
Abstract
Background
Occupational-related diseases or illnesses account for an estimated 2.4 million deaths worldwide every year. Currently, occupational hazards threaten healthcare workers’ (HCWs) lives, safety, and well-being. Therefore, providing the prevalence and major causes of occupational-related diseases may enable injury reduction and the creation of safer working environments, which are important for providing higher quality services. The current study aimed to determine the prevalence of occupational-related injuries and associated risk factors among HCWs, particularly in developing countries.
Methods
The articles published in English were retrieved using a combination of Boolean logic operators (AND, OR, and NOT), Medical Subject Headings (MeSH), and keywords in electronic databases (SCOPUS/Science Direct, Web of Science, DOAJ, PubMed/MEDLINE, CINAHL, and Google Scholars). Using Joanna Briggs Institute critical appraisal tools, a quality assessment was conducted to determine the articles’ relevance. In addition, the relevant articles were identified through a series of assessment and evaluation stages.
Results
About 721 studies were searched using electronic databases, of which 36 articles included 139,578 HCWs. The average prevalence of occupational-related injuries among HCWs in the career and previous last year accounted for 60.17%, ranged from 32% to 87.8% and 39.16%, ranged from 1.14% to 87%, respectively. The current study found that sex and hours worked, stress at work, occupation, age, training in infection prevention, use of universal precautions, recapping needles, ward work experience, staffing and resource adequacy, awareness, outdated guidelines, and previous exposure to sharp injury were statistically associated with occupational-related injuries.
Conclusions
This study revealed that 39% and 60% of HCWs experienced occupational-related injuries in the last year and during their career, respectively. Therefore, the appropriate measures must be taken to reduce the burden of occupational-related injuries by following standard precautions or occupational health and safety measures.
Keywords
Introduction
The healthcare sector is among the most unsafe working environments, putting many healthcare providers or workers (HCWs) and other staff members at risk of being exposed to various occupational hazards, such as various biological and nonbiological hazards.1,2 Currently, occupational hazards threaten HCWs’ lives, safety, and well-being.1,3,4
According to the International Labour Organization, occupational-related diseases or illnesses accounted for an estimate of 2.4 million of the total estimated deaths each year. 5 The World Health Organization reported that more than 2 million HCWs are exposed to sharp injuries, including needlestick injuries (NSIs), on a yearly basis. 6
HCWs experience more than 2 million workplace-related NSIs each year. 7 Sharp injuries to HCWs resulted in 16,000 cases of hepatitis C virus (HCV), 66,000 cases of hepatitis B virus (HBV), and 1000 cases of human immunodeficiency virus (HIV) infections in 2000. 3
Among sharp injuries, NSIs are among the most common occupational-related hazards among HCWs around the world. 7 The study conducted in 31 countries around the world reported that the last year's worldwide prevalence of NSIs among HCWs was 44.5% (95% CI: 35.7%-53.2%). 7 Another study conducted in sub-Saharan Africa also revealed that the lifetime and last 12 months prevalence ranged from 22% to 95% and 39% to 91%, respectively. 3
Additionally, exposure to blood and other infectious materials as a result of occupational-related accidents may represent a potential threat to HCWs. 8 Accidents involving contact with blood and other body fluids are attributed to the transmission of about 60 pathogens, of which HBV, HCV, and HIV are highlighted. 9
Furthermore, the risk of disease transmission from infected to other people as a result of exposure to an injury with sharp materials is estimated to be ranged from 6% to 30% for HBV, 5% to 10% for HCV; and 0.3% for HIV. 10 In general, occupational-related injuries among HCWs have continued to be a major health problem in healthcare facilities.11–13 Identifying and providing the prevalence and major causes of occupational injuries may enable injury reduction, creation of safer working environments, and reduced turnover and cost, which are important for providing higher quality services.7,14–16
Despite the major importance of these points, and in spite of various individual studies, there is no accurate evidence on the mean prevalence of sharp injuries, including sharp injuries and other injuries among HCWs, and associated factors, particularly in developing countries. Regarding occupational injuries, existing data are focused on published articles at the national level. Some reviews addressed occupational-related NSI3,17 but not other sharp injuries. The current study provides the prevalence of occupational-related sharp injuries, including NSI and other injuries. Therefore, the current study aims to determine the prevalence of occupational-related injuries among HCWs working in a health facility and associated risk factors in developing countries.
Materials and Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) criteria were followed for conducting the study. 18
Eligibility Criteria
Inclusion criteria: The systematic review includes studies that met the following criteria.
Population: Healthcare workers working in the health facilities regardless of their occupation.
Outcome: Studies reported quantitative results, such as magnitude, frequency, rate, or prevalence of any occupational-related sharp injuries and/or associated risk factors were included in the current study.
Language: Articles written in English language.
Types of included articles: Published articles available in full text and were included in the study.
Location or Region: Studies conducted in developing countries.
Survey period and publication year: Not limited.
Sources of Information
SCOPUS/Science Direct, Web of Science, DOAJ, PubMed/MEDLINE, CINAHL, and Google Scholars were used for literature searches, using main keywords. The following electronic databases were used: SCOPUS/Science Direct, Web of Science, DOAJ, PubMed/MEDLINE, CINAHL, and Google Scholars. The Boolean logic operators (“AND, OR, and NOT”), medical subject headings (MeSH), and keywords were used to search the articles from the included databases.
Search Terms and Strategies
The following are the search terms we used by the authors (DD, STT, AAT, WD, and DAM) for searching articles from the electronic databases: prevalence “OR ‘Magnitude’ AND ‘occupational’ OR ‘occupational related’ OR ‘work related’ AND ‘disease’ OR ‘injury’ OR ‘problem’ hazards” AND “healthcare workers” OR “health professional” OR “workers.” The articles were searched using Boolean logic operators (AND, OR, and NOT), Medical Subject Headings, and keywords. The search strategies used for searching the articles from PubMed are available as a supplementary file (Supplemental File I).
Furthermore, the articles were manually searched by the authors (DD, STT, AAT, WD, and DAM) to find those that were difficult to locate and missed from the included electronic databases or not indexed in the included databases. Finally, all of the identified keywords and index terms were cross-checked across the electronic databases that were included. Finally, the reference lists of the included studies were searched for further articles.
Study Selection Process
ENDNOTE software (Thomson Reuters) was used to remove duplicate articles. The PRISMA flowchart was used to guide the study selection process, displaying the publications that were included in the study and those that were excluded from the study with the reason for exclusion. The authors (DD, STT, AAT, WD, and DAM) independently selected the articles based on the titles and abstracts, applying the inclusion criteria. The articles were further read in detail and independently evaluated by the authors (DD, STT, AAT, WD, and DAM). Any disagreements made with respect to the inclusion of studies were resolved by consensus after discussion. Finally, studies that met the criteria were included in this study.
Data Extraction and Quality Assessment
The authors (DD, STT, AAT, WD, and DAM) extracted the data from the eligible articles. The data regarding author(s), year of publication, sample size, study region/country, occupation, and primary outcome (occupational-related sharp injuries, including NSIs and other sharp injuries among HCWs working in the healthcare setting) were extracted from the included studies. The data were extracted from the included articles using Microsoft Excel 2016. The Joanna Briggs Institute tool 19 was used to assess the quality and relevance of the included articles.
The evaluation tools have the following 9 evaluation criteria/parameters: appropriate sampling frame, proper sampling technique, adequate sample size, description of the study subject and setting description, sufficient data analysis, use of valid methods for identifying conditions, valid measurement for all participants, use of appropriate statistical analysis, and adequate response rate. Then, each parameter was evaluated as yes (score = 1) and no (score 0). The quality of the included articles was classified as high (85% and above), moderate (60%-85%), or low (60%). Disagreements made among the authors on what to extract were resolved by discussion after the same processes were repeated.
Results
Study Selection
A total of 721 articles were searched from the included electronic databases (SCOPUS/Science Direct, Web of Science, DOAJ, PubMed/MEDLINE, CINAHL, and Google Scholars). Then, 189 duplicated articles were excluded. Furthermore, 310 articles were removed after initial screening, and 59 articles were removed after full-text articles were assessed for eligibility. Finally, 36 articles were included in the systematic review and meta-analysis (Figure 1).
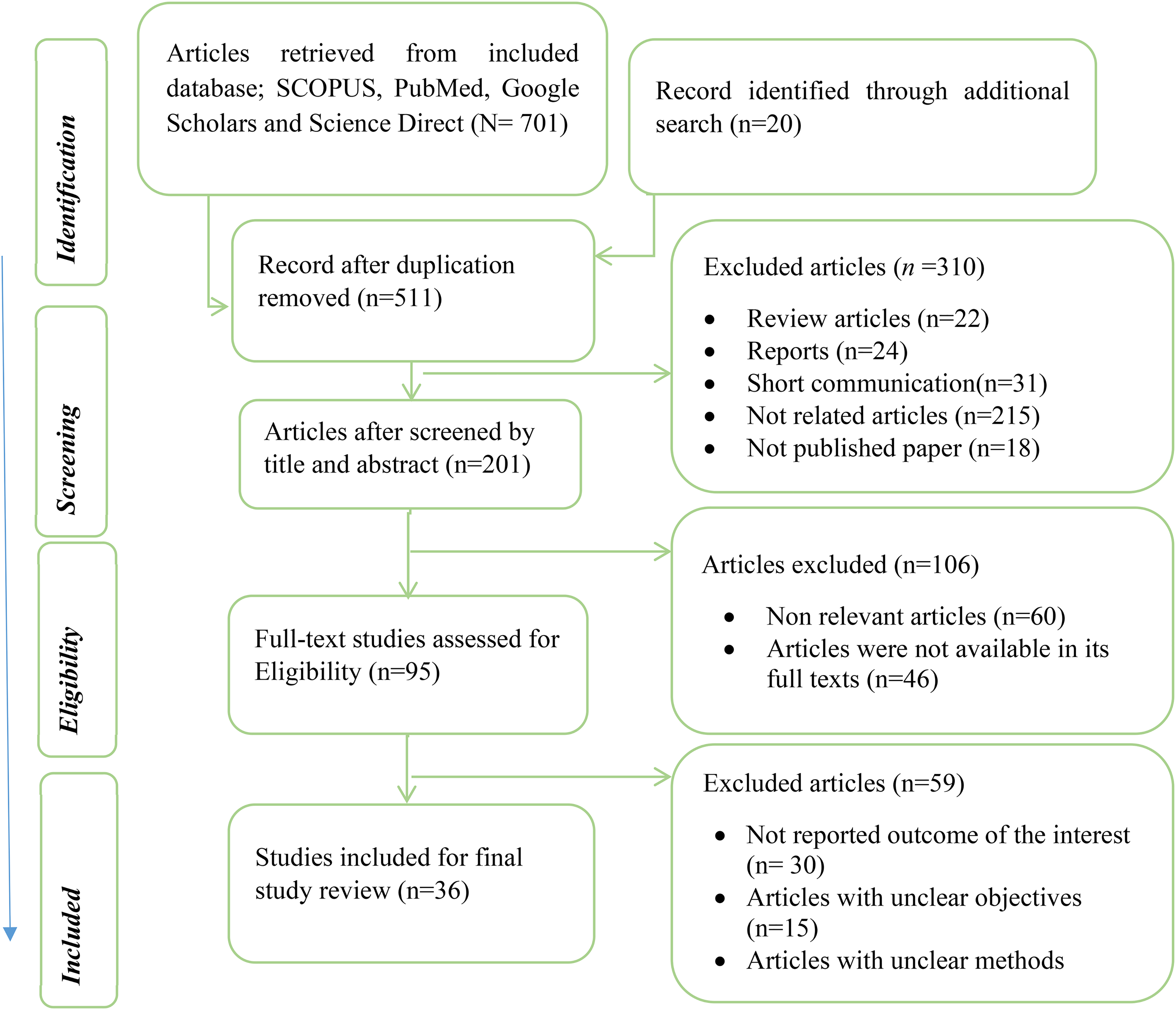
Study selection technique or process employed for selecting eligible articles, 2022.
General Characteristics of the Included Studies
In the current study, 139 578 HCWs, ranging from 76 to 61 309 HCWs were included in 33 articles, which were published from 2010 to 2021. Six articles were conducted in China,20–25 4 in Saud Arabia,26–28 2 in each India,28–30 Iran,31,32 Ethiopia,33–36 Nigeria,37,38 and Turkey.39,40 One study was conducted in each of Ghana, 41 South Africa, 42 Indonesia, 43 Taiwan, 44 Afghanistan, 45 Uganda, 28 Iraq, 46 Qatar, 47 Kenya, 48 Tanzania, 49 Korea, 50 Thailand, 15 Egypt, 51 and Afghanistan. 45
The mean prevalence of occupational-related injury among HCWs in the last year and career time was 39.16% and 60.17%, respectively. Workload, stress at work, occupation, age, training in infection prevention, use of universal precautions, recapping needles, ward, work experience, staffing and resource adequacy, awareness, outdated guidelines, and previous exposure to sharp injury were statistically associated with occupational related injuries (Table 1).
Characteristics of the Studies That Were Included in the Current Systematic Review and Meta-Analysis.

Abbreviations: NSI, needlestick injuries; NSSI, needlestick and sharp injuries; HCWs, healthcare workers; HCP, health care personally; OR, odd ratio.
Discussion
The current study aimed to determine the prevalence of occupational-related injuries among HCWs in developing countries. A total of 139 578 HCWs were included in the current review article. The prevalence of occupational injuries among various HCWs, including doctors, nurses, midwives, radiology, laboratory technicians, cleaning staff, mortuaries, housekeepers, public health, anesthetists, gynecologists, obstetricians, and surgeons was included in the current study.
The mean prevalence of occupational injury among HCWs in the last year was 39.16%, which was lower than the finding of another study that reported a 1-year global prevalence of NSIs among HCWs accounted for 44.5%. 7 Another study conducted in developing countries reported that the prevalence of NSI among HCWs was 35.7%, 17 which was lower than the current finding. The variation may be related to the scope of the study and the outcome reported. Because, the current study reported the prevalence of NSSIs, NSI, and sharp injuries.
Similarly, the current study found a lower prevalence than the findings of another study conducted in sub-Saharan Africa, which reported a one-year prevalence of NSIs ranged from 39% to 91%. 3 The variation may be attributed to the scope of the study and the type of occupational exposure to injury considered. Because the latter study was conducted mainly in sub-Saharan Africa that may not represent developing countries.
Furthermore, the current finding was supported by the findings of another study, which reported the last year's prevalence of occupational exposure to NSI among HCWs accounted for 37.8%. 55 In this study, the prevalence of occupational exposure to sharp injuries in the last year varied across the included study areas (Figure 2).

The prevalence of occupational injuries in the last year among healthcare workers.
Furthermore, the current study found that the mean prevalence of occupational injury in the career was varied across the included study areas, with the mean prevalence of 60.17%. Another study conducted in sub-Saharan Africa, which reported a lifetime prevalence of NSI ranged from 22% to 95%. 3 The variation might be attributed to the scope of the study location and the types of occupational-related injuries considered in the study. The later finding is based on studies conducted in sub-Saharan Africa.
The finding of the current study was lower than the finding of another study, which reported the prevalence of NSI in the career accounted for 64.1%. 17 However, it was higher than the findings of another study, which reported 57.0% of HCWs exposed to NSIs. 55 The variation can be attributed to the differences in types of exposure and regions or scope of the study. Because, the current study reported the prevalence of NSSIs, NSIs, and sharp injuries.
Furthermore, the current study found that the mean prevalence of occupational-related injury in the career time was varies across the world (Figure 3). Overall, the study found a prevalence of any occupational injuries in the last year and career time among HCWs working in the health facility, which accounted for 39.16% and 60.17%, respectively. However, occupational injuries have serious health problems and are a potential source of blood-borne pathogens such as HBV and HIV. Therefore, applying standard precautions, occupational health and safety measures or services, regular training on infection prevention, and proper implementation of guidelines plays a major role in reducing occupational exposure to sharp injuries and preventing infectious diseases among HCWs.

The prevalence of occupational-related injuries in the last year among healthcare workers.
Possible Prevention Strategies
Integrated approaches to occupational health and safety, including engineering measures, administrative policy, and the use of personal protective equipment should be implemented to control, eliminate, or reduce occupational exposure to injuries or hazards. 56 Furthermore, there is a need to implement priority strategies, which include strengthening of international and national policies for health at work, promotion of a healthy work environment, healthy work practices, strengthening occupational health services, development of occupational health standards, and strengthening of research. 57 By improving HCWs’ knowledge, behavior, or processes regarding the proper choice and safe operation of needles, scalpels, and other sharp devices necessary in the delivery of healthcare, education and training interventions also play a significant role in reducing sharps injuries. 58
Conclusions
This systematic review found a higher percentage of career time and previous 1-year occupational injuries in developing countries. The study suggests that about 39% and more than half (60%) of HCWs were experienced occupational-related injuries in the last year and in their career time, respectively. Therefore, efforts should be made to reduce the high burden of occupational-related injuries through effective implementation of standard precaution measures along with occupational health and safety measures.
Limitations
There was an unequal distribution of occupations among the included articles that made the comparison of occupational injuries among different occupations more difficult. On the other hand, the prevalence of occupational injuries in some countries was not covered due to the lack of studies.
Supplemental Material
sj-docx-1-hme-10.1177_23333928231192834 - Supplemental material for Occupational-Related Injuries and Associated Risk Factors Among Healthcare Workers Working in Developing Countries: A Systematic Review
Supplemental material, sj-docx-1-hme-10.1177_23333928231192834 for Occupational-Related Injuries and Associated Risk Factors Among Healthcare Workers Working in Developing Countries: A Systematic Review by Desi Debelu, Dechasa Adare Mengistu, Sina Temesgen Tolera, Alemayehu Aschalew and Wegene Deriba in Health Services Research and Managerial Epidemiology
Footnotes
Acknowledgments
The authors extend their deepest thanks to Haramaya University, Department of Environmental Health staff, for providing their constructive support.
Authors’ Contributions
DD conceived the idea and had a major role in the review, extraction, and analysis of data, writing, drafting, and editing of the manuscript. DD, DAM, STT, WD, and AA have contributed to data extraction. DD, DAM, STT, WD, and AA contributed to quality assessment, drafting, and editing of the manuscript. Finally, all authors DD, DAM, STT, WD, and AA read and approved the final version of the manuscript to be published and agreed on all aspects of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Almost all data are included in this study. However, additional data can be available from the corresponding authors on the reasonable request. Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.