
Abstract
Objective:
The objective of this study was to examine the association of patient- and county-level factors with the emergency department (ED) visits among adult fee-for-service (FFS) Medicaid beneficiaries residing in Maryland, Ohio, and West Virginia.
Methods:
A cross-sectional design using retrospective observational data was implemented. Patient-level data were obtained from 2010 Medicaid Analytic eXtract files. Information on county-level health-care resources was obtained from the Area Health Resource file and County Health Rankings file.
Results:
In adjusted analyses, the following patient-level factors were associated with higher number of ED visits: African Americans (incidence rate ratios [IRR] = 1.47), Hispanics (IRR = 1.63), polypharmacy (IRR = 1.89), and tobacco use (IRR = 2.23). Patients with complex chronic illness had a higher number of ED visits (IRR = 3.33). The county-level factors associated with ED visits were unemployment rate (IRR = 0.94) and number of urgent care clinics (IRR = 0.96).
Conclusion:
Patients with complex healthcare needs had a higher number of ED visits as compared to those without complex healthcare needs. The study results provide important baseline context for future policy analysis studies around Medicaid expansion options.
Introduction
The Center for Disease Control and Prevention estimated 91.1 million visits to the emergency department (ED) in 2010 among adults aged 18 to 64 years. 1 Emergency Department visits for health care are a major concern because a majority of these visits are for the care of ambulatory care sensitive conditions (ACSCs) and can be prevented with timely primary care. 2 Emergency Department visits for ACSCs impose significant economic burden compared to other outpatient settings. 3,4 Emergency department visits due to ACSCs account for US$38 billion of total health-care spending in the United States. 5
There is a common misperception that almost all ED users who have preventable conditions or are frequent ED users are uninsured. 6 Emergency department users often have health insurance including Medicaid or Medicare. 6,7 Emergency department visits by Medicaid beneficiaries accounted for about 12% of the total health-care spending on ED services in 2012. 8
Emergency department use among Medicaid beneficiaries has received considerable attention due to expanding Medicaid eligibility in 31 states. As there is some evidence of an inverse relationship between ED visits and community-level supply of primary care providers and health centers, 9 it could be hypothesized that providing health insurance coverage to the uninsured without corresponding increases in primary care availability may lead to increased ED visits for nonemergent care. However, published literature reveals mixed findings. Some investigations have found little or no change in the ED utilization after provision of insurance coverage to the uninsured, 10,11 while others found that the Medicaid expansion significantly increased both preventable and nonpreventable ED utilization. 12 These studies have limited ability to provide conclusive evidence because they did not include a systematic adjustment for a comprehensive set of patient- and county-level factors.
The primary objective of the current study is to use patient-level administrative claims data to examine the association between the patient- and county-level factors and the ED visits. For the purposes of the study, data on ED visits by adult, fee-for-service (FFS) Medicaid beneficiaries residing in Maryland, Ohio, and West Virginia were selected. These states were chosen as part of a long-term plan to investigate differences between the impact of the Medicaid Expansion (Ohio did not immediately expand, while the other states did) and the Health Insurance Marketplace (Maryland created a state-based marketplace, Ohio a federally facilitated marketplace, and West Virginia a partnership model marketplace). All states have many subtle differences within their Medicaid programs and benefits, as well, which can be compared easily through the Kaiser Family Foundation’s online database. 13 Andersen’s behavioral model (ABM) for health-care services usage was adopted to provide a conceptual framework for the study. 14 The ABM model posits that the health-care services utilization (ED visits in the current study) can be influenced by predisposing, enabling, need, external environment factors, and personal health practices as explained in the measures section.
Methods
Study Design
This study used a retrospective cross-sectional design with observational data.
Data Sources
Medicaid Analytic Extract (MAX) Files-2010
MAX files are prepared and released by The Centers of Medicare and Medicaid in assistance with Research Data Assistance Center. These files include (1) personal summary, (2) inpatient claims, (3) other therapy claims, and (4) prescription drugs claims. The current study used data on Medicaid beneficiaries residing in Maryland, Ohio, and West Virginia.
Area Health Resources Files (AHRF)
The Area Health Resources Files contain national-, state-, and county-level data on approximately 6000 variables. 15
County Health Rankings Data
The County Health Rankings data provides information on health behaviors, clinical care, social and economic factors, and physical environment for all counties in all states. 16 This information is compiled from 50 different data sources.
Study Population
The inclusion criteria were: FFS Medicaid beneficiaries, aged 22 to 64 years, with continuous Medicaid enrollment, not eligible for Medicare, and alive during the entire observation period. Pregnant women were excluded from the analysis because they may have unique prenatal needs (N = 68 882).
Dependent Variable
Number of ED visits
Emergency department visits were identified from inpatient and outpatient claims. To identify ED visits from the outpatient claims, CPT codes (99281-85) were used. Emergency department visits from the inpatient claims were identified using revenue codes (450-52, 456, 459, and 981).
Independent variables
Predisposing factors were age, gender, and race/ethnicity. Enabling factors were patient-level Medicaid eligibility due to cash assistance/poverty (cash eligibility, no cash eligibility), county-level college education rate, primary care use (none, fragmented, continuous), and county-level unemployment rate. Primary care use was measured using the modified, modified continuity index (MMCI) developed by Magill and Senf, 17 which ranged from 0 to 1. The MMCI was developed to solve limitations of the Usual Provider of Care and modified continuity index.
Need factors were patient-level complex chronic illness (physical health conditions, mental health conditions, physical and mental health conditions, none), Medicaid eligibility due to medical need/waiver, and polypharmacy (Yes, No). Polypharmacy was defined as concomitant use of multiple prescription drugs within a 90-day period and was based on number of prescription drugs 1 standard deviation above the mean. 18 In this study, complex chronic illness was defined as those having both physical and mental health conditions. The selection of physical and mental health conditions was based on the framework provided by the Health and Human Services Office of the Assistant Secretary of Health. 19 Both physical and mental health conditions were identified if patients had an inpatient or outpatient claim. Personal health practices were patient-level tobacco use (clinically coded into the Medicaid data) and county-level obesity rates.
External environment factors were measured at the county-level and included metro status, health professional shortage area (HPSA—no, partial, and complete shortage areas), number of hospitals with EDs, number of hospitals with psychiatric emergency services, number of rural health clinics, number of federally qualified health centers (FQHCs), number of community mental health centers, and number of urgent care clinics per 100 000 population.
Statistical Analysis
Frequencies were used to describe the characteristics of the study population. Mean, interquartile range (IQR), and 90th percentile were used to describe the frequency of ED visits. The frequency of ED visits can be analyzed using a variety of count data regression models. They include Poisson regression, negative binomial regression (NBR), zero inflated Poisson regression (ZIP), and zero inflated NBR (ZINB). After comparing the predicted and actual probabilities, and log likelihood from all 4 statistical models, NBR and ZINB models were deemed appropriate. The ZINB model is complex and difficult to interpret due to its 2-part structure, and many economists and statisticians discourage using ZINB models when NBR models fit well with the data. 20 Therefore, this study used both unadjusted and adjusted NBR models to examine the patient- and county-level factors associated with the number of ED visits.
The adjusted NBR models included predisposing, enabling, need, external environment factors, and personal health practices. The parameter estimates from the NBR models were converted to incidence rate ratios (IRRs) by exponentiating the regression coefficients, and 95% confidence intervals were estimated. Incidence rate ratio can be interpreted as the percent change in ED visits. Incidence rate ratio above 1.0 implies higher number of ED visits and IRR below 1.0 implies lower number of ED visits. The data consisted of all counties in Maryland, Ohio, and West Virginia (167) and patients nested within these counties. Therefore, the NBR models were adjusted for clustering due to counties using STATA version 14.
Results
During 2010, 46% of the study population had zero ED visits. Around, 36% beneficiaries had ≤3 ED visits, 14% had 4 to 9 ED visits, and remaining 4% had 10 or more ED visits. Table 1 summarizes the patient-level characteristics of the study population. The majority were females (56.2%), older adults aged 45 to 64 (58.1%), whites (85.3%), were eligible for Medicaid through cash assistance/poverty (81.4%), lived in counties designated as either whole/part county HPSA (79.5%), and had fragmented/no primary care use (89.4%). In all, 18% had polypharmacy and 38% had both physical and mental health conditions. About 6.6% of the study population were tobacco users.
Description of the Study Population by Patient-Level Factors Adult Fee-for-Service Medicaid Beneficiaries Multistate Medicaid Analytical eXtract Files-2010.a

aBased on 68 882 adult Medicaid fee-for-service beneficiaries aged 22 to 64 years and who are continuously enrolled for the year 2010, who are not Medicare and Medicaid eligible, who are alive and non-pregnant. County-level variables were extracted from the Area Health Resource Files and county health ranking data.
The following were the range of county-level factors: college education rate 4% to 42%, unemployment rate 2.7% to 10.5%, obesity rate 18.8% to 35.7%, number of hospitals with psychiatric emergency services/100 000 population 0 to 5.9, number of EDs/100 000 population 0 to 13.1, number of rural health clinics/100 000 population 0 to 32.9, number of urgent care centers/100 000 population 0 to 13.1, number of FQHCs/100 000 population 0 to 64.1, and number of community mental health centers/100 000 population 0 to 3.6.
Overall, the mean number of ED visits were 2 with an IQR of 0-2. Nearly, 10% of the study population had 6 or more ED visits. The frequencies of ED visits for each subgroup are presented as well. The unadjusted NBRs revealed that many subgroups of the population had higher number of ED visits: adults in the age-group 35 to 44 (IRR = 1.25) and 45 to 54 (IRR = 1.22) years; African Americans (IRR = 1.46); Medicaid eligibility due to poverty/cash assistance (IRR = 1.35); college education rate (IRR = 1.02); fragmented primary care use (IRR = 1.55); polypharmacy (IRR = 2.10); presence of physical health conditions (IRR = 2.46); presence of mental health conditions (IRR = 1.69); presence of both physical and mental health conditions (IRR = 4.23); Medicaid eligibility due to medical needs (IRR = 1.35); tobacco use (IRR = 2.54); and number of hospitals with psychiatric emergency services (IRR = 1.21). Some subgroups of the population had lower number of ED visits: female (IRR = 0.08); obesity rate (IRR = 0.95); nonmetro status (IRR = 0.81); number of rural health centers (IRR = 0.99); and number of FQHCs (IRR = 0.99). No associations were observed between ED visits and the following factors: those aged 55 to 64 years old; unemployment rate; no primary care use; no/partial county HPSA; number of hospitals with EDs; number of urgent care centers; and number of community mental health centers.
The IRRs and 95% confidence intervals from the adjusted NBR are summarized in Table 2. The relationship between ED visits and the following factors remained the same as observed in the unadjusted NBR models: females, African Americans, no medical eligibility, fragmented primary care use, polypharmacy, and presence of complex chronic illness. For example, those with polypharmacy had higher number of ED visits (IRR = 1.89) when compared to those individuals without polypharmacy. However, the association between ED visits and the following factors changed: age-group 45 to 54 (IRR = 0.78), and 55 to 64 (IRR = 0.66); unemployment rate (IRR = 0.94); no primary care use (IRR = 0.92); and number of urgent care centers (IRR = 0.96). No associations were observed between ED visits and the following factors: 35 to 44 years old, Medicaid eligibility due to poverty, college education rate, obesity rate, no/partial HPSA, nonmetro status of the county, number of hospitals with psychiatric emergency services, number of rural health centers, number of FQHCs, and number of community mental health centers.
Incidence Rate Ratios and 95% Confidence Intervals (CIs) From Multivariable Negative Binomial Regression of Adult Fee-for-Service Medicaid Beneficiaries Multistate Medicaid Analytical eXtract Files-2010.a
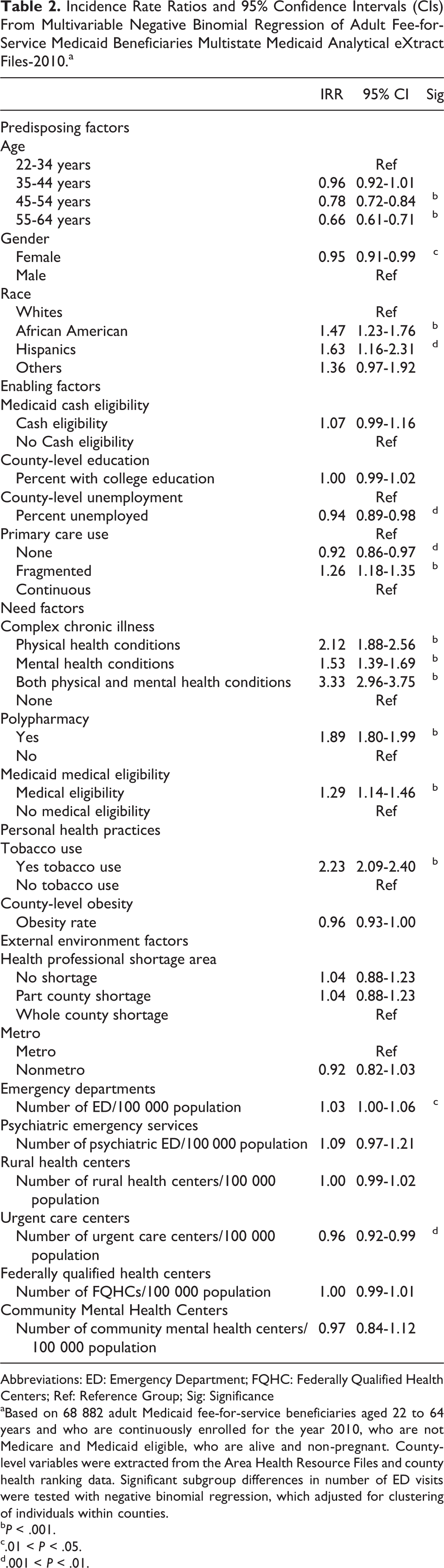
Abbreviations: ED: Emergency Department; FQHC: Federally Qualified Health Centers; Ref: Reference Group; Sig: Significance
aBased on 68 882 adult Medicaid fee-for-service beneficiaries aged 22 to 64 years and who are continuously enrolled for the year 2010, who are not Medicare and Medicaid eligible, who are alive and non-pregnant. County-level variables were extracted from the Area Health Resource Files and county health ranking data. Significant subgroup differences in number of ED visits were tested with negative binomial regression, which adjusted for clustering of individuals within counties.
b P < .001.
c.01 < P < .05.
d.001 < P < .01.
Discussion
The study findings revealed that a number of patient-level and few county-level factors were associated with the ED visits among adult FFS Medicaid beneficiaries. Among predisposing factors, the current study observed that African Americans and Hispanics had a higher number of ED visits when compared to whites. The findings on racial/ethnic disparities are consistent with the published literature on ED usage. 9,21
Among the enabling factors, county-level unemployment rate and primary care use were associated with the number of ED visits. A counterintuitive finding of this study is the inverse relationship between county-level unemployment rate and number of ED visits. The reasons behind lower number of ED visits by individuals living in counties with high unemployment rate are not known.
Findings from the current study support the published literature in which primary care use is inversely related to ED visits. 22 Medicaid beneficiaries with fragmented primary care use had higher number of ED visits when compared to those with primary care continuity. These findings suggest that timely and continuous primary care in outpatient health-care settings can reduce the frequency of ED visits among adult FFS Medicaid beneficiaries. When primary care use is fragmented, the patient may choose to use ED for nonemergency services. It has been documented that individuals without adequate primary care may delay receiving appropriate care, 23 which may in turn lead to increased use of ED.
All the need factors were associated with higher number of ED visits. Adult FFS Medicaid beneficiaries with complex needs had a higher number of ED visits. This finding is consistent with prior studies in which ED users were found to have high medical needs, 24 -29 have chronic conditions, 30 suffer from mental illnesses, 31 -38 and have greater number of psychotropic medications. 39 A plausible explanation for higher ED visits by those with chronic complex illness may be due to complications of chronic conditions, side effects, and adverse events due to multiple medications use, 40 fragmented care because of visits to multiple providers, and/or direct contraindications to therapy for one condition by other conditions themselves. 41
Among personal health practices, individuals with tobacco use had a higher number of ED visits when compared to those without tobacco use. Future research may examine whether EDs can serve as appropriate health-care settings for the provision of smoking cessation interventions. Indeed, the results from a recently published randomized controlled trial revealed that a smoking cessation intervention offered in an ED declined smoking rates among low-income smokers significantly. 42 It is plausible that ED users have limited access to other health-care providers who can encourage them to quit tobacco use.
Some county-level external environment factors were associated with ED visits among adult FFS Medicaid beneficiaries. For example, this study noted that with higher number of urgent care centers significantly lower number of ED visits were observed. This finding is consistent with another study by Weinick et al that observed about 13.1% to 27.1% of ED visits can be prevented with increased use of urgent care centers and other health-care settings. 43 Studies that have compared urgent care and ED care have found that costs of care in urgent care centers are lower when compared to EDs. 3,4
Limitations
Considering the geographic population, policy, and resource differences typically seen across states, the results of this study represent only Maryland, Ohio, and West Virginia and not generalizable to the entire Medicaid population. As Medicaid beneficiaries enrolled under managed care plans were excluded from the analytical cohort, the study suffers selection bias. The study was conducted using observational data,; therefore, it is difficult to account for selection bias, as ED users may have different attributes in unobserved variables compared to the non-ED users. The cross-sectional design of the study does not allow causal inferences. As all the independent variables were measured in the same as year as the outcome variable, temporal relationships cannot be established. Substance abuse leads to increased ED use; however, the current study could not account for alcohol use and drug abuse because of limited sample size. Additionally, administrative claims data were used, which are created for billing purposes rather than research. This may result in misclassification of diagnosis.
Conclusion
To conclude, the study is timely because many states have surveillance and other research projects to monitor the use of ED by Medicaid beneficiaries and are exploring policies and programs that can reduce preventable ED visits. 44 The current study highlighted that only very few county-level factors and many patient-level factors were associated with ED visits. These findings suggest that health-care delivery models that provide comprehensive care to complex patients may reduce the likelihood of ED visits. Implementing value-based insurance designs that provide financial incentives to promote primary care continuity may go a long way in reducing ED visits among adult FFS Medicaid beneficiaries. Our study also indicates urgent care centers may be a viable substitute for EDs in providing care for acute conditions and exacerbations of chronic conditions. Future studies need to examine whether the emerging healthcare delivery models such as medical homes, and accountable care organizations (ACO), which are specifically designed to take care of complex patients, can reduce the number of ED visits by the complex patients. Medicaid ACO demonstration projects, for example, may provide evidence about whether the new delivery models can reduce the use of ED as well as the relationship between individual-level unemployment, poverty, and ED visits.
This study provides important baseline information on Medicaid ED usage and the county- and individual-level factors driving the number of visits. As data become available, it is expected that many studies will attempt to compare and contrast ED utilization among different states who chose various policy options related to Medicaid and the Health Insurance Marketplace. Our model presents a starting point and baseline data from which to begin that exploration.
Footnotes
Authors’ Note
Data acquisition was made possible by funding from Claude Worthington Benedum Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or policy or position of West Virginia University (WVU) or any other affiliated organizations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SM and US were partially supported by the National Institute of General Medical Sciences, U54GM104942.