
Abstract
Background of the study
The protection against Coronavirus variants 2019 by pre-existing antibodies due to the current vaccination or natural infection is a global concern. In Ethiopia, case reports show that a significant number of health professionals are reported to get re-infected after vaccination. There are also more studies that revealed the symptomatic SARS-COV-2 re-infection, in particular, among healthcare providers actively engaged in Addis Ababa public health facilities.
Objective
This study has aimed at assessing the magnitude of post-vaccine reinfection of SARS-COV-2 and associated factors among health care providers in Addis Ababa public hospitals, Addis Ababa, 2022 G.C.
Methods
A facility-based cross-sectional study was conducted from July 11 to July 30, 2022. A total of 422 health professionals were included. A simple random sampling method was employed to select 40% of the total hospitals. Then the total sample size was equally allocated to each selected hospital, and then each individual was selected purposefully. The data was collected using a structured, self-administered questionnaire. The analysis was done using SPSS version 26.0, and for data entry, EPi Info version 7.1 was used. Both bivariable and multivariable logistic regression analyses were used to determine the p-value.
Results
Overall, 418 healthcare providers were enrolled in this study, making the response rate 99.05%. The magnitude of SARS-COV-2 reinfection was 60 (14.4%) (95% CI 10.8-17.9). Healthcare professionals who took infection prevention (IP) training on COVID-19 (AOR = 7.177: CI = 4.761-9.698) were associated with SARS-COV-2 reinfection; those with a history of chronic respiratory diseases (AOR = 3.029: CI = 2.406-9.133) were associated with SARS-COV-2 reinfection; health professionals who took the third dose of SARS-COV-2 vaccine (AOR = 1.75: CI = 1.14-2.68) and being a midwife were statistically significant.
Conclusion and Recommendation
This study showed the prevalence of SARS-COV-2 reinfection among vaccinated healthcare providers with a pre-vaccination infection history was high; IP training on COVID-19 was needed; educational status, profession, type of vaccine taken in the first dose, chronic respiratory diseases, and number of vaccinations were significantly associated with SARS-COV-2 reinfection after vaccination. Giving IP training, encouraging taking the vaccine as protocol, and using proper personal protective equipment are recommended.
Keywords
Introduction
Several cases of COVID-19 reinfections have been reported worldwide. Coronavirus disease is defined as an infectious disease caused by a novel coronavirus now called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 1 The first human cases of COVID-19, the disease caused by the novel coronavirus causing COVID-19, subsequently named SARS-CoV-2, were first reported by officials in Wuhan City, China, in December 2019. SARS-CoV-2 was identified in early January, and its genetic sequence was shared publicly on January 11 and 12. 2
The full genetic sequence of SARS-CoV-2 from the early human cases and the sequences of many other viruses isolated from human cases from China and all over the world since then show that SARS-CoV-2 has an ecological origin in bat populations. All available evidence to date suggests that the virus has a natural animal origin and is not a manipulated or constructed virus. Many researchers have been able to look at the genomic features of SARS-CoV-2 and have found that evidence does not support the idea that SARS-CoV-2 is a laboratory construct. 3 Globally, there are 477,312,339 coronavirus cases, of which 6,130,808 deaths and 412,392,494 cases were recovered. 4 There are also 109,555 confirmed COVID-19 cases in Asia, 8658 in Africa, 332,866 in North America, 20,269 in South America, 568,894 in Europe, 5051 in Australia, and 1,045,403 in the whole world. 1
Danish epidemiologists were excited in February when they first saw how well the Pfizer-BioNTech vaccine was working in healthcare workers and residents of long-term care facilities, who were the first to receive it in Denmark. A clinical trial1 in more than 40,000 people had already found the vaccine to be 95% effective in protecting recipients from symptomatic COVID-19. But some scientists were among the first to test its effectiveness outside clinical trials, which can exclude some unhealthy individuals or those taking medicines that suppress immune responses. 5
For COVID-19, the ultimate goal is global herd immunity, with natural infection and vaccination being the two main pathways to herd immunity.4,6 Preliminary data reveal exceptionally encouraging vaccine protection results after 6 months of mass vaccination efforts against SARS-CoV-2. While some countries have vaccinated more than half of their populations, many others are lagging. 7
Individuals who contracted the infection again ranged in age from 24 to 89. The typical time between the first and second infections was 76 days (range 19-142). Immunosuppression was present in just one patient (1/17, 5.8%) who relapsed. During chemotherapy for a hematological malignancy, this patient, a woman in her 80s, experienced modest symptoms with her first infection but acquired serious symptoms, which led to her death with her second infection. 8
Reducing reinfection is crucial given the high global rate of infection, particularly with new variations, and the slow pace of immunization. Examining reinfection, particularly the persistence of protection following natural infection, or natural immunity, will help us better understand the prospects for herd immunity, which is predicated on the idea that natural infection develops sufficient protective immunity.7,9 Even with antibodies, reinfection with different human coronaviruses happens frequently. The most recent case studies show that COVID-19 reinfection is conceivable and that a second infection could have severe consequences. The major goal of this study was to assess the prevalence of COVID-19 symptomatic reinfection and associated factors among vaccinated healthcare providers in Addis Ababa public hospitals.
Methods and Materials
Study Area
The research was conducted in Addis Ababa's public hospitals. The city has a population density of 5535.8 inhabitants per square kilometer and occupies an estimated area of 174.4 square kilometers. 10 There are 11 sub-cities and 116 woredas in the region. Eight hospitals are owned by the Addis Ababa Health Bureau, 7 by the Federal Ministry of Health, 1 by Addis Ababa University, 3 by non-governmental organizations, 3 by the military and police forces, and 34 by private owners. There are about 18,700 health professionals in Addis Ababa, and there are about 700 private clinics, with 75 of them being higher clinics, and 116 public health centres. 11
Study Design and Period
Institutional-based cross-sectional study was conducted from July 11 to July 30, 2022.
Source Populations
All health care professionals who are vaccinated at least once for SARS-COV-2 and had a history of infection before vaccination and work in Addis Ababa's public hospitals
Study Population
A healthcare professional who has been vaccinated at least once for SARS-COV-2 and had a history of infection before vaccination will work in randomly selected public hospitals in Addis Ababa in 2022.
Inclusion and Exclusion Criteria
Inclusion Criteria
Healthcare professionals who were vaccinated at least once for COVID-19 and had a history of infection before vaccination and worked in randomly selected public hospitals in Addis Ababa during the data collection period.
Exclusion Criteria
Those healthcare professionals who were on different leaves during the data collection period were excluded.
Sample Size and Sampling Technique
Sample Size
To get the maximum sample size, the previous proportion was considered to be 50%. Therefore, the required sample size of the study was determined by the single population proportion formula as follows:

After adding10%, non-response rate total sample size was 422.
Sampling Technique
Since there are about 15 public hospitals in Addis Ababa, a simple random sampling method was employed to select 40% of the total hospitals (Ghandi Memorial Hospital, Ras desta, TBGH, Zewditu Memorial Hospital, Minilik II specialized hospital, and Abebech Gobena MCH hospital). Then the total sample size was equally allocated to each selected hospital (n = 70, and for Minilik II specialized hospital and Abebech Gobena MCH hospital, n = 7) and each individual was selected purposefully. The participants were selected by asking two questions: the first was, “Have you been infected by SARS-COV-2 and diagnosed by Health care professionals either clinically or by PCR or antigen testing?” and then those who said “yes” were asked, “Have you ever been vaccinated for SARS-COV-2?” Those who answered “yes” in both questions were selected to participate in this study.
Study Variables
Dependent Variables
post-vaccine SARS-COV-2 infections with pre-vaccination infection history.
Independent Variables
Socio demographics like age, sex, weight, BMI, work experience in years, professional category, income, working area/department.
Vaccine related such as time interval between doses, types of vaccine, dose of vaccine, previously exposed to COVID.
Clinico-epidemiological profile: presence of chronic diseases
Other factors: gene difference of the variance, taking infection prevention training.
Operational Definition
SARS-COV-2: is an illness caused by a novel coronavirus now called severe acute respiratory syndrome coronavirus 2.
Vaccinated: the time after health care providers take at least one dose of SARS-COV-2 vaccine.
Vaccinated healthcare provider: those healthcare providers who are vaccinated at least one dose of SARS-COV-2 vaccines. 12
Post-vaccine SARS-COV-2 reinfection with pre-vaccination infection history: Defined as positivity for SARS-COV-2 either with PCR or a rapid antigen test before taking COVID-19 vaccines and then confirmed positive after taking at least one dose of SARS-COV-2 vaccines.13,14
Vaccine: Is a product that stimulates a person's immune system to produce immunity to a specific disease, protecting the person from that disease.
Data Collection Tool
A pretested, structured interview questionnaire consisting of items with predetermined response categories was utilized to collect data. The questionnaire was modified based on the findings of the literature review.15–18 The tool has four sections: The first section consists of sociodemographic characteristics; the second section consists of SARS-COV-2 vaccine status-related questions; the third section is about the clinico-epidemiological profile of SARS-COV-2; and the fourth section is about infection prevention-related factors. The questionnaire was designed in English.
Data Collection Procedures
Five BSC (two nurses, two midwives, and one health officer) healthcare staff were involved in data collection. The data collectors were given 1-day training prior to data collection, with a supervisor checking the completeness, accuracy, and appropriateness of the data collected every day. The data collectors were then supervised on the objectives, benefits of the study, and individual rights and informed consent on the questionnaire.
Data Quality Control
A pre-test of the questionnaire was performed on 5% of healthcare staff at Yarer General Hospital. The data was obtained after each healthcare professional gave their informed consent. A code was used to preserve confidentiality, and no names of respondents were used in any of the data collection instruments. The collected data were reviewed and checked for completeness.
Data Analysis Procedure
First, the collected data were checked for incompletion and misfiling. Then the data were cleaned and stored for consistency and entered into Epinfo version 7.1, and then it was exported to statistical package for social sciences (SPSS) version 26.0 software for analysis. Descriptive statistics like frequency, proportion, mean, and standard deviation were computed to describe study variables in relation to the population. Then this result was compiled and presented using texts, tables, graphs, and pie charts. Logistic regression (bivariable and multivariable) was used to determine the effect of independent variables on the outcome variables. Variables found to have a p-value < 0.2 in the binary logistic regression were entered/exported into multivariable analysis to identify their independent effects and then strength of association was declared at p-value < 0.05. Then, the final results were presented as an adjusted odds ratio (AOR).
Results
Socio-Demographic Characteristics of Study Participants
Out of 422 study participants, 418 respondents participated in this study, making a response rate of 99.05%. About 51.7% of health professionals were female. The mean age of the respondents was 33.7 years with a standard deviation ±7.36. Most participants in this study (61.5%, 257) are under the age of 25-34. About 227 (54.3%) participants in this study were BSC in their qualification and 101 (24.2%) were nurses. And also, 171 (40.9%) participants in this study were aged 5 years or younger. Regarding the BMI of participants, about 202 (48.3%) were in the normal range (Table 1).
Socio-Demographic Characteristics of SARS-COV-2 Reinfection Among Vaccinated Health Care Providers with Pre-Vaccination Infection History in Addis Ababa Public Hospitals, Addis Ababa, 2022 (N = 418).

SARS-COV-2 Reinfection Exposure Status of the Study Participants
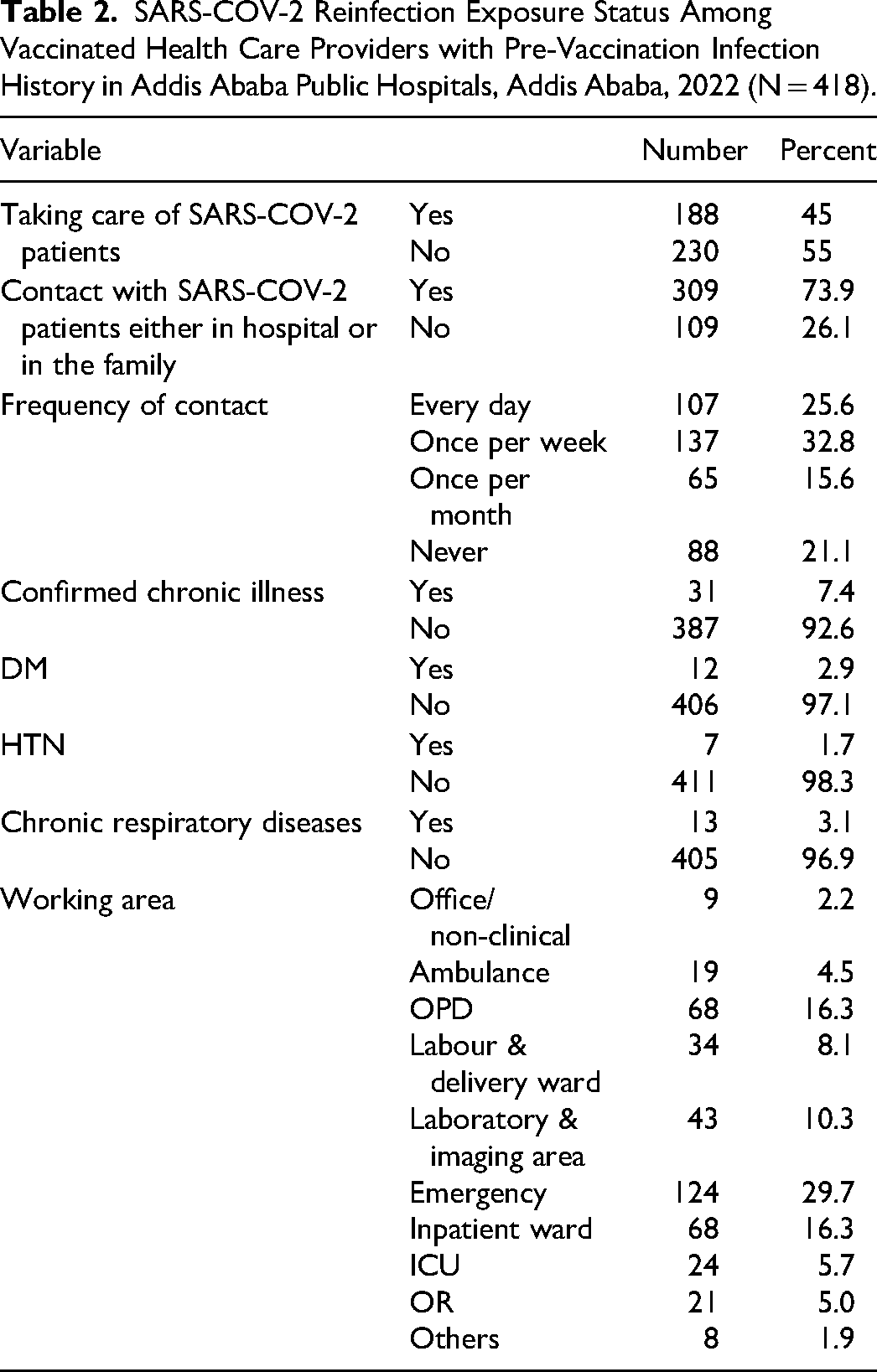
Participants in the care of SARS-COV-2 patients were about 188 (45%) healthcare providers who had contact with SARS-COV-2 patients either in the hospital or in the family. Those participants having contact with SARS-COV-2 patients either in the hospital or in the family were 309 (73.9%). About 31 (7.4%) participants have confirmed chronic illnesses like DM (12.9%), HTN (7.7%), and chronic respiratory diseases (13.1%) (Table 2).
SARS-COV-2 Reinfection Exposure Status Among Vaccinated Health Care Providers with Pre-Vaccination Infection History in Addis Ababa Public Hospitals, Addis Ababa, 2022 (N = 418).
SARS-COV-2 Vaccination Status of the Study Participants
Most participants in the study—200 (47.8%)—took AstraZeneca for their first vaccination. And also, about 321 (76.8%) participants took the second dose of the vaccines, as shown in Table 3.
SARS-COV-2 Vaccination Status of Vaccinated Health Care Providers with Pre-Vaccination Infection History in Addis Ababa Public Hospitals, Addis Ababa, 2022 (N = 418).

COVID-19 Reinfection and Infection Prevention Related Status of the Study Participants
About 60 (14.4%) (95% CI 10.8-17.9) participants were reinfected by SARS-COV-2 after vaccination with at least one dose of the vaccine. Most of them (85%) are diagnosed by rapid antigen tests. And there is no hospitalization for those who are reinfected. Regarding infection prevention, 306 (73.2%) of participants took the training (Table 4).
SARS-COV-2 Reinfection and Infection Prevention-Related Status of Vaccinated Health Care Providers with Pre-Vaccination Infection History in Addis Ababa Public Hospitals, Addis Ababa, 2022 (N = 418).

Bivariable and Multivariable Analysis of Factors Associated with SARS-COV-2 Reinfection
In this study, bivariable analysis is used to take a training on infection prevention (COR = 6.629, CI = 3.696-11.888), educational status (diploma) (COR = 3.150, CI = 1.263-7.855), profession (being a midwife) (COR = 4.917, CI = 1.175-20.581), type of vaccine taken in the first dose (taking Janssen/Johnson &Johnson) (COR = 2.346, CI = 1.221-4.508), and those healthcare professionals who have chronic respiratory diseases (COR = 5.571, CI = 1.804-17.203) were significant and exported into multivariable analysis in order to control confounders, whereas BMI, taking care or treating COVID-19 patients, and experience were not significant with the SARS-COV-2 reinfection.
In multivariable analysis, those predictors that showed statistical significance in bivariable analysis with a p-value less than 0.2 were used to run multivariable analysis. In multivariable analysis, healthcare professionals who took IP training on COVID-19 were significantly associated with professionals who did not take IP training (AOR = 7.177; CI = 4.761-9.698). The ODDs of those whose educational level diploma is about three times more exposed for SARS-COV-2 reinfection as compared to those MSC and above 3.500 (1.265-9.682), and those who are midwives were about nine times more re-infected by SARS-COV-2 as compared to other professions (9.315-1.814-17.826). The type of vaccine taken in the first dose (Johnson & Johnson) was about three times more infected by SARS-COV-2 at 3.216 (1.073-9.643). The ODDs of healthcare professionals who have chronic respiratory diseases were significantly associated with those who had no history of chronic respiratory diseases (AOR = 3.029; CI = 2.406-9.133). Regarding vaccination status, health professionals who took only the first dose of the SARS-COV-2 vaccine were significantly associated with professionals who took the third booster dose (AOR = 1.75; CI = 1.14-2.68) (Table 5).
Bivariable and Multivariable Analysis of Factors Associated with SARS-COV-2 Reinfection Among Vaccinated Health Care Providers with Pre-Vaccination Infection History in Addis Ababa Public Hospitals, Addis Ababa, 2022 (N = 418).

NB: **p < 0.05, *p < 0.02 statistically significant.
Discussion
This study focused on SARS-COV-2 reinfection among vaccinated healthcare providers in Addis Ababa Public Hospitals in 2022. In this study, 14.4% (95% CI 10.8-17.9) of participants were reinfected by SARS-COV-2 after vaccination with at least one dose of the vaccine and having a pre-vaccination infection history. Infection prevention training on COVID-19, educational status, profession, type of vaccine taken in the first dose, chronic respiratory diseases, and number of vaccinations were significantly associated with SARS-COV-2 reinfection after vaccination. These factors are almost related to the study done in mid-western 15 and in health care workers in the United Kingdom. 19
The results of this study are more significant than those of studies conducted in Vojvodina (5.3%), Serbia (2.9%), and Europe that found that the overall incidence rate of reinfections was 5.99 (95% CI 5.89-6.09) per 1000 person-months 14 (5-8), and a study of healthcare workers in the Midwest that found that participants working in COVID-clinical and clinical units experienced 3.77 and 3.57 times, respectively, greater risk of reinfection compared to those working in non-clinical areas. 15 This could be as a result of the different virus strains, which became widespread with the development of Omicron and Delta, the state of the economy, the different study locations, timing, research methods, and sample size.
The finding of this study is lower than that of a study done in Bangladesh, where 37 (38.5%) of full-dose vaccinated people were infected with the virus. 20
A study done in New Delhi, India, on breakthrough COVID-19 reinfections, after vaccinations in healthcare and other workers in a chronic care medical facility was conducted cross-sectionally and found that, after receiving any dosage of the vaccination, 19 people (16.9%) developed symptoms of COVID-19. 13 A systematic review study found almost 20% of patients, the second infection may worsen their symptoms, and those who are old or immunocompromised may experience catastrophic problems, 8 In a cohort study analyzing reinfection rates in Qatar, 22.2% of patients tested positive 45 days following the first positive test. 19 This difference may be due to the difference in time, race, and utilization of personal protective equipment.
A recent Swedish study found that, for a period of up to 20 months, natural immunity after three months was linked to a 95% reduced risk of SARS-CoV-2 reinfection and an 87% lower risk of COVID-19 hospitalization. Omicron, however, demonstrated a significant capacity for evading both naturally occurring and vaccine-induced immunity, resulting in diminished protection against reinfection but comparable protection against hospitalization or mortality brought on by reinfection. The fast growth of Omicron in South Africa resulted in a substantial rise in reinfections in mid-November 2021, in contrast to the Beta and Delta eras of dominance, during which there was no indication of immune evasion. Similar findings are significant for the dominance of Omicron globally and have also been documented in Qatar and the United Kingdom.6,8,20,21
In this study, healthcare professionals who did not receive training on infection prevention training on SARS-COV-2 was significantly associated with professionals who took infection prevention training on SARS-COV-2 (AOR = 7.177; CI = 4.761-9.698). The study conducted in Tertiary Care Hospitals in Peshawar, Pakistan, states that health professionals who did not take training for SARS-COV-2 are about 11 times more likely to be exposed to SARS-COV-2. 22 A study in Midwestern healthcare employees indicated a 2.07- and 2.28-fold increased risk of COVID-19 recurrence among COVID-clinical and clinical participants, respectively, who were more reinfected by SARS-COV-2. 8 This may be due to the fact that those health professionals who were trained on infection prevention may not use the personal protective equipment properly.
Those healthcare professionals who have chronic respiratory diseases were about 3 times more likely to be re-infected by SARS-COV-2 as compared to those who had no history of chronic respiratory diseases (AOR = 3.029; CI = 2.406-9.133).
Regarding vaccination status, health professionals who took only the first dose of the SARS-COV-2 vaccine were significantly associated with those who took the third booster dose. A study done in Vojvodina is almost similar in that incompletely vaccinated people were modestly more likely to be reinfected compared with recipients of a third booster vaccine dose. 14 This may be due to the fact that the vaccination protocol is almost the same globally. The profession of midwife was significantly associated with the other professions. This may be due to the fact that most midwives work in delivery and maternity wards, which may be crowded and have low Personal protective equipment utilization.
Strength and Limitations
Strength of the Study
The study used a structured questionnaire to assess all factors regarding SARS-COV-2 re-infection.
Limitations of the Study
The researcher was unable to employ a systematic random sampling strategy due to the limited time available for the investigation. Instead, the study participants were recruited consecutively until the sample size was reached. The information was only based on the respondents’ answers; this may introduce a bias. Not using laboratory results that were done on a regular basis will definitely underestimate the rate of re-infection.
Conclusions
This study showed the prevalence of SARS-COV-2 reinfection among vaccinated healthcare providers with pre-vaccination infection histories in Addis Ababa Public Hospitals in 2022. The study participants were selected from public hospitals. In this study, the magnitude of reinfection by SARS-COV-2 after vaccination with at least one dose of the vaccine and having a pre-vaccination infection history was high. IP training on COVID-19, educational status, profession, type of vaccine taken in the first dose, chronic respiratory diseases, and number of vaccinations were significantly associated with SARS-COV-2 reinfection after vaccination.
Recommendations
To Addis Ababa Regional Health Bureau
Giving infection prevention training on how to use infection prevention equipment for SARS-COVE-2 properly is recommended. Make available all PPE. Enforce health care providers to use the available PPE. Enforce health care providers to taking the vaccine according to the vaccination schedule up to third dose is recommended. Individuals who had history of chronic respiratory diseases should seriously use PPE and also take the booster dose.
To hospital administrators
Footnotes
Acknowledgements
We would like to thank Mr Melsew Getnet and Mr Ayine Birhane for their constant input during development of this research thesis. And our heartfelt thanks and appreciation also go to the study participants, the hospitals involved in this study, and my family and friends who provided helpful information and essential materials during this thesis preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethical approval and clearance were obtained from research and ethical committee of Kea-Med College and Addis Ababa research and emergency management directorate Institutional Review Board. Informed written consent was obtained from all study participants. Participants were informed about the objective of the study. After information is provided about purpose of the study, confidentiality of the information and all the participants were reassured of the anonymous (unnamed), and as personal identifiers were not used. The study was also carried out following relevant guidelines and regulations according to the Helsinki declaration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
All data included in this manuscript can be accessed from the corresponding author upon request through the email address.