
Abstract
Early mobilisation of mechanically ventilated patients has been suggested to be effective in mitigating muscle weakness, yet it is not a common practice. Understanding staff experiences is crucial to gain insights into what might facilitate or hinder its implementation. In this constructivist grounded theory study, data from two Scottish intensive care units were collected to understand healthcare staff experiences relating to early mobilisation in mechanical ventilation. Data included observations of mobilisation activities, individual staff interviews and two focus groups with multidisciplinary staff. Managing Risks emerged as the core category and was theorised using the concept of risk. The middle-range theory developed in this study suggests that the process of early mobilisation starts by staff defining patient status and includes a process of negotiating patient safety, which in turn enables performing accountable mobilisation within the dynamic context of an intensive care unit setting.
Keywords
Introduction
Technological advances and progression in critical care patient management have improved intensive care delivery (Kerlin et al., 2021). Pre-COVID-19 pandemic data suggests that the numbers of patients who survive critical illness over the past two decades had increased and reached a plateau in the last 10 years (Esteban et al., 2013; Scottish Intensive Care Society Audit Group, 2020; Zimmerman et al., 2013). These survivors commonly experience long-term health problems associated with their intensive care unit (ICU) stay, known as post-intensive care syndrome (Harvey & Davidson, 2016). Critical care researchers and clinicians worldwide have been shifting attention to alleviating this syndrome (Harvey & Davidson, 2016; Needham et al., 2012).
ICU acquired weakness is one of the major contributors of post-intensive care syndrome (Griffiths & Hall, 2009). This weakness is manifested in the form of muscle wasting, which has been suggested to be associated with mortality and poor patient outcomes (Ali et al., 2008; Hermans et al., 2014; Latronico et al., 2014). Importantly, mechanically ventilated patients are frequently reported to experience ICU acquired weakness (Herridge et al., 2011; Stevens et al., 2007). Muscle weakness develops rapidly and within the first hours of the initiation of mechanical ventilation support (Jaber et al., 2011; Levine et al., 2008; Parry et al., 2015; Puthucheary et al., 2013). Experts have concluded that the syndrome plays a significant role in impeding weaning (De Jonghe et al., 2007; Dres et al., 2017; Jung et al., 2016; Thille et al., 2020). Evidence shows that ICU acquired weakness in mechanically ventilated patients persists for an extended time, reducing the quality of life after hospital discharge (Herridge et al., 2011).
A strategy that has been recommended to counteract muscle weakness in intensive care is early mobilisation of mechanically ventilated patients (EM-MV) (NICE, 2017; The Society of Critical Care Medicine, 2020). The term EM-MV is used to refer to a range of mobilisation activities that have been shown to be safe and feasible for mechanically ventilated patients, including sitting on the edge of bed, sitting in a chair and walking (Bailey et al., 2007; Bourdin et al., 2010; Camargo Pires-Neto et al., 2013; Davis et al., 2013; Pohlman et al., 2010; Schweickert et al., 2009; Toccolini et al., 2015; Winkelman et al., 2012; Zanni et al., 2010). Research suggests that EM-MV is effective in improving patient outcomes and reducing hospital length of stay (Martin et al., 2005; McWilliams et al., 2015; Needham et al., 2010; Ota et al., 2015; Winkelman et al., 2012). However, despite its potential, EM-MV is still uncommon (Bahadur et al., 2008; Dinglas et al., 2013; Meg E Harrold et al., 2015; Mendez-Tellez et al., 2013; Pohlman et al., 2010; Skinner et al., 2015; The TEAM Study Investigators, 2015; Zanni et al., 2010). Its implementation poses some challenges, including ICU staff beliefs that such practice might endanger the patients (Campbell et al., 2015; Clemmer, 2014).
An earlier systematic integrative review summarised evidence on EM-MV definitions and activities, revealing the lack of an agreed definition and the need for an evidence-based definition of EM-MV (Clarissa et al., 2019). Most included studies employed quantitative approaches looking at different patient outcomes of EM-MV implementation in such patients. These studies have contributed to the understanding of its effectiveness and impact on improving patient outcomes, but what constitutes EM-MV across studies was not consistent as evidenced by varied activities from in-bed mobilisation to walking (Clarissa et al., 2019).
The review findings also show that EM-MV was commonly delivered by multidisciplinary staff (Clarissa et al., 2019) and the necessity of a team approach in its implementation has been highlighted by included studies (Barber et al., 2015; Eakin et al., 2015; Holdsworth et al., 2015; Parry et al., 2017). Several included studies were looking at decision-making and used surveys to collect data of who decides EM-MV (Bakhru et al., 2015; 2016; Hodgin et al., 2009; Nydahl et al., 2014; Skinner et al., 2008). For instance, Nydahl et al. (2014) conducted a 1-day point-prevalence survey with an aim to evaluate EM-MV routine practice of 116 ICUs in Germany. They collected data regarding the professions who decided EM-MV. Amongst 98 ICUs requiring an order to initiate EM-MV, the decision could be made by either a physician (n = 98, 84%), a nurse (n = 65, 56%) or a physiotherapist (n = 31, 27%). While the results could provide a description of which profession tends to make a decision in EM-MV, how the decision was made remains unknown. How clinical staff with different training and educational backgrounds bring their knowledge forward to inform their decision regarding EM-MV warrants further exploration.
Arguably, the multidisciplinary characteristics of the ICU team entail differing perceptions, care priorities and responsibilities, which may influence the EM-MV process. Yet, investigations of ICU staff’s experiences in delivering EM-MV are lacking. A broader understanding of how EM-MV is experienced is required, which then can facilitate its implementation in clinical practice. Qualitative research into the EM-MV process and the care team’s experiences is therefore warranted. The current constructivist grounded theory study was conducted to theorise the process of EM-MV, guided by the initial following research questions: 1. What are the experiences of staff implementing early mobilisation in mechanically ventilated patients? 2. How is the decision about early mobilisation in mechanically ventilated patients made? 3. What are the barriers and facilitators of early mobilisation in mechanically ventilated patients from the standpoints of the involved staff? 4. What is the interaction between the patient and staff during the early mobilisation process?
Methods
Study Design
Charmaz’s constructivist grounded theory methodology (Charmaz, 2000, 2014) was used to generate a middle-range theory with constructivism epistemology. Constructivism holds that reality does not exist in an independent world external to the researcher and multiple realities are constructed by the interaction between the inquirer and those being studied (Guba & Lincoln, 1994; Schwandt, 1998). EM-MV was viewed as an enacted process involving ICU staff’s actions which constructed the middle-range theory by conceptualising connections between events and experiences (Charmaz, 2014).
Study Sites and Participants
Summary of data collected and recruited participants.
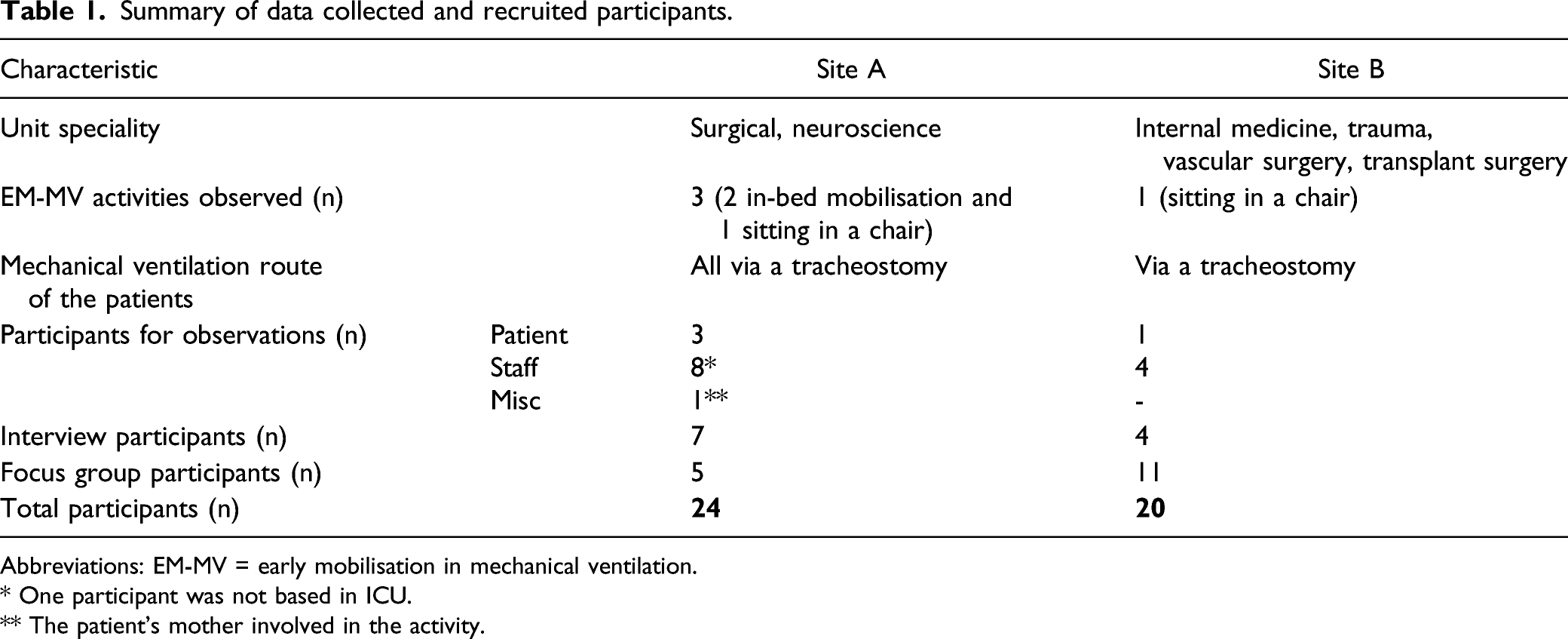
Abbreviations: EM-MV = early mobilisation in mechanical ventilation.
a One participant was not based in ICU.
b The patient’s mother involved in the activity.
The selection of hospital sites, recruitment of multidisciplinary staff and patients and EM-MV activities to be observed reflected purposive sampling. ICU staff with at least 6 months work experience who were involved in any stage of EM-MV (planning, delivery and evaluation) were recruited for observations, individual interviews and focus groups. Mechanically ventilated patients were recruited for observations. Theoretical sampling was used to generate a theoretical understanding of the staff’s experiences and the process of EM-MV, directing the research process towards the middle-range theory construction (Charmaz, 2014; Glaser & Strauss, 1967). Interview questions that changed over time and an interview with a surgeon to explore issues regarding EM-MV with post-surgery patients reflected theoretical sampling.
Data collection started with an observation and the analysis of this data informed the decision of conducting the first interview with a nurse and the development of the initial interview guide. Before commencing recruitment, study leaflets and posters were placed in the units to raise awareness of the study. Key gatekeepers (the nurse who was part of the education team, lead physiotherapists, charge nurses and hospital research team) assisted in identifying potential EM-MV activities and briefly introducing the study to potential participants. After a potential participant expressed a verbal interest, the researcher (Catherine Clarissa) followed up with them individually and sought their consent. Forty-five participants were invited to take part in this study with one person declining. The 44 recruited participants are summarised in Table 1.
Ethics
The study received a favourable opinion from the NHS Scotland A Research Ethics Committee (17/SS/0129) and was approved by the School of Health in Social Science Research Ethics Committee (NURS034). Different consent forms and participant information sheets for observations, interviews and focus groups were provided. Potential participants were given at least 24 hours to read the information pack before making a decision. All participants were made aware that they were free to withdraw from the study at any time or stage, without providing any reasons.
It was an ethical requirement to conduct all observations after the curtains were drawn around the patient and from a position in the corner without interfering with activities. Interviews were conducted in a private space in the vicinity of each study site (e.g. a consultation room) and participants were interviewed once. Focus groups took place in a meeting room adjacent to either unit.
Data Collection and Analysis
Summary of observations and participants.
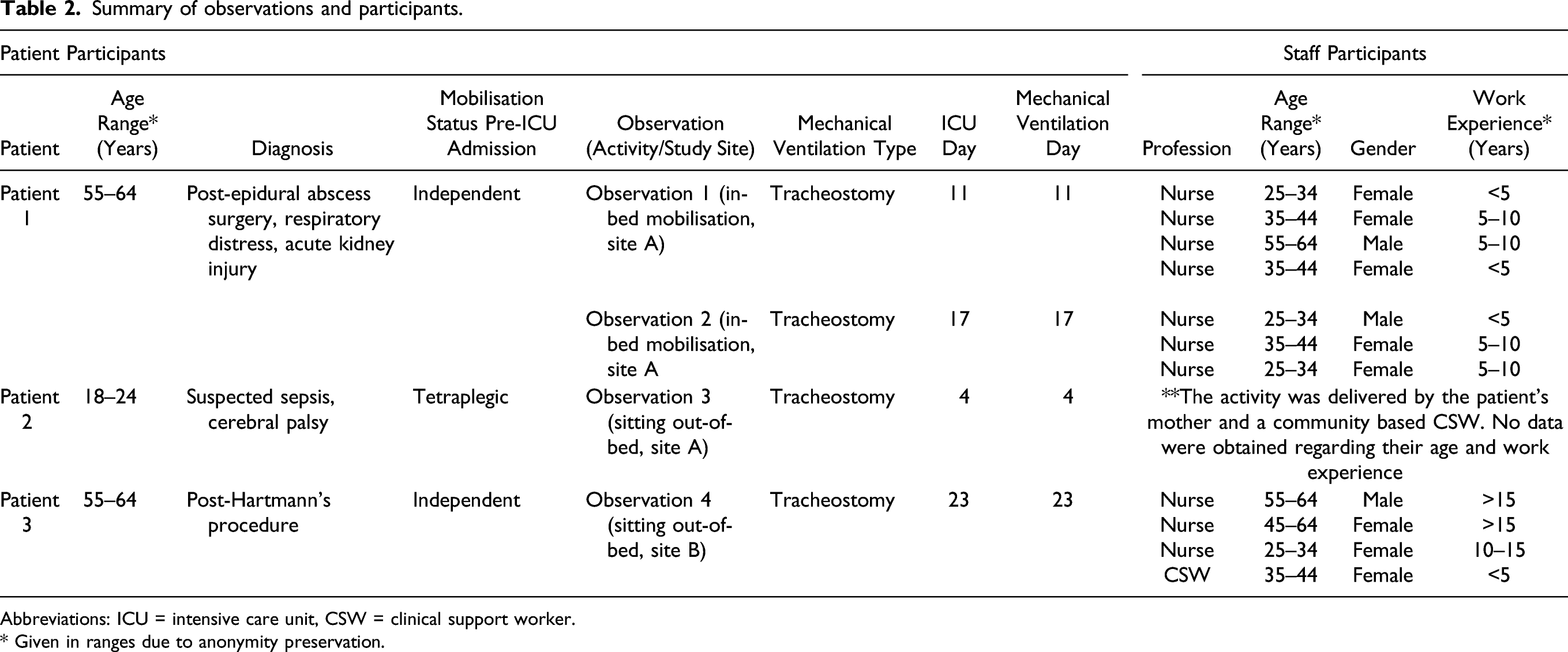
Abbreviations: ICU = intensive care unit, CSW = clinical support worker.
a Given in ranges due to anonymity preservation.
Summary of participants for interviews and focus groups.

Abbreviations: ICU = intensive care unit.
a Given in ranges due to anonymity preservation.
b The participant was not based in ICU.
Interviews and focus groups were audio recorded using password protected and encrypted digital voice recorder and transcribed verbatim by Catherine Clarissa. The interviews lasted between 27 and 82 minutes. The duration of focus groups was an average of 40 min. No participant feedback on transcripts and findings was sought.
Data collection and analysis is an iterative process including comparative analysis, initial and focused coding; memo-writing; theoretical sampling and theory building (Charmaz, 2014). NVivo12 was utilised to manage the generated data and to facilitate data analysis. The main focus at the initial coding stage were participants’ actions and the process of EM-MV: ‘What is the underlying process of this bit of data?’, ‘What are the actions of the participants in this process?’ At the focused coding stage, the initial codes were sorted and categorised analytically by contrasting similarities and differences. For instance, the initial codes performing the assessment, screening notes and using assumptions led to the development of focused code assessing individual patients.
Constant comparative analysis was continuously performed by comparing data across participants, ICU setting and incidents, which progressed towards the abstraction level of the analysis. For example, the sub-category defining patient status was constructed from the focused codes setting criteria for mobilisation, assessing individual patients, categorising patients and weighing benefits against risks. This sub-category, alongside with the sub-categories negotiating patient safety and performing accountable mobilisation, contributed to the construction of Managing Risks as the core category.
This study’s middle-range theory is grounded in data and developed with the inductive-abductive approach (Bryant & Charmaz, 2007; Charmaz, 2014; Reichertz, 2007). The initial coding phase is an example of induction in action. We employed abductive logic to develop the analysis beyond description towards theorising until data sufficiency was reached, the point at which new data did not result in further extensions and modifications of the core category (Dey, 1999). Memos were generated throughout the study, capturing assumptions for reflexivity by keeping track of decisions and thoughts. The reflexivity process enabled scrutinising the co-construction of knowledge, including shifting positions from being an outsider (as a doctoral researcher) to an insider (a critical care nurse by background) and power dynamics when interacting with participants.
Research Team
Catherine Clarissa was a female postgraduate research student at the time of the study with remaining authors as academic supervisors. Catherine Clarissa, Sheila Rodgers and Susanne Kean have backgrounds in intensive care nursing. Lisa Salisbury is a physiotherapist with a research and work background in ICU. Catherine Clarissa performed data collection and analysis and she did not know the staff nor work at the sites before study commencement. When undertaking data analysis, the emerging understanding and interpretation of the data was presented to the team, followed by critical discussion and questioning.
Results and Discussion
Results are presented by elaborating the core category and the middle-range theory that explicate the study phenomenon at a conceptual level first, continued with the sub-categories. The results and the concepts are discussed together, drawing on the logic of abduction (Charmaz, 2014; Tavory & Timmermans, 2019).
The Core Category: Managing Risks
A core category in constructivist GT accounts for the empirical data at the abstract level, providing explanation and understanding of the phenomenon in the study context (Charmaz, 2014). Through constant comparative analysis, Managing Risks was identified in this study as the core category. It reflects the core experiences of staff related to EM-MV and defined as the process by which participants make decisions about mobilising mechanically ventilated patients. Mobilisation only occurs when they perceive they can anticipate and manage risks associated with EM-MV. This core category integrates three sub-categories grounded in the data (refer to Figure 1): 1) defining patient status, 2) negotiating patient safety and 3) performing accountable mobilisation. The middle-range theory developed in this study.
The concept of risk was used to construct the middle-range theory in this study that outlines staff experiences and the processes involved in EM-MV (see Figure 1). Within the dynamic context of their ICU setting, the staff in this study engaged in Managing Risks by going through a recursive process of defining patient status and negotiating patient safety, before eventually moving on to performing accountable mobilisation. EM-MV would only be performed if staff participants were sure that the risks were feasible to be managed. They recognised the uncertainties in EM-MV due to the dynamic nature of patient conditions. Through defining patient status, staff participants ensured that only a suitable patient would be considered for mobilisation, that is, with minimal potential adverse events and when the EM-MV benefits outweighed the risks. Negotiating patient safety occurred in the context of planning safe EM-MV activities involving negotiation within the multidisciplinary team and the negotiation between staff and their patients or their relatives). When performing accountable mobilisation, participants maintain patient and staff safety by identifying potential risks and implementing preventative measures to mitigate them.
Managing Risks is conceptually linked to the concept of risk in healthcare, which has been associated with predictable and negative outcomes (Aven, 2012; Lupton, 2013). Risk management has become one avenue to ensure patient safety in healthcare delivery (Hammond, 2010; National Patient Safety Agency, 2004). In daily practice, healthcare practitioners need to use their judgement and decision-making in relation to interpreting and managing any risk in individual patient care (Greenhalgh, 2018; Heyman, 2009; Jacobs, 2000). Individual healthcare professionals are responsible for actively managing risks and avoiding harm to ensure safe and high-quality care in clinical practice (Corbett et al., 2011).
In the literature, risk management in healthcare is usually discussed on the system level focusing on improvement of organisation performance, for example, investigation and analysis of clinical incidents, monitoring the number of adverse events, reporting systems and approaches to safety (Heyman, 2009; Kuhn & Youngberg, 2002; Vincent & Amalberti, 2016). Vincent and Amalberti (2016) propose a model for a high-reliability approach to safety that can be applied in the team context in healthcare organisations. High reliability is referred to as ‘a flexible but prepared response of teams in the management of risk’ (Vincent & Amalberti, 2016, p. 29).
A link could be drawn between the risk management model with high-reliability approach presented by Vincent and Amalberti (2016) and the middle-range theory of this study. The model perceives that risk is inherent in the environment and cannot be fully predicted, although it is ‘known and understood’ (Vincent & Amalberti, 2016, p. 31). Vincent and Amalberti’s (2016) model of high-reliability approach can explain how staff participants perceived risks of EM-MV, as those can be foreseen, managed and prevented in order to maintain patient safety. In this sense, the approach can be applied to the uncertainty of EM-MV due to fluctuating patient conditions.
Vincent and Amalberti (2016) assert that the high-reliability model is suitable for professions who work in a team consisting of experienced individuals with different roles and expertise. Everyone in the team shares the same safety objective, is aware of the risk and will communicate any potential harm to the rest of the team if detected (Vincent & Amalberti, 2016) and this was evident in this study. This team approach is in line with the involvement of multidisciplinary staff in delivering EM-MV activities in this study. However, Vincent and Amalberti’s (2016) model does not reflect the social interactions presented in this study’s middle-range theory. The middle-range theory presented here offers a conceptualisation of EM-MV which takes into account the underlying interactions among individuals involved in the activity. These interactions were evident in this study, including the interplay between multidisciplinary staff in exchanging patient information when defining patient status and the complexity of interprofessional discussion when negotiating patient safety and performing accountable mobilisation.
Sub-category 1: defining patient status
Defining patient status is the process of assessing, comprehending, constructing and attaching meanings to a patient concerning their mobilisation status. When participants wanted to assign a status to their patients, they began by setting criteria for mobilisation at an individual level. Participants across disciplines (clinical support workers, nurses, physicians and physiotherapists) set patient criteria that must be met to decide whether a patient is suitable for EM-MV: physical criteria, physiological criteria and their own personal expectations. The data suggests that informal standards rather than agreed criteria are shared in the units, reflecting the diversity of participants’ understanding of EM-MV: ‘Locally, we would like to see the patients on a spontaneous mode’ (Physiotherapist 1, interview, site A). Some of the reported criteria match those observed in the literature. For example, participants expected patients to be able to engage in EM-MV, which is consistent with previous research (Parry et al., 2017; Williams & Flynn, 2013) and studies that excluded patients who were unresponsive to verbal stimulation from EM-MV activities (Bailey et al., 2007; Bourdin et al., 2010; Thomsen et al., 2008).
Participants (except clinical support workers) continued further by assessing individual patients against the criteria. They gathered all the information and knowledge about the patient concerning EM-MV from assessment or sourced from patient notes or through the social interaction between participants, such as a bedside discussion and the morning meeting. The interplay between the nursing and physiotherapy staff in exchanging patient information seems to suggest the complex nature of EM-MV assessment. If you’re unsure about a patient, you’ve maybe read notes and you think you’re not too sure if they do need us, we’d just be going up to the nurses and having a chat with them. Having a look at the chart which is at the end of the bed. Seeing how their oxygen is. Asking the nurses, “Do you need us to intervene? Do you need us to help you getting them up into the chair?” At that point we would then be stepping in to help. (Physiotherapy 1, interview, site B)
Following the assessment, participants used and comprehended the collected patient information to construct meanings to the patients as they categorised them into either eligible or not eligible for mobilisation. There was a shared understanding that most ICU patients were not eligible for EM-MV and they should be kept in bed due to their weakness, sedation levels and ventilation via an endotracheal tube: ‘But in here [the ICU], we would do the passive mobilisation for patients who are intubated and ventilated and sedated. We move them from side to side every four hours’ (Nurse 4, interview, site A). In contrast, participants felt comfortable with mobilising patients with a tracheostomy out-of-bed: ‘Generally, it’s the patient who has a tracheostomy, they get moved properly out of bed’ (Nurse 2, interview, site B). These findings show how EM-MV was perceived collectively in study settings.
The process of attaching meanings to a patient was reflected in staff’s decision-making, based on their individual clinical judgement as to whether or not the patient should be mobilised, by weighing between benefits against risks: ‘We’ll make sure we have them sitting up in the bed. Just helping prevent any community-acquired pneumonia and ventilation pneumonia’ (Nurse 1, focus group 1, site A). Several participants highlighted the importance of mobilising patients as soon as possible to maintain their muscle bulk and strength, which aligns with the evidence suggesting the benefit of EM-MV in improving the strength of limb and respiratory muscles (Chiang et al., 2006; Dantas et al., 2012; Martin et al., 2005; The TEAM Study Investigators, 2015). Yet, EM-MV with patients who were ventilated via an endotracheal tube was not common in this study. The use of an endotracheal tube was perceived as risky that could lead to serious adverse events if removed, such as death. So, somebody who’s on a lot of oxygen, where if there is a displacement of their tube, it would be disastrous. I think it’s not safe to mobilise or somebody’s on more than about 60% oxygen. If their tube becomes displaced, then they’re gonna desaturate very quickly and are likely to suffer a serious complication as a result of that. (Physician 1, interview, site A)
Death caused by tube dislodgement is not reported in previous work on the safety and feasibility of EM-MV. The reported adverse events included patient falls (Bailey et al., 2007), sudden drops or increases in blood pressure (Bailey et al., 2007; Davis et al., 2013; Liu et al., 2018), arrhythmias (Pohlman et al., 2010; Sibilla et al., 2017), oxygen desaturation (Bailey et al., 2007; Pohlman et al., 2010; Sibilla et al., 2017), patient-ventilator asynchrony (Pohlman et al., 2010; Sibilla et al., 2017), device removal (Pohlman et al., 2010; Sibilla et al., 2017), patient agitation (Pohlman et al., 2010; Sibilla et al., 2017) and patient intolerance (Liu et al., 2018). The incidence of adverse events in these studies is relatively small and unlikely to cause fatalities, yet participants in this study perceived that EM-MV may be associated with severe adverse events. This finding suggests that there is discordance between evidence and practice, influenced by participants’ risk perceptions of EM-MV, that focused on the immediate risk whilst overlooking the risks of not mobilising patients, such as ICU acquired weakness development. The following quote captures this notion. I know from the safety point of view that the risks are limited. The chances of things going wrong are fairly slim based on literature. But in reality, that’s a big pill to swallow, the responsibility of moving a patient with an endotracheal tube. I would argue if they can move all four limbs and getting out of bed, why are they still on the ventilator? I think, we certainly in this unit — the patients that are tubed probably aren’t well enough. They wouldn’t pass the risk assessment in terms of doing an active rehab goal. (Physiotherapist 1, interview, site A)
In essence, defining patient status appears to be participants’ first attempt at ensuring a safe EM-MV for their patients, which is aligned with the literature. Patient safety has been emphasised as one central element of recommended guidelines for mobilising critically ill patients (Gosselink et al., 2008; NICE, 2009; Sommers et al., 2015). International multidisciplinary ICU experts developed a consensus for EM-MV safety criteria (Hodgson et al., 2014). Both the recommendations and the consensus highlight similar points which were evident in this study, such as the importance of assessing patient condition for any potential risks, weighing up EM-MV benefits against risks before starting the EM-MV activity, and constant monitoring before and during EM-MV activities (Gosselink et al., 2008; Hodgson et al., 2014; Sommers et al., 2015). Findings from this study suggest that there is a tension between participants’ knowledge and attitudes regarding EM-MV. Whilst participants might be aware of the minimal risks of EM-MV reported in the literature, these risks were perceived individually and collectively in practice.
Sub-category 2: negotiating patient safety
Negotiating patient safety indicates that an EM-MV activity resulted from negotiations amongst ICU multidisciplinary staff, or between staff and patients, or staff and patients’ representatives. There was an ongoing negotiation amongst staff across disciplines (clinical support workers, physicians, physiotherapists and nurses), with mixed level of experiences (different durations of clinical experience), skills (have or have not mobilised a ventilated patient previously) and care priorities (different agenda of tasks for every professional). The negotiation was evident in the following aspects: timing, labour division, mobilisation goals and the preferences of patients and relatives.
The data revealed that EM-MV timing needed to be flexible and was often unscheduled due to the uncertain and dynamic nature of a patient’s condition. The most opportune time was when a patient was having sedation holds, using fewer medical devices, or tracheostomised. EM-MV scheduling would depend on how busy the unit is, the equipment, staff availability and their professional priorities. Many participants commented that EM-MV required a great number of staff and a considerable amount of time. Limited physical space and equipment was perceived as barriers to EM-MV. You need at least three staff to hoist the patient or move them to be safe. Or if the patient has drains and things, that can be a factor that stops people, because it will definitely be a barrier. They might not have enough chairs. If you’ve got five patients to get up but you only have four chairs. I know we don’t have a chair for every single bedspace. So, it can be that the equipment and staff could be a limiting factor certainly. And time. (Nurse 2, interview, site A)
Most participants (physicians, physiotherapists and nurses) regarded EM-MV as a low priority in the ICU amongst all their daily patient care tasks, with an exception for the clinical support workers because one of their primary responsibilities was mobilising patients. The issue of prioritisation was discussed in Focus Group 2, where the group went silent for a moment after the physician finished talking, suggesting that the rest of the group did not want to challenge him. Physician 1: I don’t know. I think we probably all think it’s a high priority. We ((sighing)) if you think what is obviously priority. If there are problems with their endotracheal tube, then the priority is the endotracheal tube. If they’ve issues with the ventilation, that concern is the priority. If they need some filter, that’s priority I think. But then you get something, like, I don’t know, the nasogastric tube, that couldn’t hold up to mobilisation. So I guess bits are often like the procedures, like Benton, like… Nurse 8: Line changes. Physician 1: Yeah, those kind of things will probably happen beforehand and then put the slots in after that. So not up at the top, but above from that.
This finding is not new; previous studies have suggested that EM-MV is regarded as a low priority in critical care, and conflicting care priorities are common in ICU multidisciplinary practice (Anekwe et al., 2019; Bakhru et al., 2015; Barber et al., 2015; Chaplin & McLuskey, 2020; D’Lima et al., 2018).
Personal care appears to be the nurses’ high priority. In all the observations, washing or bedmaking procedures preceded the mobilisation activities. Nurse participants in Focus Group 2 believed that they could mobilise patients if the unit culture changed and the morning shift nurses did not have to wash their patients: Nurse 8: No, we just need to discuss it further as a team, as a whole, and see if it’s something we want to culturally change within the unit. I’m sure we’ll embrace it. Nurse 4: I think night shifts could do more washes. Nurse 5: I was about to say that
Study data indicate there are differing opinions over the responsibility for EM-MV between professions, including staff roles and autonomy to make decisions or carry out the activities. Participants across disciplines had the autonomy to decide on EM-MV, except the clinical support workers: ‘Well I just do what I’m told’ (Clinical support worker 1, Focus Group 2, site B). Nurse, physician and physiotherapist participants all took individual professional responsibility, but at the same time shared this responsibility among the care team. I think the first start is from nurses and our judgement, what works better for the patient? And then if there’s any other issues, the physios can be involved and the doctors are always involved, of course. (Nurse 3, interview, site A) I don’t know if you could put a label on it but I suppose that probably is our responsibility, the physio’s responsibility, because we’re then being asked the complex questions and for support and advice when it’s not straightforward. (Physiotherapy 1, interview, site A) “Who does have overall responsibility? I’d like to say it’s a joint responsibility, but ultimately in the ICU the buck stops with the consultant so I guess the overall responsibility would be mine. (Physician 1, interview, site A)
Most participants accepted that EM-MV fell upon the physiotherapists’ expertise: ‘It's their, the physiotherapists, area of expertise and we should be able to trust them to go ahead and do what they think is appropriate’ (Physician 1, interview, site A). However, the power of EM-MV decision-making seems to remain with the physician participants, although nursing and physiotherapy staff still felt they had the autonomy to make decisions on EM-MV: ‘It [EM-MV] would start with the doctors’ (Nurse 4, interview, site A). The significant power of medical staff in EM-MV decision-making is apparent in some literature (Bourdin et al., 2010; Goddard et al., 2018). This is contradictory to most studies from the US (Bailey et al., 2007; Camargo Pires-Neto et al., 2013; Davis et al., 2013; Morris et al., 2008; Thomsen et al., 2008), the UK (McWilliams et al., 2015) and Australia and New Zealand (Berney et al., 2013) which highlight a mobility protocol that functioned as a standing order, where physiotherapists or nurses could make an independent decision without having to consult a physician.
A mobilisation plan would be devised to achieve certain goals and it could be initiated by an individual staff member from different professions, either from nurses, physicians or physiotherapists, and discussed with the multidisciplinary team. Nurses’ role was liaison, providing inputs and patient information related to EM-MV to the team. On my evening ward round, the nurses can say, ((mimicking voice)) "They sat out of bed but they were really tired" or "They sat out of bed and their blood pressure was not great". And then I can make a plan for the next day, you know, what we think is the suitable goal for the next day. (Physician 1, interview, site A)
The communication between staff could be through both verbal and written encounters. Verbal communication was conducted through handovers, ward rounds and meetings. Written communication was via bedside charts and electronic medical record system. We get access to the [electronic system’s name] notes so we can see whichever discipline written the notes. It could be the consultant. It could be one of the nurses. Anyone indicated they're struggling to clear their chest, struggling to keep their saturations up. There maybe increased oxygen and then they would be either signposting that they needed physio. (Physiotherapist 1, interview, site B)
EM-MV planning appears to be influenced by individual professional judgement. One nurse described how she would adjust the EM-MV plan based on patient conditions and what would work best for the patients, including the equipment required to mobilise them. We would ask them to squeeze our hands. Lift their arms, lift their hands up, their legs up as well just to see how the power in the legs and hands are progressing. And then I can adjust that to make our decision if they’re able to sit in a Barton chair, in a kind of recliner chair, or they just could use a Zimmer frame to just stand up. So it's not like the same pattern for every patient. It’s just a constant evaluation of the patient’s condition as well, and their strength, and they can get better from hour to hour. (Nurse 3, interview, site A)
Participants would engage with patients and relatives to discuss an EM-MV plan. Obtaining patient consent was reported as an avenue of ensuring patient autonomy to make decisions whether or not they wanted to undertake the EM-MV activity. From patients who had capacity, participants ensured that they obtained verbal or non-verbal consent. They can express their wishes. So, we would approach the patient and ask, “It’s time for your turn. Do you want me to change your position?” et cetera. And the patient can nod. They can squeeze our hands to say so and if they say yes, they like giving us a consent as well. (Nurse 3, interview, site A)
Participants often experienced conflicts with patients or their relatives when balancing autonomy and risks regarding EM-MV. Negotiation became the means to bring about reconciliation between staff and patients and between staff and patients’ relatives. Nurses appeared to be in the position of negotiating with patients, which has been noted in other studies (Kydonaki et al., 2020; Laerkner et al., 2019). Gordon [pseudonym] was using a tracheostomy, but could still communicate with the staff by mouthing the words using his lips. During the preparation, I noticed that they took a pat slide inside the room. I was standing outside the room and saw Gabrielle coming out and (the bedside nurse) asked Elsie (the staff nurse) to speak with Gordon, "I don't understand, can you help me?" Elsie came inside the room while pushing the chair and I followed her. I noticed that the patient was cursing, "I don't want to fucking do that" [sit in a chair]. Gabrielle replied, "it’s good for your chest.” The patient didn’t seem to care and said, “take it [the chair] away”. Elsie said, “Please don’t say that, it’s okay if you don’t want to do it. We can put you on your side.” After Gordon refused, Elsie took the chair back out. (Fieldnotes, observation 2, site A)
Participants would compromise with the patients or their relatives if needed as they wanted to respect their wishes. For example, in Focus Group 1, the participants explained at length some cases that they adjusted or settled the differences. Physiotherapist 1: Sometimes they’re more attended and prepared also. They would have a carer, some personal care… Physiotherapist 2: Those things can sometimes, kind of, be a bit of barrier as well. So perhaps this patient has a specific way of moving with their carers that they’ve known for a long time and they would have deteriorated and we need to get involved to establish whether we can do rehabilitation or whether that’s a new baseline that kind of anxiety around a new way of doing things in the unit and risk assessing what would be better, whether we let them do kind of their own way, but trying to make it as safe as possible. That can be quite challenging sometimes as well. Physiotherapist 1: We need to be careful not to be too risk averse Physiotherapist 2: Yeah Physiotherapist 1: So as much as we have a recommended way of helping people to mobilise with manual handling, we equally weigh it with patient’s choice and with care around the patient centred. Sometimes it’s worked for them for many years and it’s just not invoked with our current guidelines in NHS [board]. We need to be careful how we handle that because do we make that person’s way of mobilising very difficult just because of… Physiotherapist 2: Uh huh ((overlapping)) Physiotherapist 1: …a piece of paper? Or do we do what’s worked for them but we need to adjust how we then handle it.
In summary, negotiating patient safety reflects the ongoing negotiation amongst the multidisciplinary staff with mixed experiences, skills and care priorities; and between staff and patients or staff and patients’ relatives. The negotiation within the care team was about timing, labour division and mobilisation goals. The negotiation with patients concerned their decision and if the consent was given, the staff participants continued with discussing the patient’s preferences of the activity. The negotiation with patients’ relatives was about their involvement in performing the activity. The lack of staff professional boundaries is evident in our data, which can cause conflicts within a team (West, 2012). It seems that a key point raised from this finding is the necessity to clarify and articulate the roles and responsibilities of each profession in the EM-M, acknowledging ‘role distinctiveness and role interchangeability’ in their multidisciplinary collaboration (Nugus et al., 2010, p. 902).
Sub-category 3: performing accountable mobilisation
Performing accountable mobilisation is related to moving the EM-MV plan forward into action, in which participants across disciplines (clinical support workers, nurses, physiotherapists and physicians) perform the activities by ensuring that they could maintain accountability for both the involved staff and the patient. All professionals strived to protect patients from harm in different ways, depending on their roles and responsibilities. Participants, except clinical support workers, applied their professional views in assessing their patients and identifying risks related to patient condition to undertake EM-MV. And it’s like a risk assessment done in your head. This is what you do because you do it all the time. It works. So, it’s making sure the patient is safe. And like, getting out of the bed, just make sure they’re not gonna trip over, or there’s no water on the floor. We make sure the surroundings are gonna be safe for them getting out of bed into a chair. (Clinical support worker 2, interview, site B) In my head, done my risk assessment, there’s no reason why this patient shouldn’t get out of bed. But again, that isn’t about what’s wrong with the patient, that’s about doing our risk assessment around how they present at this moment. (Physiotherapist 1, interview, site A)
Participants carefully anticipated and foresaw these adverse events before commencing any EM-MV activities: ‘If we’ve had tube displacement, we would have 20 minutes to get him back into bed, get another tube down’ (Physician 1, interview, site A). The prevention measures would depend on the degree of perceived risk and the complexity of the procedure. For example, a participant explained about prone positioning. You always have to make sure you’ve got a senior doctor present. We’ve got the airway trolley ready. We’ve got our resus trolley ready as well. Just in case. (Nurse 3, interview, site A)
Another example is the observed activities of hoisting a patient from bed to sit in a chair. No physician was around and no emergency trolley was prepared. These differences suggest that prone positioning was perceived as riskier than sitting in a chair.
Patient discomfort was seen as barriers that needed to be managed before mobilising patients. Physical discomfort included pain due to a surgical wound, pressure sores and having not enough sleep or rest. Emotional discomfort was associated with lack of motivation or feeling upset. This discomfort was being relieved by addressing its sources, for instance, a pain relief was administered prior to the mobilisation activity. So that might be for some patients who have a big cut who are in a lot of pain, they would be lying in bed. “Can you sit up? Can you put the back of the bed up and actually sit up?” But with some, just getting up and sitting, it’s agony for them. You have to sort the pain out. You have to put them back down to rest with PCA [patient-controlled analgesia]. (Physician 2, interview, site A)
Staff safety issue was highlighted by several participants in this study across all professionals, except the physicians. Physicians in this study were unlikely to be involved directly in mobilising patients, as has been noted in previous research (Skinner et al., 2008). Only staff who were deemed fit could be involved in EM-MV activities. We need to make sure they’re fit to do that as well. So, if someone’s got a back pain or shoulder, we would always say to each other, ((mimicking voice)) “Listen, my back is really sore”, “I don't feel confident in doing that kind of safe mobilisation for that kind of patient.” We would find another person to replace that. (Nurse 3, interview, site A)
Confidence was required before a staff member engaged in any EM-MV activity. Staff who were not confident or deemed incompetent in mobilising patients were unlikely to take part in the activity. The feelings of anxiety and worry were identified in the data, related to the risk of harming patients, particularly in mobilising patients with endotracheal intubation. Well, when I first started to work here. It’s a long time ago, but I remember I was a little like, not panicking, but felt a little scared. Because you’ve not been working with that [EM-MV] before and nurse assistants, we don’t have much knowledge about it yet. (Clinical support worker 1, interview, Site B)
Staff anxiety and fear amongst nurses were also found in Curtis and Irwin’s (2017) and Bilodeau et al.’s (2018) studies, suggesting that they were common emotional responses for staff engaging with EM-MV. However, participants with more experience and knowledge regarding EM-MV appeared to be more confident and therefore less fearful, in performing the activity. In this sense, staff confidence appears to be linked to their competence in EM-MV. This finding corresponds to a study looking at Korean nurses’ perceived barriers and the educational needs of EM-MV (Kim et al., 2018). Kim et al. (2018) conducted a cross-sectional survey and distributed questionnaires to 151 ICU nurses in seven hospitals and found that nurses with more EM-MV experience reported fewer barriers to its practice.
In summary, performing accountable mobilisation reflects participants’ performance in delivering effective and safe EM-MV. Participants ensured patient safety by identifying potential risks and anticipating potential adverse events. They attempted to identify and eliminate sources of patient discomfort before EM-MV activities. Staff fitness and confidence were necessary to enable their involvement in EM-MV. As Finucane et al. (2000) demonstrated, there is an association between feelings and perceived risk and benefits: individuals with positive feelings towards EM-MV would perceive the risks as low and the benefits as high and individuals with negative feelings would perceive the risks as high and the benefits as low. More experienced staff could perceive EM-MV activities in a positive way and considered them as less risky and therefore displaying confidence and were more likely to perform EM-MV compared to less experienced staff. This finding may highlight the importance of providing experiential EM-MV training for staff. Simulation can be a training strategy to develop staff competency and confidence in delivering safe EM-MV as a team (Beaubien & Baker, 2004; Naik & Brien, 2013).
Implications for Research and Practice
This study’s key finding is that participants viewed EM-MV as involving a degree of risks to patients that should be managed, emphasising on the immediate risks such as adverse events resulting from the activity. This narrow focus can be problematic as the risks resulting from not mobilising patients may be overlooked, such as ICU acquired weakness that can persist years after ICU discharge (Herridge et al., 2011). Understanding of immediate and potential long-term risks is necessary to inform decision-making in ensuring that EM-MV is both safe and effective in improving patient outcomes. Further exploration of EM-MV decision-making process when weighing up between the benefits and risks of EM-MV is warranted.
The findings indicate a tension between participants’ knowledge and attitudes regarding EM-MV, reflecting a low uptake of research evidence being used to inform staff participants’ decision-making. Several strategies have been suggested to bridge the gap between research and practice, including visual cues, audit and feedback, educational meetings and materials, reminders, outreach and leadership involvement (Wuchner, 2014). Further work is required to establish the evidence of which strategies would work effectively within an ICU context.
Participants who perceived themselves as lacking in EM-MV experience reported feeling anxious and worried, indicating the association between confidence and competency. This finding may highlight the urgency of specific and tailored EM-MV training for new ICU staff. Nevertheless, anxiety was also evident in staff with years of experience. Therefore, continuous training and education related to EM-MV should be provided for all staff, including both new starters and existing staff.
EM-MV decision-making in this study was influenced by participants’ individual professional tasks and priorities in patient care, with unclear responsibility within the care team. There is a strong need to clarify and articulate the roles and responsibilities of each profession in the EM-MV multidisciplinary collaboration. Assigning a leader and having commitment towards EM-MV within the multidisciplinary team appear to be key to promoting its practice (Green et al., 2016; McWilliams et al., 2015). Improving communication is arguably imperative to achieve a shared understanding of EM-MV amongst the care team. Providing opportunities to facilitate interaction between the multidisciplinary team regarding EM-MV seems to be crucial and might be an avenue to promote collaborative practice.
Staff participants in this study discussed barriers of EM-MV that have been consistently reported in previous work, including lack of resources such as space and equipment (Bakhru et al., 2015; 2016; Barber et al., 2015; Megan E Harrold, 2013), sedation practice (Bakhru et al., 2015; 2016; Meg E Harrold et al., 2015; Megan E Harrold, 2013; Nydahl et al., 2014), competing priorities (Barber et al., 2015; Lin et al., 2020; Parry et al., 2017) and a lack of staff (Bakhru et al., 2015; 2016; Meg E Harrold et al., 2015; Holdsworth et al., 2015; Nydahl et al., 2014; The TEAM Study Investigators, 2015). They regarded that a culture change would facilitate EM-MV practice in their units. Further research to clarify the unit culture of EM-MV before implementing changes is thus recommended.
This study found that the interaction between patients and staff or between patients’ relatives and staff occurred during the planning and implementation stage of EM-MV. As nurses played an important role as a liaison in this interaction, developing effective communication skills seems to be essential in order to negotiate effectively with the patients and/or their relatives as well as with the multidisciplinary team. Therefore, training programmes for nurses in developing and improving communication and negotiation skills are recommended.
Strengths and Limitations
The scope of the theory developed from grounded theory research is substantive, which pertains to the study context (Glaser & Strauss, 1967). The middle-range theory developed in this study is practice relevant and thus useful for developing and evaluating complex interventions. The study’s strength is the rich data gathered from different methods, providing deeper insights into understanding the complex EM-MV process. However, it is important to note that our middle-range theory is limited to the study contexts.
Participants in this study appeared to have different understandings of what constitutes EM-MV which arguably affected its delivery in practice. While the best effort had been taken to observe different activities, the study only managed to observe in-bed mobilisation and sitting in a chair (refer to Table 2). Patients undertaking the observed activities were ventilated via a tracheostomy, which may indicate the typical mechanically ventilated patients being mobilised and the most frequent EM-MV activities performed across the study settings. No mobilisation of patients using an endotracheal tube was observed. Furthermore, the staff assisting the observed activities were predominantly nurses, with clinical support workers on several occasions. No physicians and physiotherapists were involved in the activities. This lack of physician and physiotherapist involvement during the observations is another limitation of this study and should be considered when applying the middle-range theory to other contexts.
Conclusions
This study explored the experiences of multidisciplinary staff being involved in EM-MV by employing a constructivist grounded theory methodology. The findings show that EM-MV is a complex intervention involving multidisciplinary healthcare professionals and a diverse patient population with varying acuity. The presented middle-range theory provides a framework that can be used to understand the social interactions between the involved individuals and explain why many mechanically ventilated patients are either mobilised or not mobilised during their ICU admission.
Footnotes
Acknowledgements
The authors thank all the research participants who graciously gave up their time to take part in this study and the ICU staff who kindly welcomed the researchers to the units.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of the first author’s PhD studies funded by Lembaga Pengelola Dana Pendidikan (LPDP) (Indonesia Endowment Fund for Education), grant number 20160222045521. The funder had no role in the design and conduct of the study nor the preparation of the publication manuscript. No other source of funding contributes to this study.