
Abstract
Introduction
Chemotherapy daycare units (CDU) routinely face difficulties, given the waiting time and work pressure. The study objectives include determining the feasibility of a multidisciplinary intervention in facilitating the growth in CDU bed utilization by ∼20%.
Methods
The quasi-experimental study was conducted during the period 1st May 2021 to 28th February 2022. The strategies of the healthcare improvement project are structured as per the Plan-Do-Study-Act (PDSA) cycle. ‘Lean thinking’ approach using the A3 sheet tool was applied, as its focus is on organization of processes. Benchmarking technique was used to attain more insight into the optimal performance levels.
Results
Plan phase: The tracks of CDU process were mapped using the ‘process flow diagram’ technique. The reasons for the perceived bed shortage and high work pressure were revealed by the Root cause analysis, which includes the 21 prioritized problem areas.
Do phase: Various interventions were implemented in the domains of communication systems, developing standard operating protocols and human resource management.
Study phase: 9 of the total 21 problem areas were cumulatively responsible for ∼80% of underutilization of CDU beds.
Act phase: The planned intervention resulted in an increase in the proportion of CDU bed utilization from 60% (18-20 patients/day) to 75% (23-25 patients/day).
Conclusion
The PDSA cycle offered optimal structure to this efficiency improvement initiative. The project outcomes were enhanced by the combination of approaches such as lean thinking and benchmarking.
Highlights
Cancer patient related services were observed in the study, and their movement through the system was measured,
Process level metrics formed the construct of study analysis, and intervention measures were implemented,
An improvement in efficiency was observed at the CDU which includes an increase in the bed utilization proportion from 60% to 75%.
Introduction
Quality improvement techniques in healthcare have traditionally focused on treatment issues and patient–physician relationship. Recent developments are focusing on issues such as timeliness and efficiency. Such units routinely face difficulties, given the waiting time and work pressure. A few common reasons for delay at the infusion center include late chemotherapy orders, waiting time for laboratory results and preparation of medications in the Pharmacy. 1 Parkes et al. 1 report the longer than expected wait time among ∼74% of chemotherapy patients at the infusion center, which in-turn affects their perception of quality of care.
The study discusses the approaches of a hospital-based chemotherapy daycare unit (CDU) towards increasing its efficiency by improving the proportion of bed utilization. It reviews and explores the current practices, and identifies areas of improvement at the CDU. The concerned hospital has 28 beds for chemotherapy administration, among which in-patients are 7 beds and daycare includes 21 beds (which is managed in two shifts). Many patients at the hospital are covered by public insurance scheme with a few preferring to pay the expenditure as out-of-pocket. A teamwork approach is required for the safe administration of toxic chemotherapy, and various checkpoints in the process include patient evaluation by Physicians, assessment of blood parameters, nursing evaluation, review of orders by the pharmacy and preparation of medication.
Other reasons for delay at the infusion center include overdue submission of chemotherapy orders and review of prescriptions by the Pharmacy. 1 The aim of the project is to improve the equity of access to CDU and the patient outcomes. The primary objective of the study includes determining the feasibility of a multidisciplinary intervention at Indrayani Hospital and Cancer Institute in Pune, India, using the Plan-Do-Study-Act (PDSA) cycle. The secondary objective is to enable the growth in bed utilization by at least 15% without proportionally adding more staff members. However, such change measures were simultaneously planned, while sustaining the prior logistic support system, quality of care and patient outcomes.
The business approach for improving efficiency includes ‘lean thinking’ which emphasizes on the organization of process. Its focus is on providing effective healthcare services to patients visiting the CDU. Each activity in the process is streamlined towards adding value for patient care, and includes an efficient delivery of services when needed by the patient. The tools used for improving the business process of CDU are discussed in the Methods section. The research is quasi-experimental in nature, lacks a control group and pre-post intervention measurements. Some of the challenges for process improvement projects in oncology care include the complexity of treatment services and the periodical changes subsequent to the innovation.
Methods
The strategies of this quasi-experimental healthcare improvement project are structured as per the Plan-Do-Study-Act (PDSA) cycle. It utilizes the collaborative efforts of physicians, nurses and pharmacists. This method is allied with clinical oncology practice at the CDU, as treatment is provided under close observation and accumulating evidence enables an improvisation of service delivery. Lean thinking approach using the A3 sheet tool was applied, as its focus is on the organization of process. Such an approach enables an effective and efficient administration of treatments to cancer patients. ‘Benchmarking’ was also used to attain more insight into optimal performance levels. The duration of the Project was from 1st May 2021 to 28th February 2022. The time required per phase is listed in Table 1, and the phase-wise application of lean management tools and benchmarking are further described.
Timelines for the various Plan-do-Study-act Phases.

The concerned unit provides chemotherapy to 30–32 patients/day. Add on cases and old pending cases include an additional 2–3 patients/day. The number of unfit patients includes 1–2/day and absentees include 1–2/day. The percentage of bed utilization/day was computed as: (total number of beds utilized/day)/(total number of beds available/day)* 100.
Results
Plan Phase
The process at CDU was analyzed during the plan phase. Lean thinking technique using the A3 sheet tool was used for an in-depth process analysis of the CDU. A3 problem solving is a lean approach for reporting issues and presenting ways of addressing them. The process of patient journey during the infusion services and production of chemotherapy was observed, and the tracks were mapped using the ‘process flow diagram’ technique. The reasons for the perceived bed shortage and high work pressure were revealed by the Root cause analysis, which includes the 21 prioritized problem areas.
Observations in Figures 1 and 2 entail the various tracks which patients fulfill on their visit to the CDU. The phase of treatment determines the movement of patients across the domains. Given the impact of each group on the process, it is imperative to optimize the flow in a group-wise manner.

Process map for treatment on day 1.

Process map for treatment on day 2.
The fish bone diagram as depicted in Figure 3 is a quality management tool, and was used in the study to find the root cause of the process change failures. This tool enables brainstorming, and seeking the right solutions for eliminating the problems faced by the organization. The head of the fish portrays the problem as underutilization of CDU beds and each bone of the spine depicts the potential causes of the problem. Each problem has sub-categories which are included to find the effects of the causes. The CDU staff members identified the gaps in the process steps, and assigned priority for the same which was assessed in the ‘rapid plant assessment’.

Fish bone diagram of root cause analysis.
The routine practice at CDU has been to initiate preparation of chemotherapy regimen, after arrival of the patient. Even the laboratory tests were done on the day of chemotherapy infusion, which results in a 2 h delay for the supply of medication from pharmacy. The bed utilization rate was also influenced by the variance in daily demand, along with contrasting appointment schedules. The measurement criteria include variables such as waiting time, medication preparation time and the time spent on bed until medication is administered. This analysis enumerates the mismatched scheduling of the logistics available at the specific time, which results in distinct planning systems at the CDU.
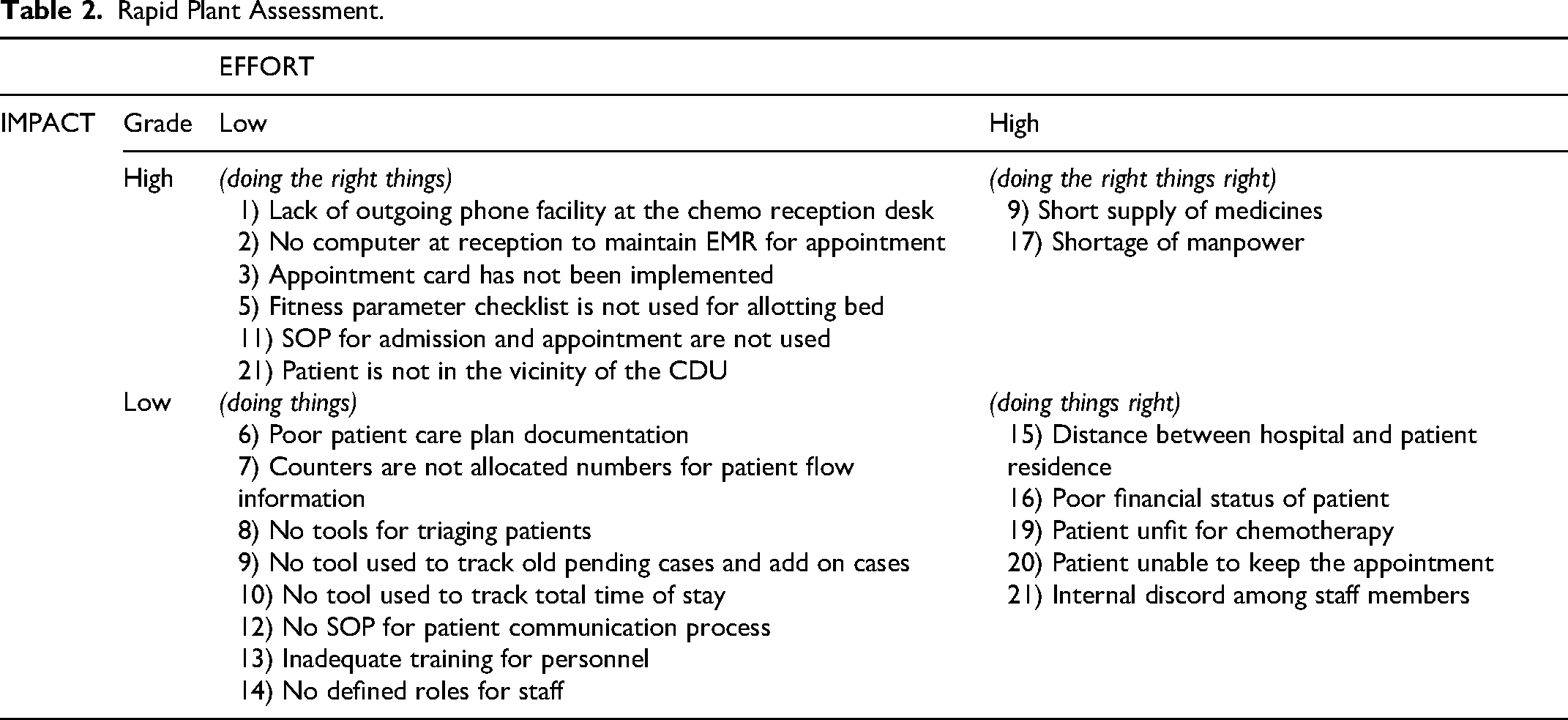
The ‘Rapid plant assessment’ (RPA) process was implemented for quickly evaluating the CDU on overall operations and progress in lean transformation. The 21 key problem areas identified in the Root cause analysis were stratified (Low/High) based on their effectiveness (Impact) and efficiency (Effort). Table 2 provides a single view of the health of the CDU's operations system. The findings offer insights about the unit's strengths and weakness, which in-turn creates a priority list of actions for developing the roadmap.
Rapid Plant Assessment.
Do Phase
A multi-disciplinary team from the CDU developed a new planning system which delivers optimal value for patients and staff. Figure 4 depicts the various interventions which were implemented for the communication systems, development of standard operating protocols and human resource. The revised efforts include Physician signing the chemotherapy orders by 1 pm, a day before the patient's infusion center appointment. The nurse reviews the list of patients and informs the pharmacist about the chemotherapy orders. Depending on the stability of drugs, the nurse prepares the mixing of chemotherapy following registration of the patient. Some exceptions include short stability drugs, monoclonal antibodies, first cycle of chemotherapy and for in-patients.

New planning system.
Following the recommendations from the previous phase, the multidisciplinary team comprising medical oncologist, medical officer, CDU nurse, pharmacist and the administrative secretary held deliberations on its implementation. The team identified the opportunities for improvement, which includes developing an effective patient communication system for streamlining the demand and improving the flow of patients, standard working procedures for patient appointment and management, and human resource for managing the staff ergonomics.
An important component was to align the planning method with the relevant departments as depicted in Table 3, towards improving the patient throughput. The measures to sustain the effect of planned interventions include multidisciplinary teamwork and implementation of the health information management system.
Measures to Sustain the Intervention.

Study Phase
Through a questionnaire, the staff members opined on the priority areas of concern. The scoring for each problem was factored based on their responsible input. Given its level of impact on the CDU process, each problem has been assigned a numerical score with the highest score indicating a greater impact. There was a total of 21 problems (areas of concern), and initial 16 of them were cumulatively responsible for ∼80% of underutilization of CDU beds. The most impactful causes in the process and their scoring are depicted as a Pareto chart in Figure 5. The column percent of each problem adds cumulatively to 100% as depicted by the red lines.

Pareto charting of factors influencing quality control.
The defects were prioritized in-order to observe the greatest overall improvement. The occurrence of the type of defect is listed in a descending order starting with the shortage of manpower, lack of appointment scheduling, lack of computer for maintaining the electronic health record, etc. Although Pareto analysis does not provide solutions to issues, the CDU will benefit by allocating resources to those with higher scores.
In the study, we used the achievable benchmarking methodology for establishing the target bed utilization rate. The baseline and target percentage for bed utilization rate were determined as 60% and 75% respectively, following literature review and desk research. The bed utilization at the CDU as shown in Figure 6, was ∼60% (18-20 patients/day), which increased to ∼75% (23-25 patients/day) post-intervention. Establishing a benchmark for performance provides a framework for quality improvement initiatives, 7 which conduced the process of continuous advancements. The capacity and demand parameters are of importance towards planning the system-wide workforce and services.

Benchmarking of bed utilization proportion.
Act Phase
Some salient outcomes which are a result of the intervention include:
New reception counter was formed for single point of communication for chemotherapy patients, Patient tracker developed for tracking chemotherapy cycles and for patient communication, Appointment card implemented for patients, Staff trained for appointment scheduling and reminder calls, New software for ONCOEMR to ensure tracking of patients and implementation of patient calendar, Increase in utilization of chemotherapy beds from 60% to 75%.
It was an arduous task to remind the staff regarding patient follow-up activities, which include telephone reminder calls. On occasions, implementation of the intervention does not lead to the desired results. In this context, the Project team deliberated on the challenges which include training the elderly staff towards adapting the new flow of process. Other complex issues include optimization of administrative processes at the CDU, and convincing the hospital management towards devoting resources for the change process in the system.
Discussion
Given the demand for cancer treatment, there is a compelling need for health services to increase efficiency and maintain optimal costs. The process of chemotherapy treatment includes various events starting from the first consultation with the Physician, lasting till the last cycle of treatment administration and extending to follow-up schedules. The process flow involves an organized set of activities, which bridge the missing links between the departments and ensure consistency in treatment services.
The PDSA cycle offered a structure to the Project, and the combination of lean thinking and benchmarking enhanced the results. The process flow diagram (Figures 1 and 2) identified the opportunities, which in-turn entitled the identification of problems in each area through a fish bone diagram. The new Planning system was devised considering the best practice of these processes. The seamless collaboration of the multidisciplinary team enabled the effective implementation of the intervention, and the members include infusion center staff, pharmacists, nurses and the attending Physician. As a result of the intervention, an improvement in efficiency was observed at the CDU which includes an increase in the bed utilization proportion from 60% to 75%.
In the recent past, healthcare systems have successfully applied lean methods and tools from the manufacturing industry. Lean thinking involves assessing what tasks add value to the organization, and identifying ways to eliminate things which do not add value. 2 Such methods have proven to be effective in workplace processes towards eliminating waste and redundancy. 3 The lean project improved the process flow for patients towards ensuring a comfortable experience and outcomes. The framework of rapid plant assessment includes assessment of new course of action and determines whether the department is lean. For ensuring a high standard of care, there is a compelling need to benchmark performance around capacity, demand, and efficiency of services.
A study by Alonso et al. 4 reports the process mapping of the chemotherapy daycare services, where-in the existing problems were analyzed throughout the process. The study reports key measures for improving the chemotherapy process which include a better linkage between medical staff, pharmacy and the administrative staff of CDU. Also, benchmarking against other tertiary cancer centers was done for ascertaining the chemotherapy practices. Other measures include improving communication, completion of standard chemotherapy forms by the Oncologist, weight forms for the patient and creation of patient information support group.
Parkes et al. 1 report the feasibility of a multidisciplinary chemotherapy pre-preparation intervention at a community hospital in US. The outcomes of such an efficiency initiative include the improvement in average chemotherapy turnaround time (70% decrease, p < .001) and patient cycle time (30% decrease, p < .001). This also resulted in a reduction of patient wait times, and enhanced satisfaction of both patients and employees. The authors also report a reduction in the cost of wasted chemotherapy (<$300) after the first month of implementation, and that the interventions did not negatively affect the capacity of the infusion center.
The healthcare improvement project by van Lent et al. 5 was structured according to the PDSA cycle. The value stream map in the study shows that patients with previous appointments are likely to arrive later than those without. The reported bed shortage and high work pressure when assessed by the Root cause analysis technique, revealed the cause as unequally distributed daily demand with peaks around 11 am and 1.30 pm. The planning system was at fault as the scheduling did not match with the availability of nurses and beds at a specific time. Due to the delayed lab results, it was found that the medication was often ordered after the original appointment time. The improvement areas as appointed by the Rapid plant assessment include information transparency and materials management. An improved planning system was thus perceived to enable the treatment of a similar number of patients with 30% less beds in an ideal situation.
The robust framework of a lean improvement methodology in managing the complex system constraints within the CDU has been reported by Lingaratnam et al.'s 3 study. This project resulted in a 38% reduction in median wait time on the day of infusion (from 32 to 20 min, p < .01), 7-day reduction in time to commencement of treatment for patients who received a combined chemoradiotherapy regimen (from 25 to 18 days, p < .01), and 22% reduction in wastage associated with expired drug and pharmacy rework (from 29% to 7%, p < .01). Efficiency improvement of the cytosuite enabled a 29% increase in the proportion of products manufactured within 10 min of appointment time (from 47% to 76%, p < .01).
Gjolaj L.N et al 6 studied the effectiveness of having a dedicated phlebotomy station inside of the infusion unit and a workflow for processing the patient samples immediately, which resulted in a 53% decrease in laboratory turnaround times (24 min vs baseline 51 min) and subsequent wait times. This project used the DMAIC (define, measure, analyze, improve, control) method to assess the critical to quality (CTQ) metrics, which include the patient wait time and laboratory turnaround time. In the ‘measure’ phase, baseline data were collected for the CTQ metrics and a Pareto diagram was created using 92 observations of delay. Missing treatment orders and laboratory delays were found to comprise 50% of all delays.
Some of the reasons for causing delay in the infusion center include late orders for chemotherapy and preparation, waiting time for reporting of results from the laboratory, review of orders by the pharmacy and preparation of medications. 1 Addressing these issues as well as other checkpoints for patient safety, will ensure an improvement in the efficiency of CDU as well as patient satisfaction. The results of the study are generalizable to other oncology practice settings, including those treating underprivileged patients covered by public insurance schemes. The success of our methods should be proved through research in comparable settings, mindful of the socio-dynamic processes in the organization which determine the use of control groups for such an exercise. The success rate is dependent on the current performance levels and improvisations done to the quality aspects.
Limitations
Certain quantitative indicators such as average patient cycle time should have been computed, which is measured as time from patient check-in to check-out from the CDU. However, this parameter was not calculated in the study, either as pre or post-intervention,
Similarly, another indicator is the average chemotherapy turnaround time, which is measured as the time from chemotherapy request by the nursing staff to its delivery by the pharmacy. We did not calculate it either as pre or post-intervention,
Following the intervention, objective measures for assessing the growth in patient numbers, staff productivity, reduction in overtime duty and employee/patient satisfaction need to have been developed,
Conclusion
PDSA is a systematic approach which supplements the problem-solving expertise required for proposing accurate solutions. The business approach of ‘lean thinking’ enabled a streamlined flow of services at the CDU, including delivery of services in a precise and accurate manner. With the available evidence, benchmarking enabled defining the performance targets. The new planning system enabled the integration of a set of interventions, which entitled an improvement in the process design leading to an increase in the efficiency of CDU. In the study, some business approaches were adapted to the healthcare system, and their successful application enabled an increase in the proportion of bed utilization. The study can have a positive impact on other oncology settings facing problems related to patient flow process or bed utilization systems.
Footnotes
Acknowledgements
1. Dr. Sanjay deshmukh. Managing Trustee, Indrayani Hospital and Cancer Institute, Alandi-Chakan Road, Alandi, Pune, India.
2. Dr. Radheshyam Naik, Group Medical Advisor, Senior Medical Oncologist, Healthcare Global, Bangalore, India.
Clinical Trial Registration
This study is not a trial.
Data Availability Statement
Due to privacy concerns, the data can be accessed by communicating with the corresponding author on the email: drvinod.r@hcgel.com
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval Statement
Since no intervention was done on human subjects directly, the Institutional Ethics Committee provided a waiver vide: NSMFEC121, dt: 17/4/2021.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Patient Consent Statement
Since patient care activities were only observed and measured, without any interviews or interventions, obtaining informed consent was not necessary.
Permission to Reproduce Material from Other Sources
If done for academic purposes, permission need not be sought. However, when used for commercial purpose, permission need to be taken.