
Abstract
Talking to friends, family, or peers about health issues might, among other things, increase knowledge of social norms and feelings of self-efficacy in adopting a healthier lifestyle. We often see interpersonal health communication as an important mediating factor in the effects of health campaigns on health behavior. No research has been done so far, however, on factors that influence whether and how people talk about health issues without being exposed to a health campaign first. In this exploratory study, we interviewed 12 participants about their communication behavior concerning six different health themes, like smoking and exercising. The results suggest that at least four types of interpersonal health communication can be distinguished, each influenced by different factors, like conversational partner and objective of the conversation. Future research should take this diversity of interpersonal health communication into account, and focus on designing health campaigns that aim to trigger dialogue within target populations.
Introduction
Researchers in the field of health communication emphasize the importance of talking about health issues (Duggan, 2006; Southwell & Yzer, 2007, 2009). In classical theories such as the two-step flow theory (Lazarsfeld, Berelson, & Gaudet, 1944), the diffusions-of-innovations theory (Rogers, 1983), the social representations theory (Moscovici, 1984, 1988; Moscovici & Hewstone, 1983), and theories on word-of-mouth communication (Matos & Rossi, 2008), interpersonal communication has been identified as a major factor in spreading information. Talking about health issues within informal social environments, such as with friends and family, might affect health behavior determinants in several ways, over and above mere information spreading. Talking about a health issue might result in a higher risk perception (Morton & Duck, 2006); it might positively influence attitudes regarding health behavior (Geary et al., 2007), lead to the discovery of norms that are prominent in the social environment (Hornik & Yanovitzky, 2003), provide people with social support (Choudhury, Erausquin, Park, & Anglade, 2015; Yeshua-Katz & Martins, 2013), or help reducing possible stigmas and taboos by loosening normative constraints (Botta & Pingree, 1997; Pettifor et al., 2004; Southwell & Yzer, 2007).
A substantial number of mass media health messages are received in an interpersonal context (Valente & Fosados, 2006), facilitating immediate interpersonal communication. Interpersonal communication is often seen as an important mediating factor in the effects of health campaigns on actual health behavior. Van den Putte, Yzer, Southwell, De Bruin, and Willemsen (2011), for instance, found that talking about an antismoking campaign influenced the intention to quit smoking. Various studies have emphasized the need for public health campaigns to focus specifically on triggering conversations (Morgan, 2009; Surkan, Dejong, Herr-Zaya, Rodriguez-Howard, & Fay, 2003; Van den Putte et al., 2011).
Jansen and Janssen (2010); Lubinga, Schulze, Jansen, and Maes (2010); and Lubinga, Jansen, and Maes (2014) have studied factors that determine whether or not people are inclined to talk when triggered by a specific health message. However, little is known about what interpersonal communication on health issues (interpersonal health communication in the rest of this article) looks like when it occurs naturally, that is, without being triggered by a health campaign. We do not know in which circumstances people talk about health issues, or how, why, and with whom. The mechanisms underlying this behavior might be very different, for instance, when talking to children about smoking compared with when talking to friends about exercising. For some, alcohol might be a more relevant topic to discuss than healthy eating, and some might find it more difficult to talk about safe sex than about safe tanning.
To be able to influence people’s behavior, in this case regarding interpersonal health communication, we need to maximize our understanding of why a target population would or would not engage in this behavior (Yzer, 2008). It is therefore important to identify factors that influence whether or not people talk or intend to talk about health issues, and why (Goldsmith & Miller, 2014; Southwell & Yzer, 2009). In the current article, we aim to explore the factors that influence naturally occurring interpersonal health communication.
Communicative Objectives
When interacting with others, people always pursue one or more objectives or goals (Clark & Delia, 1979). In that sense, interpersonal communication can be seen as reasoned, goal-oriented behavior (Southwell & Yzer, 2007, 2009); Clark and Delia (1979) identified three types of objectives that can explicitly or implicitly be distinguished in every communicative situation: (a) instrumental objectives, which focus on “the task of the communicative situation”; (b) interpersonal objectives, “involving the establishment or maintenance of a relationship with the other(s)”; and (c) identity objectives, “in which there is management of the communication situation to the end of presenting a desired self-image for the speaker and creating or maintaining a particular sense of self for the other(s)” (p. 200).
Clark and Delia (1979) indicated that multiple objectives can be prevalent in the same communicative situation. In Goldsmith’s (2001, 2004) “normative theory,” it is assumed that within a certain context, people often have multiple objectives at the same time that can conflict. This can create a complex communication situation (O’Keefe, 1988). How the hierarchy of different types of communication objectives is organized is not always clear-cut. Sometimes one has to weigh the need of communicating something effectively against the likelihood of damaging the relationship with the other person (DeTurck, 1985; Sillars, 1980). In interactions, the concept of face, or “the public self-image that every member [of a society] wants to claim for himself” (Brown & Levinson, 1987, p. 61), is particularly relevant. When making requests, for instance, people want their request to be efficacious, but they also want to maintain the face of the conversation partner, as well as their own face (Dillard, 1990).
Goffman (1959) compared participants in interaction with actors on stage, who are constantly aware of the presence of an audience in the things they do and say. He described how individuals in interaction engage in “impression management,” to create a desired impression, or face, of themselves, and also how individuals in interaction work as a team to help each other maintain face (Goffman, 1959, 1967); participants in interaction are thus continually doing “face work” to protect their own face and that of the other participants (Goffman, 1955). Dillard, Segrin, and Harden (1989) indicated that in a communicative situation, one might pursue interaction goals, concerned with social appropriateness, impression management, and avoiding face threats to all participants in the interaction. The concept “face” can be of importance for both interpersonal objectives, concerned with the relationship between the participants of the interaction, and identity objectives, concerned with managing the self-image of the speaker.
Objectives in Interpersonal Health Communication
The distinction between instrumental, interpersonal, and identity objectives discussed above can also be applied to interpersonal health communication. One might, for instance, want to instruct a child how to put on sunscreen, or wish to persuade a friend to quit smoking. In these examples, instrumental objectives are important: The main objective of the communicative act is to help the other person improve his or her health. Furthermore, in interpersonal health communication, objectives concerning the self-image or the relationship might be at play, which can conflict with the instrumental objective of, for example, persuading someone to change his or her smoking behavior. When addressing sensitive health issues, like safe sex, for instance, one might believe it is more important to maintain one’s own face and that of the conversation partner, thus preventing possible damage to the relationship, rather than effectively bringing up the health topic (Allen, Emmers-Sommer, & Crowell, 2002). In other words, in some cases, people might believe it is more important to maintain a good relationship over the short term than to prevent health risks over a longer term (Cline, Freeman, & Johnson, 1990).
Research Question
As described above, we aimed in the present study to explore factors that influence interpersonal health communication of people before they have been exposed to a health campaign. We did not have a strict hypothesis, and therefore speak of an “explorative study” in this article. We aimed to gain more knowledge about the kinds of conversations people have about health issues and the reasons they give for (not) having these conversations, for the purpose of providing greater insight into both health communication research and practices regarding factors that should be taken into account when designing health messages that aim to trigger conversations. As Southwell and Yzer (2007) have stated, “To harness motivations [for conversations] for campaign purposes, we need frameworks with which to predict conversational occurrence.” With the current article, we attempt to contribute to such a framework. To that end, we formulated the following research question:
Method
To explore the factors that influence whether or not people talk about health issues, we carried out a qualitative descriptive study by means of conducting in-depth interviews (Elliott & Timulak, 2005). This method is particularly useful for new areas of research, such as the one described in this article, because it enables researchers to extract meanings that are embedded in people’s experiences, which might otherwise not be brought out (Yeshua-Katz & Martins, 2013). The study protocol was approved by the institutional ethical committee (CETO) of the Faculty of Arts of the University of Groningen, The Netherlands.
Participants
In this study, we aimed to get a broad view on (self-reported) communication behavior. To that end, we selected 12 Dutch participants varying in sex, age, and level of education: Six participants were men and six were women; six participants were younger than 25 and six were older than 50; six participants had a low level of education and six had a high level of education. 1 With this composition, we could make comparisons between maximally varying groups of participants in our data analysis. We used no specific criteria for participant selection. We recruited participants through a snowball method, starting from our personal network, and in this way, we composed a convenience sample. We contacted participants personally by email or telephone, and asked whether they wanted to participate in the study. All received a financial compensation of 10 euros (about US$11) for their participation, and provided informed consent prior to their participation.
After conducting and analyzing 12 interviews, we identified four types of communication behavior, which are the main focus of the rest of this article (see the “Results” section). These four types of communication behavior were confirmed in the rest of the interviews, indicating thematic saturation.
The Interviews
All 12 interviews were conducted, audio-recorded, and transcribed verbatim (following, for example, Edwards, Donovan-Kicken, & Reis, 2014) by the same trained interviewer. The interviewer conducted all interviews in the homes of the participants. The interviews were semistructured and contained questions regarding when, why, and with whom participants actually talked, or would talk, about the health themes: “(drinking) alcohol,” “healthy eating,” “exercising,” “smoking,” “safe sex,” and “safe tanning.” We deemed these themes relevant to a wide audience when talking with different conversation partners, such as friends, family, or romantic partners. Alcohol, for instance, is a theme that can be discussed among adolescents when drinking together, but also between parents and children when talking about the dangerous consequences of excessive drinking.
In every interview, we addressed a number of questions for each health theme: “Do you ever talk about this theme? Why, with whom, and in which situations?” and “Would you talk about this theme? Why, with whom, and in which situations?” In this way, we ensured that we addressed both the self-reported communication behavior and the intentions of participants to talk about health issues. 2 Furthermore, we asked follow-up questions that picked up on answers that participants gave, to gather more information on their communication behavior. An example of a follow-up question was, “And did people talk to you about this afterward?” in response to a participant sharing an anecdote about drinking too much alcohol when going out. During the interviews, the interviewer invited the participants to talk about the issues addressed in the interview in their own words and manner. In a few cases, participants needed some encouragement from the interviewer to talk more extensively about a theme.
We removed any information linking to the identification of participants, for example, names, from the transcripts. The mean duration of the interviews was 28 minutes (SD = 9 minutes). Each health theme was addressed separately in each interview, resulting in a total of N = 72 “interview sections” that could be analyzed. We conducted the interviews in Dutch and translated the examples discussed in the rest of this article into English. 3
Analysis of the Interview Data
We analyzed the interview data using basic elements of grounded theory (Strauss & Corbin, 1998). Two coders were involved in each of the coding steps. 4 The interview data were first divided into codable information units, consisting of the response of each participant to each interview question or each follow-up question, to preserve the context and meaning of participants’ utterances (cf. Helme et al., 2011). Next, in the “open coding” step, the information units were labeled according to the information they contained. Examples of labels were “easy topic of conversation” or “afraid to address drinking behavior of friend.” The final dataset consisted of N = 462 labels, which were then categorized in the “axial coding” step. This coding step was performed by discussing and comparing labels in multiple meetings over a period of several weeks, resulting in six categories and their definitions, discussed in the “Results” section. After defining the categories, both coders separately categorized the labels according to those definitions, which resulted in a substantial agreement (kappa = .75). 5 Labels that both coders did not agree on were discussed, until full agreement was reached.
We secured the credibility of the findings by systematically comparing observations within and across study participants before finalizing the categorization of the data (Charmaz, 2006; Thomas & Magilvy, 2011). We continued this process until thematic saturation was reached, and no new categories emerged from the data. Furthermore, multiple coders were involved in each step of the coding process, each of whom was to reach full agreement in the labeling and categorization before moving on to the next step. Finally, the two coders searched for representative examples of the categories across the interview data (Yeshua-Katz & Martins, 2013), which we discuss in the next section of this article.
Results
Six categories of factors were identified that might influence participants’ conversational behavior about health issues: (a) type of communication behavior, (b) communication objective, (c) health theme, (d) conversation partner, (e) participant characteristics, and (f) conversation context. The results discussed below are arranged according to the category “type of communication behavior.” For each type of communication behavior, we discuss factors, in the form of the other five categories that we found to influence its occurrence.
We identified the following types of communication behavior emerging from participants’ descriptions of their interpersonal health communication intentions and behavior: (a) admonishing the conversation partner regarding health behavior: urging him or her to adapt health behavior, to prevent damage to his or her own health and/or that of others, for example, telling the conversation partner not to smoke; (b) casual talk about a health issue: talking about a health theme in a social situation, for example, exchanging information about healthy eating or about tanning behavior among friends; (c) educating the conversation partner about a health issue: providing the conversation partner with information on a health issue to prevent him or her from performing unhealthy behavior, for example, parents educating their children on the dangers of alcohol; and (d) negotiating about a health issue: attempting to reach agreement with each other on performing healthy behavior for the benefit of both the self and the conversation partner, for example, communication between sexual partners about condom use.
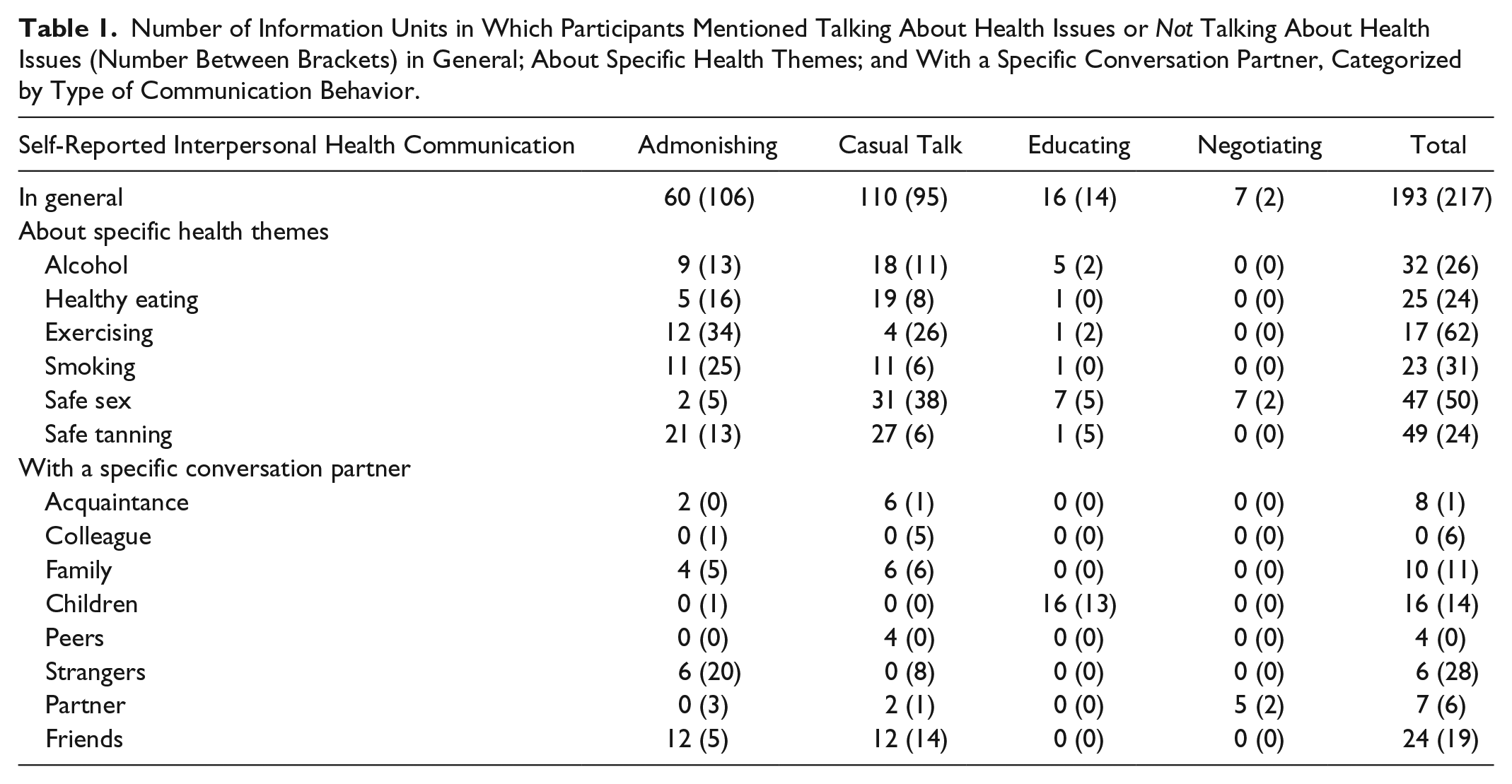
The tables referred to below represent the number of information units in which participants mentioned talking about a health issue. The numbers between brackets indicate the number of information units in which participants specifically mentioned not talking about a health issue. In Table 1, we show the number of information units in which participants indicated to talk, or not to talk, in general, about specific health themes, and with a specific conversation partner. The results described in this table are arranged by type of communication behavior. The results in Table 1 suggest, for instance, that participants in general most often made statements about casual talk and that participants most often made statements about not admonishing someone. Furthermore, the results in Table 1 suggest that participants most often reported talking about health themes with friends, and most often reported not talking about health themes with strangers.
Number of Information Units in Which Participants Mentioned Talking About Health Issues or Not Talking About Health Issues (Number Between Brackets) in General; About Specific Health Themes; and With a Specific Conversation Partner, Categorized by Type of Communication Behavior.
Admonishing
The first type of communication behavior that we distinguished was admonishing, which occurs when someone urges a conversation partner to change his or her health behavior, for example, when telling someone they should not drink alcohol. Admonishing mainly seemed to serve instrumental objectives, that is, “getting something done” through the interaction. Participants admonishing someone appeared to feel “obliged” to communicate their message, even if this did not improve their own health outcomes: They not only indicated that they admonished a smoker who smoked in their proximity, which would improve their own health outcome, but also admonished parents who did not put sunscreen on their small child, which would not improve their own health outcome. Furthermore, in a more subordinate position, admonishing appeared to serve interpersonal and identity objectives. When admonishing the conversation partner, he or she may experience this as a face threatening act which could possibly lead to damage to the relationship. Admonishing the conversation partner could also result in the face of the self being threatened because of the risk of being seen as a nuisance. Still, participants seemed to feel a moral obligation to admonish other people rather urgently, as evidenced by the many instances of “admonishing” in Table 1.
A factor influencing the occurrence of admonishment was the health theme. The results in Table 1 indicate that participants most often admonished someone when it concerned the health theme of “safe tanning.” The results in Table 1 furthermore indicate that participants most often did not admonish someone when it concerned the health theme of “exercising,” followed by “smoking.” Participants did not think that “safe tanning” was a very difficult topic about which to admonish someone, as is shown in the following example:
I think this is one of the easier things, because then you can eh, without directly, when someone is too fat, then they could feel hurt or something about it, but like . . . “Don’t sit in the sun too long, don’t you know that’s not good for you?” “Dry skin, shouldn’t you put something on that?” All examples of how to say something about this. (Participant 12)
For “exercising,” the person admonished might feel attacked about his or her weight or looks. Admonishing someone about his or her exercising behavior is thus more direct and perhaps more sensitive, in which case interpersonal and identity objectives might be more prevalent than instrumental objectives.
The occurrence of admonishment furthermore seemed to be influenced by the conversation partner, that is, the person being admonished. The results in Table 1 suggest that participants most often admonished friends and that they most often did not admonish strangers. This indicates that, for admonishing, the social proximity of the conversation partner plays a role. It may be more appropriate to admonish someone in a socially proximate relationship, such as a friend, than to admonish someone in a socially distant relationship, such as a stranger.
Another factor influencing the occurrence of admonishment appeared to be participants’ characteristics. In Table 2, we show participants’ self-reported communication behavior on health themes arranged according to participant characteristics. The results in Table 2 indicate that older participants more often than younger participants do not admonish someone, as in the following example concerning “alcohol,” in which an older participant expresses a fear of reprisal:
. . . Nowadays you can get hit easily. Then they say: “What’s it to you?” So you don’t bring it up. It’s like when someone is destroying something, that you’d say “Don’t do that.” “What’s it to you?” Because people are different than they used to be of course. They hit other people more easily. . . . Or they get angry. That they say: “Hey oldy, mind your own business!” (Participant 7)
Number of Information Units in Which Participants Differing in Characteristics Mentioned Talking About Health Issues or Not Talking About Health Issues (Number Between Brackets), Categorized by Type of Communication Behavior.

The results in Table 2 furthermore suggest that participants with a high level of education admonish someone about their health behavior more often than participants with a low level of education. The participants’ gender did not seem to be related to the occurrence of admonishment.
Casual Talk
For casual talk, like gossiping, small talk, or casual exchange of information, the main concerns of the participants did not seem to be with instrumental objectives, as with admonishing behavior. Rather, casual talk appeared to arise from interpersonal and identity objectives; that is, it concerned maintaining a good relationship with the conversation partner and maintaining a positive self-image. In several cases, for instance, we found that participants thought it was easier or more pleasant to talk with like-minded people about a specific health theme. The example below, on the theme of “smoking,” illustrates that the main objective of the participant is to maintain a positive self-image, by being among like-minded people and thus likely not to violate social norms, and to maintain a good relationship with the conversation partner(s) by gossiping about an out-group.
And do you think, then, that it is easy in such a situation to talk about this with like-minded people?
With like-minded people, yes, then you are completely free, like “God, what are they thinking?” like that.
The occurrence of casual talk appeared to be influenced by the health theme that was the topic of communication. In Table 1, we see that participants most often indicated a willingness to talk, but also to not talk (e.g., with a different conversation partner) casually about the health theme “safe sex.” Furthermore, participants appeared to talk casually about “safe tanning,” and not to talk casually about “exercising.” In the following example, a participant refers to casual talk about “safe sex”:
So you think it’s easy to talk about this?
Yes, everybody has sex.
Another factor that was found to influence the occurrence of casual talk is the conversation partner. As we can see in Table 1, participants most often (do not) seem to talk casually with friends. Whereas participants indicated that they talked casually with friends about some health topics, they indicated they did not talk casually with friends about other health topics, as in the following example, where a participant mentions not talking casually with friends about “safe tanning”:
. . . getting sun burnt, that’s something for the short term, so everybody takes this . . . into account. But I never talked about this with friends, like: “Then I might get cancer in the far away future.” (Participant 5)
Participants furthermore appeared to talk casually with family and acquaintances, and not with strangers. This suggests that participants might mainly talk casually with conversation partners with whom they wanted to maintain a good relationship, that is, someone they already know.
Furthermore, the occurrence of casual talk seemed to be influenced by participant characteristics. The results in Table 2 show that older participants more often than younger participants indicated that they talked casually about health issues. Furthermore, the results in Table 2 suggest that participants with a high level of education indicated that they did not talk casually about health issues more often than participants with a low level of education. Moreover, the results in Table 2 suggest that women participants talked casually more often than men participants, whereas men participants mentioned not talking casually more often than women participants.
Another influencing factor regarding the occurrence of casual talk was the conversation context or, more specifically, the presence of someone in the communicative situation whom the topic personally concerns. In Table 3, it is indicated in n = 54 cases that it matters whether a person whom the topic personally concerns is present in the communicative situation and that this determined whether or not participants talked casually about a health issue. In n = 181 cases, this did not seem to matter in determining whether or not to talk casually about a health issue. An example on the health theme “healthy eating” when the presence of a person whom the topic personally concerns does matter is as follows:
Is this then a difficult topic to talk about as long as no one around is obese?
No, then it is just not difficult. But if people are around who are obese, then I think it’s difficult to say something about this topic.
Number of Information Units in Which Participants Indicated That It Does or Does Not Matter Whether Someone Is Present in the Communicative Situation Whom the Topic Personally Concerns, Categorized by Type of Communication Behavior.

This example indicates that the presence of a person whom the topic personally concerns might matter when this personal relevance is obvious or visible, such as when this person is obese. It might be more difficult to estimate whether a person has an alcohol addiction or has skin cancer, for instance.
Educating
For educating, as for admonishing, the main concern of participants appeared to be with instrumental objectives, that is, with getting the conversation partner to perform healthy behavior. Although this objective is the same as for admonishing, educating might occur more indirectly, that is, through providing the conversation partner with information on which to base his or her decision to adapt or not to adapt health behavior. Furthermore, educating seemed to be used preventively, whereas admonishing seemed to be used when the conversation partner was already performing unhealthy behavior. Again, as with admonishing someone, interpersonal and identity objectives were found to play a role, creating a struggle between the wish to be effective and the wish to prevent damage to the relationship, and damage both to own identity and that of the other person. In the following example, a participant talked about his wish to educate his children effectively on “safe sex,” even if they felt uncomfortable talking about this issue:
. . . I think it’s easier to talk with my children about that than the other way around. That’s the way the relationship is defined. You don’t talk about sexuality with your parents, but your parents think they should talk about this with you . . . it’s better to have said this once too many than once too little. Better safe than sorry. (Participant 11)
A factor determining the occurrence of educating was the health theme. The results in Table 1 indicate that educating is most common for the health theme of “safe sex.” The results in Table 1 furthermore show that participants gave reasons to not educate someone about the health theme of “safe tanning,” as in the following example:
. . . I talked about this in the summer, with my wife. That you should protect yourself against that, against too many sunbeams. Not with my kids, they don’t listen anyway. (Participant 10)
Another influencing factor in the occurrence of educating was the conversation partner. The results in Table 1 indicate that participants mentioned educating only in the context of children. This indicates that whereas for casual talk the relationship between conversation partners was mainly horizontal, as between friends, for educating the relationship between conversation partners was vertical, as between parents and children. The following example describes a parent educating her children about “alcohol”:
. . . and I can tell my own kids, like: “Don’t drink so much!” Or: “You know that’s bad for you, your brains will be damaged, you’re not going to be fit, what you’re doing in the weekend will bother you for three days,” things like that. But it’s always in a kind of mother role of course, like eh, mothers always have something, right. That’s partly fear that something will happen to your kids, and in general of course. (Participant 12)
Furthermore, the occurrence of educating appears to have been influenced by participant characteristics. The results in Table 2 suggest that only older participants mentioned educating, which can be explained by the fact that the older participants all had a child or children, whereas none of the younger participants did. Furthermore, the results in Table 2 indicate that participants with a high level of education more often mentioned educating than participants with a low level of education. The gender of participants did not appear to influence the occurrence of educating behavior.
Negotiating
For negotiating, as for admonishing and educating, the main concern of participants appeared to be with instrumental objectives, in this case with getting both the self and the conversation partner to perform healthy behavior. Furthermore, as with admonishing and educating, interpersonal and identity objectives were found to play a role, for example, when negotiating about an issue increases the risk of damage to the relationship or to own identity.
A factor influencing the occurrence of negotiating was the health theme. The results in Table 1 indicate that participants only mentioned (not) negotiating about the health theme of “safe sex.” Another influencing factor in the occurrence of negotiating was the conversation partner. The results in Table 1 furthermore indicate that participants only mentioned (not) negotiating with their partner or sexual partner, as in the following example:
Is this something that you easily talk about, with friends, or sexual partners?
Naturally with sexual partners, then it makes sense, then it has to be discussed.
This health theme might be the only one in which both conversation partners stand to gain the same advantage from the communicative act: that is, maintaining their sexual health. This type of communication behavior, thus, only occurs with a conversation partner that is highly socially proximate, and with whom the relationship is horizontal: namely, the sexual partner. Participant characteristics did not appear to influence the occurrence of negotiation behavior.
Discussion
In this study, we explored factors underlying interpersonal health communication. To be able to trigger conversations about health campaigns, we need to know more about whether people talk about health issues, with whom, and why. In the present study, we attempted to contribute to more knowledge on this issue. The results show, first of all, that interpersonal health communication is not one general type of behavior. We found at least four different categories of communication behavior, each with its own determinants, and each with its own objectives: admonishing, casual talk, educating, and negotiating. The idea that communicative acts vary for different contexts and different conversation partners has been suggested before, both in theory (Hymes, 1972) and in empirical research (Goldsmith & Baxter, 1996). To our knowledge, we were the first, with the present study, to link this idea to health communication, and to explore factors that might influence the occurrence of interpersonal health communication in more detail.
Our results have suggested that interpersonal health communication is goal-oriented behavior, as was asserted by Southwell and Yzer (2007, 2009), and that for every category of health communication behavior, there is a different dynamic of instrumental, interpersonal, and identity objectives. For admonishing, educating, and negotiating, the main concern of participants appeared to be with instrumental objectives, that is, with the effectivity of the communicative act. This does not mean, however, that interpersonal and identity objectives do not play a role in these types of communication behavior. Multiple communicative objectives can be prevalent in one communication situation, and might sometimes conflict. Interpersonal and identity objectives are always at stake, but often as subordinate objectives.
In casual talk, however, participants appeared to be primarily concerned with interpersonal and identity objectives, and not so much with instrumental objectives. For example, participants indicated that, if an obese person were present in the communicative situation, they would not casually talk about “healthy eating” out of fear of hurting the obese person’s feelings. If an obese person is not present in the communicative situation, however, participants indicated that they would talk, that is, gossip, about this person and his or her behavior. Gossiping with “like-minded people” might serve both interpersonal and identity objectives, through behaving and communicating according to the social norms that are prevalent in the communicative situation.
The diversity of different types of communication behavior, as found in the present study, should be taken into account when doing research on interpersonal health communication, and also when designing health campaigns that aim at triggering interpersonal health communication. It appears that, for every type of communication behavior, health theme, type of conversation partner, and so forth, different factors might play a role. As was indicated in the introduction, if we are to influence people to talk about health issues, we need to know why the target population would or would not engage in this behavior (Yzer, 2008).
Previous research on this topic (Donné, Jansen, Huijbers, & Hoeks, 2016; Hughes & Lewinson, 2015) has attempted to apply a well-known model for predicting reasoned behavior toward interpersonal health communication, the integrative model for behavioral prediction (IMBP; Fishbein, 2000; Fishbein & Yzer, 2003). The IMBP has been used previously for predicting health behavior, such as safe sex behavior. Interpersonal communication, just like some types of health behavior, extends from attitudinal, normative, and efficacy beliefs that people have about performing that behavior (Southwell & Yzer, 2007). Even though Hughes and Lewinson (2015) found the IMBP to be applicable for uncovering motives for aging women’s sexual health communication with health care providers. Donné et al. (2016) found that it was difficult to distinguish attitudinal, normative, and efficacy beliefs for a social behavior like interpersonal communication. The results of the present study indicate, rather, that it is essential to distinguish between different types of communication behavior.
Fishbein (2000) and Fishbein and Yzer (2003) indicated that, to be effective, interventions should focus on triggering specific types of behavior instead of one general category of behavior. Our results suggest that for interpersonal health communication, this might indeed be the case. Depending on the health topic and the target group, some health campaigns should focus on triggering admonishing, whereas other campaigns should focus on triggering casual talk, educating, or negotiating. Different types of communication behavior might be persuasive in different ways and in different contexts. Health campaign designers should be as specific as possible about what kind of interpersonal communication behavior exactly is desired.
In this exploratory study, we revealed some noteworthy results, providing a new perspective on interpersonal health communication behavior. Future research on interpersonal health communication should look beyond the question of whether people talk about health issues or not, and look at how people talk about these health issues, and what the effects of these types of communication behavior are for eventual health outcomes. Moreover, future research could focus on identifying determinants of health communication in larger groups of participants, to find out whether the findings of the current study hold true in other contexts. Finally, in the present study, participants were interviewed about their conversational behavior on health issues. This might have caused them to feel obliged to talk about these health issues, as if these issues were something they should talk about. Future studies on interpersonal health communication might therefore consider applying methods other than in-depth interviews, such as observational methods.
Conclusion
In the exploratory study described in this article, we empirically looked in detail at the factors that might influence interpersonal health communication. From the literature, the effects that interpersonal health communication might have on health campaign outcomes are only known to some extent. We know that conversations about health issues can be effective, but we do not know how and under which circumstances this would be the case. The results of the present study suggest that different types of communication behavior might be effective in different types of health contexts. Our study can serve as the basis for extending knowledge about the effects of interpersonal health communication on health outcomes. This interpersonal health communication is a vital part of health campaign effectiveness.
Footnotes
Authors’ Note
The study protocol was approved by the institutional ethical committee (CETO) of the Faculty of Arts of the University of Groningen, The Netherlands, and the participants provided informed consent.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.