
Abstract
Introduction
This analysis is a part of ongoing quality improvement efforts aiming at improving hypertension control among various racial minority groups seen in a large outpatient practice with a special focus on two war refugee populations, the Hmong and the Somali populations.
Method
Deidentified medical records were reviewed for adult hypertensive patients who had an outpatient encounter with a hypertension diagnosis during the years 2015 through 2019. The study outcome was the rate of uncontrolled hypertension, defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg, and stratified by race, age, and gender.
Results
There were 752,504 patient records representing 259,824 unique patients (mean age 61 ± 13 years) with 49.1% women, 82.1% white 8.3% African American, 4% Asian, 1.6% Hispanic, Somali 0.6%, and 0.2% Hmong. Hmong men had the highest rate of uncontrolled HTN (33.6%) followed by African American (31.3%) then Somali (29.2%). Among women, African Americans had the highest rate (28.6%) followed by Hmong (28.5%) then Somali (25.7%). In all races except Somali, the rate of uncontrolled hypertension was highest in the 18–29 age group, decreased progressively over the next several decades, then increased again in the ≥70 age group.
Conclusion
Hmong, African American, and Somali groups have the highest rates of uncontrolled hypertension. Efforts to address hypertension management need to be tailored to the specific characteristics of each racial group and to target young adults.
Keywords
Introduction
Hypertension is the leading cause of cardiovascular disease and stroke 1 and poses a significant economic burden with estimated healthcare cost of $48.5 billion annually. 2 The definition of hypertension has evolved over the years. The American College of Cardiology and the American Heart Association (AHA) define hypertension as systolic blood pressure (SBP) ≥ 130 mm Hg and/or diastolic blood pressure (DBP) ≥ 80 mm Hg in their joint 2017 guidelines. 3 Before that, the cutoff was ≥ 140/90 mm Hg which is the current definition of hypertension adopted by the European Society of Cardiology and the European Society of Hypertension. 4 The estimated prevalence of hypertension in the United States is 45.4% with more than half of the individuals having uncontrolled hypertension. 2 In the United States, studies have consistently demonstrated racial disparity in hypertension particularly among African American and Mexican-American individuals. 5 Immigrants and war refugees represent another vulnerable group6–8
Exposure to humanitarian crises such as war, leads to worsening cardiovascular disease. 6 Groups that are exposed to armed conflict in low and middle income countries appear to have a higher prevalence of coronary heart disease and cerebrovascular disease. 9 They are also subject to massive trauma, which can result in psychiatric disorders such as depression and posttraumatic stress disorder that can increase risk of cardiovascular disease. 7 Multiple studies have revealed a higher prevalence of cardiovascular disease and associated risk factors, including hypertension, hyperlipidemia, and diabetes, among refugee groups.6–8 Studies of Syrian, Hmong, and Cambodian refugees showed a high percentage of individuals with hypertension and other cardiovascular disease risk factors.6,10,11 The underlying pathophysiology in these populations is complex and likely multifactorial. It can be attributed to acute stressors during war, socioeconomic factors, and adapting to a more Western lifestyle including changes in physical activity and diet. These can result in stimulation of the sympathetic nervous system and a proinflammatory response with endothelial dysfunction, which prompt atherosclerotic changes.6,12,13
Our healthcare organization owns and operates several hospitals as well as primary and specialty clinics within the State of Minnesota which has a diverse racial/ethnic distribution including 79.1% white, 7.0% African American, 5.6% Hispanic, 5.2% Asian, and 1.4% American Indian and Alaska native. 14 Minnesota is also home for nearly 91,000 Hmong and 70,000 Somali people who entered the country as war refugees. 15 Over time, the shared experience within our organization indicated high rates of uncontrolled hypertension among the Hmong and Somali populations. These impressions generated the interest to analyze our institutional data to (a) assess the rate of uncontrolled hypertension, defined as ≥ 140/90 mm Hg, in our outpatient practice and (b) explore the racial/ethnic differences with special focus on the Hmong and the Somali populations.
Methods
This retrospective descriptive study is a part of a multifaceted efforts to address disparity in cardiovascular disease within our organization. Our intention was to understand the current state of disparity in hypertension control among our ambulatory patients. The study hypothesis was that there is a racial gap in hypertension control, regardless of antihypertensive regimen. The study outcome was uncontrolled hypertension which was defined as SBP ≥ 140 mm Hg and/or DBP ≥ 90 mm Hg. 16
We identified all adult patients who had an outpatient encounter with a hypertension diagnosis between 2015 and 2019. For a patient to be included, the diagnosis of hypertension had to be met within the prior 24 months by having had at least two qualifying encounters with hypertension, ICD 10 code I10. A qualifying encounter was defined as (a) a completed encounter (b) at one of the following clinics: internal medicine, family medicine, geriatric medicine, cardiology, nephrology, endocrinology, pediatrics, and med peds, and (c) with one of the following provider types: physician, advanced practice provider, medical resident, or fellow. Each patient's race/ethnicity was extracted from the electronic medical record (EMR) based on the self-reported race, ethnicity, country of origin, and primary language. Hmong patients were identified by the combination of Asian race and Hmong primary language. Somali patients were identified if the country of origin was Somalia or their primary language was Somali.
Patients were excluded if they were deceased, older than 85, receiving hospice care, a permanent nursing home resident, encountered at an immigration/refugee screening clinic, had end stage renal disease or kidney transplant, pregnant or had been pregnant within 12 months, between the ages of 66 and 85 with at least one encounter for frailty and advanced illness within 12 months, or were only seen by a nurse. The National Committee for Quality Assurance definition of advanced illness was adopted. 17
This analysis was done as an internal organizational effort to understand the impact of race/ethnicity on hypertension control, as such, the institutional review board classified it as quality improvement and allowed the analysis to proceed without requiring a full review or signed informed consent. Due to legal restrictions, raw data from this study cannot be shared. Aggregated data outputs are available from the corresponding author on reasonable request, following approval from the relevant data custodians.
Statistical Method
Patient characteristics of the 5-year cohort were summarized and described. The annual rate of uncontrolled hypertension was calculated as the percent of patients with elevated blood pressure (SBP ≥ 140 mm Hg and/or DBP ≥ 90 mm Hg) to the whole cohort and was stratified by age, sex, and race. If a patient had multiple encounters in a calendar year, the encounter with the latest date was used. If multiple encounters occurred on the same date, the encounter with the lowest blood pressure reading was used. Thus, although patients could only appear once in a year, they could appear multiple times over the 5-year period of observation. With the anticipated large sample size, only descriptive analysis was pursued without comparing the various groups for statistical difference. SAS 9.4 was used for all summarizations.
Results
A total of 752,504 patient records were included in the analysis representing 259,824 patients with mean age 61 ± 13 years and with 49.1% women, 82.2% white (n = 213,501), 8.3% African American (n = 21,429), 4.0% Asian not including Hmong (n = 10,307), 1.7% Hispanic (n = 4281), 0.6% Somali (n = 1483), 0.2% Hmong (n = 582), 2.5% other or mixed races (n = 6161), and 0.8% (n = 2080) with no race/ethnicity information (table 1). Those with other, mixed, or no race reported were included in the overall summaries but excluded from analyses of specific racial groups. On average, a patient contributed to 3 years of data with 13% of patients appearing in one year and 14% in all 5 years.
Patient Characteristics.

SD: Standard Deviation
Notes: Patient characteristics measured at first year in study cohort; No subgroup summary of n = 8241 with other, mixed, or missing race information; Diabetes/vascular Diagnosis is defined as having any of the following diagnoses diabetes mellitus type 1 or type 2, coronary artery disease, stroke, and peripheral vascular disease; All patients have hypertension diagnosis
The annual rate of uncontrolled hypertension ranged between 21.2% and 24.2% (Figure 1) and was higher in men than women (appendix Figures 1 and 2). Hmong men had the highest rate of uncontrolled hypertension (33.6%) among all men followed by African American (31.3%), Somali (29.2%), Hispanic (24.7%), Asian (20.5%), and white men (19.4%). Among women, African Americans had the highest rate of uncontrolled hypertension (28.6%) followed by Hmong (28.5%), Somali (25.7%), Hispanic (22.3%), Asian (19.2%), and white women (17.2%; appendix Figure 2).
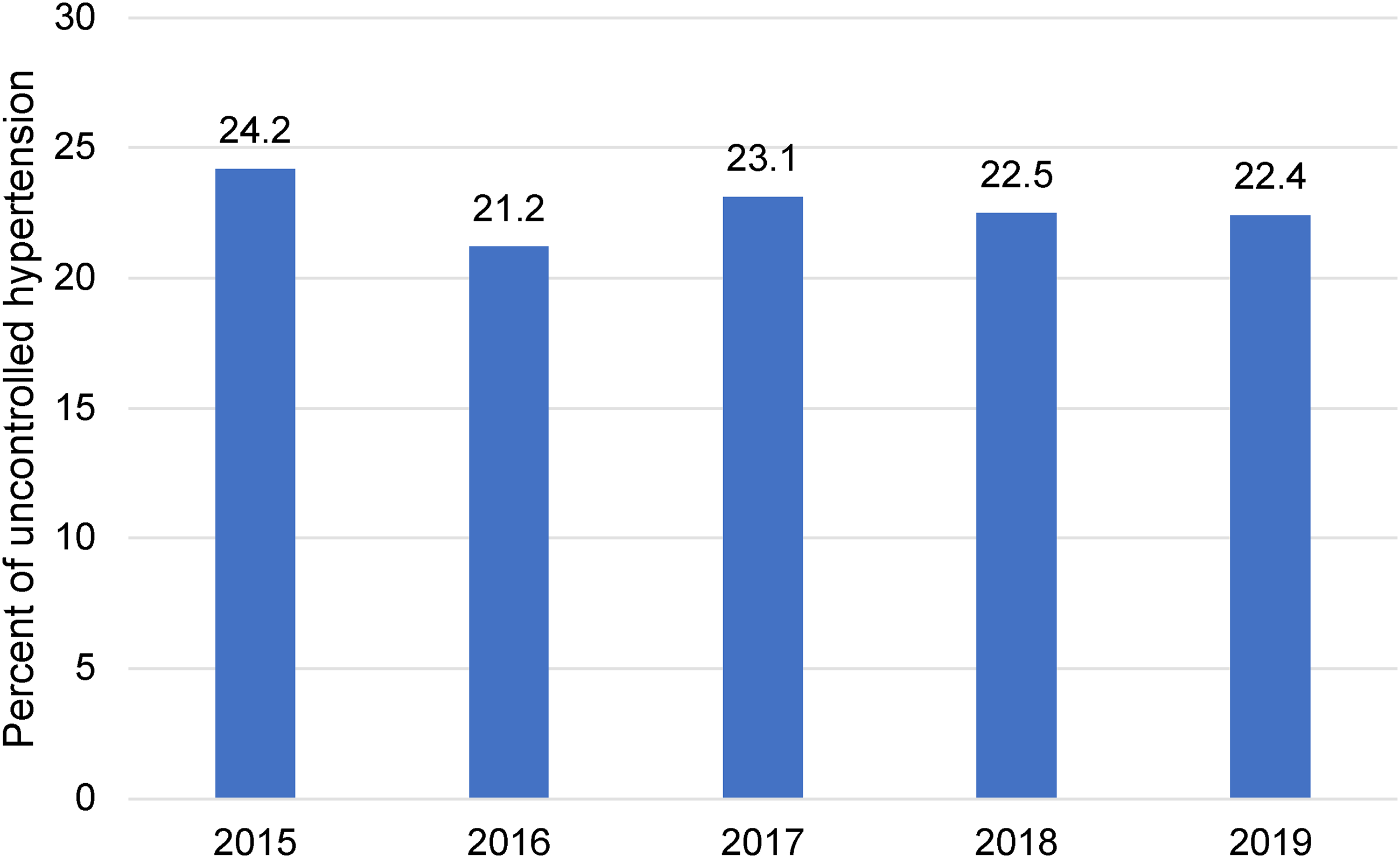
Prevalence of uncontrolled hypertension by study year. The rate of uncontrolled hypertension remained stable over the course of the study.
The rate of uncontrolled hypertension varied by age. The highest rate (33.7%) was observed in the 18–29 age group. The rate decreased progressively over the next four decades reaching its lowest (20.0%) in the age group 60–79 years then increasing again in patients aged 80 years and older (25%). This pattern remained consistent over the course of the study (appendix Table 1 and appendix Figure 3). Young African Americans had the highest rate of uncontrolled hypertension up to the age of 49 then from age 50 to 79, Hmong had the highest rate. Somalis had the lowest rate (28%) in the 18–29 age group and the highest rate (36.2%) in the ≥80 age group (Figure 2).

Prevalence of uncontrolled hypertension by age and race. The rate of uncontrolled hypertension was highest in African American patients followed by Hmong patients up to the fifth decade then the order is switched for the rest of the decades with Somali patients taking the first place in the ≥80 age group. All racial/ethnic groups except Somali had the highest rate of uncontrolled hypertension in the 18-29 age group with gradual reduction over the subsequent decades then a slight increase in the two oldest decades.
Discussion
In our sample of ambulatory patients, there was a racial disparity in hypertension control. While the observation of high rates of uncontrolled hypertension in African American and Hispanic groups is consistent with previous studies, the same observation in the Hmong and Somali groups is novel, and will be the focus of our discussion.
There is no epidemiologic data of hypertension in Hmong-Americans. The limited available literature suggests an increased risk of hypertension starting at young age. In a study that examined the rate of cardiovascular diseases among the newly arriving Hmong refugees, the rates of hypertension and pre-hypertension were 8.2% and 9.6% respectively in individuals ≤ 20 years and were 16.5% and 36.2%, respectively in individuals > 20 years. 10 Another study that examined the blood pressure of school children identified a high risk of hypertension in Southeast Asian refugee children, particularly among Hmong children. 18 As for the Somali population, there is even a smaller body of literature. One of the few studies of Somali cardiovascular health surveyed 1156 Somalis from our state of Minnesota and found a high prevalence of diabetes mellitus, obesity, dyslipidemia, and lack of physical exercise. 19
An important similarity between the Hmong and the Somali populations is that they largely entered the US as war refugees, a condition that has been associated with cardiovascular disease.6–8 War refugee individuals are at a higher risk for cardiovascular disease even compared to non-refugee migrants as noted by a recent systematic review of literature from 1977 to 2020 which calculated a relative risk of 1.71 (95% CI 1.03, 2.83). 20 Moreover, some studies have found a positive association between cardiovascular risk factors in immigrants and the length of stay in their new country. For example, a study of about 55,000 immigrants to the US showed that, after adjusting for region of birth, income, age, and sex, immigrants residing in the US for ≥10 years were more likely to be overweight/obese, diabetic, and hypertensive than those residing in the US for <10 years. 21
Another observation in our analysis is that the youngest age group having the highest rate of uncontrolled hypertension which was consistent in all 5 years of the study and all racial/ethnic groups except the Somali population. Epidemiologic studies have consistently shown high rates of uncontrolled hypertension in young adults.11,22,23 In a study that followed 3208 young adults ages 18–39 after the initial diagnosis of hypertension, only 48% achieved hypertension control within 24 months. 24 The explanation of this phenomenon is likely multifactorial and it is unknown if it varies by race. A qualitative analysis of two focus groups highlighted a negative perception of the diagnosis and treatment of hypertension among young adults, an aversion of using social media to communicate hypertension-related material for fear that their peers would see it, and a dislike of the educational material received in clinic because it did not address the issues that are important to young adults. 25 The same researchers surveyed the primary care providers who identified altered self-identity, blood pressure variability and medication side effects as important barriers to hypertension control in young adults. 26
Based on the results of this analysis, our organization is developing a program for hypertension management to address racial disparity using self-monitoring and virtual team-based care. We collaborated with the AHA to deploy blood pressure kiosks at the Hmong market in St Paul and the Division for Indian Work in Minneapolis. We have also collaborated with the AHA on cross cultural adaptation of education material to Hmong which included a document on hypertension. 27 We have organized multiple outreach events targeting local minority communities focused on hypertension. We are also conducting a research project utilizing a Mobile Health Clinic to identify individuals with elevated blood pressure, provide them with hypertension-related education, a blood pressure device for self-monitoring, and a referral to primary care.
Our retrospective study has limitations. Since it was initially conceived as an internal analysis to explore the magnitude of racial disparity and identify target populations, we did not include variables that are known to impact hypertension such as body mass index, concomitant conditions, medical management, lifestyle, or social determinants of health. The identification of the Hmong and the Somali subjects relied on the country of origin and the primary language as documented in EM.Therefore, we might have wrongly categorized some of the patients if the language or the country of origin were not the target ones. We had no control over missing or inaccurate data. Despite these limitations, our study remains informative with a large sample size, especially for the racial minorities of interest, a 5-years observation period, a wide range of patient ages, and a stable blood pressure trend over the study years. Further research is needed to confirm our findings and to examine the causes of disparity and interventions to address these disparities.
In conclusion, we did observe disparity in hypertension control in our sample of ambulatory patients. African American, Hmong, and Somali patients have high rates of uncontrolled hypertension. More granular data on race, ethnicity, and country of origin are needed on a state-level and national-level to better identify sub-populations with high rates of uncontrolled hypertension who are likely to need tailored interventions. The high rate of uncontrolled hypertension in the 18–29 age group highlights the importance of early intervention.
Supplemental Material
sj-docx-1-hme-10.1177_23333928231192830 - Supplemental material for Describing Racial Disparity in Hypertension Control in a Large Minnesota Outpatient Practice
Supplemental material, sj-docx-1-hme-10.1177_23333928231192830 for Describing Racial Disparity in Hypertension Control in a Large Minnesota Outpatient Practice by Haitham M. Hussein, Ella Chrenka, Mai Kau Yang and Karen L. Margolis, Thomas E. Kottke in Health Services Research and Managerial Epidemiology
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.