
Abstract

Introduction
Opioid analgesics can be prescribed to patients presenting with acute noncancer pain in primary care.1,2 In a recent study, 3 we demonstrated that providers who received emails comparing their opioid prescribing patterns to other providers prescribed less opioids to patients presenting with acute noncancer pain at initial visits compared to providers following an electronic health record (EHR) guideline. In follow-up to this primary study, we examined patient reported pain, pain interference with function and activity, and treatment satisfaction across these different provider-facing interventions.
Methods
The parent study was a multisite, cluster-randomized clinical trial of opioid-naïve patients (≥18 years) presenting with acute musculoskeletal pain or non-migraine headache. Patients were recruited between September 2018 and January 2020 from 48 primary care clinics representing three healthcare systems. Patients were seen by 525 providers from one of four conditions: (a) control (providers received EHR guideline on opioid prescribing at time of initial visit), (b) opioid justification (control plus a request to enter free text justification for prescribing opioid); (c) provider comparison (control plus monthly e-mails regarding their opioid prescribing practices compared with peers); and (d) opioid justification and provider comparison combined.
In a sub-study, a pre-specified secondary outcome was a composite average mean score of reported pain and pain interference with function and activity over the past week as measured by the three-item pain, enjoyment of life, and general activity (PEG) scale. 4 Satisfaction with treatment was measured by a single-item Likert scale from 1 to 10, with 10 indicating highest satisfaction. The PEG was administered at the initial qualifying visit to establish a baseline 4 and online or by phone with the satisfaction scale at 1-, 6-, and 12-month follow-ups. We had 87–99.9% power at baseline mean PEG scores of 3.5, 5.0, and 6.5 to test for equivalence of PEG scores among comparator groups through 12 months of follow-up. We also collected demographic (age, gender, and race) and opioid prescription data at baseline.
To examine differences in patient outcomes by intervention condition, we conducted a repeated-measures ANOVA via SAS software version 9.4 at each follow-up. We reported average mean scores and standard deviations for PEG and satisfaction at each time point. Per IRB-approved protocol, patients provided verbal consent to participate in this study.
Results
Of 2237 patients with baseline PEG scores, 38 (1.7%) received an opioid prescription at initial qualifying visit and 1142 (51%) reported a PEG 4, indicating moderate to high severity. Of those with a baseline PEG, 605 (27%; mean age 46.5, 46% female, 91% White, 7.3% Hispanic) agreed to follow-up surveys. PEG scores decreased across all intervention groups at 1-, 6- and 12-month follow-ups compared to baseline (Table 1); no significant differences in PEG scores were observed across these groups (Figure 1). Overall, patient mean satisfaction ratings were high (>7.5) at 1-month follow-up and steadily improved at 12-month follow-up across all groups (Table 1). We observed no significant differences in patient satisfaction across groups.

PEG scores at baseline and follow-up, by provider-intervention group.a
PEG Scores and Satisfaction Ratings From Baseline to 12-Month Follow-Up, by Provider-Intervention Group.
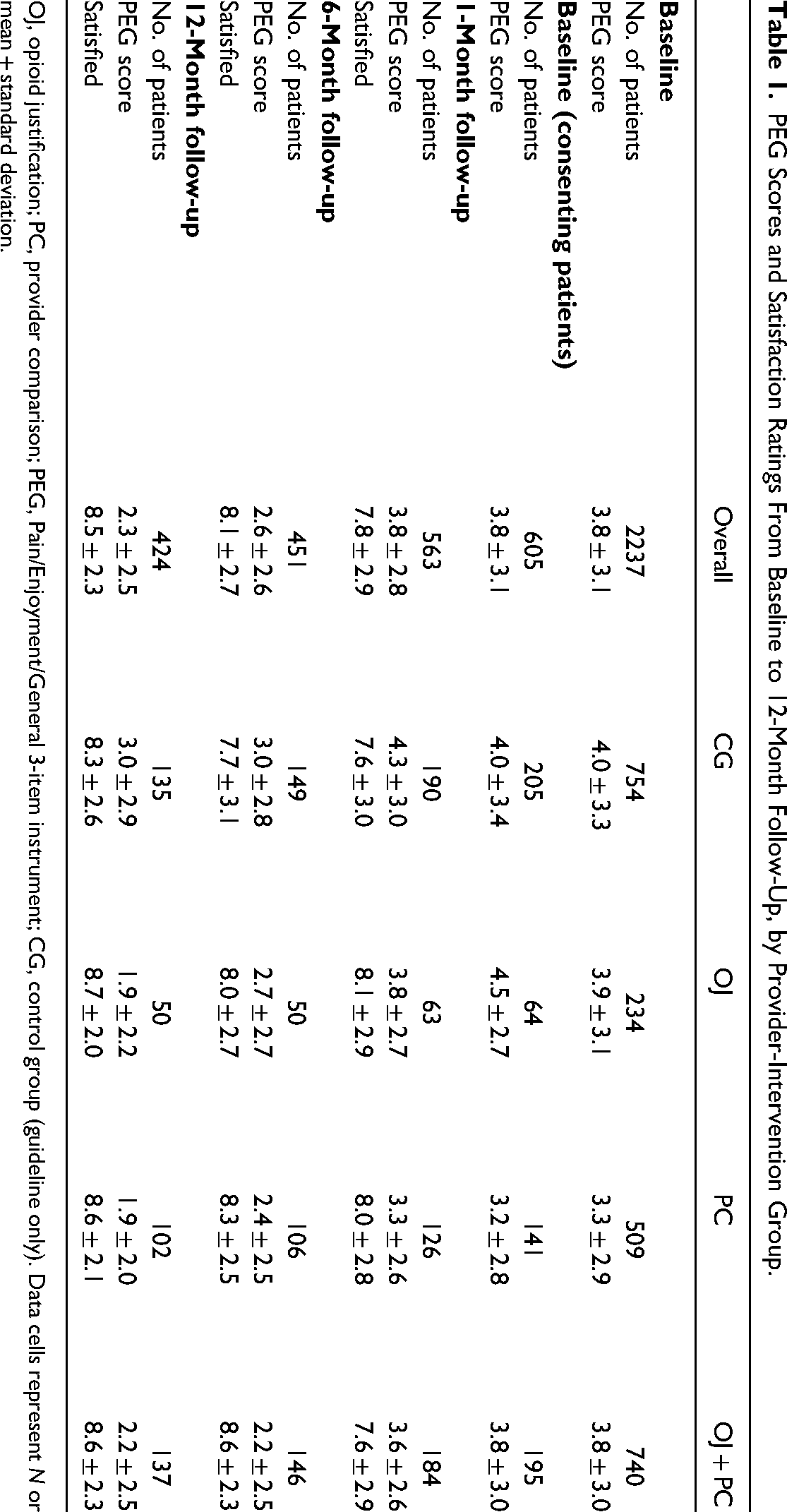
OJ, opioid justification; PC, provider comparison; PEG, Pain/Enjoyment/General 3-item instrument; CG, control group (guideline only). Data cells represent N or mean + standard deviation.
Discussion
As this study evaluated an acute musculoskeletal pain cohort, pain outcomes were expected to improve in most patients. Indeed, opioid-naïve patients presenting with acute noncancer pain in primary care reported steady improvement in pain intensity and interference, and treatment satisfaction across 12-months of follow-up. A key finding from this clinical trial is that pain improved at approximately the same degree whether or not patients were in an intervention condition that lowered initial opioid prescribing. These findings add to the evidence supporting provider-facing interventions to reduce unsafe opioid prescribing and subsequent risk of misuse and chronic opioid therapy.3,5,6
Limitations of this study were low and disproportionate participation rates (ie, 99% of results were from one health system), population-based comparisons only, and lack of data on non-opioid pain treatments delivered.
We conclude that provider-facing interventions that reduce opioid prescribing in primary care have no observed association with patient outcomes in reported pain and satisfaction with care.
Footnotes
Author Contributions
Dr Kraemer had full access to all study data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: All authors.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Hardy, Howey, Cochran.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: Wasan, Kraemer.
Obtained funding: Kraemer, Gordon, Cochran, Wasan.
Administrative, technical, or material support: Cochran, Kraemer, Wright, Wasan.
Supervision: Kraemer, Wright, Cochran, Gordon, Wasan.
Key Collaborator Contributions
The authors would like to acknowledge the instrumental contributions of Andrew Althouse, PhD from the Center for Research on Health Care, University of Pittsburgh School of Medicine, Pittsburgh, PA, and Melissa Kern, MPH from the Center for Pharmacy Innovation and Outcomes, Geisinger Health, Danville, PA to this report. Dr Althouse contributed to maintaining data integrity and all statistical analyses. Kern supervised data collection and protocol implementation. These individuals were compensated for their contributions through the same PCORI funding supporting this trial.
Additional Contributions
The authors thank the support and collaboration of PCORnet and the PaTH Network. They express gratitude to the patients, patient advocates, clinicians, representatives of national organizations and health systems, and public and private partners on the stakeholder advisory board for their participation in the trial from conception to completion. These individuals were not compensated for their contributions.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Gordon reported grants from the National Institutes of Health, Veterans Affairs, and US Department of Health and Health Services during the conduct of the study as well as personal fees from UpToDate and board service with the American Society of Addiction Medicine, Association for Multidisciplinary Education and Research in Substance use and Addiction, and International Society of Addiction Journal Editors outside the submitted work. Dr. Wright reported grants from the Patient-Centered Outcomes Research Institute (PCORI) during the conduct of the study and grants from Pfizer and grants from the National Institute on Drug Abuse outside the submitted work. Drs. Cochran and Hardy reported grants from PCORI during the conduct of the study. Dr. Wasan reported consulting fees from Greenwich Biosciences and grants from Parallel outside the submitted work. No other disclosures were reported.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This trial was entirely supported by award UOP-1609-36881 from PCORI.
Role of the Funder/Sponsor
PCORI did not play a role in the design or conduct of this study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Data Availability Statement
Deidentified data are available per PCORI policy. A URL for data access is not yet available. Requests may be made to Dr. Kevin Kraemer at