further, when patients observe problems in other patients, they sometimes forget about their own issues. As Aslam (55yo, male) stated: “When I come here [HD centre], I forget my own [problems]. The pain of other patients worries me more than my own.” In contrast, some patients compared themselves to those who are in better health, in an upward comparison. Shahida (48yo, female) described her observation: “All the patients, that are along with me, they stay healthy and stable [during HD], I don’t know whether they are fine at home too. I have seen them being more active than me.” This type of cognitions can impact or injure a patient’s self-esteem and diminish motivation.
Pragmatism
Patients who think of HD as a means to an end have been termed “pragmatists” (Cornish & Gillespie, 2009). Visualizations of a darker side of life without HD can also act as a motivation toward undertaking HD. As Badar (59yo, male) stated: “If one will not come here for dialysis, he/she might go to the graveyard instead.” Further, some patients think in terms of the cost and benefits of treatment, assessing the benefits of HD to help them to cope. Nadia (35yo, female) explained:
There are benefits and losses too. The benefits are that instead of lying on the bed, it’s better to come here for four hours. Once I go back, I can do my household chores. If I will not do that [HD], I will be on the bed. So, it’s [HD] better than that.
This type of thinking helps patients receiving HD to accept HD in their life and to develop a more positive experience of their treatment.
Thoughts of death
Participants described thinking about death, either that they were waiting for death, or they were afraid of HD due to its association with inevitable death. For some patients, during the early stages of HD thoughts of death seemed like a better option than HD. Ishak (24yo, male) described his death-related thoughts: “One keeps on thinking about his/her death. Such as, who knows when I will die or where will I die?.” Irfan (47yo, male), another patient, stated that he wished his daughter to be married before his death. Further, patients receiving HD are also impacted by the death of other patients. The death of fellow patients often devastates patients as they think this previews their own impending demise. As a patient participant, Amjad (39yo, male) expressed: “I had a patient [name of fellow patient] with me. I used to have a great chat with him. He was sixty, we developed a great friendship. We would visit each other and would chat often. But he died after two months. This had made a huge impact on my mind.”
Adopting the role of patients
Participants reported of others who adopted the role of patients and did everything to fulfill role-related duties. Amjad (39yo, male) observed that some patients adopt a patient’s role: “Patient attach a label of a patient to themselves and fulfill its duties.” This phenomenon was also observed by the HD technician interviewed in this study. He stated: “Sometimes patients make up their mind that they are incapable of doing anything because of their illness. Instead of using their willpower, they become dependent on others for tasks like commuting to dialysis centres, etc.” This finding about HD also appears to be unique in the context of Pakistan and might reflect the importance of the family structure in Pakistan where, unlike in the Western world, usually one family member takes responsibility of the other family members. It is a cultural imperative to take responsibility of sick family members. This might be the reason that the sick family member with this mindset thinks that family members should take care of others. Being sick, they consider themselves as eligible for dependence on other family members. This culture fosters a dependency on others, thinking of themselves as patients, thus reduces efforts of independence and/or adaptation to their illness.
Emotional difficulties
Patients receiving hemodialysis in our study described the experience of strong emotions due to the commitment required to regularly attend HD. Aslam (55yo, male) explained his feeling: “I am upset since the beginning [of HD] due to its nature. Because we are neither among [the] living nor are we dead.” Additionally, patients receiving HD reported an “alien effect.” Salman (31yo, male) explained his state of mind as: “For me, this is like living in a dream. It seems that my eating, drinking, movement, and meetings with people are not part of my routine, it is rather a dream.” Further, patients receiving HD experienced a loss of interest in daily activities. Salman stated that: “I don’t feel like doing anything.” Some patients receiving HD show anger or irritability, as reported by Majid, a dialysis technician, who was working with patients receiving HD for 15 years. As Majid (stated: “They become irritated, they feel bad over small things and get hurt easily.”
Typically, patients receiving HD experience several significant emotions from the beginning of treatment onward. Khalid (45yo, male) explained his journey from denial to adaptation.
When I was first told that I should go with the dialysis, I left from outside of the dialysis centre. Then I ran here and there for alternate treatment. . . . . .Once, when I fainted, they took me to the hospital where I had dialysis in an emergency. For four days, I was not in my right mind; I was talking foul and was abusing others. After that, I kept on having dialysis. I was getting better . . . now I am habitual. Now it’s nothing special. Now, if someone says they have a [kidney]problem, I say dear make fistula, dialysis is not a problem.
Financial burdens
There was agreement that hemodialysis and financial problems were interlinked. One participant physician stated that “the financial issue is the major problem.” Asif (50yo, male), the aforementioned participant who lost his Dubai-based job due to ESRD, felt it was hard for every HD patient to bear the overall financial expenses of an ongoing dialysis treatment. He stated: “It is not about being poor. You have to spend money on dialysis [and] when the patient will not do any job, how can he get any money?.” Usually, in government hospitals, where HD services are provided for free in Pakistan, patients must wait for several months before they can be allocated to a dialysis center. Irfan (47yo, male), who has been on HD for 4 years, was currently doing HD at a non-government organization based HD center, where he described his experience as follows: “I have applied [for dialysis in a government hospital] many times. They put my name on the waiting list, but I never got a place there.” One physician interviewed in this study explained: “The government sector cannot bear the [financial] burden [of this disease]; therefore, many patients have to get treatment from the private health sector. That’s an economic and psychological burden too [for patients receiving HD].” In Pakistan, the minimum cost of maintenance HD is typically USD $1,680 per year for each patient, which poses a significant financial burden for most Pakistani patients receiving HD where the average annual income is the equivalent of USD $420 (Rizvi et al., 2011); therefore, patients with low income are more likely to refuse HD treatment in Pakistan (Shafi et al., 2018) as places in government hospitals are scarce, and private HD centers are expensive (Jha, 2013). Due to financial problems and a scarcity of HD facilities in Pakistan, patients with ESRD cannot get the medically recommended number of HD sessions per week, which is a minimum of three (Himmelfarb & Ikizler, 2019) as per international health standards. A nurse participant working at a HD center stated:
“Sometimes the patient does dialysis twice weekly because we don’t have enough facilities or machines available, sometimes it’s thrice-weekly or in the rare cases, it’s only fortnightly.”
Occupational challenges
Occupational challenges were found to be associated with hemodialysis in Pakistan. This study showed that it was hard to continue with an income-generating job while on maintenance HD due to patients’ general weakness, treatment repetition, and the time-consuming nature of HD. Khalid (45yo, male) described that he was unable to continue his work with HD:
I cannot do any work. For example, today [after dialysis] when I will reach home in the evening, I will not be tranquil. I will have to sleep through the night to get relaxed the next day. Then after two days, I will have to come back for dialysis again. That is why I cannot do any work and I am unemployed right now.
Moreover, it is difficult for patients receiving HD to find employment due to Pakistani society’s stigmatization of HD. Amjad (39yo, male) shared his experience: “We can’t get a job, no one gives us a job. . . . . . . . . . . . Now I want to be a volunteer, but people tell me not to do it, you cannot do it.” However, some patients continued to have an income-generating employment. Sultan (60yo, male) has been on HD for 14 years. He maintained his job while on HD until he retired a couple of years prior to participating in this study. He shared: “I think if one is working, it passes time [faster]. If someone is not working, he will irritate family and neighbours [laughter]. . . . If one doesn’t work, he gets irritated.” One participant physician also observed that some patients receiving HD were working by managing to schedule the time of their HD sessions with the requirements of their job. He stated: “Here, there are some patients who are managing their job with dialysis. They are earning and supporting both [their families and their treatment]. For them, dialysis is not a problem.” When a patient is employed and generates an income, their financial matters are also easier to manage.
The experience of HD was found to be associated with various challenges such as emotional, social, cognitive, financial, and HD treatment related. However, despite adversities associated with HD, the way patients with ESRD perceive HD in their life defines their life with HD.
Conceptualizations of HD
Whilst all participants recognized the importance of HD for their survival, their views of HD were not uniform. HD was conceptualized as positive when considered as a lifeline and as an “alternate kidney” that is necessary for survival. One patient, Komal (32yo, female) stated: “As long you are given a life by God, you must protect it from suffering. This (HD) is a means to do that, in other words, this (HD) is our life.” Further, as HD partially and temporarily replaces the function of the kidneys, participants explained that the HD machine was like an alternate kidney for them. Badar (59yo, male), an HD patient, explained: “Since my kidneys have stopped functioning properly, this (HD) acts as an alternative to my kidneys.” Patients receiving HD in this study reflected that their life continues because they undergo HD. Hence, in the life of patients with ESRD receiving HD, the body and HD machine become an interwoven unit.
Several patients receiving HD conceptualized the treatment as an imposition because they did not view it as a choice, but rather as an activity imposed on them for survival. Usman (21yo, male), a HD patient, stated: “It is mandatory. If I did not do it, my health would deteriorate. I would not be able to walk, breath, lie down, and(or) sleep with ease.” HD was conceptualized by some of participants as a punishment resulting from their misdeeds. For example, Salman (31yo, male) describes it as “This dialysis to me. . .Do you understand punishment?? . . . . . . . [That dialysis] seems to me as punishment.” This maladaptive coping strategy adversely affects the mental health of patients receiving HD. This strategy is rarely reported in other domains and may be a distinctive feature of the Pakistani context.
Discussion
As intended, our study provided an in-depth analysis of the lived experiences of ESRD patients in Pakistan, reliant on hemodialysis machine for survival, from the perspective of patients, dialysis nurses and doctors who are involved in their care. Maintenance HD is a lifelong survival treatment for the vast majority of patients with ESRD in Pakistan (Sinha & Bagga, 2015); nevertheless, it was associated by participants in our study with various challenges. The implications of HD procedures on everyday life, social, cognitive, emotional, occupational, and financial issues influenced patient experiences of HD in the Pakistani context in distinct ways.
Our study found that time-consumption during HD and the need for the treatment to be continuously repeated to ensure survival make this machine dependent hemodialysis experience most challenging for ESRD patients. These findings are consistent with previous research (Hagren et al., 2005; Herlin & Wann-Hansson, 2010; Welch & Austin, 1999). Further, also congruent with studies conducted in other countries (Clarkson & Robinson, 2010; Kaba et al., 2007; Tu et al., 2014; Yapa et al., 2020), several similar limitations were reported by patients, for instance, restricted fluid intake, dietary, and travel restrictions were reported to be taxing the lifestyle of Pakistani patients receiving HD, effectively restricting social engagements of patients with family and friends. This is because food and travel are traditionally the central components of social gatherings in Pakistani culture. Moreover, the patients receiving HD in our study reported significant HD-associated symptoms and side-effects, such as physical weakness, fluctuation of blood pressure, and headache during and after HD treatment. Associated symptoms may be due in part to less than optimal treatment protocols in Pakistan. These symptoms made the overall HD treatment experience sometimes more troubling than it usually is in other countries (Kuipers et al., 2019). Patients receiving HD in our study were dependent not only on HD machine but on a caregiver due to their age and general physical weakness or frailty for self-care, hygiene, transportation, and treatment (Shahgholian & Yousefi, 2015). Nevertheless, participants managed to maintain various levels of independence when they were medically better. Moreover, we identified that elderly patients receiving HD in Pakistan were often finding it harder than younger ones to manage the emotional challenges associated with HD treatment. This is consistent with the findings of Ulusoy and Kal (2020) who have reported similar findings previously in Pakistan. Our findings also indicate that attention should be given to the mental health of elderly patients receiving HD in Pakistan. We have also found that patients receiving HD from rural areas were facing difficulties managing their lives in Pakistan, as most HD centers are in larger cities, often far from patients’ homes. From our study, it becomes clear that engaging in HD treatment drastically changes the lives of patients with ESRD and their families in Pakistan. The demands of ongoing maintenance HD on patients profoundly affect their lives. For example, as related by our participants and in existing literature, areas such as studies, work, and life plans are significantly affected (Dekkers et al., 2005; Small, 2010). Due to the hefty financial expenses involved with it, only a few participants in our study were waiting for a kidney transplant. Most Pakistani patients with ESRD thus view HD as a permanent renal replacement therapy (Taber et al., 2014).
Consistent with the findings of Ng et al. (2015) in Singapore, our study found that patients receiving HD, who visit a particular center regularly for treatment, interact with other patients and HD nurses there, creating a social support network almost akin to family. These findings support the work of Borzou et al. (2014), noting the role of HD nurses in positively influencing patient well-being and significantly affecting the experience of HD. In the current study, similar to the study of Pasyar et al. (2020), peer support among patients receiving HD, was found equally beneficial for both recipients and mentors. Moreover, previous research findings are congruent with ours in that social support from family and friends generally helps patients receiving HD cope better with their life-changing and lifelong chronic condition of ESRD (Al Nazly et al., 2013; Shahgholian & Yousefi, 2015). However, consistent with existing literature (Clarkson & Robinson, 2010; Hagren et al., 2005; Small, 2010), our participants sometimes chose to avoid socialization due to fatigue, physical deterioration, and an overall changed lifestyle due to their chronic disease and the implications of the ongoing treatment. Therefore, the support from dialysis nurses and peers in dialysis center is important. The social stigma associated with HD as inevitably resulting in death reported by participants, has not been observed in other contexts and appears to be specific to the Pakistani context.
Findings from our study indicate that patients receiving HD often engage in social comparison, pragmatism, adapting to a patient’s role, and thoughts of death. Further, in our study few patients receiving HD were observed to adopt a patient’s role. Adapting to a patient’s role, patients receiving HD often find comfort in being taken care of by others and become increasingly dependent. In such cases, patients are less likely to live a functional life with HD, as they relinquish responsibility for their care to family members and adopt the role of a helpless patients. Thus, they find their condition as a justification to escape their responsibilities toward themselves and others. Dependency was also imposed on patients receiving HD by their families. These findings were unique to Pakistan due to dependency of family members on each other, being a cultural norm.
Congruent with the studies conducted by Hain et al. (2011), and Ahmad and Al Nazly (2015), our study found patients receiving HD experienced considerable emotional difficulties; hence, some were just surviving rather than enjoying their lives. Moreover, significant shifts in emotions among patients receiving HD in Pakistan were found in our research, from the onset of maintenance HD to the later stages in their life, while still attending maintenance HD. This emotional distress has also been previously noted by other authors as being often ignored (Shahgholian & Yousefi, 2015). Therefore, our study supports the findings of Dąbrowska-Bender et al. (2018), which emphasized that patients with ESRD on HD should be provided with psychological care, which has the potential to improve their quality of life (Taylor et al., 2016). However, due to limited resources, the psychological concerns of patients are typically ignored (Jha, 2013). Hence, our study underscores the need for affordable and readily accessible psychological support along with HD treatment, which are commonly not provided.
We found that financial constraints are affecting patients with ESRD negatively when they attend HD in Pakistan, which is similar to the findings of Anees et al. (2018). Due to the scarcity of affordable HD facilities in Pakistan, the majority of patients on HD undergo hemodialysis only twice weekly instead of the global standard of thrice-weekly (Jha, 2013). Financial difficulties were linked to occupational problems in our study. Our study findings are consistent with Shahgholian and Yousefi (2015), who have confirmed that HD is often time-consuming and repetitive; hence, deprived most participants of their energy and time. This, in turn, makes it difficult for them to combine work with their necessary treatment on an ongoing basis (Al Nazly et al., 2013). However, in contrast, our study also highlights that some patients can carry on with their paid employment in addition to attending HD regularly. These findings are supported by literature that states being gainfully employed provided patients receiving HD with financial independence, less loneliness (Herlin & Wann-Hansson, 2010), and also aid coping with HD itself (Tu et al., 2014).
Although all patients in our study were undergoing maintenance HD, there were significant differences between patients as to how they experienced and conceptualized their treatment. This finding challenges the previously published literature that highlighted negativity associated with HD (Anees et al., 2018; Bhatti et al., 2014). It has further accentuated the need for mental health support programs specially tailored to the needs and culture of patients receiving HD in Pakistan, that engender or encourage positive conceptualization of a chronic treatment regimen.
Strengths and Limitations
Our study provides a nuanced picture of the lived experience of patients with ESRD undergoing maintenance HD in Pakistan, which was informed by patients receiving HD, and nephrologists, HD nurses, and technicians working with these patients. Another strength of the current study is that it gives the voice to the optimistic aspects that are often ignored in Pakistani studies. Specifically, despite scarcity in medical facilities and financial problems associated with HD in a developing country, some machine-dependent HD patients manage to survive and lead a close to normal life while engaging in HD treatment. This may reflect the various ways patients conceptualize HD and its influence on their lived experience. Further, this study highlights the need of culturally tailored psychological intervention, which is based on needs of patients receiving HD. Moreover, our study highlights the importance of peer educator model for patients receiving HD in Pakistan.
There were certain limitations to the current study. First, those patients receiving HD who quit HD were not represented in the study even though their views could further enrich the data. Thus, for future research, there could be an in-depth analysis of the new and long-term patients receiving HD in Pakistan in cross sectional studies as well as long term follow up in longitudinal studies.
Conclusion
The findings of the current study provide important insights into the lived experience of Pakistani patients dependent on hemodialysis machine for the survival. Emotional and financial burden of ongoing HD treatment drastically changes the lives of patients with ESRD and their families. Further, most patients receiving HD lose their job due to the HD’s time-consuming nature and associated physical side effects. However, some patients could continue with their employment, earn an income, and live independently when they receive adequate support. The social stigma surrounding HD through its perceived association with death may be unique to the context of Pakistan. Nevertheless, patients found dialysis nurses and fellow dialysis patients at the HD centers could provide an important social support system that helped to counter the social and emotional repercussions of the stigma they experienced. The findings of our study indicate patient experiences related to receiving HD varied and were influenced by patient thoughts about the procedure and other individual factors. Despite adversities related to HD in Pakistan, some patients receiving HD managed to keep themselves engaged and optimistic. However, many Pakistani patients receiving HD would benefit from targeted psychological support. We propose that such interventions may enhance and maintain positive perceptual and thinking patterns, which would assist individual patients with ESRD to conceptualize HD positively, enhance their self-esteem, improve their physical and mental functionality, and enhance their overall lived experience.
Supplemental Material
sj-docx-1-gqn-10.1177_23333936221128240 – Supplemental material for “Machine-Dependent”: The Lived Experiences of Patients Receiving Hemodialysis in Pakistan
Supplemental material, sj-docx-1-gqn-10.1177_23333936221128240 for “Machine-Dependent”: The Lived Experiences of Patients Receiving Hemodialysis in Pakistan by Haseeba Shouket, Eyal Gringart, Dierdre Drake and Ulrich Steinwandel in Global Qualitative Nursing Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.