
Abstract
Introduction
Postpartum depression (PPD) is a nonpsychotic depressive state that begins after childbirth. In Ethiopia, there was limited evidence about the prevalence and factors associated with PPD in terms of residence.
Objective
To assess disparities in PPD among urban and rural mothers in the Shashogo district, Hadiya zone southern Ethiopia 2022.
Methods
Community-based comparative cross-sectional study design was employed from May 3 to July 3, 2022. A sample size of 556 (185 from urban and 371 from rural) was calculated using a double population proportion approach and mothers in the postpartum period were randomly selected from both urban and rural settings using stratification followed by single stage and the systematic random sampling method. Data were gathered by trained data collectors using an interviewer-administered questionnaire and analyzed using SPSS Version 25. Statistical significance was declared at a P value of < .05
Results
One hundred forty-four (26.6%) mothers in the postpartum period with 95%CI [23-30] were depressed, of which 37 (19.8%) with 95% CI [14-26] in urban and 107 (30%) with 95% CI [25-35] found in a rural setting. Unplanned pregnancy, low maternal social support, assisted delivery, no antenatal care (ANC) follow-up, no postnatal care (PNC) follow-up, and low household income were independent predictors of PPD in rural residence whereas unplanned pregnancy, low maternal social support, assisted delivery, and antenatal depression were independent predictor of PPD in urban.
Conclusion
PPD was found to be high in the study area as compared to national/global burden. Unplanned pregnancy, low maternal social support, and assisted delivery were predictors for both urban and rural. Low income, no ANC, and PNC follow-up were associated with PPD in rural settings only whereas antenatal depression is a predictor of PPD in urban settings.
Introduction
Postpartum depression (PPD) refers to a nonpsychotic depressive state that begins in the postpartum period after childbirth. 1 Globally about 10% to 15% of postpartum women are affected with PPD. 2 There was a wide disparity in the assessment of the problems worldwide because more than 90% of research was done in developed nations but, only 10% in low and middle-income nations. 3 In developing nations, the prevalence of postpartum depression has nearly doubled compared to the developed world. 4 PPD is very prevalent in Africa; however, it receives insufficient research and care. According to a systematic review and metaanalysis, the pooled prevalence of PPD in Africa in 2020 was 16.84%. 5 In South Africa's rural communities, PPD affected 50.3% of the mothers, making it a severe health concern. PPD is one of the most common mental problems in women after giving birth which has negative effects on mothers, neonates, and families. 6 Children of depressive mothers likely experience probable affection, and impaired psychomotor and cognitive growth. 7 There are 2 main kinds of PPD: postpartum or maternity “blues,” which is a mild mood problem of short duration, and postpartum major depression, a severe and potentially life-threatening illness. 4 Rather than a single cause, PPD symptoms are most likely the result of a combination of physiological, physical, and emotional factors. 8 Compared to women in urban areas, women in rural communities could have fewer access to and poorer quality mental healthcare.9,10
Despite the potential negative effects of PPD, the condition is frequently misdiagnosed and untreated. 11 There is growing evidence that nonmental health professionals deliver psychosocial therapies for PPD, but there is insufficient data from rural, low-income national settings. 12 The majority of mothers who were affected with PPD were single, unemployed, and had a history of a mental disorder. 13
There have been reports of a high frequency of PPD in urban Zimbabwe, but little is known about the situation there in rural areas. 9 According to a 2018 study conducted in Kenya, 18.7% of women had PPD. 14
According to a systematic review carried out in Ethiopia in 2020, the pooled prevalence of postnatal depression was 22.9% with a 95% confidence interval (95% CI) of 17.75% and 28.03% 15 and unplanned pregnancies, spousal violence, and a lack of social support were all characteristics that were associated with PPD.
High PPD case flow to the district's primary hospital and informal reports from community members draw our interest to research this health problem. As per our knowledge, this is the first study of its kind in the study area and PPD is highly reported among rural women as compared to urban women based on health facilities medical records. PPD had received little attention in the study area. Even though there were differences in the accessibility and availability of healthcare facilities between rural and urban areas, which may have a direct or indirect impact on how often women use these services, there were limited studies conducted in urban and rural areas to provide evidence on disparity in PPD. So that the primary aim of this study was assessing disparities in PPD among urban and rural mothers in Shashogo District Hadiya Zone; SNNPR, Ethiopia. The early detection of PPD and its associated factors in terms of residence aids in the development of an effective strategy for reducing maternal mortality and morbidity. The research contributes to the body of knowledge on maternal mental health and aims to raise awareness among healthcare professionals. PPD research would provide critical information to program managers and policymakers in their efforts to address such health issues. It could also be used as a foundational piece of knowledge for the academic community.
Methodology
Study Area and Period
From May 3, 2022, to July 3, 2022, the research was carried out in the Hadiya zone Shashogo district. Hadiya zone is one of the zones in Ethiopia's Southern Nations Nationalities and Peoples regions. In 2021/2022, the estimated population size of the zone was 148 504, with 72 767 males and 75 735 females (Hadiya Zone Health Department 2021). The estimated number of postpartum women was 5138, with 98% antenatal care (ANC) coverage in the specific study district. There were 34 601 women in reproductive age groups, 4737 children under one year old, and 5138 estimated live births.
Study Design
Community-based comparative cross-sectional study design was conducted among rural and urban mothers in the postpartum period in the Shashogo district in 2022.
Populations
Target Population
All the postpartum mothers in Shashogo district in 2022.
Study Populations
All postpartum mothers in the study period in selected Kebeles.
Eligibility Criteria
Inclusion Criteria
All postpartum mothers in the postpartum period who lived in the area for more than 6 months.
Exclusion Criteria
Seriously sick postpartum mothers who were unable to respond.
Sample Size Determination
The sample size was calculated using the double population proportion formula with a 95% CI and a 5% margin of error by using Epi info Version 7. For objective one (prevalence of PPD among rural and urban communities of the study area), sample size was computed using a double population proportion formula. Due to the lack of prior research in a comparable setting, the prevalence of PPD (P1) was considered to be 50% in rural communities and P2 (prevalence of PPD in urban = 33.8%) from Mizan Tepi town.
16

Sample Size Calculation for Objective 2 of the Study at Shashogo District, Southern Ethiopia, 2022.

By comparing the sample size obtained for the 2 objectives of the study, the minimum required sample size to answer those objectives becomes 354. Finally, by adding a 5% nonresponse rate and 1.5 design effect, the sample size became 556.
Sampling Procedure
The Shashogo district was stratified into urban and rural kebeles. From each stratum, proportionate sample sizes were chosen. Single-stage sampling techniques were used to select 9 kebeles from 32 rural kebeles and 2 kebeles from 4 urban kebeles. In the chosen area, there were 1200 postpartum mothers during the study period. Finally, every second value was used in a systematic random sampling technique to select study participants for study from selected kebeles in both strata (Figure 1).

Schematic presentation of proportional allocation.
Study Variables
Dependent variable; PPD: according to Edinburgh Postnatal Depression Scale (EPDS) questions after adding up all the scores, those women who scored ≥ 10 were concluded to have PPD. 18
Independent Variables
Sociodemographic variables: age, educational status, marital status, family size, occupation, husband education, husband occupation, and household (HH) income.
Social support variables: husband support, friend support, and family support.
Substance use variables: cigarette smoking, alcohol drinking, and chat chewing.
Obstetrics variables: obstetric complication, mode of delivery, birth outcome, undesired fetal sex, antenatal care, postnatal care, parity, unwanted pregnancy/birth, difficulty of breastfeeding, illness of infant, infant loss after birth, antenatal depression, gestational age, and abortion.
Psychiatric variables: women who had predefined mental illness.
Operational and Term Definitions
- PPD: according to EPDS questions after adding up all the scores, those women who scored ≥ 10 were concluded to have PPD.
- Postpartum period: it is a period beginning immediately after the birth of a child (the delivery of the placenta) and extending for 6 6-week postpartum period.
- Social support: the perception that one is cared for or has assistance available from other people which is measured using a 6-item questionnaire rated on a 5-point Likert scale (from 1 = never to 5 = always) developed by Webster and colleagues on family support, friendship network, help from spouse, conflict with a spouse, feeling controlled by a spouse, and feeling unloved by a spouse. 19 After reverse coding the negative questions, the computed possible score for this scale is 30 and the value is categorized into 3. Scores ranging from 24 to 30, are considered as high, scores ranging from 18 to 23 are considered as medium, and a score below 18 is considered low. 20
- Urban/rural: urban areas are densely populated, characterized by high-rise buildings, busy roads, and industrialization. On the other hand, rural areas are sparsely populated, characterized by natural landscapes, agriculture, and low population density. 21
Data Collection Tool
A structured interviewer-administered pretested questionnaire was used to collect information from study participants. The instrument was adapted from previously published scholarly articles4,5,11–13,16,22–24 and was designed in the English language and then translated into Amharic and to the local Hadiyisa language. Ten-question EPDS is a valuable and efficient tool for identifying PPD were employed. 25 Maternal social support was measured using 6 questions with 5-Likert scale responses whereas the wealth index was calculated using HH asset ownership data, and the resulting index was ranked into 5 quintiles. 26
Data Collection Procedure
Data were gathered using a pretested questionnaire administered by an interviewer. Face-to-face interviews were used to collect information from mothers in the postpartum period in the district's rural and urban communities.
Data collectors were 4 diploma nurses who worked in the Maternal and Child Health Department at various health centers, and they received 2 days of training. Data were gathered by visiting women in their homes during their postpartum period. Local extension workers and the Health Development Army (HDA) aided the data collectors in their door-to-door visits to postpartum women under the supervision of one supervisor.
Data Quality Assurance
We used an adapted questionnaire that was pretested for accuracy, response language clarity, appropriateness, estimating the time required, and cultural sensitivity. A necessary change was made. For 2 days, data collectors and supervisors were trained to ensure data quality. Supervisors checked completed questionnaires on a daily basis for consistency and completeness.
Data Analysis
Data was coded, entered, and cleaned using Epi data Version 4.6 before being exported to SPSS Version 25 for analysis. To characterize the study population, descriptive statistics such as percentage and frequency were used. The Hosmer-Lemishow test was used to assess model fitness whereas Cronbach's alpha was used to assess the tool's internal consistency for EPDS and Maternity Social Support Scale. Initially, residence was tested for association as an independent predictor of PPD; accordingly, being in a rural setting was associated significantly with PPD with a P value of .01; finally, factors associated with PPD were examined separately for rural and urban populations. Each independent variable was associated with PPD using a bivariable logistic regression model. Variables with P values < .25 in the bivariable model were entered into multivariable logistic regression to account for the potential effect of confounders. Finally, multivariable logistic regression was used to identify the independent predictors of PPD in urban and rural women. The odds ratio at 95% CI and P value < .05 were used to declare the associations between dependent and independent variables and their statistical significance.
Results
In this study, 542 mothers in the postpartum period were interviewed successfully with a response rate of 97.5%, of which 187 (34.5%) were from urban and 355 (65.5%) were from rural communities. Those who were absent for at least 2 home visits during the data collection period and were unwilling to provide information were the reason for no response.
Sociodemographic Characteristics
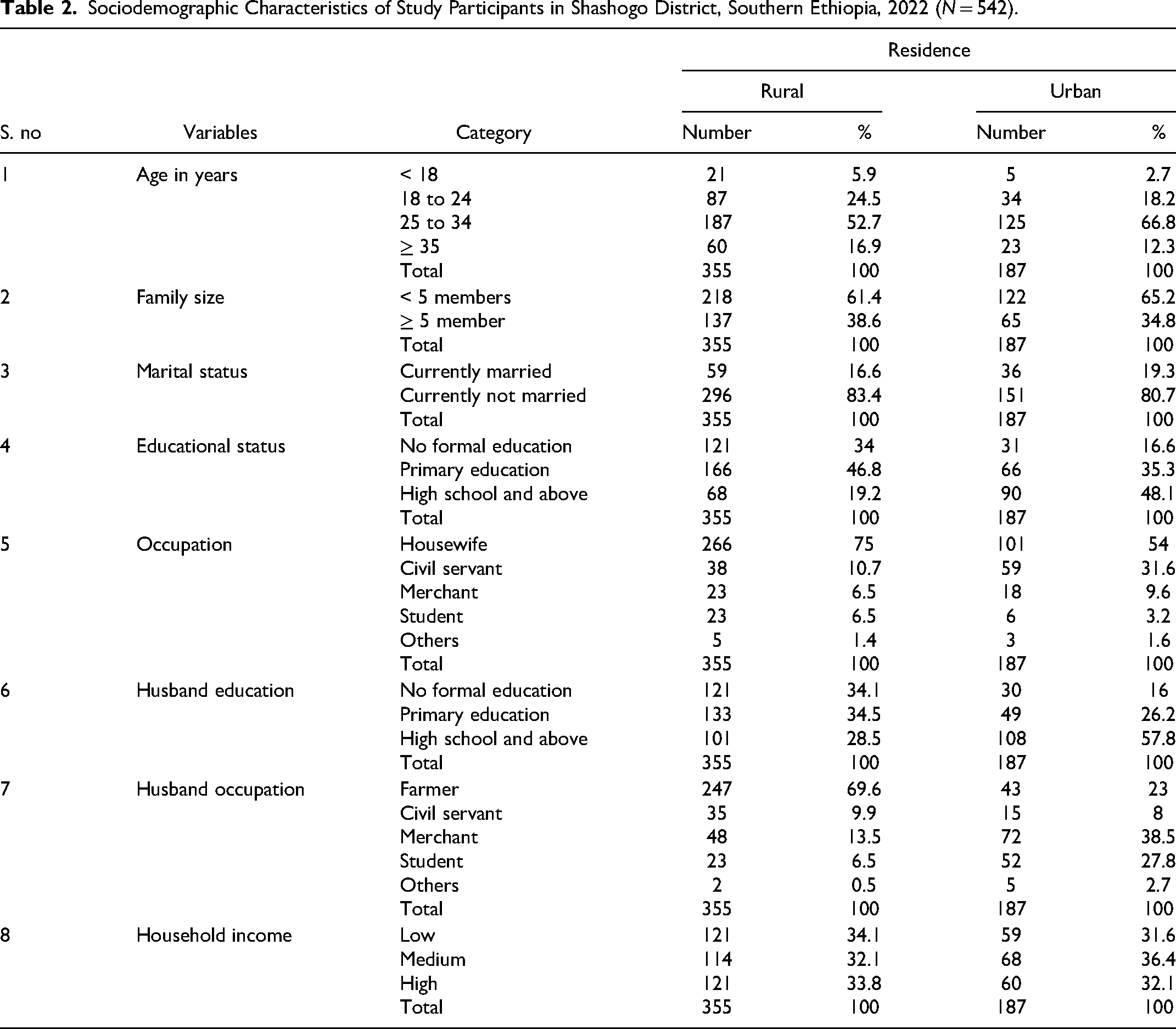
The respondents’ mean age was 28.8 (SD 5.3) in the urban and 28.7 (SD 6.7) in the rural setting. The majority of respondent's age group was 25 to 34 years, with 52.7% living in rural areas and 57.6% in urban areas. In terms of marital status; among participants, more than three-quarters [296 (83.4%)] were currently married and the rest were not married in rural settings whereas 151 (80.7%) were married and the rest were not married in urban settings. In both rural and urban areas, the majority of respondents are Hadiya, with 249 (70%) and 116 (62%), respectively. In terms of educational attainment, the majority of rural (166 (47%) and urban 66 (35%) residents attended primary school. More than half of the respondents 218 (61.4%) in rural and 122 (65%) in urban) had fewer than 5 family members. Almost one-third of respondents; 121 (34.1%) in rural HHs and 59 (31.6%) in urban HHs had a low HH income (Table 2).
Sociodemographic Characteristics of Study Participants in Shashogo District, Southern Ethiopia, 2022 (N = 542).
Obstetric Related Factors
The majority of study participants, 239 (67.3%) in rural and 59 (31.6%) in urban, were multipara. Among all respondents, nearly 1 in 5 [74 (20.8%)] rural women and nearly 1 in 4 [45 (24.1%)] urban women had abortions at some point in their lives. Furthermore, 119 (33.5%) rural women and 50 (26.7%) urban women had unplanned pregnancy. In terms of antenatal care, 211 (59.4%) of rural women and 141 (75.4%) of urban women had antenatal care at least once during their current pregnancy. Furthermore, 159 (44.8%) rural women and 41 (21.9%) urban women gave birth at home, with the remainder giving birth at a health facility. The majority of postpartum women, 290 (81.7%) in rural and 143 (76.5%) in urban, had SVD and others had assisted delivery. Among all births, 147 (41.4%) were male in rural areas and 86 (46%) were male in urban areas, with the remainder being female. The sex of the newborn was undesired by 183 (51.5%) in rural areas and 63 (33.7%) in urban areas. The majority of the women, 251 (70.7%) from rural areas and 137 (73.3%) from urban areas, had no postnatal care. Furthermore, 99 (27% of rural women) and 46 (24.6%) of urban women in the postpartum period had a history of antenatal depression. About 88.8% of rural respondents and 60.1% of urban respondents experienced complications during pregnancy and/or childbirth (Table 3).
Obstetric Characteristics of the Women in Postpartum Period in Shashogo District, Southern Ethiopia in 2022 (N = 542).

Abbreviations: ANC, antenatal care; SVD, small vessel disease.
Psychiatric Factors
More than three-quarters of rural 285 (80.3%) and nearly three-quarters of urban respondents 137 (73.3%) had no family history of mental illness, while 84 (23.7%) of rural and 53 (28.3%) of urban respondents had a history of previous depression (Table 4).
Personal and Family History of Mental Illness of Respondents in Shashogo District, Southern Ethiopia, 2022.

Substances use
More than one-fifth of the study participants 80 (22.5%) in rural and 52 (27.8%) in urban had a history of chat chewing, and 106 (29.9%) in rural and 49 (26.2%) in urban had a history of alcohol consumption during their current pregnancy. On the other hand, 61 (17.2%) of rural women and 36 (19.3%) of urban women have a history of chat chewing during their current pregnancy (Table 5).
Substance Use of Respondents in Shashogo District, Southern Ethiopia in 2022.

Maternal Social Support
Among the participants, 124 (34.9%), 106 (29.9%), and 125 (35.2%) had low, medium, and high social support in a rural setting, respectively, whereas 87 (46.5%), 33 (17.6%), and 67 (35.8%) of study participants had low, medium, and high social support in an urban setting, respectively (Table 6).
Maternal Social Support of the Postpartum Women in Shashogo District, Southern Ethiopia in 2022.

Prevalence of PPD
The prevalence of PPD was determined using the Edinburg Postnatal Depression Measuring Scale, which consists of 10 questions. Postpartum women were classified as depressed if their total sum score was > 10, but not as depressed if it was < 10. As a result, 144 (26.6%) of the total study participants were depressed, with a 95% CI of [23%-30%] of which 107 (30%) were in the rural community with a 95% CI of [25%-35%] and 37 (19.8%) were in the urban community with a 95% CI of [14%-26%] (Figure 2).

Prevalence of postpartum depression among urban and rural mothers in postpartum period in Shashogo district, Southern Ethiopia in 2022.
Factors Associated With PPD
The multivariable analysis revealed that of the 22 variables in the model, unplanned pregnancy, low maternal social support, and assisted delivery were associated with a higher risk of PPD in both urban and rural areas. However, no ANC follow-up, no PNC follow-up, and low HH income were associated with a higher risk of PPD in rural women, whereas antenatal depression was associated with PPD in urban women (Table 7).
Factors Associated With PPD Among Urban and Rural Postpartum Women in Shashogo District, Southern Ethiopia; 2022.
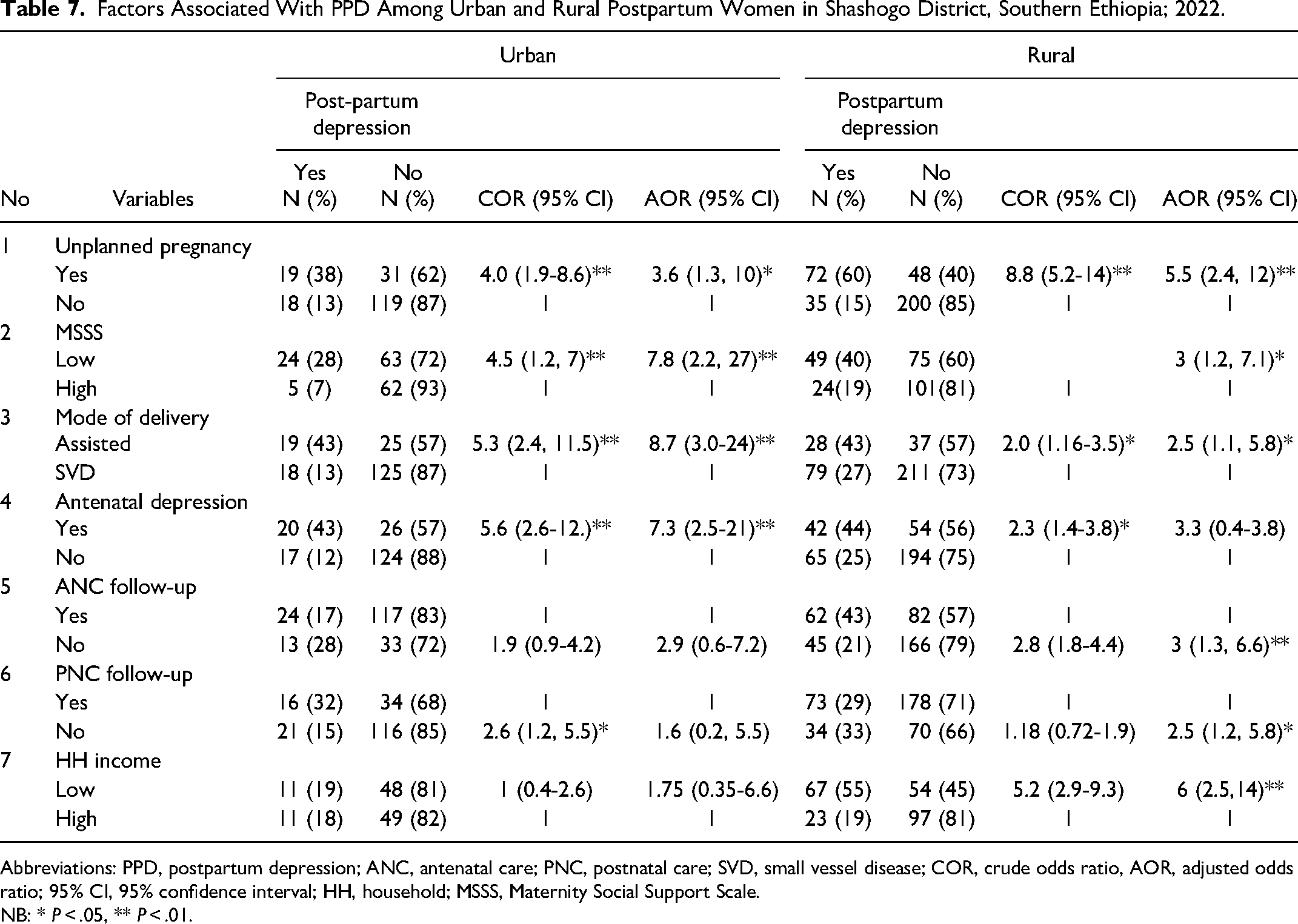
Abbreviations: PPD, postpartum depression; ANC, antenatal care; PNC, postnatal care; SVD, small vessel disease; COR, crude odds ratio, AOR, adjusted odds ratio; 95% CI, 95% confidence interval; HH, household; MSSS, Maternity Social Support Scale.
NB: * P < .05, ** P < .01.
The study revealed that participants who had unplanned pregnancy had 5.5 times higher odds of PPD as compared to those with planned pregnancy among rural women with 95% CI [2.4-12] and the odds of PPD among women with unplanned pregnancy was 3.6 times higher with 95% CI [1.3-10] in an urban setting. Mothers having low maternal social support had 3 times higher odds of developing PPD as compared with women with high social support with 95% CI [1.2-7.1] in rural, whereas 7.8 times higher odds with 95% CI [2.2-27] in urban settings. Mothers having assisted delivery had 2.5 times higher odds of experiencing PPD as compared with SVD with 95% CI [1.1-5.8] in rural and had odds of 8.7 times higher to develop PPD with 95% CI [3.0-24] in urban, respectively.
Postpartum women without ANC follow-up in rural areas, on the other hand, had 3 times higher odds of experiencing PPD compared to those with ANC follow-up history 95% CI [1.3-6.6]. Besides, in rural areas, mothers who had no PNC follow-up had 2.5 times higher odds of PPD compared to those who had PNC follow-up, with 95% CI [1.2-5.8]. and low HH income was associated with 6 times higher odds of PPD as compared with those who have higher HH income with 95% CI [2.5-14] in rural settings.
In urban areas, having a history of antenatal depression increased the risk of PPD by 7.3 times when compared to mothers who had no history of antenatal depression, with a 95% CI of [2.5-21] (Table 7).
Discussion
The current study sought to compare PPD rates among urban and rural mothers in Hadiya zone Shashogo district, southern Ethiopia. The prevalence of PPD in urban areas is significantly lower than in rural areas, and living in rural areas is significantly associated with PPD. Overall prevalence is consistent with a finding from a systematic review and metaanalysis study conducted in low and middle-income countries, which shows a prevalence of PPD of 25.8%. 12 This might be due to the socioeconomic resemblance of the countries. The finding in urban setting is in line with the systematic review conducted in Ethiopia in 2020 15 and the study conducted in Debre-Birhan in 2018. 4 The PPD prevalence in rural communities is comparable with the findings from the study result in rural districts in Zimbabwe in 2018. 9 Contrastingly, the finding on PPD prevalence from the current study is lower than the study finding on the rural community of Western Cape, South Africa. 13 This disparity may be attributed to time variability, sociocultural disparities, and study participant variation, as well as differences in sampling methods used, as we used a 6-week postpartum period while comparable studies used a 12-month period.
Factors Commonly Associated with PPD Both in Urban and Rural
Unplanned pregnancy and postpartum depression: There is a significant association between unplanned pregnancy and PPD both in urban and rural. The finding in the urban setting from the current study is comparable with the findings from a study conducted in Mizan Aman town in 2018, in which unplanned pregnancy had a significant association with PPD with 95% CI [1.7, 16.6]. 27 Furthermore this study's finding is comparable with the finding of a systematic review conducted in Ethiopia in 2020, 28 finding from a study in Ankesha district Awi zone North West Ethiopian 2019 20 and in Bench Maji zone, Southwest Ethiopia in 2017. 27 This could be because of inadequate preparation for pregnancy and childbirth leaves mothers unable to cope with the challenges and feeling anxious. It could also be because unplanned pregnancy has a greater impact on maternal health by negatively affecting mothers’ psychology and can also bring economic burden and social judgment, which can lead to postpartum depression. This consistency could also be attributed to socioeconomic similarities. In contrast, the studies conducted in Debre-Birhan Ethiopia, the United States, and Nepal found no significant association between unplanned pregnancy and PPD when compared to planned pregnancy.4,18,29 This could be due to variation in time and sociocultural characteristics and variability in study participants and time.
Findings from the current study revealed that there is a statistically significant association between PPD and low maternal social support. This finding shows that postpartum mothers with low social support in urban develop PPD with odds of almost 8 times higher and odds of experiencing PPD nearly 3 times higher in rural settings as compared with those who have high social support. This is comparable with the findings from the study conducted in Mizan Aman town in 2018, 27 with 95% CI [1.1-10.3], in Awi zone, with 95% CI [1.55-11.43], 20 in Debrebirihan town in 2018 with 95% CI [1.01-26.18], East Wollega zone in 2019, 95% CI [2.25-19.29] 30 and with the systemic review conducted in Ethiopia in 2020 22 which all reveals that low social support had statistically significant impact on increasing odds of PPD. This could be due to a lack of important support from close family members, husbands, and other intimate friends which could disrupt women's emotions and contribute to PPD.
The current study also revealed that there is a statistically significant association between PPD and assisted delivery as compared to spontaneous vaginal delivery in both urban and rural settings. The finding from this study contrasts with the findings from the studies conducted in Addis Ababa in 2016 with 95% CI [0.4-1.8], 19 in Mizan Aman town in 2016 with 95% CI [0.34-1.25] 16 and in East Wollega in 2019 with 95% CI [0.46-7.48] 30 which revealed that PPD and assisted delivery were not significantly associated. This may be due to the difference between study setting, time variability, and sociocultural variation.
Factor Associated With PPD in Urban
According to the current study's findings, there is a statistically significant association between antenatal depression and PPD with 95% CI [2.5-21]. These show that postpartum women in urban with antenatal depression develop PPD with odds of nearly 7 times higher as compared with those who had no antenatal depression. This finding is in line with the study conducted in Gondar town in 2020 11 on the causal mechanism of PPD, which reveals that PPD was independently predicted by having antenatal depression. 11 Besides, the study conducted in Addis Ababa in 2015 on PPD and associated factors also reveals the same findings. 8 This might be due to the sociodemographic resemblance of the population in the urban and this shows that antenatal depression is ground for PPD. Contrary to this, the study results in the Bench-Maji zone, southwest Ethiopia in 2017 show that there is no statistically significant association between PPD and antenatal depression. 16 This might be due to variations in the time of investigation, and sociocultural variability.
Factors Associated With PPD in Rural
The current study exposed that there is a statistically significant association between PPD and no ANC follow-up during pregnancy with 95% CI [1.3-6.6]. This finding is in line with the findings from the study conducted in Gondar town Northwest Ethiopia in 2020, 17 which the participant who did not follow ANC had odds of 4 times more likely to be depressed as compared with those who had ANC follow with 95% CI [1.81-9.05]. This could be because ANC service utilization provides health promotion, disease prevention, and treatment, specifically increased birth and complication readiness, which may reduce mental strain and maintain psychological stability during pregnancy. As a result, PPD may increase in these groups that do not have ANC follow-up.
Furthermore, there is a statistically significant association between developing PPD and not having a postnatal follow-up with 95% CI [1.2-5.8]. This finding is comparable with the finding from a study conducted in 2020 in Northwest Ethiopia 17 with a 95% CI of [1.11-3.0], and also with the study in Gondar in which PPD was independently predicted by having low postnatal care services 95% CI [1.11-3]. 11 This might be due to lack of important message and psychological support from professionals during this period.
Besides, there is a statistically significant association between low HH income and PPD as compared with high HH income, with 95% CI [2.5-14], which reveals that the odds of PPD among the women who had low HH income increased with 6 folds as compared with those who had high income. This is comparable with the findings from the systematic review conducted in Ethiopia in 2020, 22 that reveals low income was significantly associated with the increased odds of PPD [95% CI]. On the other hand, this finding is comparable with the finding from the study conducted in Addis Ababa which shows that respondents who had low HH incomes developed depression with odds 2 times during the postpartum period as compared to those respondents who had high HH incomes 95% CI [1.19-4.2]. In contrast to this, the study conducted in rural communities in South Africa in 2015 shows that there is no statistically significant association between PPD and low income of the HH. 13 This difference might be due to time differences and differences between the socioeconomic characteristics of respondents and sociocultural variability among the study participants that low HH income causes PPD by making the living style more stressful and thus, in turn, causes PPD.
Limitations and Strengths of the Study
Strength of the Study
The study was conducted through home-to-home visits, which assisted in reaching out to mothers who were unable to visit healthcare facilities during the postpartum period, increasing representativeness and generalizability. The study was conducted in both rural and urban settings, identifying the prevalence and factors associated with PPD separately and displaying the exact figure for each location.
Limitation of the Study
Only history was used to quantify antenatal depression and previous history of depression. It is better if strong design, such as prospective cohort designs to justify such an association. Social desirability bias might occur when mothers provide information. The severity level of PPD is not shown in the study.
Conclusions and Recommendations
PPD was more common among postpartum women in the study area than it was globally, especially in rural mothers. In addition, assisted delivery, unplanned pregnancies, and a lack of maternal social support increase the risk of PPD in mothers in both urban and rural areas. In contrast to rural communities, where low HH income and a lack of antenatal and postnatal follow-up are independent predictors of PPD, antenatal depression is an independent predictor of PPD in mothers who live in urban areas. Therefore, this issue requires urgent attention from health professionals and Maternal and Child Health Department heads, especially in terms of early detection, in order to lower morbidity in this group of women.
In order to explore concerns such as previous depression history and antenatal depression of women with PPD, further research with prospective design and longitudinal follow-up should be undertaken. It is strongly advised to routinely screen mothers during the postpartum period and to integrate maternal and mental health care. Together with other health professionals, health extension workers must focus on information communication education and behavioral change communications on PPD. Because of this, Ethiopian health policymakers and medical professionals ought to place a greater emphasis on mothers who have a history of unintended pregnancies, antenatal depression, and inadequate social support.
Supplemental Material
sj-docx-1-hme-10.1177_23333928231217843 - Supplemental material for Disparities in Postpartum Depression Among Urban and Rural Mothers in Hadiya Zone Shashogo District Southern Ethiopia Community-Based Comparative Cross-Sectional Study
Supplemental material, sj-docx-1-hme-10.1177_23333928231217843 for Disparities in Postpartum Depression Among Urban and Rural Mothers in Hadiya Zone Shashogo District Southern Ethiopia Community-Based Comparative Cross-Sectional Study by Kassahun Mekuria, Tilahun Beyene, Bereket Aberham Lajore, Tsegaye Melkamu and Tekle Ejajo in Health Services Research and Managerial Epidemiology
Footnotes
Abbreviations and Acronyms
Acknowledgments
First and foremost, gratitude goes to my almighty God who helped me throughout all thesis work. Secondly, I would like to express my sincere gratitude to the School of Public Health, College of Medicine and Health Science, Wachemo University for giving me this golden opportunity to write my thesis. Finally, I would to acknowledge the Shashogo district health office, all my data collectors, and study participants for providing the necessary information.
Authors’ Contributions
Kassahun Mekuriya conceived the idea and wrote the proposal, participated in data management, analyzed the data, and drafted the paper. Tilahun Beyene, Tekle Ejajo, and Bereket Aberham Lajore revised and approved the proposal, revised the analysis, and the subsequent draft of the paper. Kassahun Mekuriya, Bereket Aberham Lajore, and Tsegaye Melkamu conducted and revised the analysis, presentation, interpretation, and subsequent draft of the paper. All authors read and approved the final manuscript. I confirm that all authors meet the ICMJE criteria.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
Ethical approval was obtained from the research and ethical committee of Wachemo University, written letter was obtained from the Shashogo district health office to select kebeles. Each study participant was asked to give verbal consent after explaining the nature, purpose, and procedure of the study. The anonymity and confidentiality of the respondents were strictly maintained. The participant was assured that their participation was without any enforcement, and they had the right to withdraw or refuse to give information at any time in the study without any penalty.
Funding
The author(s) received no financial support for the research, and authorship of this article.
Data Availability Statement
Data collected and utilized for this study is available on reasonable request through the corresponding author Bereket Aberham Lajore and his contact detail is bereketema41@gmail.com.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.