
Abstract
Objective
To describe characteristics of a nationally representative sample of patient visits that ended with a referral for follow-up medical care after discharge from hospital emergency department (ED) visits.
Methods
We used 2018 National Hospital Ambulatory Medical Care Survey data to identify patient characteristics associated with higher rates of visits with referrals for follow-up medical care after ED discharge from nonfederal short-stay and general hospitals throughout the United States. Referral included categories of all disposition variables that indicated referral to a source of care consistent with the patient’s clinical condition at ED discharge.
Results
Approximately 97 million of 130 million visits (29 700/100 000 US resident population) were referred for follow-up medical care during 2018. Visit referral rates were higher among females (33 100) than among males (26 300/100 000 population); higher among Black patients (61 700) than among White patients (25 600/100 000 population); highest in the South (33 200/100 000 population); and similar rates in Nonmetropolitan (29 900/100 000 population) and Metropolitan Statistical Areas (30 200/100 000 population). Visit referral rates were higher for patients with Medicaid/Children's Health Insurance Program (CHIP) (66 900) than those with Medicare (31 500) or private insurance (14 000/100 000 population). Abnormal clinical findings and injuries were the discharge diagnoses most often referred for follow-up medical care.
Conclusion
Higher visit referral rates were observed among female sex, non-Hispanic Black race, Medicaid/CHIP, abnormal clinical findings, and injuries. Future studies might reveal reasons that prompted higher referral rates among various patients’ characteristics.
Keywords
During 2018, approximately 130 million visits were made to hospital emergency departments (EDs), 1 representing an increase of 11% from 2007 ED visits. 2 ED visits have increased consistently, and the characteristics of patients with high rates of ED use for primary health care services have not changed (eg, Medicaid recipients, Medicare recipients, older persons, and non-Hispanic Black patients).1,2 Although concerns with ED overcrowding and associated excess costs continue to dominate health care delivery and policy debates,3,4 the Affordable Care Act has begun to alleviate certain problems.5,6 Published reports demonstrate that unnecessary ED visits can be reduced drastically among frequent users and pediatric patients when such visits are followed by receipt of social services outside the ED,3,7,8 thus alleviating unnecessary ED visits. Although US ED visits focus on alleviating emergency medical concerns, such visits also present opportunities for addressing vital social care needs of the served community. 9 Because the majority of patients who receive primary care services from EDs have insurance coverage, researchers have recommended that shifting those services out of EDs can reduce the volume of unnecessary ED visits by providing better and more accessible primary care to which ED patients are referred. 10
Medical providers working with community-based organizations have successfully delivered medical and social services to populations who experience risk for disease acquisition and transmission. 11 By addressing nonmedical needs of these patients, unnecessary ED visits might be decreased. 12 Published research results indicate economic benefits when social service referrals are incorporated into ED care 13 because persons who repeatedly use EDs often have social, substance abuse, or mental health problems that worsen their chronic illness. 14 Although certain factors (eg, patient age, race/ethnicity, diagnosis, health condition, availability of primary care provider, health insurance, income, homelessness, and resources) influence patient disposition and referral at the end of an ED visit,15-17 one public health goal is achieving the best possible outcome for each patient and the patient’s community. ED visits will continue to be vital in our health care delivery system. Optimal disposition of ED visits and referral for follow-up medical care are shared interests of patients, government officials, and health insurance companies because of population growth, hospital readmissions, maximizing clinical care, racial/ethnic disparities in care and outcomes, and ED overcrowding.16,18-21 We describe characteristics of patients and ED visits that result in referral for follow-up medical care in a nationally representative sample of ED visits by age group, sex, race/ethnicity, US geographic region, insurance payment type, and diagnosis, and we highlight inequalities by population group.
Methods
Study Sample
The National Hospital Ambulatory Medical Care Survey
In the 2018 survey, 490 hospitals were selected for the survey; 112 of those hospitals were determined to be ineligible; 378 hospitals were eligible; and 323 of the eligible hospitals eventually participated, for a response rate of 85.5% (unweighted) and 88.5% (weighted) (see ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHAMCS). At each sampled ED, staff were asked to complete encounter forms for a systematic random sample of patient visits occurring during a randomly assigned 4-week reporting period. Forms might also be abstracted by the field representative. Five or fewer reasons for an ED visit could be reported (ie, complaints or symptoms), preferably by using the patient’s own words.
Measured Patient and Visit Attributes
On the patient record form, the attending physician’s primary diagnosis is usually the most important item that reflects the provider’s best judgment at the time of visit. NHAMCS-ED has 5 diagnosis fields. Referral for follow-up visits are forms of visit disposition and reflects where the patient went after leaving the ED. For example, a patient might (a) require no additional follow-up, (b) be asked to return to the ED, (c) left before the completion of a treatment, (d) left without being seen, (e) be admitted to the hospital or intensive care unit, (f) be transferred to another facility, (g) be dead on arrival or die in the ED, (h) be admitted to the observation unit then discharged, (i) be admitted to the observation unit then hospitalized, (j) be transferred to a psychiatric hospital, or (k) be transferred to a nursing home. Sixteen disposition options are available on the survey form, 8 of which support follow-up referral visits. We selected all visits for which follow-up referrals were indicated by 1 = Yes for that disposition code. The primary diagnosis codes for visits with these referral follow-up codes were indicated by major International Classification of Diseases, 10th Revision (ICD-10) categories (eg, certain infectious diseases, blood disorders, neoplasm, eye and adnexa diseases, musculoskeletal system, or respiratory diseases). 22 The expected source of payment (PAYTYPER) is based on hierarchical recode by using the hierarchy payment of Medicare, Medicaid/Children's Health Insurance Program (CHIP) (or other state-based program), private insurance, worker’s compensation, self-pay, no charge/charity, other, and unknown. (A special request was made to obtain relevant denominators for calculating referral rates for payment type from the National Center for Health Statistics.)
Statistical Analysis
We analyzed the data by using SAS version 9.4 procedures designed for NHAMCS’s complex sample design. We restricted our analysis to visits paid for by private insurance, Medicare, or Medicaid. All other payment options were grouped as Other (eg, self-pay, no charge, or worker’s compensation). We calculated visit referral rates per 100 000 among the 2018 US resident population and 95% CI by age group, sex, race/ethnicity, Metropolitan Statistical Area (MSA), and census region. We examined the diagnosis type by age group and race/ethnicity. Estimates of the 2018 US population denominators for calculating visit rates were obtained from the US Census Bureau. Regarding hospital EDs, a visit is defined as a direct contact with a physician or a staff member acting under the direction of a physician for the purpose of seeking care and rendering health services. Data are weighted to generate US national estimates from the complex survey design.
Results
The sample of 20 291 completed patient record forms was from 378 hospital EDs, nested within 279 emergency service areas for response rates of 60.2% (weighted) and 57.3% (unweighted). The analytic sample of 15 518 ED visits represented an estimated 130 million ED visits 1 during 2018, of which 80% (approximately 97 million) were referred for medical follow-up after discharge. The rate of referral for follow-up medical care was 29 700 visits/100 000 US resident population during 2018 (Table 1). The highest referral rate was among those aged ≥75 years (36 400 visits/100 000 population), followed by those aged 0-14 years (33 000 visits/100 000 population). In 2018, female patients (33 100 visits/100 000 population) were referred more often for follow-up medical care after an ED visit than male patients (26 300 visits/100 000 populations). Approximately, half of the visits with referrals were made by non-Hispanic White patients, and the rate of referral for this population (25 600 visits/100 000 population) was less than half the referral rate for non-Hispanic Black persons (61 700 visits/100 000 population). Although referral rates by census region were similar, the highest referral rate was in the South (33 200 visits/100 000 population), followed by the Midwest (29 800 visits/100 000 population). The majority of those referred were from a MSA (87%), possibly reflecting the distribution and location of the sampled EDs. However, referral rates were similar for both MSA and non-MSA (30 200 vs 29, 900 visits/100 000 persons).
Number and Rates of Emergency Department Visits per 100 000 US Resident Population Among Patients who Were Referred for Follow-up Medical Care, by age, sex, Race/Ethnicity, US Census Region, MSA or Non-MSA and Insurance Payment Type, National Hospital Ambulatory Medical Care Survey—United States, 2018.
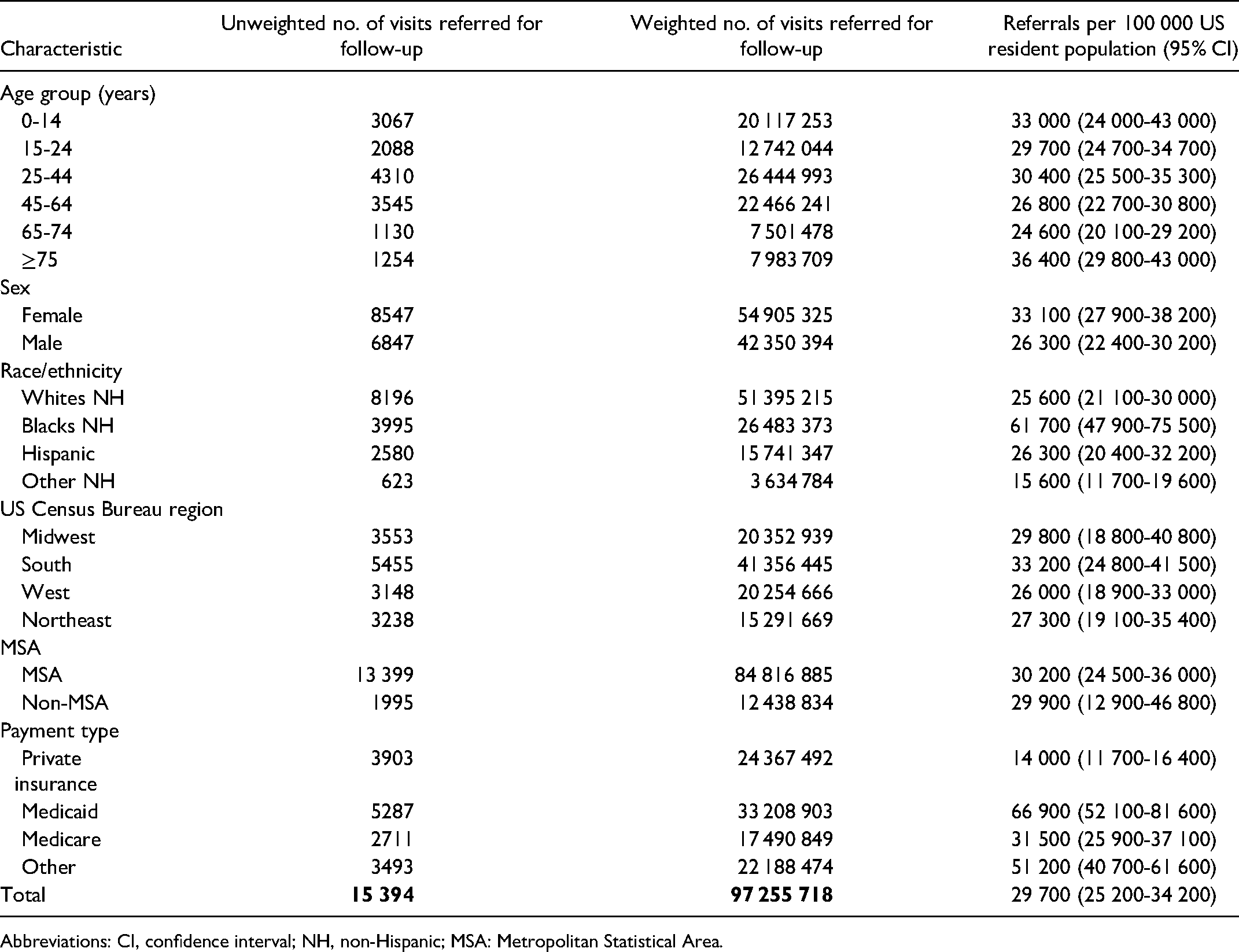
Abbreviations: CI, confidence interval; NH, non-Hispanic; MSA: Metropolitan Statistical Area.
Medicaid was the single most likely payment type for follow-up referrals (66 000/100 000 population), followed by Medicare and private insurance. Approximately one-quarter of referral visits were from abnormal clinical findings (estimated 25 233 579 visits), followed by injury, poisoning, and other external causes (approximately 18 802 244 visits) and respiratory system diseases (approximately 10 684 485 visits) (Table 2). Abnormal clinical findings and injuries were also the leading diagnoses by age group and race/ethnicity. Injury was the leading diagnosis for those aged ≤15 years. For White patients, Black patients, and all age groups (except ≤15 years), mental and behavioral disorders were among the 10 leading diagnoses. Infectious diseases were the fourth leading diagnosis among those aged ≤15 years (Appendixes A and B). The type of disposition recorded supports abnormal clinical findings where an estimated 90% of referrals were categorized as return or refer to a physician or clinic for follow-up services (Table 3).
Number and Percentage of Emergency Department Visits That Received a Referral for Follow-up Care, by Condition Diagnosis Category, National Hospital Ambulatory Medical Care Survey—United States, 2018.

Abbreviation: CI, confidence interval.
Number and Percentage of Emergency Department Visits Referred for Follow-up Medical Care by Type of Disposition, National Hospital Ambulatory Medical Care Survey—United States, 2018.

Abbreviation: CI, confidence interval.
Abnormal clinical findings represented a considerable proportion of referral visits. These were a conglomeration of ill-defined conditions for which no diagnosis could be assigned by the attending physician. Typically, these diagnoses are used when etiology is unknown, when a provisional diagnosis is made but the patient fails to return for further investigation or care, when a precise diagnosis is unavailable for any reason, when a case is referred elsewhere before the diagnosis is made, or when the patient presents with a transient condition at the initial encounter. 20 Because practical solutions for these problems are unknown, we examined injury visits for which practical approaches to prevention exist (Table 4). Referrals visit rates for injury were highest among persons aged 0-14 years (7887/100 000 population); among males (5867/100 000 population); among Black patients (9339/100 000 population); and in the South (6181/100 000 population). Nine of 10 follow-up referral visits for injury were from a MSA (approximately 16 million visits).
Number and Rates of Emergency Department Visits for Injuries That Received a Referral for Follow-up Medical Care by age, sex, Race/Ethnicity, US Census Region, and MSA or Non-MSA, National Hospital Ambulatory Medical Care Survey—United States, 2018.

Abbreviations: CI, confidence interval; NH, non-Hispanic; MSA: Metropolitan Statistical Area.
Discussion
Previous research examining ED visits demonstrated that unnecessary ED visits might be drastically reduced if primary care practices (eg, extended times for facility operation) are addressed apart from problems related to patient characteristics associated with unnecessary ED visits. 11 Increasing percentages of the US resident population among older age groups might explain why ED visits by persons aged ≥75 years accounted for the majority of visits with referrals. The concentration of chronic conditions (eg, diabetes or hypertension) that lead to recurring hospital ED visits in the South might explain higher rates of referral in this geographic region.23-25 A higher prevalence of chronic conditions, eg, diabetes, hypertension, and other conditions 26 may explain the higher referral rates among Black patients. Moreover, similar referral rates for MSA and non-MSA are reassuring. A closer examination through a chart review of abnormal clinical findings and their associated diagnostic codes is essential for understanding the causes of different referral rates by age, race/ethnicity, insurance payment type, and sex, including within-group differences.
Although millions of ED visits for infectious diseases occur annually, we do not know with certainty why so many visits are not referred for follow-up medical care; the following explanations are plausible, however. First, many infectious diseases cannot be definitively diagnosed during a short hospital ED visit. Second, vaccination, pre- and postexposure prophylaxis for certain infections (eg, HIV infection, hepatitis A and hepatitis B infection, or typhoid disease) are the focus of ED attention when persons who need these services are identified. 27 Tuberculosis (TB), a major infectious disease frequently first diagnosed in hospital EDs, has decreased substantially in the United States 28 because of concerted efforts at the national, state, and local levels. As a supplement to local health department efforts, screening patients for latent or active TB infection in hospital EDs and referring them for follow-up medical care can be effective in preventing reactivation of TB disease and infection transmission, thus further reducing TB incidence in the United States. 13 Menzies et al 29 also have identified higher risks for active TB and latent TB infection among non-US born US residents who immigrated from countries with a high incidence of active TB. Such patients can be screened for latent or active TB infection during hospital ED visits and referred for follow-up medical care to reduce TB incidence among US residents. 29 One advantage of the NHAMCS-ED is that its reliable and uniformly collected estimates can be used with confidence for addressing and monitoring such public health challenges as TB or HIV infection.
This analysis demonstrates that visits for injuries have higher referral rates for follow-up medical care, reflecting relative certainty of the diagnosis and need for follow-up medical care. Injuries remain a major public health concern in the United States. Modifiable health behaviors (eg, not wearing seat belts in cars or helmets when riding bicycles or motorcycles) and other behaviors that lead to motor vehicle or violence-related injuries (eg, texting while driving, driving while under the influence of alcohol or drugs, and gunshot or knife wounds) account for a substantial proportion of hospital ED visits. 30 ED physicians have opportunities for screening these patients for injury risk factors and for referring them to sources of preventive interventions. 31 A recent intervention linked young victims of interpersonal violence to sources of health care and social services for meeting their psychosocial needs. The associated study concluded that referral of young victims of violence from the ED for psychosocial services can be successful by using a case-management model and an alliance between a health care system and a social service agency. 32 Ensuring that ED practitioners identify patients who can benefit from follow-up counseling, behavioral interventions, and medical care after ED discharge is crucial.
Our study findings have at least 5 limitations. First, US national and regional estimates are not state-specific. However, states can use those estimates (eg, findings regarding injuries listed in Table 4) as proxy measures of racial/ethnic disparities within states with large numbers of minority populations. Second, NHAMCS does not contain information regarding the quality of hospital ED care, which is indicated in part by the patient’s satisfaction with ED and follow-up care and the care outcome that in turn depends on follow-up medical care received after ED discharge. This study is strictly descriptive and was not designed to include inferential statistics because follow-up medical care is a conglomeration of multiple referral options. As such, independent risk factors associated with all (combined) medical care follow-up referrals would be less informative and counterproductive in addressing this concern. Additionally, we did not examine comorbidities which could be important in referrals for certain population groups (eg, older adults, patients living in the South who may have higher chronic conditions, etc). Third, because we do not know the location of the particular EDs included in the sample analyzed, Black populations who had higher referral rates might have been disproportionately included; weighting should have reduced incompletely the salience of this limitation. Because non-Hispanic Black populations have higher ED visit rates than other population groups, 33 assuming that the same might be true for referrals is reasonable. Fourth, information abstracted must be identified in the record, but the quality of documentation cannot be determined by this study. Lastly, because visits with a second-, third-, fourth-, or fifth-listed diagnosis were not included in the sample analyzed, the estimates might be low.
Future studies should examine the reasons why visits in the South were referred for follow-up at higher rates overall and for injury-specific–related visits, compared with other regions. The majority of referrals were from MSA; therefore, because the economic benefit of social services for large hospitals is well-documented, 13 greater attention to strategies for reducing and preventing injuries is likely to provide positive results. Given the increasing importance of health information systems, linking referrals to enhance follow-up services is vital, including system evaluation. The majority of referrals are paid through Medicaid insurance or Medicare, which means that substantial populations are still relying solely on the government for their health care delivery. Nationally, Medicaid/CHIP and Medicare patients represent 52% of ED visits, 1 and the same percentage was referred for medical follow-up during 2018. However, the number of adults aged ≥65 years has increased, and a considerable percentage of those persons are still working. Traditionally, Medicare would be paying for the majority of those referrals, but apparently, older adults are prepared with financial tools and resources that are needed as the population ages. Many older persons continue to work, thus earning a living, including employer-supported health insurance, and are creating a new way of looking at the future (eg, financial freedom). In our study, private insurance represents approximately one-fourth of all referrals (approximately 24 367 492 during 2018), compared with Medicare (17 490 849 referrals). This major finding might also indicate that those who have private insurance are getting better care than the others who do not (ie, a disparity of health care among persons having private vs government care) have private insurance. Future research should examine any differences in patient referrals by health insurance type and the same discharge diagnosis. Lastly, because access to primary care providers is important in reducing ED visits, implications of the recent health care reform on ED visits should be examined. For example, expansion of the Community Health Centers might potentially reduce both social service referrals and ED visits because social services are incorporated in those centers’ operation. 34
Conclusion
Results of this study provide health care insurance companies, federal and state governments, and health policy officials with important statistics on referrals for follow-up medical care after ED discharge. Results indicate disparities in several patient characteristics. Because disposition of ED visits and referral for follow-up visits are shared public health interests, understanding the reasons for these disparities is crucial to maximize health outcomes. Partners, collaborators, and allies may use these estimates to design programs for the population who are disproportionately affected (eg, injury prevention).
Supplemental Material
sj-xls-1-hme-10.1177_23333928221111269 - Supplemental material for Characteristics of Emergency Department Patient Visits Referred for Follow-Up Medical Care After Discharge, National Hospital Ambulatory Medicare Care Survey—United States, 2018
Supplemental material, sj-xls-1-hme-10.1177_23333928221111269 for Characteristics of Emergency Department Patient Visits Referred for Follow-Up Medical Care After Discharge, National Hospital Ambulatory Medicare Care Survey—United States, 2018 by Nelson Adekoya, Henry Roberts and Benedict I. Truman in Health Services Research and Managerial Epidemiology
Supplemental Material
sj-xls-2-hme-10.1177_23333928221111269 - Supplemental material for Characteristics of Emergency Department Patient Visits Referred for Follow-Up Medical Care After Discharge, National Hospital Ambulatory Medicare Care Survey—United States, 2018
Supplemental material, sj-xls-2-hme-10.1177_23333928221111269 for Characteristics of Emergency Department Patient Visits Referred for Follow-Up Medical Care After Discharge, National Hospital Ambulatory Medicare Care Survey—United States, 2018 by Nelson Adekoya, Henry Roberts and Benedict I. Truman in Health Services Research and Managerial Epidemiology
Footnotes
Authors Note
The findings and conclusions in this report are those of the author and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Acknowledgments
The authors acknowledge the editorial support of C. Kay Smith. In addition, Christopher Cairns (CDC/NCHS) provided appropriate denominators and reviewed the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.