
Abstract
Objectives
In light of the increasing number of employed dentists and the decreasing rate of self-employed dentists, the factors that impact the decision to set up a dental office in Germany were investigated. Central to this approach is the provision of comprehensive dental care.
Methods
Using a pairwise comparison technique, the analytic hierarchy process (AHP), location factors identified as relevant in a systematic literature review and then prioritized by the professionals were weighted and ranked.
Results
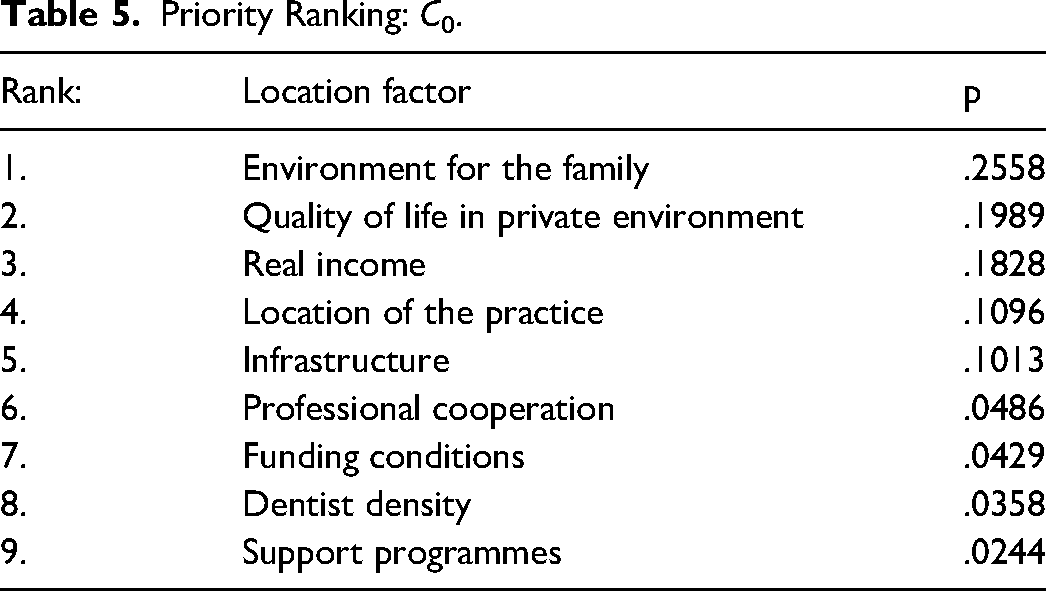
According to this, five factors generally dominate the decision to open a dental office. These are, in descending order: environment for the family, quality of life in the private environment, real income, perception of location, and good infrastructure. The strongest impact on the rank order of the influencing factors is the socio-demographic characteristic of gender. For female dentists, the family environment is in the first place (p = .3196/C.R. = 0.1502). For male colleagues, this influence ranks third (p = .1550/C.R. = 0.1468) and real income receives the first place (p = .244/C.R. = 0.1468). For female dentists, the influence of income ranks fifth (p = .076/C.R. = 0.1502). Female and male dentists who grew up in rural areas were less likely to prefer employment (13.6%) than subjects of urban origin (40.2%).
Conclusion
The method of AHP is a way to map a priority list of all relevant factors. It can successfully show variations related to specific personal attributes. Obviously, there are factors that are of greater importance for the decision-making process to set up a dental office.
Keywords
Introduction
Monitoring and assessing service provider satisfaction allows management and policymakers in general to identify specific areas for improvement in output and allocation. An analysis of the scientific literature shows that service provider satisfaction in the medical sector has so far rarely been investigated except in general practice.1–6 Researchers have tried to find a set of criteria covering a range of provider satisfaction characteristics. However, there is no scientifically sound evidence on the priorities of satisfaction criteria for practitioners of dentistry.
The paper analyses the satisfaction of service providers with the dental office based on the location factors perceived as relevant. An investigation was performed to identify variations among service providers’ priorities in socio-demographic characteristics.
Applying the Analytic Hierarchy Process (AHP) method to analyze the results of an expert survey, a new approach to service provider satisfaction criteria is presented. The paper puts forward a model that would allow those responsible for the control and mandatory provision of dental care (in Germany: Allgemeiner Sicherstellungsauftrag – § 72 SGB V) to prioritize location factors and better allocate dental services.
Background
There is a need to prevent a deficit of professionals in the German healthcare system.7,8 Under Pareto optimality, the highest possible level of welfare is given to everyone for the resources they own. This is automatically realized under ideal market conditions only, which allow for an efficient resource allocation by the “invisible hand”. 9 In the real world, however, ideal market conditions rarely exist. As a result, market failures occur, meaning that the market does not allocate resources efficiently and social welfare is less than optimal. The German health system is administered by the state through complex regulatory structures, whereby the market has little influence. Appropriate mechanisms must therefore emerge to manage resource allocation in response to the demand for social welfare. Two systematic literature reviews in the past have revealed that research on interventions to increase the proportion of health professionals practicing in rural and other underserved areas is of limited reliable evidence.10,11 In a literature review by A. Langer, it was found that the studies in the field of health services research on “Supporting and Inhibiting Factors for SHI-Physicians in Germany” are of low methodological quality because economic evaluations are not provided. 12 The prognosis in dentistry likewise indicates that it is imperative to critically look at the allocation and its causal factors. 13
The Career Choice in Dentistry
Until 2007, there was a legally mandatory regional allocation system for dentists, as there is in the medical sector. However, since the Statutory Health Insurance Competition Strengthening Act (the so-called Gesetzliche-Krankenversicherungs-Wettbewebs-Strärkungs-Gesetz), there are no longer any spatial allocation restrictions related to the setting up of dental offices. The same year, the opportunity for permanent employment was also anchored in law, the Panel Doctors’ Rights Amendment Act (the so-called Vertragsarztrechtsänderungsgesetz). Along with self-employment, there has been the option of working as an employed dentist since. Since that time, there have been several relevant developments. Firstly, investment costs rose substantially and were hyperinflationary. 14 Moreover, the number of new dental offices is declining. 15 Subsequently, the number of employed dentists rose continuously. In 2007, the number of permanently employed panel dentists was 726; in 2021, it was 16,259. At the same time, the number of self-employed panel dentists sank from 55,432 to 46,717. 16 While the population per dentist (dentist density) remains almost constant, the ratio of self-employed to employed dentists is changing noticeably in favor of employment. In 2011, 82.5% of practicing dentists in Germany were self-employed and in 2020 it dropped to 65.8%. 16 (Table 1)
Development of Dentist Density in Germany. 16

The federal state of Rhineland-Palatinate is mainly rural region. The forecast of the Health Care Atlas of the Association of Statutory Health Insurance Physicians Rhineland-Palatinate shows a total of 1524 dentists in need of replacement by 2023, which corresponds to 57% of the dentists currently working in Rhineland-Palatinate. 17 However, self-employment in small and low-populated areas was considered a desirable region to practice in by less than 10% of participants in Nele Kettler's survey. 18 Every new office set up or taken over contributes to the provision of a comprehensive public health service. While self-employed dentists are distributed regionally in about proportion to the population, the supply of dental care services in the sense of employment opportunities is mostly concentrated in large cities. 19
In the future, it will be more difficult to recruit new doctors to replace dental offices where owners are retiring for age-related reasons in many rural regions. 19 Considering the key decision-makers, these are first and foremost the providers of dental services. Therefore, the career choice of dentists can be analysed in detail to be able to steer the provision in the best possible way and to ensure nationwide access and availability of dental care.
Methods
As the review of previously published studies has shown, dentists’ decisions depend on both rational and intuitive factors and are always subjective in certain instances.20,21
Relying on the theory of bounded rationality, which is better known as the behavioral model of choice than the assumptions of the rational actor, and the theory of satisficing, which has developed from these assumptions, the factors found serve as heuristics that make it possible to represent the influences of the highly complex decision leading to an alternative. 22
Assessing and ranking a set of nine factors requires a process of complexity reduction. The process of creating a hierarchy of factors becomes more difficult with the integration of more factors. Therefore, a method is needed that makes an assessment seem viable. 23
An ordinary type of utility analysis seems unsuitable to evaluate a given set of alternatives based on several subjective and objective criteria. Answering the questions addressed in this paper requires a more elaborate method. 24 Following the framework of Sabaei et al the decision model was derived. The agents want to opt for the best alternative, but not only by considering the best and the worst criterion to have an impact on the final decision and a pairwise comparison is the preferred method to manage the scales. With an explicit method of multi-criteria decision-making (MCDM), the analytic hierarchy process (AHP), developed by the mathematician T. L. Saaty, complex decision-making can be determined. 25
The technique of the analytical hierarchy process (AHP) enables a decision-maker or group of decision-makers to deal with the main challenge of how to weigh a set of alternatives. The AHP as a multi-criteria decision-making approach (MCDM) appears to be a suited method for linking the identified factors and subsequently valuing its impact on the decision of the founders of a dental office. 26 It was used in this study to examine whether the output of the selected location factors has a decisive impact on the service provider's satisfaction with the dental practice. All criteria of a decision must be evaluated in pairwise comparisons of each other. Through the AHP, the importance of the factors can be assessed in relation to each other, and the available information can be used to take a decision. Thus, the most significant difference to the classical scoring model is that the evaluation not only distinguishes which factor or result is better or more important but also how much better or worse the respective variable is. Moreover, the computation of a consistency ratio can be used to verify the validity of the results. Assuringly, the methodological model was tested before this study. 27
Study Design
The type of mixed-method research design used in this study is exploratory sequential mixed. This entailed the collection of qualitative and quantitative data in two phases. Qualitative data collection and analysis were done through a systematic literature review. The second phase focused on tracing expert opinions on business indicators to identify the ranking of the relevant factors.
Survey Material
After the first review phase, from May to August 2020, all criteria found were categorized. Six socio-demographic characteristics were identified (see Table 2), and nine relevant heuristics were defined as selected location factors, shown in Table 3. Hometowns were categorized after the Federal Office for Building and Regional Planning (BBSR): origin as rural ≤ 20,000 inhabitants – origin as city > 20,000 inhabitants. The anonymous online survey was conducted from February to March 2021.
Relevant Personal Attributes.

The Selected Location Factors – SLF.

Participants
Based on the purposive sampling technique dentists (N = 375, aged 26–64 years old) participated in this study and were selected. All participants were members of the regional dentist association Landeszahnärztekammer Hessen (LZKH).
Anonymization of Participant Information
Identifying information has been anonymized to ensure participant safety and privacy.
Performance of AHP
The results of 36 pairwise comparisons of all experts in AHP according to Saaty's approximation method were calculated. 25 With the geometric mean aggregation procedure of the judgments of the individuals in a group, represented by reciprocal pairwise comparisons, the principals of AHP are satisfied. 28 The differentiation into groups was made comparatively in each case by the socio-demographic attributes.
The execution model has four steps.
First step is to structure a problem in a hierarchy (i.e.
26
). The second step is a pairwise comparison of all given alternatives In the third step the priority vector or Eigenvector is calculated by the approximation method.
Sum the elements of each column j: Divide each value by its column sum: Mean of row i: In this step the approximation of consistency (CI) following the axiom of transitivity is calculated.
It is based on the fundamental scale (i.e. Figure 1), also developed by T. Saaty.
25


Fundamental scale example.
Consistency (CI):
Axiom of transitivity: If
And by using the proclaimed ratio index (RI) each AHP will have a consistency ratio (CR).
Consistency Ratio (CR):
In his first remarks on the tolerance of inconsistency, T. L. Saaty recommended not much more than 10%, i.e. CR ≤ 0.1.
25
Inconsistency, which is an error in the measurement of consistency, has been widely discussed since then. A consistency ratio of
Results
The group decisions are plotted in the reciprocal matrix and calculated according to the approximation method (i.e., Step 2 to Step 4 20 ). A total of 375 out of 1162 dentists answered the questionnaire (47.5% female). This represents a response rate (RR) of 32.3%. Table 4 shows the reciprocal matrix A with the group results of all participants. It includes the calculated Normalized Eigenvektor (NEV) and the consistency ratio (C.R.). Further Table 5 summarizes the results. The priorities are here presented in descending hierarchical rank order. The AHP ranking can be precisely differentiated by the proportional breakdown. Thus, not only a nominal order but also the exact weighting (p) is evident. It is furthermore possible to look at the preferences according to socio-demographic characteristics. These results can now be compared in order and weighting.
AHP Overall: C0.

Priority Ranking: C0.
The group decisions were selected and ranked according to the socio-demographic data of the subjects (see Table 6). Table 7 shows exemplary group comparisons of interest. While there were no significant changes in the positions of the factors in the three age groups, there are considerable differences in position between the groups singles and married/in partnership, as well as parents and no children. Here there are differences in seven ranking positions. There are also seven changes in position between males and females. In contrast, only two differences in rank were evident among participants with a specialization compared to those with no specialization. The group decision of no main wage earners must be considered inconsistent and should not be assessed in the following. Further inconsistencies are to be rejected. While for male dentists, income comes first, for women the first rank is taken by the environment for the family. For females, real income comes in the fifth position. According to this survey, 34.66% of female dentists want to work as an employee. Among male dentists, 22.34% stated that they would prefer to be employed. Among dentists who had grown up in a rural area, 13.61% preferred permanent employment. Of those who were of urban origin, 40.20% stated that they preferred employment (see Table 7). The ranking of the urban dentists to the overall ranking (C0) did not change. For dentists of rural origin, however, the perception of the region of the dental office is more important than income. The competitors (dentist density) have a greater influence on the decision to set up a dental office, and professional cooperation is of much lower priority for this group.
Investigated Group Decisions.

Priority Ranking by Socio-Demographic Characteristics.

Discussion
This work is based on a literature review and an AHP, the popular integrated approach to multi-criteria decision-making (MCDM). 23 The AHP can process a large number of quantitative and qualitative factors, as in the present case. The study conducted is an instrument for evaluating relevant criteria in the decision-making process of dental providers, incorporating socio-demographic characteristics. The criteria and characteristics used should always be reviewed.
The five most influential criteria together result in a total weight of 85.13% to 83.35% regarding the decision groups investigated. The factors of dentist density, professional cooperation, financing conditions, and funding programs therefore together account for only between 14.87% (female) and 16.84% (rural). They can be considered negligible for the decision.
According to current findings, social factors seem to be much more relevant than classic economic factors. This can help affected municipalities in rural areas to change their focus on promotion activities about securing the dental health supply. The gender-specific differences also suggest that the monetary influencing factors are marginal with the trend of increasing numbers of female dentists. A trend towards employment can also be justified by the strong desire for work-life balance, meaning the strong weighting of the factors ‘environment for the family’ and ‘quality of life in the private environment’.
Practice
For the individual dentist, it may be useful to develop a more complex representation with subcategories. After that, the decision could be structured and, if necessary, simplified or even improved. Following the results, it seems to make sense to consider the socio-demographic differences and explore them in more detail. One way of further development could be to ask the students at the end of their studies to evaluate the factors. Gender-specific research on self-employment in dentistry can also make an important contribution to future dental care concepts in the long term. The finding that the influence of private quality of life and family environment is most relevant for the majority of respondents should be a basis for further considerations.
Policy
However, for a global consideration and implementation within the framework of a survey, it seems sensible to keep the comparisons to a minimum. It could be a relief to consider some factors as negligible based on the present results in order to improve the implementation of further studies.
The findings from this work confirm that employment is becoming more and more popular but can also be weakened for rural regions when looked at in a differentiated way. But in principle, it can be expected that dentists are much more likely to settle close to where they grew up. One potential strategy to address the imminent shortage of dentists in rural areas and promote community development is to focus on promoting dental career paths in primary and secondary schools. By actively encouraging and engaging students in rural communities to consider dentistry as a viable career option, there is a higher likelihood of increasing the number of dentists who will return to their own communities for practice. This targeted approach aims to attract new dental providers and combat the scarcity of dentists as the retirements of private practitioners continue as the existing misallocation is further increasing. Thus, advertising the attractiveness of a region can only be successful to a limited extent. However, a good infrastructure, together with a family-friendly environment and attractive leisure opportunities, can already significantly influence the decision. The greater number of employment opportunities in urban areas may be a major reason for the high preference for practicing as an employed dentist. After all, 40.20% of dentists of urban origin and only 13.61% of dentists of rural origin want to work as employees.
Limitations
The desired data depends on the reliability of the designed questionnaire. The number of respondents provides a significant and representative sample. But the quality of the dentists surveyed can be discussed as insufficient. A proportion of 54% of the participants was already set up in their practice. Depending on the objective, this circumstance can lead to bias. There is a difference between assumptions and experience, which can be seen as an additional bias in the weighting of the factors.
In addition, limiting the analysis of influences to a single point in time is less meaningful than a longitudinal study. Thus, in addition to the statistical accuracy of the evaluations, a trend analysis would also be more evident.
The AHP has been criticized in the literature, too. The most discussed weakness of its theoretical foundation is the rank reversal problem. Saaty's approach is extremely sensitive, given that the rank requirement may change if an option or attribute is added or removed. Ishizaka and Lusti could demonstrate that the ranking contradiction phenomenon increases linearly with the inconsistencies and the matrix dimension. 31 They also showed that only very close priorities suffer from ranking contradictions.
Conclusion
The approach proposed could increase the effectiveness of directing resources to the factors that are most influential in dental provider satisfaction. It can assist researchers and policymakers in effectively addressing the problem of declining dental offices. It may be appropriate to advertise dental offices in a targeted manner to service providers to solve allocation issues. The ability of the AHP to present the priorities and weightings of the factors examined in a simplified and clear organizational structure can assist municipalities and stakeholders to develop strategies and create targeted incentives to ensure dental healthcare providers in the areas under consideration. To gain deep insights into the motivations of the dental providers, this method inevitably makes a priority list out of all the participants’ weightings. In each individual consideration, the relevant factors are always implicitly included. Securing dental care in rural areas will remain a necessary subject of future debate. Strategies to address this issue are desirable and will hopefully be the subject of future research.
Footnotes
Acknowledgments
The author is thankful to the Landeszahnärztekammer Hessen for supporting the expert survey by providing a link in their mobile Application.
Ethical Approval and Participant Consent
An ethical board approval was not required for this study as the online survey conducted was anonymous and did not contain any ethically concerning questions. By participating in the survey, each participant consented to the use of their anonymised data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.