
Abstract
Acquired brain injury (ABI) is one of the greatest causes of death and disability among children in Canada. Following ABI, children are required to transition back to school and adapt to the physical, cognitive, behavioral, social, and emotional demands of the school environment. We conducted a qualitative systematic review of students’ and parents’ experiences of the transition back to school following ABI. We identified 20 articles that met our inclusion criteria. Six themes emerged: (a) lack of ABI-specific education for families and professionals, (b) communication-related factors as a facilitator and/or barrier to transition, (c) emotional focus, (d) peer relationships, (e) supports, and (f) ABI sequelae in the classroom. Students’ and families’ personal motivations and abilities and the support they receive in their environment affect their experiences of transitioning back to school and the disrupted occupations they face.
Acquired brain injury (ABI) is an umbrella term referring to damage that has occurred to the brain following birth (Savage & Wolcott, 1994). ABI refers to damage as a result of a traumatic brain injury (external exertion of force resulting in either open or closed injuries) or non-traumatic brain injuries (vascular accidents, anoxic injury, infectious disease, metabolic issues, or toxicity affecting the brain; Savage & Wolcott, 1994). They can result in varied levels of disability or impairment and cause a number of functional or performance issues (e.g., hearing and/or vision loss, difficulty concentrating, seizures, need for mobility aide, depression; Ontario Brain Injury Association [OBIA], 2012; Savage & Wolcott, 1994). ABI is often associated with a number of complex and ongoing sequelae over an extended recovery period. It is the leading cause of morbidity and mortality in the Canadian pediatric population (Canadian Institute of Health Information, 2006). With recent advances in medical and rehabilitative practices and technology, survival rates following ABI are increasing (Kramer & Zygun, 2013). Improved survival rates lead to higher demands on community rehabilitative and educational systems in supporting the reintegration of children and youth affected by ABI back to their everyday lives (Shaw & McCabe, 2008). Beyond the initial reintegration, increased survival rates require additional long-term planning for the children’s altered and continually changing levels of ability (Shaw & McCabe, 2008).
ABI has been described as “an invisible epidemic” (Carter & Spencer, 2007, p. 34) that has financial, educational, and emotional consequences for the children and families that experience it. As survival rates for children and youth with myriad chronic diseases increase, their return to community and school becomes a major rehabilitative focus (Newacheck & Hafon, 1998; Shaw & McCabe, 2008). The shift in the health care sector’s focus from hospital-based recuperation to community- and school-based reintegration and rehabilitation takes a large burden of care off of the health care system and emphasis is instead placed on the children’s long-term recovery or rehabilitative goals (Newacheck & Hafon, 1998; Shaw & McCabe, 2008). However, the move to community-based rehabilitation places increased onus on family and education system members, who do not necessarily have the education, training, or resources needed to help children and youth through their recovery process (Lindsay, Proulx, Thomson, & Scott, 2013; Shaw & McCabe, 2008).
Following ABI, children and youth must also cope with the effects of the injury on their maturing brains; for example, ABI can influence the development of their personal and social identities, as well as their individual and overall maturation into adulthood (Bogan, Livingston, Parry-Jones, Buston, & Wood, 1997; Gauvin-Lepage & Lefebvre, 2010). In their ABI-related transitions back to daily life, children and youth may struggle to regain their identity, social standing, and pre-injury knowledge (Agnihotri et al., 2014; Chan & Fong, 2011; Glang, Todis, Cooley, Wells, & Voss, 1997; Ylvisaker et al., 2005). They must also adjust to their new sequelae and/or physical abilities (Mealings & Douglas, 2010; Ylvisaker et al., 2005). During this transition, students are required to return to complex and multifaceted school environments; they must simultaneously navigate the interwoven physical, cognitive, social, and behavioral demands of school, which can be especially challenging for youth with varied levels of ABI severity (Bogan et al., 1997; Bruce, Chapman, MacDonald, & Newcombe, 2008; Mealings & Douglas, 2010; Mealings, Douglas, & Olver, 2012). To promote a successful hospital-to-school transition, students’ specific ABI-related needs and abilities should be considered during the creation of school reintegration and education plans.
Research on hospital-to-school transitions following ABI has recently proliferated. Authors of previous review articles have focused on both qualitative and quantitative studies of transition experiences (e.g., Mealings et al., 2012) and the usefulness of interventions that target hospital-to-school transitions among youth with ABI (Lindsay, Hartman, Reed, Gan, Thomson, & Solomon, 2015). However, researchers have not yet synthesized findings specifically on the qualitative experiences of hospital-to-school transitions among youth with ABI. Synthesizing and understanding such experiences is important to inform the development of future interventions and identify which educational and rehabilitative supports are appropriate. The integration of findings from multiple qualitative studies, rather than a single study, can also grant researchers deeper and more generalizable insights into the experiences, opinions, and needs of students and parents (Erwin, Brotherson, & Summers, 2011; Lindsay, 2014). Finally, qualitative synthesis allows researchers to identify user- and researcher-indicated gaps in the current literature, which can help them identify areas for future research and intervention (Major & Savin-Baden, 2010). To address these knowledge gaps, we have synthesized the qualitative literature on hospital-to-school transitions among children and youth with ABI from the perspectives of students and their parents.
Method
Search Strategy
We designed our search strategy in collaboration with a hospital librarian. We searched seven electronic databases—including Ovid MEDLINE, HealthSTAR, ERIC, EMBASE, Cochrane Database of Systematic Reviews, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and PsycINFO—for articles published between 1989 and June 2014. We set the historical limit of 1989 to capture research that anticipated or explored the early implementation of the Individuals With Disabilities Education Act (IDEA; P.L. 101–476). This act was introduced in the United States in 1990, and it affected how students with disabilities—such as those who have experienced brain injuries—access education. Our search criteria included terms related to hospital-to-school transitions, ABI, and limiters on age (child, youth) and year (1989 to June 2014).
We screened articles for relevance, based on the following inclusion criteria: (a) the article focused on a sample of children and/or youth (average sample age of 6–20 years) who experienced ABI and/or their parents, (b) the article reported original qualitative research that focused on student or parent experiences of hospital-to-school transition following the student’s ABI (including transition planning stages and/or the transition process and/or reflection on the transition process after it had occurred), (c) the research entailed qualitative design for data collection and analysis, (d) the article was published in a peer-reviewed publication or as a thesis between 1989 and June 2014, and (f) the article was available in English. Note that age range has been used to delineate between child/youth and adult care populations, and not as a parameter for analysis. We excluded articles that (a) reported on research entailing only quantitative data collection and analysis, (b) were editorials or opinion articles, and (c) were program descriptions, program or literature reviews, or practice frameworks.
Our database search returned 4,761 unique articles (Figure 1). We imported them into Endnote© referencing software and removed duplicates. Two authors screened each title for eligibility and identified 85 articles that were potentially relevant. We then reviewed the abstracts and full texts of those articles and found that 68 did not meet our inclusion criteria. Three authors read the remaining 17 articles and confirmed their appropriateness. We identified an additional three articles by searching the reference list of each article selected for inclusion. We included a final sample of 20 articles in our synthesis. We resolved any discrepancies in our selection of articles through discussion among the research team.
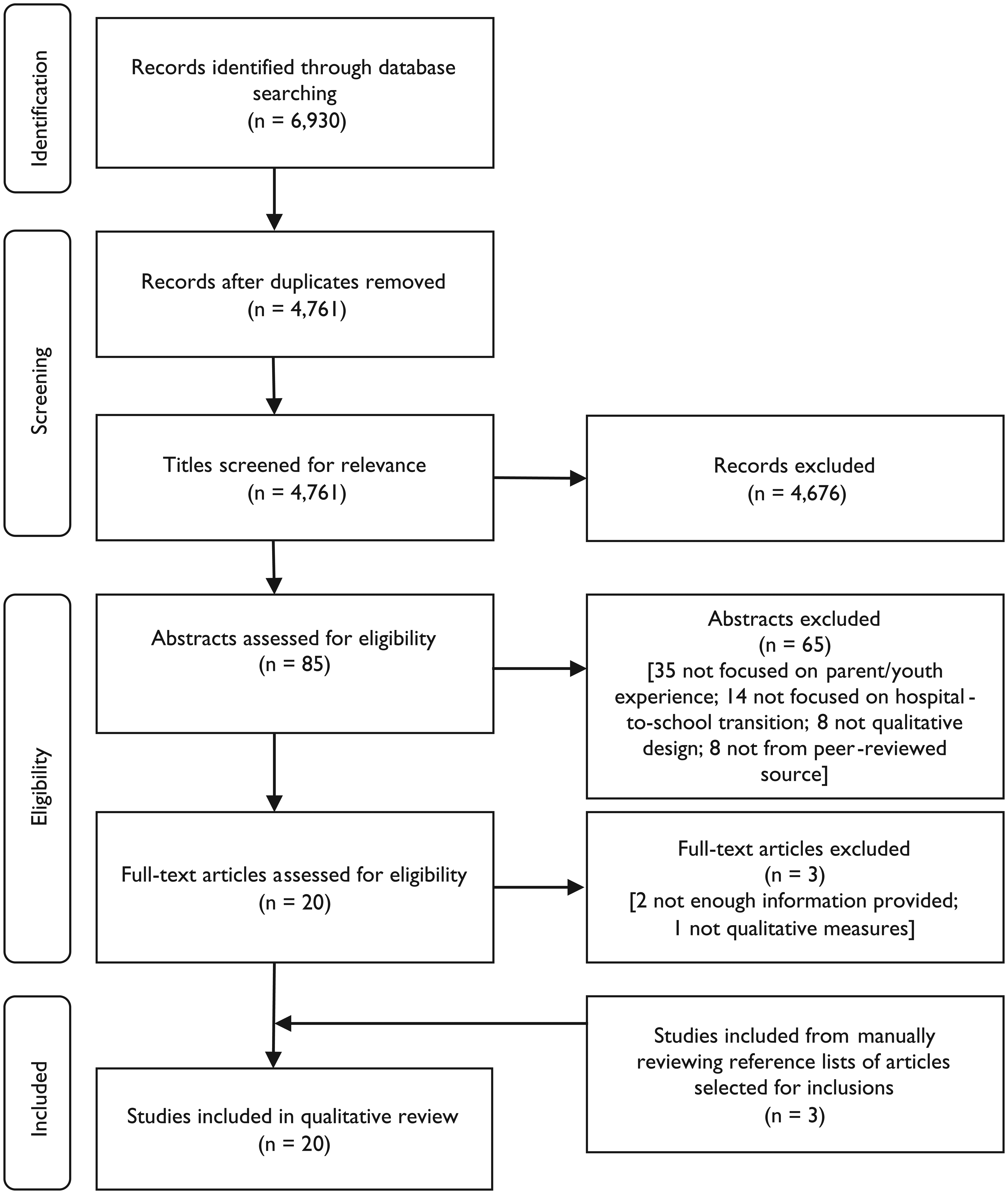
Flow diagram of article inclusions and exclusions.
Analytical Approach for Review and Synthesis
We used Major and Savin-Baden’s (2010) approach to qualitative research synthesis to synthesize and analyze the data. First, we extracted data from each unique article—including bibliographic, methodological, outcome, and limitation-based information. Then, we used Major and Savin-Baden’s reciprocal translation analysis technique to consider each article in relation to the others to identify themes that most closely addressed hospital-to-school transition experiences among students and their families following ABI. This process involved (a) multiple readings of each article by two or more authors; (b) data extraction from each article, as described above; (c) identification of first-order themes and collection of quotations to support those themes; (d) identification and comparison of first-order themes across studies; (e) identification of second-order themes across the articles; (f) development of third-order interpretation from the articles and wider literature; and (g) iterative return to the original texts to review emerging themes and ensure their adequacy in explaining findings (Major & Savin-Baden, 2010). For clarification, first-order themes are defined as themes within each individual article either presented by the authors or derived by the synthesists (Major & Savin-Baden, 2010). Second-order themes are composite themes represented or starkly not represented across studies (Major & Savin-Baden, 2010). Finally, third-order interpretation involves organizing structures or overarching principles for the themes that have emerged (Major & Savin-Baden, 2010).
Theoretical Approach
Following our analysis of the research, as described above, we drew on the concept of occupational disruption (Whiteford, 2000) to inform our interpretation and presentation of the themes that emerged. We situated occupational disruption within the framework of the Model of Human Occupation (MOHO; Kielhofner, 2008) to allow for a better understanding of how occupations are chosen and formed both before and following an occupational disruption. In this context, “occupation” draws from the occupational science definition; it encompasses the various activities with which people occupy their time—the activities that bring meaning and purpose to their lives (Asaba, Blanche, Jonsson, Rudman, & Wicks, 2007). This includes the daily activities that individuals both want to engage in (e.g., socializing, playing games, going to school) and need to engage in (e.g., going to school, chores, self-care). An activity that is laden with such meaning and purpose in one’s life is referred to as an occupation.
An occupational disruption may occur when an individual’s ability to engage in their normal patterns of occupation is disrupted by personal, health, or environmental changes (Whiteford, 2000). Researchers have used this concept to explore a variety of changes in people’s abilities to participate in daily occupations—including changes following acute injury (Molyneaux-Smith, Townsend, & Guernsey, 2003), chronic fatigue syndrome (Hughes, 2009), and imprisonment (Whiteford, 2000). An occupational disruption refers to a temporary state that can be resolved under supportive conditions (Whiteford, 2000). Examples of potentially supportive environments include family, social systems, rehabilitative care settings, and work environments, and they are all considered within a wider environmental context of rehabilitation policy and practice which can in itself be supportive or unsupportive (Molyneaux-Smith et al., 2003). If the disruption is left unsupported and unresolved, it can lead to occupational dysfunction (Hughes, 2009; Whiteford, 2000), which is a chronic inability to participate in occupations following a prolonged period of occupational disruption. Thus, exploring occupational disruption involves identifying (a) the occupations that are disrupted; (b) the old, new, and altered skills that are required to re-engage in those or other meaningful occupations; and (c) the environmental supports that are required to regain versions of previous occupations that were disrupted by the ABI. We do not intend to imply that a student must or should reclaim occupations that they held prior to an ABI, but intend to explore whether and how occupations are incorporated into students’ lives as they transition back to school.
We use the MOHO as a framework to explore occupational disruption in relation to participants’ volition (motivations, values, interests), habituation (roles, routines, habits), and performance (skills required to perform task; Kielhofner, 2008). We also consider environment, which affects volition, habituation, and performance. All four components concurrently affect the ways in which occupational engagement is regained or altered following disruption (Kielhofner, 2008). We have used the components of the MOHO to explore the ways a student regains or alters occupations that have been disrupted following an ABI.
Quality Appraisal
We maintained the quality of our review by measuring the quality of articles selected for synthesis and maintaining quality control measures in our own research processes. We screened articles selected for the synthesis using the Qualitative Research Quality Checklist (QRQC; Saini & Shlonsky, 2012; see Table 1). The QRQC allows researchers to assess articles based on 25 criteria—such as purpose; setting; data collection and analysis methods; ethical issues; bias; compatibility between research question, design, and methods; and evidence provided for conclusions. For our purposes, we only included the first 21 criteria of the QRQC, as the latter four are specific to justice-oriented and participatory action-based research, which did not apply to our sample.
Qualitative Research Quality Checklist (QRQC).

Source. Adapted from Saini and Shlonsky (2012).
Note. R = is this question relevant to the study?; SI = is there sufficient information that this study addresses the question? C = open section for researcher comments; Y = Yes; U = Unspecified by the authors; N = No.
Thesis or dissertation.
Published abstract.
We used peer evaluation at all stages of our synthesis (Major & Savin-Baden, 2010) to maintain quality through group agreement. Two members of the research team screened articles returned from our initial database search. All members of the team discussed each of the 20 full-text articles considered for inclusion until consensus was reached regarding their inclusion. Laura Hartman maintained a thorough audit trail of team reflections, decisions, and meetings throughout the process.
Results
Characteristics of Included Studies
We identified 20 articles that met our inclusion criteria for qualitative synthesis. The reported studies originated from the United States (n = 9), Australia (n = 5), Canada (n = 3), the United Kingdom (n = 2), and Scotland (n = 1; see Table 2) and were all available in English. Six articles focused on parent experiences of hospital-to-school transitions following ABI (Backhouse & Rodger, 1999; Berbaum, 2008; Bruce, Newcombe, & Chapman, 2012; Cheung et al., 2014; Plotts & Jantz, 2012; Robson, Ziviani, & Spina, 2005), seven focused on youth experiences (Bogan et al., 1997; Carter & Spencer, 2007; Gauvin-Lepage & Lefebvre, 2010; Linden & Jordan, 2012; Mealings & Douglas, 2010; Roscigno, Swanson, Vavilala, & Solchany, 2011; Todis & Glang, 2008), and seven addressed both parent and youth experiences (Boylan, 2014; Bruce et al., 2008; Haarbauer-Krupa, King, Wise, Gilliam, & Hendrix, 2013; Richey, 2008; Rosenthal, 2013; Sharp, Bye, Llewellyn, & Cusick, 2006; Vaidya, 2002).
Overview of Included Studies.

Note. ABI = acquired brain injury; GCS = Glasgow Coma Scale; TBI = traumatic brain injury; ns = not specified.
The articles reported on a diverse pool of participants, including at least 172 children and youth (students), 113 parents/guardians, and 67 education or health care professionals. However, one article (Haarbauer-Krupa et al., 2013) did not specify the number of participants; therefore, we could not determine the exact numbers of total participants. Note that while 67 health and education professionals were included in the sample, we only sought articles and feedback from parents and students (for information on clinical and educational professional perspectives, see Hartman, Duncanson, Farahat, & Lindsay, 2015). Two of the articles (Linden & Jordan, 2012; Plotts & Jantz, 2012) did not report the age range of students. The remaining articles reported on students—either as participants or as children of participants—who ranged in age from 4 to 17 years old.
The articles reported on studies that entailed varied methods and methodological approaches to collecting and interpreting qualitative data. For data collection, 11 of the reported studies entailed individual interviews (Bogan et al., 1997; Boylan, 2014; Bruce et al., 2008; Bruce et al., 2012; Cheung et al., 2014; Mealings & Douglas, 2010; Plotts & Jantz, 2012; Robson et al., 2005; Roscigno et al., 2011; Sharp et al., 2006; Vaidya, 2002), five utilized multiple methods for purposes of case studies (Berbaum, 2008; Carter & Spencer, 2007; Haarbauer-Krupa et al., 2013; Richey, 2008; Rosenthal, 2013), two included focus groups (Backhouse & Rodger, 1999; Gauvin-Lepage & Lefebvre, 2010), one collected written responses to qualitative survey questions (Linden & Jordan, 2012), and one used a combination of interview and observation (Todis & Glang, 2008). For data analysis and interpretation, nine of the reported studies primarily applied thematic analyses (Berbaum, 2008; Bruce et al., 2008; Bruce et al., 2012; Cheung et al., 2014; Linden & Jordan, 2012; Mealings & Douglas, 2010; Richey, 2008; Robson et al., 2005; Rosenthal, 2013), two described coding through software (Bogan et al., 1997; Plotts & Jantz, 2012), and one each utilized inductive processes (Backhouse & Rodger, 1999), interpretive phenomenological analysis (Boylan, 2014), case study chronology (Carter & Spencer, 2007), analytical structures approach (Gauvin-Lepage & Lefebvre, 2010), Collaizzi’s phenomenological framework (Roscigno et al., 2011), grounded theory methods (Sharp et al., 2006), and inductive coding (Todis & Glang, 2008). Two studies did not specify data analysis techniques (Haarbauer-Krupa et al., 2013; Vaidya, 2002).
Only five of the 20 articles reported the use of a theoretical perspective. Berbaum (2008) used the theories of normalization of education (Wolfensberger, 1975) and neuropsychological learning theory (Rourke, Bakker, Fisk, & Strang, 1993). Gauvin-Lepage and Lefebvre (2010) applied an ecological approach (Bronfenbrenner, 1979). Mealings and Douglas (2010) used the theory of social interactionism (Corbin & Strauss, 1998). Richey (2008) explored the topic through the lens of inter-subjective truth (Coles, 1989). Finally, Rosenthal (2013) framed her work with a combination of Self-Determination Theory (Deci & Ryan, 1985), Self-Efficacy Theory (Bandura, 1986), the Kubler-Ross Grief Cycle (Kubler-Ross, 1969), and the Lezak stage model (Lezak, 1986).
Upon completing the QRQC (see Table 1), we found that the research questions of our selected articles appropriately addressed our own research question. Saini and Shlonsky (2012) caution users of the QRQC that not all indicators on their checklist will be relevant to each study. Such relevance is dependent upon the authors’ ontological and epistemological stances. The absence of a criterion from an article does not necessarily mean that the study is of poor quality. Therefore, the QRQC was used to guide our evaluation of the quality of each article, and the presence or absence of a criterion did not guarantee our interpretation of the article’s overall quality. Across our sample of articles, we noted a particular lack of clarity regarding sample selection procedures within the studies, the range of methods used to triangulate data, who collected and analyzed data, how researchers handled ethical issues and biases, and whether audit trails and reflective journals were used by researchers.
Parent and Youth Experiences of Hospital-to-School Transition Following ABI
Six themes emerged from our review regarding youth and parent experiences of back-to-school transitions following ABI: (a) lack of education on ABI for family and professionals, (b) communication-related factors as a facilitator and/or barrier, (c) emotional focus, (d) peer relationships, (e) support for students and families, and (f) ABI sequelae in the classroom. We describe the themes below and provide a table of illustrative quotations for each theme (see Table 3).
Demonstrative Quotations.
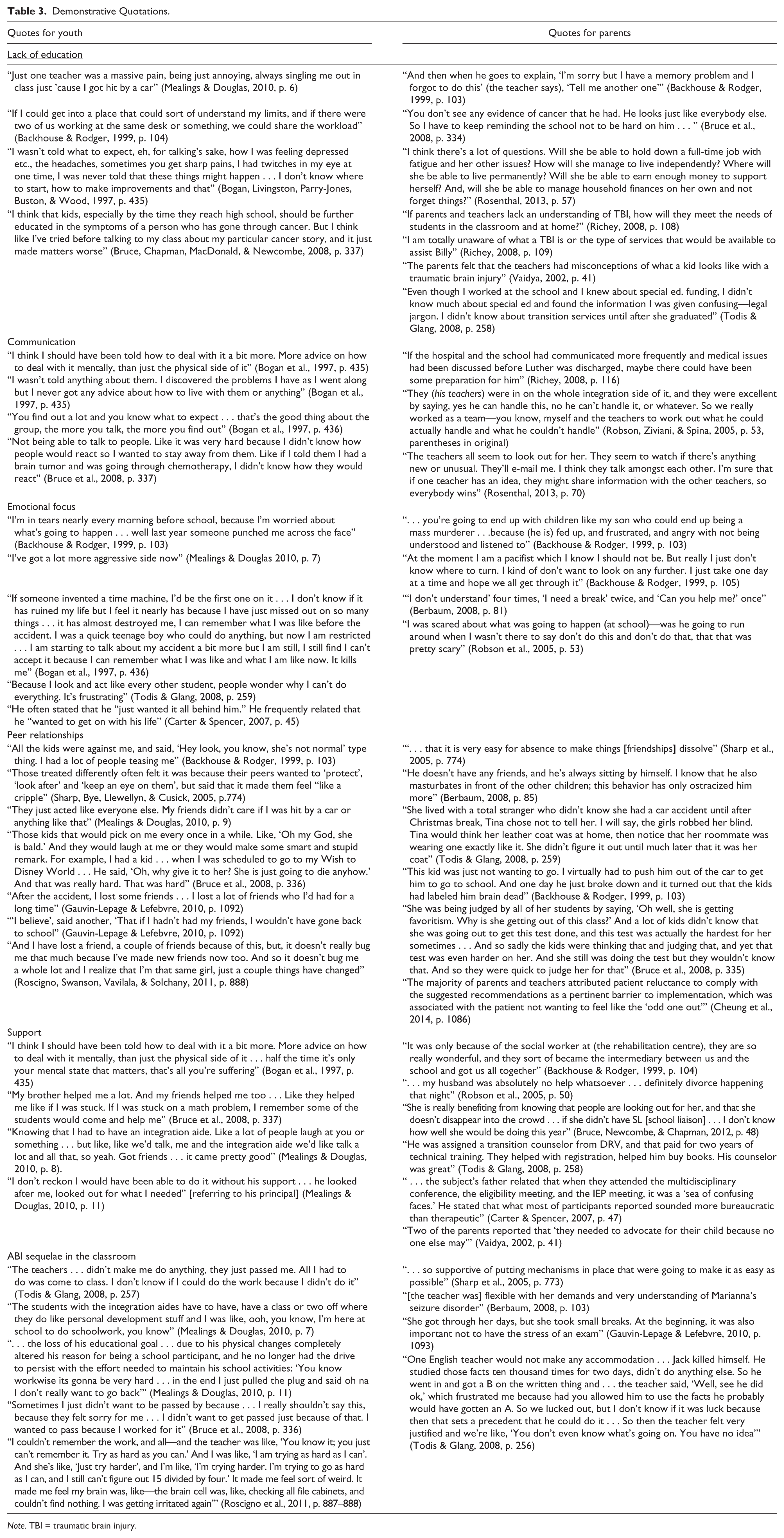
Note. TBI = traumatic brain injury.
Lack of Education on ABI for Family and Professionals
In 10 of the reported studies, students and parents alike highlighted a lack of education on ABI as a barrier to their successful transition back to school (Backhouse & Rodger, 1999; Bogan et al., 1997; Bruce et al., 2008; Cheung et al., 2014; Mealings & Douglas, 2010; Richey, 2008; Rosenthal, 2013; Sharp et al., 2006; Todis & Glang, 2008; Vaidya, 2002). Greater understanding of the students’ needs in the classroom environment would have promoted a better supported, smoother transition back to regular classroom functioning and associated occupations. As one student in Backhouse and Rodger’s (1999) article explained, “ . . . teachers didn’t really help me much work wise, because they didn’t know where to place me. They’d never had anyone like this before” (p. 103). Similarly, students in Vaidya’s (2002) article suggested that lack of teacher knowledge posed a “major obstacle” to their return to school following ABI. One mother from Backhouse and Rodger’s (1999) study provided an illustrative example of her struggle with a teacher who did not understand the cognitive deficits that can result from ABI:
Cause we found that (it was like) talking to a brick wall with the teacher’s aides and the teachers to begin with, because I’d be saying, “Look, (S) is not coping with this, we’re not coping with it.” We were doing most of the homework at home for him basically. They were sending deadlines, saying it has to be done. And they didn’t listen to us at all. And they got me so (worked) up I felt I was breaking down just thinking of facing these people, and I didn’t want to feel like that on top of everything else. So I ended up avoiding them. (p. 103, parentheses in original)
Backhouse and Rodger (1999) mentioned that all parents in their study expressed frustration at some point because of their belief that teachers would not listen to them or accommodate their children’s classroom needs. This is an example of the ways in which educators’ lack of knowledge on ABI may contribute to a larger negative environment for the students and their families. This negative environment may, in turn, negatively affect students’ volition or drive to put effort into their school participation, while contributing to frustration among parents and students alike.
Parents also expressed frustration at their own lack of knowledge on available resources following their child’s ABI. Specifically, Backhouse and Rodger (1999), Todis and Glang (2008), and Richey (2008) all stated that parents expressed frustration at their own inability to find information. Richey summarized, “When parents and school professionals know what behaviors and characteristics they will be faced with and how to accommodate students returning to home from hospital and then to school following a TBI, it lessens frustrations for all concerned” (p. 100). The lack of education and access to information regarding transitions to school following ABI created frustration for educators, parents, and students, and impeded students’ abilities to regain or re-shape the classroom-based occupations that they possessed prior to their injury.
Communication-Related Factors as a Facilitator and/or Barrier
Eleven of the 20 articles discussed communication-related factors as facilitators and/or barriers to students’ transitions back to school following ABI (Backhouse & Rodger, 1999; Bogan et al., 1997; Bruce et al., 2008; Carter & Spencer, 2007; Cheung et al., 2014; Plotts & Jantz, 2012; Richey, 2008; Robson et al., 2005; Rosenthal, 2013; Todis & Glang, 2008; Vaidya, 2002). Students highlighted a lack of information communicated from clinicians or educators on how they can adjust to their new sequelae of ABI in the school setting (Bogan et al., 1997; Carter & Spencer, 2007). Students from Bogan et al.’s (1997) study did, however, find that when communicating with peers regarding how to navigate the daily challenges following from ABI, “the more you talk, the more you find out” (p. 436). The presence or absence of open communication on how to perform daily roles influenced students’ abilities to find adaptive ways to return to their disrupted occupations (Bogan et al., 1997). Understanding how to adjust back to daily life was important to students’ return to occupational engagement, creating routines around their new ways of performing occupations, and ultimately their ability to regain or achieve a new sense of normalcy in their daily lives.
Parents spoke at length about the detrimental effects of gaps in communication between the school, home, and hospital. Parents reported that their experiences of their child’s transition back to school was hindered by a lack of communication on available programs (Backhouse & Rodger, 1999; Richey, 2008; Todis & Glang, 2008), lack of preparation for the next steps in the rehabilitation process (Carter & Spencer, 2007; Cheung et al., 2014; Plotts & Jantz, 2012; Richey, 2008; Vaidya, 2002), and lack of available information in plain language that they could understand (Cheung et al., 2014; Richey, 2008; Vaidya, 2002). A lack of transparency and communication often interfered with parents’ abilities to support their child’s return to disrupted occupations, to identify their child’s support needs, and to know how to obtain that help. One parent from Richey’s (2008) article stated, “they had tried to explain to me at the hospital meeting but I can’t remember. Then again at the school they had tried to explain TBI [traumatic brain injury], but I didn’t understand some of the terminology” (p. 108, square brackets added). Another parent from Todis and Glang’s (2008) article described her struggle to keep teachers informed from year to year: “Every year I tried to start the year by informing new staff. They’d say, ‘Ok, ok,’ and then mid year, ‘Your kid’s got problems!’ Then they would spend the last half of the year trying to get something in place” (p. 255). This parent, like many others in the articles we reviewed (Richey, 2008; Robson et al., 2005; Rosenthal, 2013), made an effort to facilitate clear, early, and ongoing communication with the educators, but her efforts were often not recognized quickly enough to meet her child’s classroom needs.
Conversely, parents found that the presence of open and ongoing communication helped to create a supportive environment for their child’s return to classroom engagement (Bruce et al., 2008; Robson et al., 2005; Rosenthal, 2013). One parent in Bruce et al.’s (2008) article gave the following advice: “Keep in touch with the teachers. Keep them aware of the progress and what to expect, and limitations. And also if they see something wrong, act on it right away. Don’t wait” (p. 335). This advice, echoed by parents in Rosenthal’s (2013) publication, encourages parents to remain vigilant and advocate for their children to receive the attention and care they need. Communication must be bi-directional, whereby parents and students communicate new or changed needs to educators and school-based clinicians and demand feedback and ongoing communication in return. Parents and students reported that open, ongoing communication contributes to an environment of understanding in the classroom, which helps to focus everyone’s efforts on making sure that students are able to perform in their school-based occupations. Open, bidirectional communication that allows students to feel supported in their classroom-based occupational engagement may contribute to students’ volition to continue to work toward rebuilding classroom competencies.
Emotional Focus
Twelve of the 20 articles addressed participants’ emotional focus, as manifested through feelings of anger, frustration, and depression. Emotional responses varied between parent and child perspectives (Backhouse & Rodger, 1999; Bogan et al., 1997; Boylan, 2014; Berbaum, 2008; Carter & Spencer, 2007; Cheung et al., 2014; Linden & Jordan, 2012; Mealings & Douglas, 2010; Richey, 2008; Robson et al., 2005; Roscigno et al., 2011; Todis & Glang, 2008). Parents often conveyed frustration with the ways in which their child’s ABI was addressed in the school and the health care systems, rather than with the ABI itself. They sought support within their environments, which is important for regaining disrupted occupations (Molyneaux-Smith et al., 2003; Whiteford, 2000). One parent explained, “I could not get the school and the hospital on the same page. I became very frustrated with the system” (Richey, 2008, p. 117). Another stated, “I’m really fed up . . . he should be in an inclusive classroom with the other normal kids . . . I’ve been yelling at this placement all year, but it’s falling on deaf ears with the district” (Berbaum, 2008, p. 89). As outlined here, parents’ frustrations are related to the previously discussed issues of communication and education, but present prevalently enough to be addressed independently from the previous themes.
In contrast, students’ frustrations largely stemmed from their inability to engage in pre-injury occupations with the same level of functioning as they were previously able to. The inability to perform previously held occupations, or even the perceived inability to perform occupations as well as before, affected students’ volition to pursue those difficult occupations. For example, one student expressed anger and insecurity when a staff member tried to assist her while dressing: “I’m not stupid. I know how to do this!” (Berbaum, 2008, p. 113). Students also expressed frustrations over their need to repeatedly ask for help, their need to take frequent breaks, and their difficulty in understanding what was asked of them (Berbaum, 2008). Following their ABI, students also reported experiencing anger and aggression in their social interactions, anxiety, sadness, apprehensiveness, loss of control, decreased confidence, impulsivity, and panic attacks (Bogan et al., 1997; Carter & Spencer, 2007; Mealings & Douglas, 2010).
Finally, students simultaneously experienced the desire to cope and frustration that they had not returned to their pre-ABI functioning, or what they considered “normal,” activities. One student from Mealings and Douglas’s (2010) article said, “Knowing I could do something beforehand, before me accident and then knowing I couldn’t do it now . . . just messed with my head” (p. 7). A student from Bogan et al.’s (1997) article explained the difficulties of outside expectations for recovery:
One of the doctors said, not long after I had my accident, you’ll be fine, give it two years and you’ll be brand new and that was it, that was all he said . . . and as the two year date is coming up and I don’t feel any better, I feel worse. The two year date came and passed and I blamed myself constantly . . . I should be better, it is just me who is holding it back. (p. 436)
Students’ volition to continue pursuing previously held occupations diminished as time passed with little marked improvement, along with their belief that they would be able to perform such occupations again.
The desire to return to previous habits or routines to feel “normal” again led other students to move toward rebuilding their lives. For example, one student from Bogan et al.’s (1997) article recalled that her will to move on facilitated her coping: “I wasn’t feeling sorry for myself. I just put my head up and got on with my life” (p. 437). However, students’ continually evolving abilities affected their habituation of occupations, making it difficult to create a routine of stable occupations with their new skills and abilities. In addition to aggression and depression related to the ABI, students were also required to cope with the loss of their previous “normal” way of functioning and were unsure if they would ever regain it. For many students, however, admitting that they may never return to their previous functioning also triggered a desire to cope with their current level of functioning and begin the process of setting goals to accomplish pre-injury capabilities.
Peer Relationships
Thirteen of the 20 articles addressed students’ peer relationships (Backhouse & Rodger, 1999; Bogan et al., 1997; Boylan, 2014; Bruce et al., 2008; Carter & Spencer, 2007; Gauvin-Lepage & Lefebvre, 2010; Linden & Jordan, 2012; Mealings et al., 2012; Plotts & Jantz, 2012; Roscigno et al., 2011; Rosenthal, 2013; Sharp et al., 2006; Todis & Glang, 2008). For many students, reuniting with friends and returning to their social life was a major volitional contributor to transitioning back to school. As one student in Mealings and Douglas’s (2010) article remarked, “It was like that was the whole point of me wanting to go back to school like hang around with my friends” (p. 6). The desire to return to their previous social endeavors acted as a motivator to return to the school environment.
However, after returning to school, many students noticed changes in their abilities and opportunities to engage in peer relationships. The increased demands of rehabilitation on students’ free time, increased effort and hours to keep up with school work, and altered class schedules to accommodate their new curricula left students with less time to socialize with peers. A friend of one student with ABI shared that, despite giving up time with friends, her friend with an ABI “studied relentlessly and then she’d wake up the next morning and couldn’t remember what she studied” (Todis & Glang, 2008, p. 259). Another student described how the time required for rehabilitation impeded her social endeavors: “We were supposed to go away to [the state university] together and be roommates, but because of the accident I stayed home that year [to continue rehabilitation]” (Todis & Glang, 2008, p. 259, square brackets in original). Even during class time, students’ opportunities to socialize with peers were limited. At some schools, youth with ABI had special classes or spent time with an educational aide so they could cover material at a different pace than the rest of the class. While students’ volition to regain disrupted social occupation was strong, their inability to fit social occupations into their routine and maintain peer relationships led to continued difficulty returning to meaningful social endeavors.
When socialization did occur, some students with ABI noticed that their relationships had changed and their friendships were harder to maintain. One student in Bruce et al.’s (2008) article explained that the isolation and fear of rejection was difficult, stating, “Not being able to talk to people . . . was very hard because I didn’t know how people would react so I wanted to stay away from them” (p. 337). Another student from Roscigno et al.’s (2011) article explained that she had difficulty understanding why her friends were disappearing:
Yeah, [my friends came over at first] but then they saw me, and they saw the way I acted, and then they didn’t come over anymore. I think it happened pretty fast. [I knew by] the way they avoided me at church. Like, they would always like, I would be talking to someone, and then one of the other friends would say, “Oh, come on, so-and-so, let’s go do this! Bye, see you later!” And I was always kind of naïve of why they didn’t bring me, but yeah, later, I understood it all. (p. 888, square brackets in original)
Parents and peers suggested that other students distanced themselves from students with ABI because they demonstrated inappropriate behavior, comments, and reactions—all of which are common in youth following ABI (Kehle, Clark, & Jenson, 1996; Ylvisaker et al., 2005). One set of parents described the post-injury behavior of their son as being “socially inappropriate at times,” remarking that he “shows a lack of inhibition . . . misinterprets social cues or over-reads social cues” and struggles to understand social norms (Carter & Spencer, 2007, p. 49). Parents of another student who struggled to maintain friendships said her son’s “social misjudgments and subsequent behavior severely tested the one remaining, close, friendship he had” (Carter & Spencer, 2007, p. 45). Parents also indicated that when their children became aware of their social deficits, they were reluctant to participate in social activities. For example, the parents of one young man with ABI said that their son was “afraid of establishing an intimate relationship” (Carter & Spencer, 2007, p. 49). While peer support and social interactions initially acted as motivators to return to school for many, students’ changed abilities to appropriately perform peer-group occupations subsequently became a barrier to school reintegration.
Supports
Eleven of the articles addressed supports for students and families as they returned to school (Backhouse & Rodger, 1999; Bogan et al., 1997; Boylan, 2014; Bruce et al., 2008; Bruce et al., 2012; Carter & Spencer, 2007; Gauvin-Lepage & Lefebvre, 2010; Haarbauer-Krupa et al., 2013; Mealings & Douglas, 2010; Robson et al., 2005; Rosenthal, 2013). Peer relationships served as a major source of support but will not be addressed here as they were explored in the previous subsection. Students and parents suggested that support from family and the community were essential to the process of returning to school (Bogan et al., 1997; Bruce et al., 2008; Carter & Spencer, 2007; Gauvin-Lepage & Lefebvre, 2010; Mealings & Douglas, 2010). One student in Mealings and Douglas’s (2010) article explained,
They [family] wanted what was best for me sort of thing . . . like if I wanted to go back, they were with me on that . . . They were like with me all the way, like agreeing with me and sort of like, if he wants to go back let him go back and all this. Yeah, so yeah, it was pretty good. (p. 8, square brackets in original)
Parents also drew on the support of their neighbors and other community members. For example, community members told one mother in Gauvin-Lepage and Lefebvre’s (2010) article: “If you need help, don’t be afraid to ask” (p. 1092). Parents and students also described the support of professionals as helpful in the return-to-school process (Bruce et al., 2012; Haarbauer-Krupa et al., 2013; Mealings & Douglas, 2010; Rosenthal, 2013; Todis & Glang, 2008). For example, one parent in Rosenthal’s (2013) study reflected upon the ways to make the hospital-to-school transition more smooth and said, “The more support they have, the sooner they’re going to feel better about things” (p. 77). Specifically, participants cited teachers, integration aides, principals, school liaisons, and counselors as key agents in students’ successful and comfortable transition back to the classroom.
The absence of support also stood out to students and parents as significant (Backhouse & Rodger, 1999; Bogan et al., 1997; Bruce et al., 2008; Robson et al., 2005). Students in Bogan et al.’s (1997) article called for more support and advice regarding the mental and emotional “suffering” they experienced. Parents shared a desire for more support from teachers, rehabilitation staff, community programs, and their own partners. One parent shared her frustration with the school’s reasoning, recalling the following examples: “There was no money. There’s a bigger need. We have too many kids. We have one resource teacher . . . she would go weeks without any extra help” (Bruce et al., 2008, p. 335). Supportive environments, including supportive people and policies, are necessary to resolve occupational disruptions following major life events; the student and parent views reported in the articles reviewed show this holds true for the return to school following ABI.
ABI Sequelae in the Classroom
Eleven of the 20 articles specifically addressed the impact of ABI sequelae on students’ classroom reintegration and functioning (Berbaum, 2008; Bogan et al., 1997; Bruce et al., 2008; Gauvin-Lepage & Lefebvre, 2010; Mealings & Douglas, 2010; Plotts & Jantz, 2012; Roscigno et al., 2011; Sharp et al., 2006; Todis & Glang, 2008; Vaidya, 2002). The articles addressed ABI-related classroom challenges in three major ways. First, students described feeling different from their previous selves in the classroom (Bogan et al., 1997; Bruce et al., 2008; Gauvin-Lepage & Lefebvre, 2010; Mealings & Douglas, 2010; Roscigno et al., 2011; Todis & Glang, 2008). Parents and students alike provided examples of difficulties associated with the realization that students did not hold the same capabilities as before—and would have to learn how to adjust to the parameters of their new or changed levels of ability. For example, one student in Bogan et al.’s (1997) article explained,
The thing that really got me was I sat my prelims and now I’ve got my prelims on a bit of paper . . . and now they don’t mean anything. Now they could be someone else’s . . . I’m different now. I don’t have the same intellect as what I did then. (p. 436)
Teachers and parents did not always recognize or understand the effects of ABI on the students’ skills and knowledge and would urge students to try harder (Roscigno et al., 2011). Parents did, however, eventually recognize the toll that this took on their children. They witnessed the enormous effort put forward by their children to complete the simplest tasks, while coming to the realization that their children would likely have to change their previously held educational and vocational goals (Mealings & Douglas, 2010; Todis & Glang, 2008). This suggests that students and members of their support networks must adjust their expectations of what proficiency will look like for them as they return to previously held occupations following ABI. They will have new levels of ability—and will have to work within those parameters to return to their daily occupational engagement.
The second way in which ABI sequelae affected classroom experiences relates to students’ and parents’ negative experiences in the classroom following ABI (Bruce et al., 2008; Carter & Spencer, 1997; Mealings & Douglas, 2010; Todis & Glang, 2008; Vaidya, 2002). Classroom concerns ranged from students being ignored by teachers and passed through the system (Bruce et al., 2008; Mealings & Douglas, 2010; Todis & Glang, 2008) to teachers being unwilling to make accommodations in the classroom based on students’ new abilities (Mealings & Douglas, 2010; Todis & Glang, 2008; Vaidya, 2002). In Carter and Spencer’s (2007) case study, the school administration suggested that a student move to a new school following ABI, communicating that his previous school had additional academic requirements that the school did not feel he could meet. However, the student and his family did not consider this “a viable option” because it would remove him from the physical and social settings that he was familiar with, which they felt would cause him more difficulty and confusion. Another student from Todis and Glang’s (2008) article suggested that he felt ignored by his teachers, stating, “I graduated with a B average, and for the last two years they said I didn’t need special ed anymore, but I never really learned to read or write” (p. 258). Such an oversight might lead to delays in resuming disrupted occupations following ABI, as a supportive environment is critical to occupational performance and growth (Kielhofner, 2008; Whiteford, 2000). It will likely also hider transitions into and through future occupational opportunities that require literacy and basic classroom skills.
The final area of ABI sequelae in the classroom involved receiving help in the classroom itself. Berbaum (2008), Mealings and Douglas (2010), Plotts and Jantz (2012), Sharp et al. (2006), and Vaidya (2002) all highlighted the need to put mechanisms in place to help students reintegrate into the school setting—for example, by allowing students time to leave class early to avoid crowded hallways (Vaidya, 2002) or being flexible in demands when seizures or other conditions must take priority (Berbaum, 2008). One parent in Gauvin-Lepage and Lefebvre’s (2010) article explained that her daughter “got through her days, but she took small breaks” (p. 1093). A student in Mealings and Douglas’s (2010) article met with his principal and speech language pathologist and found “ . . . that was really helpful as well, just sort of organising what was going to happen, sort of had a bit of structure to go back and have a try of certain things” (p. 9). Having these simple accommodations, and professionals who were willing to provide them, helped students to transition more smoothly and left them feeling supported as they habituated to new ways of being in the classroom.
Discussion
Students’ volition to return to disrupted occupations or engage in new ones was often affected by their own desires, as well as their perceptions of other people’s expectations. Students benefitted from supportive environments in which adults and peers were educated on ABI and its sequelae, and perceived support helped students feel comfortable and motivated to try to regain occupations. Similarly, Mealings et al. (2012) found that students benefitted from being included in communication and ongoing planning regarding their education, as well as from feeling supported and validated in their progress.
Students throughout the included studies said that their volition was also affected by their emotions, outlook, and affect following ABI, including emotional distress, depression, anxiety, anger, and fear. Similar emotional and mental health issues have also been explored in the wider ABI-related literature (Ilie et al., 2014; Mealings et al., 2012; OBIA, 2012). The range of emotions identified by students and parents in the articles we reviewed might be related to emotion-oriented coping, where emotional reactions and ruminative behaviors may comprise part of the student’s strategy to attempt to reduce stress (Harper, 2012). According to Harper (2012), the way that individuals cope with stress determines their functional outcome, as well as later engagement in their daily lives.
Students’ habituation, including their social roles, is also affected following the occupational disruptions of an ABI. In the articles we reviewed, students’ abilities to maintain previous relationships or create new ones affected their emotional experiences following ABI and their desire to attend and participate in school. Previous studies have also described restricted social interactions and ability to interact with peers as a notable outcome for children and youth with ABI (Bedell & Dumas, 2004; Glang et al., 1997; Savage, Pearson, McDonald, Potoczny-Gray, & Marchese, 2001). According to Rauch and Ferry (2001), students with ABI tend to have smaller social networks, but the presence of supportive social networks can buffer the negative emotional and mental health effects that accompany isolation and self-doubt following ABI. They argue it is necessary for a student to recognize and value the support he or she receives, for him or her to benefit from it. Glang et al. (1997) also touted the role of peers in providing support to students transitioning back to school following ABI, and they created a specific intervention aimed at fostering supportive social interactions in the school following ABI. Glang et al.’s (1997) findings support the findings of our review, in that students’ maintenance of peer relationships—and the support they received from those relationships—helped them reintegrate into their school and social lives. Conversely, a perceived lack of social identity or perceived outsider status was related to increased emotional difficulty, and it affected the students’ desire to return to school or remain in the school environment.
Following ABI, students’ performance of school-related occupations was affected physically, socially, cognitively, and behaviorally. Students and their parents expressed frustration with their actual or perceived ability to perform in classroom settings. Mealings et al. (2012) listed a number of cognitive, emotional, physical, and psychosocial difficulties that affect classroom participation, such as fatigue, memory issues, organization skills, difficulty making decisions, anxiety, reduced motivation, physical inability to write, difficulties with vision or hearing, pain, dizziness, speech issues, and general social concerns. Many physical and some cognitive issues can be accommodated while a student is in rehabilitation and long-term plans can be put in place; however, as described above, emotional and social issues are often more complex to address.
In addition to their true ability to perform tasks and activities involved in their school-related occupations, students’ perceptions of their abilities also affected their engagement. For example, some students eventually abandoned social or educational occupations because they perceived that their peers were excluding them or their educators were not supportive, encouraging, or understanding of their new or changed abilities. To return to occupations, students required accommodation for skills and tasks that they were no longer able to complete, assistance with tasks that they might regain or perform differently than before, and encouragement to continue to strive toward engagement in a way that matches their abilities.
Finally, as stipulated by Whiteford (2000), supportive environments are essential in regaining of disrupted occupations. In OBIA’s (2012) survey of adults who had experienced ABI, only 40% of respondents indicated they were satisfied with their “ability to receive the support [they] need” (p. 47). While this statistic applies to an adult population, the articles included in this study indicate similar concerns for children and youth. Savage et al. (2001) stated that family-centered care and professional support for the family throughout the process—including consideration of the families’ preferred times and venues for meetings, provisions of information ahead of time so families have time to review it and ask thoughtful questions, and ongoing communication with families—are helpful in the return-to-school process following ABI. By supporting the family unit in navigating services and transitions, professionals allow the family to support the student themselves in the transition process. Gan, Gargaro, Brandys, Gerber, and Boschen (2010) provided a number of recommended supports for families following pediatric ABI, including supports for the student, peers, professionals, and family supporting them, respite care, family counseling, and future planning. Within the school environment specifically, they identified the support of educators and administrators as helpful when present. Educators have similarly reported thinking that families and students must be supported in the return-to-school process (Berbaum, 2008; Bruce et al., 2012; Cheung et al., 2014), but they posit that the family is often its own biggest support, through family advocacy (Berbaum, 2008; Richey, 2008).
Educators, administrators, parents, and others can provide support by developing an understanding of the student as a person and ABI as a disability. Education and communication between stakeholders can foster this process. The distinct absence of education on ABI for educators, families, and students is unique neither to our findings nor to ABI as a condition. Similar issues have also been identified in other studies of ABI (Gan et al., 2010; Hartman et al., 2015; Mealings et al., 2012; Savage et al., 2001), as well as research on autism (Lindsay et al., 2013) and cancer (Prevatt, Heffer, & Lowe, 2000). Greater education for all stakeholders—including education on what to expect from the student, what gains are likely and unlikely to be made, and best-practices for modifying classrooms, social time, and curricula—will allow for more accurate expectations and successful curricular planning for students’ return and reintegration following ABI. Other studies also highlight the importance of peer education on disabilities such as cancer and ABI and their associated sequelae (Glang et al., 1997; Prevatt et al., 2000). In addition to the issues described by parents and students in this review, the literature indicates that educators agree with the need for clear, ongoing communication between stakeholders to foster an environment where students can thrive (Ball & Howe, 2013; Berbaum, 2008; Mohr & Bullock, 2005; Richey, 2008; Smith, 2005; Vaidya, 2002).
Future Directions
Future directions for research on hospital-to-school transitions following ABI are manifold. First, formal communication and educational channels for parents, educators, clinicians, and students should be created. This will promote the appropriate and sensitive communication of information to help students to transition back to educational settings that are appropriate for their cognitive and recovery levels. These communication and educational channels should include all stakeholders that contribute to the support and education of students, families, and educators. Based on the included studies, we believe that it is crucial to have a space for parents and students to advocate for their ongoing and evolving needs throughout the transition process and beyond. In addition, a holistic approach to the reintegration process should be instituted. That holistic approach should address the cognitive, behavioral, physical, and academic abilities of students, as well as their evolving social and emotional needs throughout the transition process.
Furthermore, the interventions and formal channels described above should be researched for their utility in supporting students’ transition back to school following ABI. Researchers should consider the perspectives of various stakeholders—including students, parents, educators, rehabilitation specialists, government funders, school boards, and so forth—as well as the fidelity of the interventions themselves. Finally, more research is needed to explore whether hospital-to-school transitions differ by age of the student, gender, ethno-cultural status, geographic location, socio-economic status, and type of school (i.e., public, private). These factors are relevant to the return-to-school process because they might affect the geographic and economic availability of services to students and educational institutions.
Limitations
Our literature review was limited by our ability to read only English-language articles, as well as our use of English search terms. In addition, we did not discriminate between research on different types or experiences of ABI, including the type or severity of injury, the length of time since injury, or the services available or sought by participants. Finally, we did not discriminate between research on different types of educational settings or different spans of time between students’ injury and return to school.
The articles themselves presented several limitations as well. Similar to our own limitations, many of authors did not differentiate between levels of injury, time elapsed since injury, or level of education before injury. Only 15 articles reported participants’ genders (Berbaum, 2008; Bogan et al., 1997; Boylan, 2014; Bruce et al., 2012; Carter & Spencer, 2007; Cheung et al., 2014; Gauvin-Lepage & Lefebvre, 2010; Mealings & Douglas, 2010; Richey, 2008; Robson et al., 2005; Roscigno et al., 2011; Rosenthal, 2013; Sharp et al., 2006; Todis & Glang, 2008; Vaidya, 2002). Only five reported students’ ethnicities (Berbaum, 2008; Richey, 2008; Roscigno et al., 2011; Todis & Glang, 2008; Vaidya, 2002). Only eight discussed social class (Berbaum, 2008; Bogan et al., 1997; Bruce et al., 2012; Bruce et al., 2008; Cheung et al., 2014; Gauvin-Lepage & Lefebvre, 2010; Roscigno et al., 2011; Todis & Glang, 2008). Social factors, as mentioned previously, may affect geographic and economic availability of educational and health care services for returning students. Moreover, most of the articles we reviewed did not report the pre-morbid learning status of students beyond sporadic self-reports from participants. Information regarding prior learning abilities might be relevant to our understanding of students’ knowledge, including the knowledge they lost and gained following pediatric ABI. Our recommendations should be considered in light of these limitations.
Conclusion
In our review, we synthesized the findings of 20 articles on the transition back to school following hospitalization for ABI from the perspectives of parents and students. In these articles, we identified six areas of focus for families and students following ABI, including (a) lack of education on ABI for families and educators, (b) communication-related factors as barriers or facilitators to the reintegration process, (c) emotional focus, (d) peer relationships, (e) support for students and family, and (f) ABI sequelae in the classroom. The return-to-school process is a gradual journey. Along this journey, students learn more about their new and evolving selves. These views are not only influenced by their abilities but also by their outlooks, emotions, social processes, and self-perceptions.
Based on the articles we reviewed, we suggest that fostering supportive environments allows students to strengthen their volition to regain occupations, roles, and perceived and actual skills following ABI.Future research should focus on formalizing processes to support students and families as they transition back to school. If properly supported in the transition back to school and daily function, students and their families can explore new ways of engaging in desired and necessary occupations and successfully reintegrating back into the physical, social, and cognitive realms of school.
Footnotes
Acknowledgements
The authors acknowledge the contributions of Pui Ying Wong, Health Sciences Librarian, in the data collection process.
Authors’ Notes
Alana Tibbles and Alicia Paniccia are both credited with equal contribution and second authorship of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.