
Abstract
Introduction
Conflicting reports for preterm birth and stillbirth during the lockdown imposed during the COVID-19 pandemic have emerged. Most of the studies are related to the initial waves of the pandemic.
Objectives
This study aims to evaluate changes in preterm birth and stillbirth rates during various waves of COVID-19 in northern Iran.
Methods
This is a retrospective cohort study to evaluate preterm birth and stillbirth rate based on weight distribution per 1000 live births during lockdown periods in 5 peaks of the COVID-19 pandemic using the regional data registration system at Mazandaran University of Medical Sciences in northern Iran. We compared these rates with the corresponding months 4 years before the pandemic. The odds ratio for the primary outcome was estimated by logistic regression.
Results
We observed an overall increased rate of preterm birth during the pandemic compared to the pre-pandemic period (4.7% vs 2.8%, P < .001). The overall stillbirth rate increased during the COVID-19 pandemic compared to the pre-pandemic period (7.48/1000 vs 5.41/1000, odds ratio: 1.38 [1.21-1.57]). This increase in the rate of stillbirth was significantly observed in the fifth wave of the COVID-19 pandemic (P < .001).
Conclusion
Our study showed that adverse pregnancy outcomes increased during lockdown periods of a global pandemic. Further studies from geographically diverse regions to evaluate different behavior changes during pregnancy and access to prenatal services, and its impact on pregnancy outcomes is recommended.
Introduction
Stillbirth and preterm birth are the 2 main causes of neonatal mortality worldwide. 1 Various causes can lead to stillbirth and premature delivery. 2 The COVID-19 pandemic has imposed important challenges on health systems and its management policies such as lockdowns made access to health centers difficult. 3 At the beginning of the pandemic, a decrease in preterm birth rates was reported in Denmark, Netherlands, and Ireland.4–6 On the other hand, an increase in stillbirth rate was reported in the United Kingdom, Italy, Nepal, and India.7–10 Conflicting results have been reported regarding the rate of stillbirths and preterm births during the pandemic, and different results have been shown in meta-analyses.11,12 Reduction of stress due to balance between work and life, more rest for pregnant mothers, less exposure to infections, fewer medical interventions, reduction of trauma and pollution, and more strict adherence to health principles are possible reasons for reducing the rate of premature birth during lockdown periods. On the other hand, the reasons for the increase in premature birth rates in some studies included more stress due to concerns about the pandemic, financial challenges, and reduced maternity services. 2 Many of these studies did not assess preterm birth and stillbirth simultaneously to capture the true impact of the pandemic. 13 Furthermore, most of these studies were only related to the onset of the pandemic.
Mazandaran is one of the most populous provinces in northern Iran. Its area is 23 842 square kilometers and it has also been identified as one of the most affected regions since the spread of the SARS-CoV2 was announced. 14 After the official report of the first case of infection with COVID-19 in Iran on 28 February 2019 and its rapid spread in all the provinces of the country, the plan of social restrictions including the closure of schools and sports halls, reducing office hours, controlling entry and exit to cities, staying at home, and social distancing was implemented from March 4, and, in the first wave of the pandemic, a strict lockdown plan was implemented and continued in subsequent waves. 15
Most of the studies conducted about the rate of stillbirths and premature births were limited to the beginning of the pandemic, and fewer data have been published regarding the impact of lockdown during the next waves. In addition, conflicting results were shown in different parts of the world, and researchers have recommended the need for more investigations. 16 Although periods of COVID-19 lockdown have been associated with reductions in preterm births in some high-income countries, it is unclear how changes in low-income settings have affected these rates concerning access to maternity health services. 17 Therefore, this study was conducted to investigate the rate of stillbirths and premature births during the lockdown period of COVID-19 during the 5 waves of this disease in northern Iran.
Materials and Methods
In a retrospective cohort study, we examined the entire number of preterm babies and stillbirths in Mazandaran province, where the lockdown was implemented over the 5 waves of the COVID-19 pandemic from March 2020 to September 2021. We obtained information over the study period from the Iranian Maternal and Neonatal Network (IMaN). This network in the Department of Maternal and Neonatal Health of the Vice-Chancellor of Treatment records all births (live and dead) and maternal and neonatal health information electronically in hospitals across the country. The rate of stillbirths and premature births in these periods was compared with similar periods in the 4 years before the pandemic (2019-2016). The 5 pandemic waves (peaks) in this study included March to April 2020, July to August 2020, November to December 2020, April to May 2021, and July to September 2021.
We included all singleton or multiple pregnancies delivered at or greater than 24 weeks and before 37 weeks. Babies who were born at full term and less than 24 weeks were excluded from the study. The study area included 14 cities with 17 maternity hospitals. Since cases of preterm birth outside maternity hospitals are very rare in Mazandaran province, the study constitutes the entire population of eligible newborns inside maternity hospitals.
We collected stillbirth rates as well as preterm births based on weight distribution including VLBW (very low birth weight) and ELBW (extremely low birth weight) per 1000 live births. Then we compared each of these ratios with the same months of the previous 4-year period. A stillbirth was defined as the birth of an infant at 24 weeks of gestation or more who died before or during delivery. Because all premature babies were included in the study; therefore, the sampling method was a census, and accordingly, the sample size was not determined.
Statistical Analysis
All data analyses were performed using STATA version 14 software. Data description was done with percentage, mean, and standard deviation. To compare the rate of premature and stillbirth in the period before and after lockdown, Rate-Ratio with a 95% confidence interval (CI 95%) was presented. the odds ratio for the primary outcome was estimated by logistic regression. P < .05 was considered significant.
Ethical Consideration
The study was approved by the research ethics committee of Mazandaran University of Medical Sciences (N: 1399.8065). The dataset did not contain information that could be used to identify the patient, so the study was exempt from informed consent requirements.
Results
From March 2020 to September 2021 (during the 5 pandemic waves), there were 45 976 live births, and the total number of live births during the 4 years before the pandemic (the pre-pandemic period) was 124 920. Overall, a significant increase in preterm delivery rates was observed during the pandemic period compared to pre-pandemic years (4.7% vs 2.8%). Table 1 illustrates the rate of preterm delivery according to the weight classification of the baby in 2 categories, VLBW and ELBW.
Total Preterm Birth Rate per 1000 Live Births During and 4 Years Before the Pandemic.
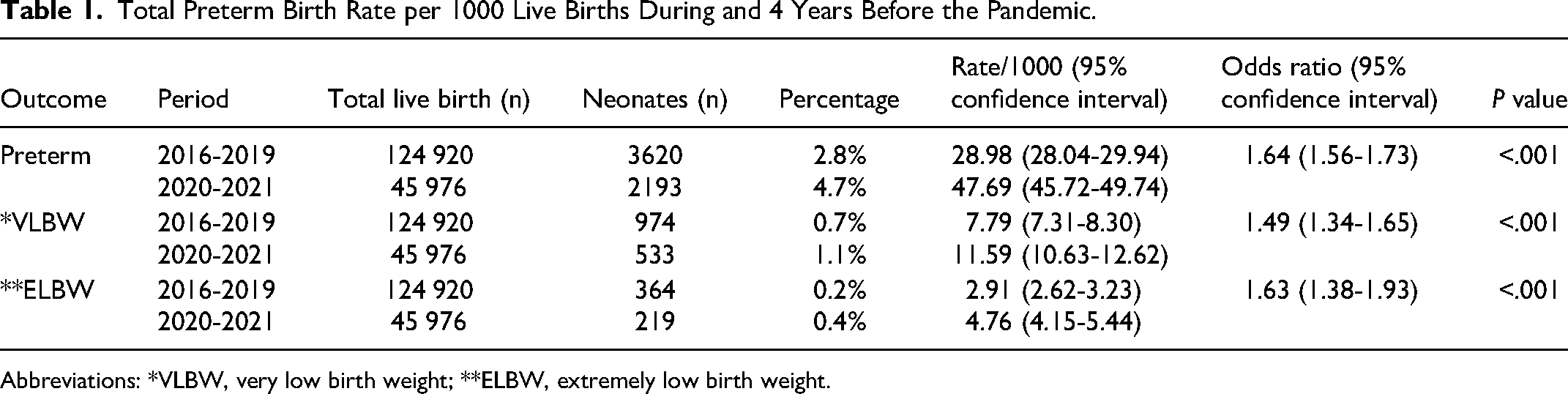
Abbreviations: *VLBW, very low birth weight; **ELBW, extremely low birth weight.
Details of preterm births during each wave of the COVID-19 pandemic compared to similar periods in the 4 years before the pandemic are shown in Table 2.
Comparing the Rate of Preterm Birth in 5 Waves of the Pandemic With Similar Pre-Pandemic Periods.

Abbreviations: *VLBW, very low birth weight; **ELBW, extremely low birth weight.
The first peak of the pandemic was the only period in which the preterm birth rate in the region unexpectedly decreased compared to similar periods before the pandemic (Figure 1), although this difference was not statistically significant (P = .064). The preterm birth rate per thousand live births during the pandemic and pre-pandemic period was 6.00 (3.80-9.00) and 4.77 (3.84-5.87), respectively, in private maternity hospitals which had no statistically significant difference (odds ratio: 1.26 [95% CI: 0.79-1.98], P = .32).

Comparison of preterm birth rates (per 1000 live births) in the first peak of the pandemic with the corresponding months 4 years before the pandemic.
Overall, there was a significant increase in stillbirth during the 5 waves of the COVID-19 pandemic compared to the pre-pandemic period (7.48 [6.71-8.32] vs 5.41 [5.01-5.83], RR: 1.38 [1.21-1.57]). Details of stillbirth rates during the 5 waves of the COVID-19 pandemic are given in Table 3. During the fifth wave of the COVID-9 pandemic, a significant increase in the rate of stillbirth has been observed (P < .001).
Comparison of Stillbirth Rates in 5 Pandemic Waves With the Same Period Before the Pandemic.

Discussion
The results of this study showed that during the COVID-19 pandemic, the births of premature babies increased compared to the previous 4-year period. Because of known seasonal fluctuations in birth or access to health services, we compared the difference between the periods of national COVID-19 lockdown with the corresponding epochs of the previous 4 years. An unprecedented reduction in the birth of premature babies during the first wave of the pandemic was observed although it was not statistically significant. The increase in the rate of stillbirths was detected during the pandemic period and in a significant way in the fifth wave.
Maslin et al investigated the rate of preterm births before and during the COVID-19 pandemic in South-West England. The decrease in premature births in this study has been maintained even in the period of COVID-19 and, unlike our study, it did not affect the increase in stillbirths. 18
Contrary to some studies that reported a decrease in the hospitalization of premature babies during the lockdown period of COVID-19 at the beginning of the pandemic,6,16,19–21 a retrospective study on 46 neonatal intensive care units from 17 different countries, showed that the number of extreme preterm hospitalizations did not change significantly during the lockdown period. The selected countries were selected from different regions of Western and Eastern Europe, Asia, and North America, and there were no statistical differences between the levels of lockdown restrictions. This study did not confirm previous reports of a major reduction in the rate of extremely preterm births during the first phase of the pandemic. However, as the authors of this article have mentioned, this survey was conducted only in one wave. 22
A serious decrease in the rate of emergency births was observed in a study by More et al during the pandemic, and the rate of stillbirths increased significantly at the same time. The authors of this study believed that the stay-at-home policy led to patients’ fear of going to the hospital and higher stillbirth rates. This study did not investigate subsequent waves of the disease and did not conduct more specific research on preterm infants. 23 Although it seems that the benefits of quarantine have been stronger in developed countries, the reduction of preterm births during the lockdown period is not only related to the socioeconomic development of countries. Many other factors can also affect this rate.24,25 A nationwide cohort study in Sweden showed that there is no association between birth during the pandemic and the risk of preterm birth or stillbirth. 26
The trend of premature births in our study has been increasing, which requires the investigation of its various causes and factors, in which even issues unrelated to the pandemic can be considered involved. Previous studies showed that most maternal healthcare indices sharply declined with the announcement of the COVID-19 pandemic in Iran but soon started to recover after a gap of 1 to 2 months. 27
Two studies in India, like our study, reported an increase in stillbirths during the COVID-19 lockdown period. In this study, the lack of prenatal care and lack of access to the urgent transfer system to the hospitals were mentioned as one of the possible main risk factors for this increase. However, there was no significant difference between the causes of stillbirth between the period of COVID-19 and other periods. 28 In the second study, fear of contracting the disease, inadequate quality care services, and mother's transportation problems were the main obstacles to mothers’ access to care services and increased intrauterine death. 29
In a study conducted regarding health services during the COVID-19 pandemic in Iran, private hospitals scored much higher in patient satisfaction than public hospitals. 30 The rate of preterm birth in our study did not show any difference between private and public hospitals before and after the pandemic. As almost all tertiary maternal hospitals in Mazandaran province are located in public maternity hospitals, it seems the reason for the increase in stillbirths in our study may have not been by chance. During the immediate period of COVID-19, high-risk mothers were less likely to be transferred to tertiary care facilities. Probably, this initially led to a decrease in the premature birth rate, but then the proportion of babies with certain consequences such as stillbirths increased.
In our study, an increase in stillbirths was seen in the fifth wave of the disease, which coincided with the spread of the SARS-CoV-2 Delta variant in the country. The Delta variant severely affected Iranian health services due to a serious shortage of medical supplies. 31 Mothers’ fear of contracting the disease and lack of access to maternity care in this period led to the lack of adequate prenatal care and an increase in stillbirths. Due to the lack of access to the pregnancy records of these mothers, we could not investigate the causes of this issue. It seems that policymakers and health service providers should focus more on maternity care during COVID-19 and other pandemics in the future, especially in developing countries. In addition, by increasing women's awareness through mass media and making prenatal services more accessible, using virtual care systems during the lockdown period can be effective in reducing adverse pregnancy outcomes.
Recently, a meta-analysis using harmonized data from 26 countries reported evidence of an increased risk of stillbirth in the first month of lockdown in high-income countries. An association between lockdown and stillbirth in the second to fourth months of lockdown was found in Brazil. Researchers found no association between lockdowns and stillbirths in the second to fourth months of the lockdown for the high-income countries, although the researchers noted that the estimates may be imprecise due to the rarity of the stillbirth event. In addition, they concluded that the moderate reduction in preterm birth observed during early pandemic lockdowns was interpreted as a cessation of large numbers of preterm births globally and warrants further research into causal pathways. 32 In our study, the reduction of preterm birth occurred only in the first wave of the disease at the beginning of the COVID-19 pandemic. However, the rigid stay-at-home policy during the first wave can lead to a reduction in the mother's exposure to infectious agents or environmental physical hazards, which itself plays an important role in preventing preterm birth. With the subsequent acquaintance with health protocols, the process of childbirth has become closer to the pre-pandemic situation and has taken an increasing trend. This could have various reasons not related to the pandemic, but the involvement of pregnant women with SARS-CoV-2 could also be an increasing factor in the early termination of pregnancy in our region. 14
The strength of our study is that we have examined the effects of lockdown during different waves of the COVID-19 pandemic, while most studies have only examined one (initial) wave of the disease. Such an inclusion consistency over 5 waves and comparison with the corresponding epochs of the previous 4 years could reduce the bias.
The following limitations are acknowledged in this study: First, in the data registration system used, we were unable to distinguish mothers with COVID-19 infection from uninfected mothers to investigate the intrinsic role of COVID-19 infection in causing preterm birth or stillbirth. Second, due to the retrospective nature of the birth cohort data, we could not examine all the parameters involved in preterm birth. Our observations suggest a theory of potential association between changes in socioenvironmental conditions and lack of access to appropriate prenatal care during the lockdown in a low-income setting, and this study was not designed to assess causality.
Conclusion
Despite the decrease in preterm births during the lockdown period in the first wave of COVID-19 infection, the overall increase in the rate of preterm and stillbirth rates during the other waves suggests that each community may have a different behavioral and socioenvironmental response during that period.
It may have obvious negative health effects and increase adverse pregnancy outcomes. Further studies are needed to investigate the impact of lockdown on behavior change during pregnancy and access to prenatal services so that the results can be effective for better management in recent and future pandemics.
Footnotes
Authors’ Note
All data generated or analyzed during this study are included in this article. Ethical approval was obtained for this report from the research ethics committee of Mazandaran University of Medical Sciences (IR.MAZUMS..REC.1399.8065). As the study was retrospective and the dataset did not contain information that could be used to identify the patients, the study was exempt from informed consent necessities.
Acknowledgments
The authors would like to thank Mozhgan Gholami for her assistance in the data collection and the Clinical Research Development Unit (CRDU) of Boo Ali Sina Hospital, Mazandaran University of Medical Sciences for their support and cooperation throughout the study.
Authors’ Contributions
RF, HN, and VGS are responsible for designing and conducting the study and they developed the first draft manuscript. MM is responsible for data interpretation and analysis. All authors agreed on the final submitted version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted by a grant from (1399.8065) Mazandaran University of Medical Sciences as a residency thesis.