
Abstract
Background
Worldwide 1.2 billion women suffer from micronutrient deficiency. Feeding diversified foods during pregnancy prevents pregnancy complications such as severe anemia, low birth weight, and birth defects. However, the status of minimum dietary diversity and associated factors among pregnant women were not explored in the study area; therefore, this study was conducted at the Arba Minch Health and Demographic Surveillance Sites (AMHDSS).
Method
A community-based cross-sectional study was conducted from December 19, 2021, to October 30, 2022, on randomly selected 635 pregnant women. The data were collected through face-to-face interviews, and measurements of mid-upper arm circumference using a tablet; then exported to Statistical Package for Social Sciences version 25. Descriptive statistics were used to describe the characteristics of the study participants and presented by text, figures, and tables. Binary logistic regression was used to determine factors associated with pregnant women MDD-W. Independent variables with a P-value < .05 were considered as associated factors.
Findings
98.2% of the pregnant women responded to this survey, more than half, (53.3%) of them achieved MDD-W, and 24.2% of the pregnant women were undernourished. The MDD-W was associated with household food security (AOR = 0.55, CI: .36, .83), meal frequency, (AOR = 1.62, CI: 1.1, 2.5), house ownership (AOR = 0.52, CI: .29, .9), ownership of banana farms (AOR = 1.7, CI: 1.02, 2.8), antenatal follow-up (ANC) (AOR = 1.9, CI: 1.1, 3.3), and occupational status (AOR = 6, CI: 2.1, 17.6).
Conclusion
The MDD-W outcome in this study was higher than that in other studies. The MDD-W is associated with, ANC follow-up, meal frequency, living in a food-secured household, ownership of a house, and pregnant women's merchant occupation. For optimal pregnancy outcomes; the AMHDSS and stakeholders might need to work in collaboration to increase ANC coverage and meal frequency for pregnant women. In addition, micronutrient supplementation, and increasing the availability/production capacity of food-insecure households are expected.
Introduction
Pregnancy is a unique period in a woman's lifetime and is characterized by radical anatomical, physiological, and biochemical changes in the woman's body system. 1 Pregnancy requires extra energy and micronutrient supplementation to overcome the growing demand of the fetus; therefore on average, a pregnant woman may need 85, 285, and 475 kcal/day during her first, second, and third-trimester, respectively, more than a nonpregnant woman. 2 Essential micronutrients and macronutrients are also the major food items needed for the normal anatomical and neurological development of a growing fetus.3,4
Most micronutrients that are necessary for normal pregnancy are found naturally in different food items, and few micronutrients are found when a pregnant woman is supplemented by a healthcare provider during antenatal clinic (ANC) visits or her pre-conception care; Iron, iodine, calcium, vitamin A, B12, D, antioxidants, and water are among the essential micronutrients. 5
Evidence suggests that there is a direct relationship between improved maternal dietary diversity and optimal brain function of newborns and children because nutrients are the fundamental elements of human body components such as deoxyribonucleic acid synthesis, neurotransmitters, hormone metabolism, and an important constituent of enzymes.6,7
The global estimated prevalence of at least one micronutrient deficiency (MD) among women reproductive-aged (15-49) is 69% which is approximately 1.2 billion women suffering from MD. The majority, (57%) of micronutrient deficiencies occur in east Asia and the Pacific followed by sub-Saharan Africa. Approximately 384 million east Asian and 307 million south Asian women are affected by MD. 8 Findings from developing countries have shown that micronutrient deficiency and protein-energy malnutrition have a substantial impact on mortality and disability-adjusted life years. 9
Worldwide around 41.8% of pregnant women are affected by anemia, and at least half of this anemia burden is assumed to be related to iron deficiency anemia which would have been prevented by consuming diversified foods. Anemia during pregnancy increases the risk of premature delivery 2-fold and 3-fold for low birth weight neonates.3,10 On the one hand, one of the hypotheses for the development of preeclampsia is inadequate calcium-rich food consumption in pregnant women; pre-eclampsia contributes 15% to 20% of all maternal deaths (40 000 maternal deaths per year) and 37% of neonatal deaths worldwide.3,11–13
Only, 28.8% of pregnant women met the minimum dietary diversity for women (MDD-W) in low- and middle-income countries due to inadequate nutritional intake or low supplementation during pregnancy.14,15 Poor maternal micronutrient consumption is associated with preterm delivery, low birth weight, birth defects, small for gestational age neonates, visual complications (vitamin A), intracranial hemorrhage, neurological developmental impairment (vitamin B-12), neural tube defects (folate), and spontaneous abortion. 16
To encounter malnutrition disorders, and micronutrient supplementation, the World Health Organization (WHO) set a strong recommendation on food category accreditation and paid special attention to micronutrient supplementation in pregnant women.4,17 However, a micronutrient supplementation strategy is impossible in poor and middle-income countries. The food and agriculture organization of the United Nations (FAO) developed the minimum dietary diversity for reproductive-aged women (MDD-W) as a guide for the measurement of micronutrient adequacy to overcome the above problems. 18
The MDD-W for pregnant women was studied in a few northern and southeastern Ethiopians, and the result was between 19.5% and 44.8%.19,20 The gaps in these studies were the use of the open recall method, measurement differences (9 vs 10 food categories), and exclusion of first-trimester pregnant women. The MDD-W results in previous studies were associated with information about pregnancy nutrition, pregnancy nutrition awareness, and family size20,21 without using standard data collection tools, and measuring the nutritional status of the pregnant women. This study was conducted to address the comprehensive minimum dietary diversity of a pregnant woman and its associated factors at the Arba Minch Health and Demographic Surveillance Site, Southern Ethiopia.
Method
Study Setting and Study Period
A community-based cross-sectional study was conducted from December 19, 2021, to October 30, 2022, in the Arba Minch HDSS kebeles. There are 31 kebeles (the smallest administrative unit of Ethiopia) surrounding the Arba Minch town, among which 9 kebeles are used as a target of Arba Minch HDSS which is run by Arba Minch University. The kebeles are found approximately 500 to 650 km south of Addis Ababa. According to the HDSS report the total number of females aged 15 to 49 years in the 9 kebeles was 18 642 in 2021.
Source Population and Study Population
All pregnant women living in the Arba Minch HDSS were the source population while randomly selected pregnant women in the 9 kebeles of the Arba Minch HDSS were the study population. Pregnant women were not excluded from this study.
Sample Size Determination and Sampling Procedures
Different sample size determination technique was applied to get the highest sample size for this study; out of the different techniques, single population proportion formula for a cross-sectional study gave the highest sample size of 635 pregnant women with the following assumptions 95% confidence interval (CI), 4% margin of error, 40.1% dietary diversity practice report from Gonder town, 22 and adding 10% for nonresponse rate.
There were a total of 8221 pregnant women found in Arba Minch HDSS kebele obtained from the health postfamily folder by the aids of the health extension workers in each kebele: The study sample size was proportionally allocated based on each kebeles share [(Chano Chalba (778/60), Zigiti Mer (974/75), GentaMey (376/29), Kolla Shara (1385/107), ZeyseDem (751/58), Kolla Shelle 1217/94, ShelleMella (919/71), Gatse (1127/87), Laka (712/55)]. A simple random sampling procedure was applied to obtain each study participant using the households code.
Study Variables
Dependent Variable
Minimum Dietary diversity of pregnant women.
Independent Variables
Sociodemographic characteristics: age of the women, marital status, and educational status.
Reproductive and obstetric history: parity, home delivery history, gravidity.
Health service utilization status of a pregnant woman: ANC visit, pregnancy immunization (TT vaccine), and deworming
Information about nutrition
Pregnancy Nutrition awareness
Household food insecurity access scale
Operational Definitions
Data Collection Tool and Procedure
A semi-structured data collection questionnaire was prepared in English after reviewing the literature on the study topics.20,26,27 The questionnaire has 7 parts; sociodemographic characteristics, Reproductive and Health service utilization, Information about pregnancy nutrition, and pregnancy nutritional awareness. MDD-W is a dichotomous indicator of whether a pregnant woman consumed 05 out of the 10 food categories. 18 The data collection tool also includes the Household Food Insecurity Access Scale (HFIAS) assessment. 24 Family income was assessed according to available household assets. 28 Finally, the nutritional status was assessed by measuring the mid-upper-arm-circumference (MUAC) of a pregnant woman. Data were collected using a face-to-face interviewer-administered technique, and MUAC measurements. Open data kit software was used to collect the data, and the Arba Minch HDSS server was used to store, receive, and send the data. The data were collected by 9 trained BSc degree midwives and supervised by 5 MSc degree holders.
Data Quality Control
The data quality was maintained by a pre-test conducted on 5% of the sample size in 3 kebeles that are not involved in Arba Minch HDSS Kebeles: Both the data collectors and the supervisors took a 4-day training about the study aim, research ethics, the electronic data collection procedure, and the techniques of interviewing on the sensitive issues such as food security questions: The use of an open data kit for data collection to avoid missing data. The data collection process was supervised.
Data Processing and Analysis
The collected data were exported to Excel and Statistical Package for Social Sciences version 25.0. Simple frequencies, crosstabs, and ranges along with the median were used to describe the study participants’ character. The information is presented using text, figures, and tables. The independent variable household wealth index was constructed using principal component analysis by considering the 27 available household assets and categorized as “0” for not available assets and “1” for the available asset. The KMO and Bartlett's test sphericities were checked and found to be 0.823, and a P-value of .000, respectively. A multicollinearity test was performed, and the variance inflation factor was less than 3. Binary logistic regression was used to determine the associated factors with MDD-W. Variables with a P-value of < .25 in bivariate logistic regression were considered in the multivariable logistic regression analysis. Hosmer-Lemeshow model fitness tests were performed. Variables with a P-value < .05 along with 95% CI, and adjusted odds ratio (AOR) were declared as associated factors.
Ethical Considerations
Ethical approval was obtained from the Arba Minch University College of Medicine and Health Sciences, Institutional Review Board (IRB) with IRB reference number IRB/1127/2021. Permission was secured from the respective Arba Minch HDSS kebele administrative office. After a brief explanation of the study's purpose, written, informed consent was obtained from each study participant; For those participants below 18 years old assent and consent were obtained from her and her husband, respectively. In the case of respondents who could not read, and write; an eye witness who did not participate in the study signed parallel to her fingerprint. The participants’ information confidentiality was maintained by providing special codes throughout the study period. The COVID-19 protection precautions were maintained.
Results
Socio-Demographic and Economic Characteristics of a Pregnant Woman
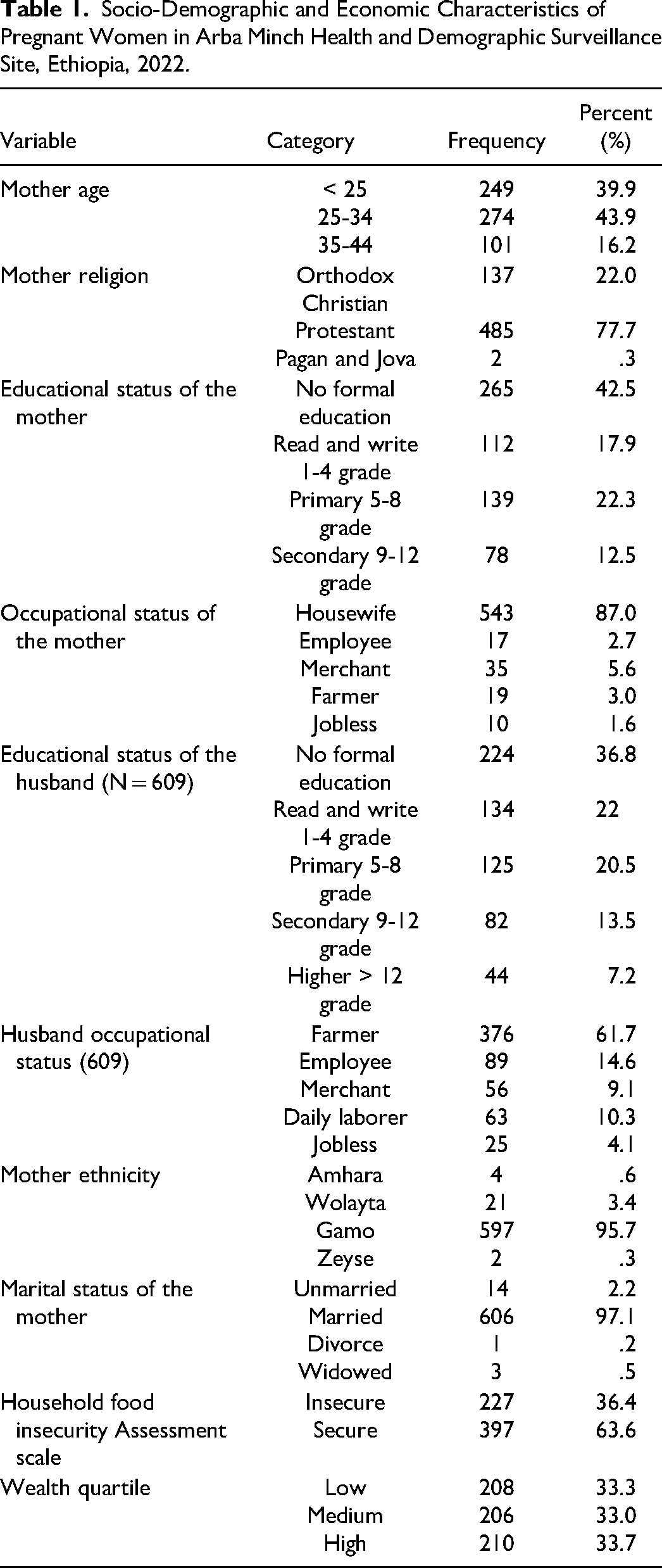
Out of 635 sampled pregnant women 624 gave a response to this survey, making a response rate of 98.2%. One-fourth of the pregnant women were between the age of 34 to 44 years old. A significant number of pregnant women were married 606 (97.1%). Most, 543 (87%) of the pregnant women in this study were housewives in addition to this 78 (12.5%) of them were completed secondary and above educational level. Regarding the husband's educational status majority, 224 (36.8%) of them did not have formal education. More than two-thirds of respondents’ husbands were farmers. The majority, 397 (63.7%) of the households were food-secured, and one-third, 210 (33.7%) of the households fell under the high wealth quartile (Table 1).
Socio-Demographic and Economic Characteristics of Pregnant Women in Arba Minch Health and Demographic Surveillance Site, Ethiopia, 2022.
Reproductive and Health Service Utilization Status of Pregnant Woman
Among the 624 pregnant mothers, only 95 (15.2%) were primigravidas, and nearly half of the multiparous women involved in this study had a history of home delivery (257/529). Most, 379 (60.7%) pregnant women had ANC follow-ups for the current pregnancy, and among these 61 had 4 or more ANC follow-ups. Nearly half of the households had 2 to 4 children. Approximately one-third of the pregnant women were dewormed, and 48.4% (302) received tetanus toxoid vaccination during their current pregnancy.
Minimum Dietary Diversity and Extra Meal Consumption of Pregnant Women
In this study more than half, 53.3% (95% CI: 49-57) of the pregnant women achieved the MDD, and the mean dietary diversity score was 4.67 food items with a maximum of 10 and minimum of 01 food item consumption. The majority, 545 (87.3%) of the pregnant women consumed (grains, white roots, tubers, and plantains) food category within the last 24 h: followed by other vegetable food categories 471 (75.5%). Category 04 (meat, poultry, and fish) was the least consumed food category in this study 40 (6.4%). More than 60% (375) of the pregnant women did not establish extra meal time (Figure 1).

Frequency/percent distribution of food groups consumed by pregnant women in Arba Minch Health and Demographic Surveillance Site, Ethiopia, 2022.
Pregnancy Nutrition Awareness and Source of Information
The majority, 540 (86.5%) of the pregnant women were aware that food is necessary for the normal functioning of the body system. More than three-fourths, 492 (78.8%) of the pregnant women were aware of the importance of food for fetal wellbeing however, nearly a quarter of the pregnant women were aware that an unbalanced diet may lead to abortion. Less than half, 269 (43.1%) of the pregnant women in this study had no information about pregnancy nutrition, and approximately 44.7% (279), 27.1% (169), and 28.2% (176) of them had medium, low and high awareness regarding pregnancy nutrition, respectively.
Nutritional Status of Pregnant Women
Among the 624 pregnant women who participated in this study one-fourth, 151 (24.2%) of them were undernutrition. The minimum and maximum MUAC were 18 and 34 cm, respectively, with a median of 24.
Factors Associated With Minimum Dietary Diversity of Pregnant Women
The multivariable logistic regression analysis shows that the following independent variable is significantly associated with MDD-W in pregnant women: food-secured households (AOR = 0.55; 95% CI: 0.36, 0.83), meal frequency within 24 h (AOR = 1.62; 95% CI: 1.1, 2.5), tetanus toxoid vaccination during the current pregnancy (AOR = 1.78; 95% CI: 1.06, 2.9), deworming history of the women (AOR = 1.85; 95% CI: 1.14, 3), house ownership (AOR = 0.52; 95% CI: 0.29, 0.9), ownership of banana farm (AOR = 1.7; 95% CI: 1.02, 2.8), extra meals, (AOR = 0.51; 95% CI: .3, .8), ANC follow-up (AOR = 1.9; 95% CI: 1.1, 3.3), and merchant pregnant women (AOR = 6; 95%, CI: 2.1, 17.6) (Table 2).
Factors Associated With Minimum Dietary Diversity Among Pregnant Women in Arba Minch Health and Demographic Surveillance Site, Ethiopia, 2022.

Abbreviations: COR, crude odds ratios; AOR, adjusted odds ratios; MDDP, Minimum Dietary Diversity Among Pregnant Women.
** = Significance variables.
Discussion
In this study more than half, 53.3% (95% CI: 49, 57) of the pregnant women achieved the MDD-W. The finding of the current study is in line with the results from Southwest Ethiopia 51%, 29 Nepal, 55%, 30 and Cameroon, 53%. 31
The current study finding is lower than that finding in Pakistan 89%. 32 A possible reason might be the inclusion of all trimesters of pregnant women in the current study while the previous excluded, the economic inflation impact on food expenditures in the current study, 33 and the majority (87%) of the study participants in the current study were housewives. The current study is also lower than that study conducted in Addis Abeba, 60.90%, 34 Alamata General Hospital, Ethiopia, 61.2%, 35 Kenya, 61%, 36 Indonesia, 57.9%, 37 the discrepancy might be due to the socio-demographic variations such as rural residency in the current study, educational status difference and interventional effect in Adiss Abeba.
The current finding is higher than 9 similar Ethiopian studies, Dessie town, 45.2%, 38 west Gojam, 19.9%, 20 Gonder town, 40.1%, 22 Misha wereda, 29.5%, 27 Shahemene town, 25.4%, 39 Illu Babur, 34.5%, 40 Public Health Institution in Mizan-Aman Town 25.1%, 41 Bale zone, 44.8%, 42 and Dire Dawa, 43%. 19 The MDD-W in this study was also greater than that of studies conducted in Ghana 46.1% 43 and Kenya 20%. 44 The possible reasons might be demographic and cultural differences, as previous studies were conducted in areas where the habit of cultivating and consuming vegetables/fruits was low, 45 and cut-off point difference.
In this study, the odds of MDD-W were 45% less likely to be achieved among food-insecure pregnant women than among food-secured pregnant women. The possible agreement would be that a food-insecure pregnant woman might not have access to a variety of foods. This finding is similar to those reported in other areas, such as Raya Azebo, 35 West Gojam, 20 Gurage Zone studies, 46 and Mizan Aman hospital. 41
Pregnant women who consumed more than 3 times within 24 h and those who had established an extra meal time were more likely to achieve MDD-W than their counterparts. This is supported by east Gojam, and Raya Azebo: when meal frequency increased the likelihood of achieving MDD-W also increased.27,35,47 This is because a higher meal frequency increases the likelihood of avoiding the consumption of the same food item within 24 h.
Pregnant women who had ANC follow-up during the current pregnancy were nearly twice as likely to achieve MDD-W than pregnant women who had no ANC follow-up; this finding is supported by Adiss Abeba, Ethiopian study 34 ; Pregnant women who received tetanus toxoid vaccination and deworming during the current pregnancy were also twice as likely to achieve MDD-W. Counseling about a balanced diet, and nutritional supplementation is one part of the ANC care plan; therefore this might be the possible reason for pregnant women's MDD-W achievement.
Pregnant women who had no private houses were 48% less likely to eat 5 or more food items within 24 h than their counterparts. This finding agrees with the finding from Kenya, 48 the reason behind this might be that individuals without house ownership might lead unstable life spending extra money on a house.
Merchant Pregnant women were 6 times more likely to feed 5 or more food items than housewife pregnant women and this finding is supported by one Ethiopian study, Raya Azebo. 35 The possible reasons might be that merchant pregnant women have the chance to access food items from the market and the nature of merchant occupation is also related to the tendency to access different nutritional information.
Pregnant women who owned banana farms were nearly twice as likely to attain MDD-W. This finding is supported by other studies.22,27,41,49,50 Selling bananas for the rest of the Ethiopian region in the study area is a common agricultural train. Due to the high income generated by banana farms; people's living standards are better. Thus, pregnant women may have access to a variety of food items.
Conclusion and Reccomondations
Conclusion
In this study, 53.3% of the pregnant women achieved the minimum dietary diversity for reproductive-aged women to measure micronutrient adequacy. The outcome of this study was higher than that of other studies. However, this finding is low because pregnant women need adequate energy and micronutrient-rich food items. The minimum dietary diversity for pregnant women in this study was associated with health service utilization such as ANC follow-up, deworming, tetanus toxoid vaccination, eating > 3 times per day, establishing extra meal time for the pregnancy, securing food, owning a private house, ownership of the banana farm, and pregnant women's merchant occupation.
Recommendation
The Arba Minch HDSS office in collaboration with the Arba Minch surrounding wereda administrative might need to work together to improve the minimum dietary diversity among housewives, increase the ANC visit coverage, and provide continuous professional advice about the advantages of increased meal frequency during pregnancy. In addition, micronutrient supplementation, increasing availability, and production capacity of food-insecure households are expected from stakeholders. It would be better if other researchers in this field conducted qualitative studies.
Strengths and Limitations of the Study
This study has the following strengths; food item categorization error was avoided, and recall bias was minimized due to the use of a list-based technique. The study also investigates a major public health concern; the nutritional status of pregnant women in the study area at the same time. However, the study has limitations such as a lack of qualitative data supplementation; the outcome of this study might be influenced by seasonal variation and different occasions, such as religious festivals because this study used a single 24-h dietary recall method.
Footnotes
Acronym and Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.