
Abstract
The use of World Health Organization’s (WHO’s) Safe Surgery checklist is an established practice worldwide and contributes toward ensuring patient safety and collaborative teamwork. The aim of this study was to elucidate operating room nurses’ and operating room nursing students’ experiences and opinions about execution of and compliance with checklists. We chose a qualitative design with semistructured focus group discussions. Qualitative content analysis was conducted. Two main themes were identified; the Safe Surgery checklists have varied influence on teamwork and patient safety, and taking responsibility for executing the checks on the Safe Surgery checklist entails practical and ethical challenges. The experiences and opinions of operating room nurses and their students revealed differences of practices and attitudes toward checklist compliance and the intentions of checklist procedures. These differences are related to cultural and professional distances between team members and their understanding of the Safe Surgery checklists as a tool for patient safety.
Background
In 2008, the World Health Organization (WHO) introduced the Safe Surgery checklist (SSC) as a strategy to improve patient safety and interprofessional teamwork during surgical interventions (WHO, 2009a). Based on the worldwide piloting and implementation of the SSC (WHO, 2016), research demonstrated that the SSC procedures contribute toward decreasing complications and deaths related to surgical interventions (de Vries et al., 2010; Haugen et al., 2014; Haynes, Berry, & Gawande, 2015; Haynes et al., 2009; Jammer et al., 2015).
The WHO implementation manual points out that the whole team is responsible for the safety initiatives and that the circulating operating room nurse (ORN) or any clinician participating in the operation can run the SSC safety checks (WHO, 2009b). The SSC is also mentioned as a standardized tool for team communication during surgical interventions with the aim to stimulate communication and diminish hierarchy (WHO, 2009b).
Challenges are found in terms of communication and collaboration in surgical teams—a hierarchical environment, team members not knowing each other, differing communication patterns and conflicting opinions on teamwork are some of the issues mentioned (Coe & Gould, 2008; Dharampal, Cameron, Dixon, Ghali, & Quan, 2016; Gillespie, Chaboyer, Wallis, & Fenwick, 2010; Rydenfält, Johansson, Larsson, Åkerman, & Odenrick, 2012; Rydenfält, Johansson, Odenrick, Åkerman, & Larsson, 2013). Attempts to improve communication have been initiated in hospitals parallel with the implementation of the SSC (Pugel, Simianu, Flum, & Dellinger, 2015; Vats et al., 2010). However, examples of challenging communication and hierarchical structure still exist (Bleakley, Allard, & Hobbs, 2012; Pugel et al., 2015).
According to Bleakley et al. (2012) and Bergs et al. (2015), structured interventions for team education and training are essential to succeed in using the SSC. The interventions may result in necessary changes in culture in surgical teams through learning and practice. On a wider scale, Russ et al. (2015) argued that team training can provide a strong safety culture, which can contribute to improving compliance with the SSC requirement.
A holistic responsibility for patient care is embedded in the culture of the nursing profession (International Council of Nurses [ICN], 2012; Olsvold, 2010). Among the caregiving tasks is the expectation that nurses must maintain an overview of patient care and follow-up treatment. These expectations are of both a professional and a moral nature and are important anchor points for nurses. Responsibility is described and perceived as a basic moral value in nursing. Nurses are obliged to consider both ethical and professional questions when performing caring tasks (Guglielmi, 2010). According to Solbrekke (2008), professionals sometimes have to compromise between what is considered ethically best practice and what is possible to achieve in different situations. In perioperative settings, compromises may be necessary, for example, in critical emergencies, in relation to cultural aspects of hierarchical positioning or to the different personnel who are executing the SSC.
Researchers have reported that ORNs play important roles in the surgical team, such as executing care tasks, attending to safety aspects and serving as coordinators (Gillespie, Chaboyer, Wallis, Chang, & Werder, 2009; Gillespie & Hamlin, 2009). ORNs prepare the patient for the surgical procedure, such as positioning, performing infection prevention measures, preparing instruments and assisting surgeons, all the while taking care of the vulnerable human being on the operating table. They coordinate the lists, communicate with other team members, help ensure compliance with the SSC, and monitor progress in the surgical procedures and report to management. They are present, circulating, and have the opportunity to initiate actions if needed (Rothrock, 2011).
Other studies highlight the need for changes in culture related to compliance with the SSC, teamwork, and communication in surgical teams (Aveling, McCulloch, & Dixon-Woods, 2013; Parmelli et al., 2011). According to Bergs et al. (2015), there are multifaceted challenges related to implementation of the SSC. They highlight different perceptions among the surgical team members such as the importance of the SSC safety aspects, collaborative teamwork, and communication.
The aim of this study was to elucidate ORNs’ and ORN students’ experiences and opinions pertaining to how the team executes and follows the SSC procedure to contribute knowledge regarding more deeply embedded challenges related to culture in surgical teams.
Method
Study Design
We chose a descriptive study design with qualitative data collection in focus group discussions. Focus group discussions is the preferred method when descriptions, meanings, opinions, and reflections are to be the sources of knowledge about a phenomenon or a specific situation or issue. According to Krueger and Casey (2015), one of the main purposes of focus group discussions is to promote interaction between the participants. Interactions, rather than individual interviews, can bring about even deeper and more consistent knowledge (Krueger & Casey, 2015; Malterud, 2012, 2017). In focus group discussions, opinions can be challenged, views can be contradicted, and new opinions can emerge through the encouragement of a variety of viewpoints. This presupposes an atmosphere that allows different perspectives to be voiced and become the object of discussion.
The focus groups were convened 2 times, based on the rationale that the first discussion could activate reflections and alertness pertaining to the issues and topics discussed in daily work in the operating department. It was thought that second focus group discussions would likely give the participants an opportunity to reflect more deeply and to discuss their awareness in terms of SSC compliance (Krueger & Casey, 2015; Malterud, 2012, 2017). During the second focus group discussions, no new issues were brought up. The time interval between the first and second discussion varied from 2 to 6 weeks because of practical arrangements, such as rotation schedules and personnel resources. In addition, focus group discussions are effective in reaching many participants at the same time and are less time consuming.
Setting
The research setting was a continuous-shift operating department at a large university hospital in Norway. The operating department serves approximately 12,000 surgical interventions per year.
The SSC was piloted in the orthopedic section during spring 2009. In late autumn, the same year, the SSC was implemented in all six sections in the operating department.
The surgical team consists of nurse anesthetists, ORNs, anesthesiologists, and surgeons. The circulating ORNs have the coordinating role during surgery. At the time of the focus group discussions during spring 2013, the formal responsibilities for executing the SSCs were incorporated and enacted in the hospital’s procedures. The procedure states that the whole team is responsible for executing the SSC even though the anesthesiologists are responsible for “sign-in” and the surgeons are to execute the “time-out” and “sign-out.” The procedure states that the directors of the surgical sections are responsible for ensuring that professionals are familiar with the procedure and are trained in using it.
Sample
The second author, head nurse of the operating department, informed potential participants about the study, its purpose, and progress plan and invited ORNs and ORN students at the operating department’s morning meetings verbally and later by email to participate in the study. The email included a separate sheet for consent. In addition, the second author occasionally approached potential participants directly and reminded them of the opportunity to participate.
ORN students are registered nurses with a minimum of 2 years of clinical experience before they can enroll in the training program for operating room nursing. They participated in the focus group discussions related to educational progress. They had completed two of the three-term long education program and had already signed work contracts after ORN graduation and were “enrolled” in the operating department. The students’ practice includes periods in all six surgical sections and this contributes toward providing them with an overview concerning compliance with the SSC.
During the education program, the students had lectures about the SSC, and they had experienced surgical interventions only after the hospital had implemented the SSC. Because of their knowledge and experience, it was thought that students’ participation might widen and supplement the discussions. However, several of the ORNs had experience both prior to and after implementation of the SSC.
Data Collection
During the spring of 2013, the third author conducted six focus group discussions. Three groups were convened twice for discussions of approximately 1 to 2 hours in duration. The third author, a professor employed at a university college in a different nursing discipline, had no direct connection professionally or personally with the participants neither before nor after the focus group discussions. An assistant was hired for technical assistance, to take notes and write summaries and was not included in the authors’ team.
The discussions took place in a meeting room adjacent to the operating department during work hours. During the discussions, the assistant operated the tape recorder, wrote summaries and read them aloud to the participants before closing the discussions. The participants were thereby given the opportunity to supplement the summaries if needed. This procedure was deemed to be a form of participants’ validation.
The focus group discussions started with an open-ended invitation to discuss experiences and opinions with the SSC in the surgical settings. An interview guide was used during the focus group discussions focusing on key issues, such as how the SSC was executed, reflections on compliance and what changes were needed. The discussions were recorded and transcribed verbatim by the first author and amounted to 124 pages of text.
Ethical Considerations
The study was performed in accordance with the Declaration of Helsinki (World Medical Association [WMA], 1964/2013). The ethical committee at the university hospital approved the study according to standard ethical criteria such as informed consent, confidentiality, and potential consequences for the participants (WMA, 1964/2013). The approval number of the mandatory report sheet version 1.0 is 12–049. The management of the operating department at the university hospital gave their permission to conduct the focus group discussions.
The participants were informed that participation was voluntary and that they could withdraw from the study at any time without giving any reason. Furthermore, they were informed that the data used in any of the presentations would be anonymized. The participants gave their informed, written consent.
Analysis
The text was analyzed by the three authors based on a qualitative approach for content analysis (Kvale & Brinkmann, 2009; Malterud, 2012, 2017). First, the text was read repeatedly to get an overall impression of what was discussed in the focus groups.
Next, the authors searched for meaningful units related to the issues in the interview guide. Then the meaningful units were condensed and coded into five subthemes and further abstracted into two main themes. Examples are shown in Table 2.
All three authors discussed the analysis process systematically until the findings and interpretations were consolidated and, in line with Malterud (2012, 2017), consensus was reached.
Results
Nineteen ORNs, 18 women and one man and two women ORN students participated in the focus group discussions (Table 1). Age was between 29 and 59 years; the average age was 47 years. Experiences in operating room nursing varied from 1 to 24 years. In the results and discussion sections, the students are referred to as ORNs due to the low number and anonymity.
Demographic Data of the Participants.

Note. OR = operating room; ORN = operating room nurse; OD = operating department.
In the presentation of results and discussion, the students are referred to as ORNs due to a low number.
Examples From the Analysis Process.
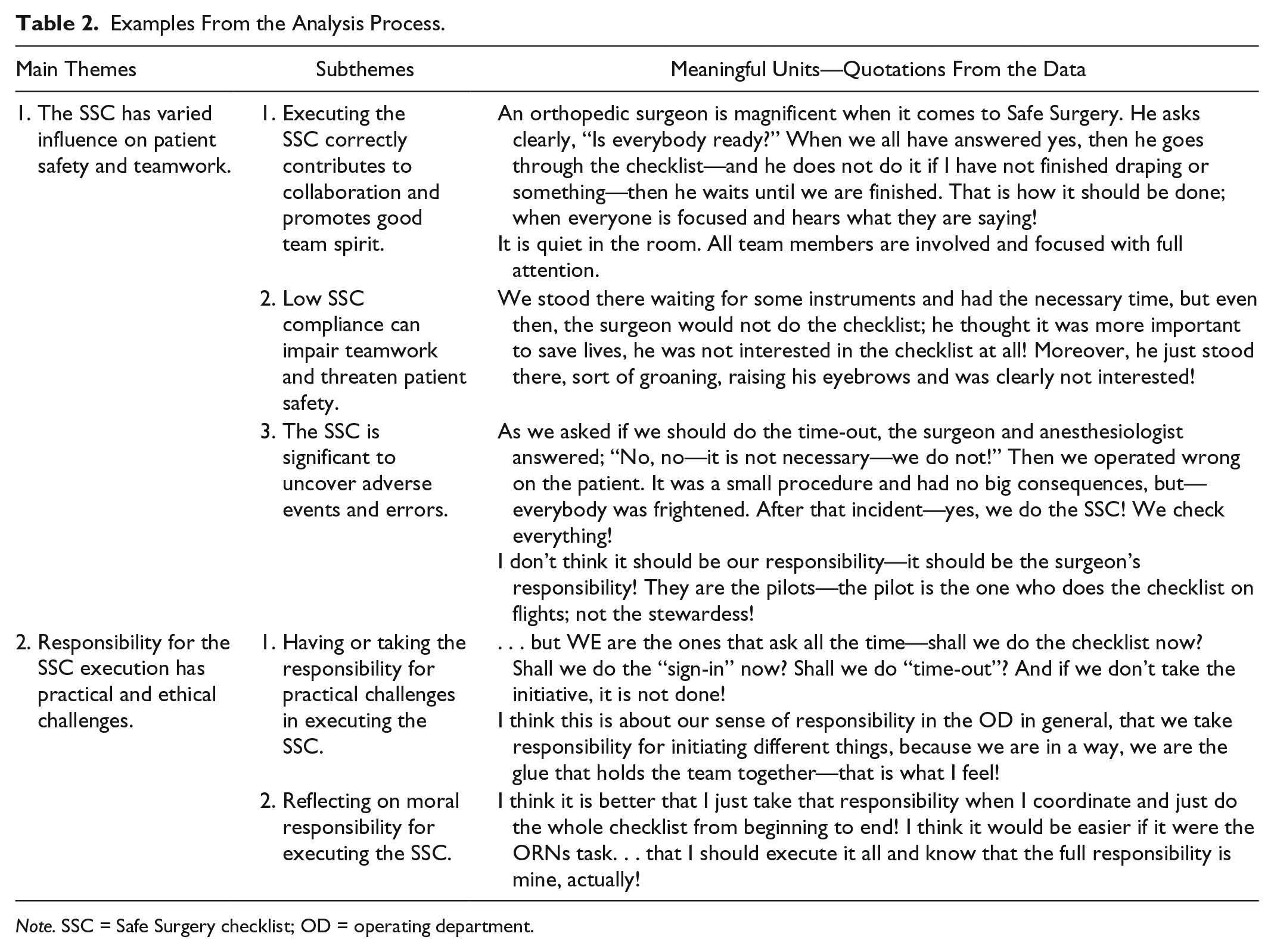
Note. SSC = Safe Surgery checklist; OD = operating department.
The results consist of two main themes and five subthemes. The first main theme was about the ORNs’ experiences of and opinions about the varied influence of the SSC execution on patient safety and teamwork. The subthemes were related to the impact of correct execution and high compliance on teamwork, the impairment of teamwork when the SSC was insufficiently executed or omitted and the significance of the SSC as a tool for patient safety.
The second main theme dealt with the practical and ethical challenges related to responsibilities for patient safety implicit in the SSC. The subthemes comprise the ORNs’ feelings of facing the dilemma of taking or not taking responsibility for implementing checklists and their ethical reflections on this dilemma.
Main Theme 1: The SSC Has Varied Influence on Patient Safety and Teamwork
Subtheme 1: Executing the SSC correctly contributes to collaboration and promotes good team spirit
Mutual respect
The participants discussed the importance of all team members’ efforts in terms of the patients’ outcome. The discussions revealed that team members who know each other by name and profession know what to expect from each other in terms of tasks, responsibilities, and performance during the surgical procedures. Moreover, mutual respect within the team contributed to everyone doing a good job—and as one participant mentioned, “It does something for your self-esteem, for your self-confidence.”
They discussed how treating a fellow team member with respect, and getting respect in return, made it easier to speak up, communicate concerns, and ask questions. It was important to admit that errors might occur and that admitting errors could promote openness and trust within the team. One participant mentioned, “I just want to mention that the checklist can’t guarantee that we don’t make mistakes—it’s just a means for making us better!”
Open communication
They concluded that when sharing crucial information, all team members were alert, and that open and confident communication contributed to patient safety. The participants also underscored that successful SSC execution depended on the persons’ presence during surgery. This was about their knowledge of the SSC as a consistent tool for patient safety, attitudes to collaborative teamwork and compliance, discipline in execution, and verbalization. They gave an example of what they assessed as a perfect way of doing the checks:
An orthopedic surgeon is magnificent when it comes to Safe Surgery. He asks clearly, “Is everybody ready?” When we all have answered yes, then he goes through the checklist—and he does not do it if I have not finished draping or something—then he waits until we are finished. That is how it should be done; when everyone is focused and hears what they are saying!
They discussed how following SSC procedure influenced the degree of compliance. The procedure was followed “to the letter”; it was quiet in the operating room, all team members were focused and gave the speaker their full attention, and all three phases were correctly executed. The participants agreed that when the checklists were completed correctly, the working environment benefited.
Subtheme 2: Low SSC compliance can impair teamwork and threaten patient safety
Poor teamwork
The participants discussed examples of low or lacking compliance. They stated that it was “person dependent (e.g., depending on the formally responsible physician)” and compliance varied. They mentioned examples when only one or a few team members attended the checks, when the checklist was recited like a muttered monolog or a conversation between the anesthesiologist and the surgeon without communicating to all team members. One participant exemplified,
Very often we have seen somebody walk to the board, “Let’s see here,” as if he was summarizing something, muttering, and “Oh yeah, we have done that!” “Did we? Was it the team that did it—or was it you? Alone?”
The participants discussed that SSC checks were done parallel with other tasks such as dressing for surgery or distributing instruments. They mentioned that phases were omitted; the physicians had forgotten or neglected to execute the SSC in spite of reminders from the ORNs. When reminded by an ORN, a performing surgeon answered “No! We don’t care!”
Unacceptable behavior
They discussed episodes of communication and behavior characterized by indifference, harassment, exclusion, and ridicule on the part of physicians during the SSC execution. One participant gave an example of unacceptable behavior during an emergency, but after the situation had calmed, the ORN reminded the surgeon of the need to execute the time-out. She said,
We stood there waiting for some instruments and had the necessary time, but even then, the surgeon would not do the checklist and he thought it was more important to save lives, he was not interested in the checklist at all! Moreover, he just stood there, sort of groaning, raising his eyebrows and was clearly not interested!
Another ORN responded,
It’s about the (physicians’) grumpy attitudes, I think. How management has told us to do this (the SSC) and then didn’t follow-up to ensure that it is performed, justifying the attitude that “It has no consequences if I don’t!” and causing surgeons to ask “Are you bringing this list now again!” and “No, it’s not important; it doesn’t matter!” and so forth.
The participants discussed that situations like these sometimes annoyed them or made them angry. Moreover, having to cope with such straining situations was negative for the work environment and could result in a lack of vitality and energy in the staff.
Varying levels of knowledge
The participants also described different levels of knowledge among the team members about the SSC procedures. They mentioned that some physicians did not even know that it was a routine procedure in the operating department, and instead of just executing it, they spent valuable time protesting and asserting that the SSC was time-consuming, and that it was more urgent to start the surgery.
Subtheme 3: The SSC is significant to uncover adverse events and errors
Discovering potential errors
The participants’ discussions of safety issues revealed multiple examples of adverse events or errors. They highlighted situations where the team members were aware and made an adequate effort to prevent adverse events that could have jeopardized patients’ safety. They discovered, for example, a lack of prescribed antibiotics or antithrombosis medication and a lack of registration of patients’ allergic reactions. During the “sign-in,” they discovered that the incision site was not marked and positioning was wrong.
The participants also discussed a general awareness in the team and the feeling that there had been some changes in attitudes:
An anesthesiologist one day said that we should do the checklist. “Oh, yes,” I said—“have you reached that level now? That was surprising.” and he answered, “Yes, we didn’t do it last week and I thought that the patient was another patient, and things nearly went wrong.” It’s a little amusing to hear that they can be introspective and see that OK, this (SSC) has a function!
Lack of information
Also discussed was the failure to communicate the planned surgical intervention to all team members, which made it challenging to prepare for the right equipment, plan positioning, and preoperative skin disinfection. In addition, the lack of such information could lead to adverse events and errors. One participant reported,
When we asked if we should do the “time-out,” the surgeon and anesthesiologist answered; “No, no—it is not necessary—we won’t do it!” Then we operated wrong on the patient. It was a small procedure and had no big consequences, but—everybody was frightened. After that incident—yes, we do the SSC! We check everything!
Furthermore, the sign-out procedure also proved that histological tissues to be sent to analysis had been incorrectly labeled, as one participant reported,
I asked the surgeon at the “sign out” if the histological tissue was marked correctly and he answered “Yes!”—even though he didn’t double check. It turned out that the patient’s name on the labeling was wrong. Yeah, there was nobody who—well—they just say “yes” without checking it again!
The participants agreed that executing the SSC was an important tool for patient safety. It did not guarantee flawless surgical proceedings, but it bettered the odds of detecting errors and acting preventively.
Main Theme 2: Responsibility for the SSC Execution Has Practical and Ethical Challenges
Subtheme 1: Having or taking the responsibility for practical challenges in executing the SSC
The ORNs’ responsibility for compliance
The participants discussed the responsibilities related to the SSC execution. They mentioned that despite a clear SSC procedure in the hospital, they often took responsibility for carrying out the SSC when compliance varied. They gave reminders or simply executed the procedures themselves. One participant reported, “After that last time I think I’ll just do it; I don’t mind who has the responsibility—when it’s not done, I’ll do it; get it done! Then I don’t get annoyed that it’s not done.”
Reasons suggested for low compliance with completion of SSC varied from forgetting to do the checks to directly refusing to do them. The ORNs discussed their strong feeling of responsibility and their commitment to getting the SSC done. One participant summarized “. . . but we are the ones that ask all the time—shall we do the checklist now? Shall we do the ‘sign-in’ now? Shall we do ‘time-out’? And if we don’t take the initiative, it is not done!” Others confirmed by saying “Yes!”
All participants had experienced physicians who reacted adequately to reminders and executed the SSC. However, they also experienced the opposite followed by unpleasant reactions.
Emphasize the formal responsibility
The participants discussed that it was somewhat of a paradox that they felt this strong responsibility to comply whereas the OTNs did not have the formal responsibility to do so. The participants had differing opinions in terms of giving reminders, taking over, or completing the checklist procedures themselves. Some of them cited patient safety as the most crucial issue; others stated that they refused to be “babysitters” or “watchdogs” for the physicians, whether they were anesthesiologists or surgeons, and the OTNs stressed that it was the physicians who had the formal responsibility. They mentioned that SSC completion was documented only in ORNs’ journal and was not included in the patient’s surgery notes. They discussed that mandatory documentation in the patients’ surgery notes could be the coercive measure to make the physicians take their responsibility. Several ORNs agreed to this and added that it might make the physicians accountable. One participant said,
They (i.e., the physicians) possibly would have taken Safe Surgery more seriously if they had to do a formal documentation and see to it that it was done. Only the nurses document it . . .If you read the surgery notes, there is nothing about executing the checklists! . . . If documentation was mandatory, you could read it in the patient’s surgery notes. Then you could see where the problem lies—whether it is the surgeon or the anesthesiologist’s fault, or that it is not done at all—and why it is not done!
Empowered ORNs
The participants also discussed that they needed courage and self-confidence to speak up to physicians when the SSC was insufficiently executed. They mentioned that some of the ORNs were tough, raised their voices, and called for attention; others did not, as the following quotation shows:
Tough—no, stand there shouting when an arrogant surgeon comes into the room and doesn’t care about the SSC—shall the ORN be tough and go for it anyway? No—well, I am tough and do it, but not everyone is.
They also stated directly who was responsible, as another ORN said, “I asked, shall we do the SSC? The answer was ‘No, we won’t!’ Well ok, I said, you have the responsibility here—so, it’s ok.”
They also mentioned that low compliance or refusal on the part of the physicians seldom was formally sanctioned by filing deviation reports, for example. Furthermore, writing these reports was viewed as another time-consuming task.
Subtheme 2: Reflecting on moral responsibility for executing the SSC
Shift in focus from patients to team members
The participants discussed their perceived responsibilities during surgery and for following up the SSC when compliance was insufficient. They mentioned that when team members discussed and even quarreled about why and how to execute the SSC; the focus was diverted from the patient to the team members’ opinions and reactions. This shift in focus was perceived to increase the risk of negative patient outcomes.
They also discussed whether they should take the full responsibility and execute the SSC or complete uncompleted checklists. Some ORNs felt that the safety issues were most important, and somebody had to act in terms of the checklist—namely, they themselves. They emphasized that they had seen hazardous consequences for the patients when the SSC was omitted. One of the participants said that she would like to have the formal responsibility for the SSC procedures. She said,
I think it is better that I just take that responsibility when I coordinate and just do the whole checklist from beginning to end! I think it would be easier if it were the ORN’s task . . . That I should execute it all and know that the full responsibility is mine, actually!
Others felt that those who were formally responsible should execute the SSCs. They argued that it was wrong that the nurses should have to take the responsibility and that a better strategy would be to give feedback to the physicians on an insufficient job with the SSC. They also discussed this matter by comparing the professional position of the surgeon to that of the ORNs on the team; as one said, “I don’t think it should be our responsibility—it should be the surgeon’s responsibility! They are the pilots; the pilot is the one who does the checklist on flights; not the stewardess!”
The participants discussed that the reason why they felt responsibility was that they were concerned for patient care and safety. They had experienced that the SSC procedures had revealed shortcomings, and the team together had achieved preventive actions. They claimed these experiences substantiate the claim that they needed to take the responsibility when compliance was low. One of the ORNs said,
I think this is about our sense of responsibility in the operating department in general, that we take responsibility for initiating different things, because in a way, we are the glue that holds the team together—that is what I feel!
They reminded each other that the responsibility for executing the SSC belonged to the whole team according to hospital’s procedure. Despite disagreements within the groups of participants on how to act, a majority took the responsibility to remind the staff, or they executed the checklist themselves when the physicians did not, even though this sometimes irritated or discouraged the nurses.
Discussion
Experiences of SSC Use on Patient Safety and Teamwork
According to the results, SSC execution influenced teamwork and patient safety in positive and negative ways. Furthermore, the SSC, when correctly executed, prevented adverse events and errors. There might be several reasons why the ORNs in general held themselves responsible for SSC compliance. Both professionally and morally, they are subjected to national legislation (The Health Personnel Act, 1999) and their ethical codex (ICN, 2012) that stipulate commitment to patient safety in treatment and care. Because of a correctly executed SSC, several adverse events and errors were prevented. This motivated ORNs to work at increasing compliance such as sharing information and promoting opportunities to be prepared if something unexpected should happen. In addition, situations that threatened patient safety appeared to prompt changes in attitudes toward the SSC, followed by better compliance. In these cases, compliance may have been motivated by ORNs anxiety related to experiences of the heightened risk of haphazard and unsafe surgical practices when the SSC is not used.
The ORNs had a professional understanding that the SSC was meant to be a team-unifying procedure, so that they worked to promote communication and collaboration parallel with other tasks. This can in turn generate predictability and a unified understanding of the SSC in surgical teams as highlighted by Gillespie, Chaboyer, Wallis, and Fenwick (2010; Gillespie, Chaboyer, Longbottom, & Wallis, 2010). Well-functioning surgical teams can build a culture of collaborative teamwork and patient safety (Gillespie, Chaboyer, Longbottom, & Wallis, 2010). In addition, Wagner (2014) drew lines between patient safety and safety for the personnel when reporting on a safety culture.
The results elucidated that when the SSC was insufficiently executed or omitted, it entailed a threat to patient safety and collaborative teamwork. Physicians were given the SSC in the form of hospital management’s demand, with sparse information. In addition, they were not included in the preparation and implementation processes. The SSC can represent a threat to the professional autonomy of physicians, who might maintain focus on professional, personal, and hierarchical power structures. The SSC was not their chosen responsibility and they received no formal sanctions if they did not participate in completing the SSC. Management’s demand and reminders from ORNs could annoy physicians and cause strained teamwork. This could have contributed to physicians’ refusal to use the SSC. Bergs et al. (2015) highlighted physicians’ hierarchical positioning, lack of knowledge, and lack of ownership as barriers in the implementation processes and the SSC execution.
Moreover, ORNs hold the lower position in the hierarchy, and it can be challenging to speak up to a surgeon who refuses to run the checklist or reacts with hostility to reminders to do so. When exposed to such reactions, ORNs can become stressed, reserved, and reticent. Furthermore, disruptive behavior on the part of physicians might contribute to resisting change, preserving the entrenched hierarchy, postponing development in teamwork, and widening the distance between the professions. These situations were seldom discussed and negative experiences were left unaddressed. Cochran and Elder (2014, 2015) and Higgins and MacIntosh (2010) highlighted similar findings pertaining to surgeons’ disruptive behavior in perioperative environments, indicating that challenges in communication are often embedded in the hierarchical culture. In addition, when ORNs perceived the writing of deviation reports as time-consuming and therefore did not write them, they gave the operating department’s management no grounds for pursuing the matter.
Low compliance or omission on the part of the formally responsible physicians was an important factor influencing ORNs’ perceived commitment to the SSC procedures. They compensated for the fact that physicians did not take the responsibility and might thereby have been complicit in concealing noncompliance with the SSC requirement. By not taking actions on the SSC, the risk of jeopardizing the patients’ outcome is evident. Several studies reveal that the rates of complications and deaths related to surgery decreased when the SSC was executed (de Vries et al., 2010; Haugen et al., 2014; Haynes et al., 2015; Haynes et al., 2009; Jammer et al., 2015).
Our results highlighted different levels of knowledge and understanding of the SSC among team members. This could be related to lack of information or discussions on procedures, few or no peers encouraging the teams, no time for training or pure ignorance. According to Bate (2000), changing culture entails a change in thinking. New ways of thinking must come before or simultaneously with organizational, structural, and personal change. Parmelli et al. (2011) highlighted that there is no generalizable strategy for changing culture in health care settings. Furthermore, they mentioned the importance of managements’ involvement and support to change the local culture.
Implementation of the SSC must be regarded as a change of culture. A new way of thinking requires education, team training for all members, discussions, and shared understandings of implications and must involve the employees. These elements were often ignored at the time of SSC implementation. According to Gillespie, Chaboyer, Wallis, and Fenwick (2010), low SSC compliance can be related to different perceptions of the SSC intensions within the team, lack of leadership, lack of management support, and no team discussions about purpose and how the checklists are to be executed. An explanation of low compliance in our operating department might relate to lack of information and knowledge, especially among physicians. In addition, the fact that there were no arenas for joint information and discussions about challenges might have been a factor in insufficient SSC execution. Prioritizing information and having discussions require time. Time schedules are tight in the operating departments. By investing in team education and training, teamwork and safety issues could profit. The value of prevention rather than treatment can be addressed as well as strengthening teamwork (Bergs et al., 2015; Conley, Singer, Edmondson, Berry, & Gawande, 2011; Parmelli et al., 2011; Pugel et al., 2015). In the wake of the SSC implementations, it is highlighted that the checklist itself is no guarantee of safer surgery. It is the way the SSC is understood and executed that matters. Patients’ safety is not anchored in the procedures themselves, but in communicating crucial aspects of surgery within the team and acting according to them (Bosk, Dixon-Woods, Goeschel, & Pronovost, 2009; Dharampal et al., 2016; Leape, 2014; Rydenfält, Ek, & Larsson, 2013).
The results showed that one argument physicians voiced was that execution of the checklist was time-consuming and caused delays. This argument is contrary to the results of Thomassen, Brattebø, Heltne, Søfteland, and Espeland (2010) who noted a balance between safety issues and efficiency. When SSC routines and compliance are solid, execution optimized safety and time efficiency.
Ethical Dilemmas on Responsibilities and Patient Safety
The results showed that the ORNs felt a strong responsibility for the patients’ safety, accompanied by practical and moral obligations. The ORNs reflected over why they perceived this strong moral responsibility and often executed the SSC even though the responsibility formally belonged to the physicians. This may reflect a commitment to the ethical guidelines for nurses (ICN, 2012), which provide guidance on making decisions when faced with practical and ethical dilemmas, such as insufficient SSC compliance. Furthermore, in line with Wellard and Heggen (2011), nurses act upon tasks forgotten or even ignored by other health care workers because of nurses’ holistic perspectives on patient care and their perceptions of the importance of contributing to the work environment. Moreover, in line with Olsvold (2010), ORNs acted on the SSC as if it is “everybody’s” responsibility in the operating department. The fact that ORNs carried out the SSC procedures can be related to an ethical and practical conviction in favor of patients’ safety, even though they had different opinions as whether it was the right strategy to take. Executing the SSC themselves might also be inspired by the nurses’ integrated professional and moral perception of responsibility (ICN, 2012; Olsvold, 2010; Solbrekke, 2008; Wellard & Heggen, 2011) to avoid exposing patients to potentially adverse events and errors. However, this may represent an ethical dilemma for nurses. If they choose to remind the responsible physicians and demand that the SSC be done, it could result in conflict in the team. Focus is taken away from the patient, and a hostile atmosphere could arise. If ORNs choose not to act, they condone malpractice and jeopardize patients’ safety. A professional nurse’s disclaimer of the ethical aspect of responsibility could be result in inner moral conflict, which in itself can result in feelings such as a bad conscience, shame, guilt, and anger (von Post, 1998).
To act upon ethical dilemmas demands that ORNs have professional and personal courage, an ability to present professional argumentation and the stamina to promote patients’ rights, implicitly the safety protected under the SSC requirement. ORNs who were willing to set aside thoughts about possible hostile reactions from physicians and promote the SSC procedures, appeared to be responding to their ethical duty to take care of the patients during surgery. They had to rely on their competence, speak up for patient safety, and stand firm in discussions and challenges in the surgical team.
Sandelin and Gustafsson (2015) found in their study that ORNs were silenced and became reticent in strained situations, and they spoke only when addressed or they confronted the surgeon with an admonition that hostile behavior was not acceptable. Johnson and Kimsey (2012) highlighted speaking up as most crucial in patient safety work and suggested an organized team-training course to prepare the members for challenging situations.
The results revealed that quality in executing the SSC requirements varied. One reason for varied quality might be that other professionals in the surgical team rely on the ORNs, as employees in the operating department, to take overall responsibilities including the SSC procedures along with patient-caring tasks and tasks related to “invisible” responsibilities (Olsvold, 2010; Wellard & Heggen, 2011). This can generate a “laid-back” attitude among other team members, who might think that the SSC procedures will be executed anyway. Furthermore, when ORNs take the responsibility for SSC procedures, it ensures patient safety, although it might undermine WHO’s objective to develop teamwork and communication (WHO, 2009a).
Limitations
There are several limitations in this study, especially regarding recruitment and sample. The second author asked ORNs and students to participate by open invitation, by email, and by giving reminders in passing. This way of recruiting entails both benefits and biases. The researcher’s familiarity with the ORNs’ knowledge and skills enabled recruitment of a sample representing several sections in the operating department. However, it was possible that ORNs who were approached directly may have found it difficult to say no and participated in the study despite feeling uncomfortable about doing so. Although delegate recruitment by a third party would have minimized this, during data collection, participants did not display any discomfort and appeared willing to share their experiences. Participants were asked to keep issues discussed in the groups confidential. However, the authors could not guarantee that participants maintained confidentiality.
Convening students with their mentors and future colleagues in focus group discussions can be challenging. They might feel that their brief operating room practice is a limiting factor; they could have few reflections to offer and become silent. Even so, participating students can provide broader theoretical knowledge about the SSC procedures in the discussions. Therefore, we invited students to participate in this study as future colleagues and to involve them in the operating department’s projects. Only two ORN students participated in the focus group discussions. To diminish the chances of revealing the students’ identity, they are referred to as ORNs in the results and discussion sections.
This study was conducted by one discipline (nursing) and limited to the experiences of ORNs. Research focusing on physicians is needed to fully understand their experiences in using SSCs. Finally, the first and second authors are originally ORNs. This may have contributed to professional “blindness” and in turn might have been instrumental in their overlooking important elements in the analysis process. Despite this, our results are in line with what other studies reveal (Gillespie, Chaboyer, Wallis, & Fenwick, 2010; Rydenfält et al., 2012; Sandelin & Gustafsson, 2015). This gives reasons to assume that our results are trustworthy and transferable in a comparable context both nationally and internationally.
Conclusions and Implications for Practice
The aim of this study was to elucidate ORNs’ and ORN students’ experiences and opinions pertaining to the execution of and compliance with the SSC requirements. Thus, this study has contributed to adding knowledge related to culture in surgical teams.
The SSC, when conducted correctly, represents an important tool for patient safety. By executing the SSC, the team was alerted to preventing jeopardizing situations and made surgical interventions more predictable, less time-consuming and more effective. The ORNs’ overall concern was the SSCs execution itself, not who executed the checklist.
The ORNs in this study had a shared understanding of the SSC as a positive teamwork-promoting tool. Well-functioning teams encourage mutual respect and trust, which are essential values for all team members doing a safe job for the patient. This also strengthens the safety culture in the working environment, and it contributes to job satisfaction among team members.
The study showed clearly the consequences of insufficient implementation of the SSC. Furthermore, it revealed a gap between the hospital’s procedures and practice related to responsibility for the SSC execution. Cultural change is not a haphazard task, but needs conscious preparation, repeated education, personal as well as shared accountability in surgical teams, follow-up and audit by leadership. Issues to be addressed in practice include getting team members to agree on a procedure for executing the SSC that focuses on the patient safety and diminishes single professions’ different ways of understanding. Setting aside time to consolidate a common understanding of responsibilities might be a strategy for better SSC compliance. Until the SSC execution is a customary practice, the hospital’s management must demand and make the responsible professions accountable for compliance.
ORNs have an important function in the surgical team. However, they need to acknowledge their competences and take their rightful place as equal members of the team. In addition, they must speak up and take responsibilities for patient safety, encouraged and supported by the operating department’s management.
To acquire further knowledge and understanding of the SSC issues, similar studies at other operating departments would be interesting, with a view to comparing results. It would also be appropriate to investigate the experiences and opinions of nurse anesthetists and physicians in surgical teams.
This study has yielded important insight into the ORNs’ experiences and opinions of patient safety, teamwork, responsibility, and safety culture. It provides grounds to conclude that patient safety issues and teamwork are coequal with taking the responsibility for SSC compliance.
Footnotes
Acknowledgements
The authors thank the operating room nurses and operating room nursing students for participating in the focus groups, for generously sharing their experiences and reflections on the execution of the SSC. They also thank Assistant Professor Kirsten Braaten for technical assistance during the focus group discussions and Director of the operating department Anne-Grete Moen at Akershus University Hospital for facilitating the study. Their gratitude also goes to librarian Lilja Berg at the Oslo and Akershus University College of Applied Sciences for invaluable support with the EndNote library.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from Oslo and Akershus University College of Applied Sciences in Norway. The purpose of the funding is to finance research and professional development.