
Abstract
Background
Patients often present to emergency departments (EDs) with concerns that do not require emergency care. Self-triage and other interventions may help some patients decide whether they should be seen in the ED. Symptoms associated with low risk of hospitalization can be identified in national ED data and can inform the design of interventions to reduce avoidable ED visits.
Methods
We used the National Hospital Ambulatory Medical Care Survey (NHAMCS) data from the United States National Health Care Statistics (NHCS) division of the Centers for Disease Control and Prevention (CDC). The ED datasets from 2011 through 2020 were combined. Primary reasons for ED visit and the binary field for hospital admission from the ED were used to estimate the proportion of ED patients admitted to the hospital for each reason for visit and age category.
Results
There were 221,027 surveyed ED visits during the 10-year data collection with 736 different primary reasons for visit and 23,228 hospitalizations. There were 145 million estimated hospitalizations from 1.37 billion estimated ED visits (10.6%). Inclusion criteria for this study were reasons for visit which had at least 30 ED visits in the sample; there were 396 separate reasons for visit which met this criteria. Of these 396 reasons for visit, 97 had admission percentages less than 2% and another 52 had hospital admissions estimated between 2% and 4%. However, there was a significant increase in hospitalizations within many of the ED reasons for visit in older adults.
Conclusion
Reasons for visit from national ED data can be ranked by hospitalization risk. Low-risk symptoms may help healthcare institutions identify potentially avoidable ED visits. Healthcare systems can use this information to help manage potentially avoidable ED visits with interventions designed to apply to their patient population and healthcare access.
Keywords
Introduction
Acute care comprises a large part of ambulatory care and much of it does not take place in an office setting. 1 Emergency departments (EDs) see many acute care visits but there has been a trend toward use of other methods for accessing healthcare including urgent care centers, retail clinics, and telemedicine visits. 2
Access issues may be driving some of the use of ED visits. The National Health Interview Survey showed that barriers to usual care were significantly associated with ED use. 3 Barriers to care such as being “unable to get through on phone,” “couldn’t get an appointment soon enough,” and “not open when you could go” were all associated with ED use.3,4 Consistent with access issues driving ED visits, Weinick et al concluded that many emergency department visits could be managed at urgent care centers and retail clinics. 5 After hours acute care availability within urgent care centers and retail clinics has been associated with some decreased ED use but has not necessarily decreased cost of care.6,7 However, even with alternative forms of healthcare access and extended hours, overcrowding and “clinically unnecessary use of EDs” is still a problem in the US and UK.8,9
Healthcare has seen a radical change within the last few years. During the pandemic, there was a need to direct patients with COVID symptoms to the appropriate healthcare setting. Directing all those concerned about COVID to the ED could have resulted in ED overcrowding, and potentially more virus transmission to those in the ED already burdened with other disease. To help reduce ED visits and make COVID care and detection more efficient, Mayo Clinic and the University of California, San Francisco successfully developed online self-triage and self-scheduling systems for COVID that diverted asymptomatic and symptomatic patients without severe symptoms to outpatient testing, thus avoiding ED visits.10–12 These interventions for COVID demonstrated the potential for broader interventions to decrease unnecessary ED visits.
There is no consensus on how to identify an unnecessary or avoidable ED visit. Different criteria for identifying avoidable ED visits have surfaced in the literature. 13 Hospital admissions from the ED, 13 procedures and tests done in the ED, 14 medications dispensed, 15 diagnosis codes, 16 and chart review 17 have all been used to assess whether an ED visit was avoidable or not. In this study, we use national ED visit data and associated hospitalization risk to identify potentially avoidable ED visits. Using complex survey analysis on this national data, we can estimate the probability of hospitalization associated with each reason for visit. Our aim was to supply healthcare institutions with a comprehensive list of reasons for visit and their associated risk for hospitalization. Reasons for ED visits associated with low risk of hospitalization could represent opportunities to safely expand care alternatives to the ED such as online self-triage, e-visits, video visits, and self-scheduled office visits. Other interventions such as coaching patients when and how to use various forms of access also need to be explored.
Methods
This was a retrospective analysis of the National Hospital Ambulatory Medical Care Survey (NHAMCS). NHAMCS is a survey conducted yearly by the National Center for Health Statistics (NCHS) division of the Centers for Disease Control (CDC). 18 We used the emergency department surveys of NHAMCS for this study.
Data Collection and Preparation
Data used for this study was collected and curated by the CDC and is available online. 19 Each year over the past several decades, the CDC has collected data from EDs across the US. The survey has a complex sampling design, intended to represent the entire US population's ED visits by utilizing patient weighting factors. The survey results are reported yearly and have data fields that are well-defined and can be combined over multiple years. The years that we used in this study were from 2011 through 2020, for a total of 10 consecutive years. The combined 10 years represented over 220,000 ED visits in national EDs across the US.
The national ED dataset consists of fields that can be used in retrospective analysis. The items of interest for this study were the primary reason for visit (presenting symptom), patient age, and the binary outcome of admission to the hospital (coded ADMITHOS). 20
The survey has coded reasons for the ED visit. These reasons for visit have been developed over several decades, going back to the early 1970s. 21 Reasons for an ED visit (coded RFV) can be multiple and are contained in five different fields, labeled RFV1 through RFV5. RFV1 is the primary reason for visit, RFV2 is the secondary reason for visit, and so on up to RFV5, the fifth reason for visit if applicable. All the visits have an associated RFV1 code, with a small number of RFV1 s coded −9, 89970, 89980, or 89990 which had the respective descriptions blank, 0.25% of entries; no reason for visit, 0.03%; not enough information, 0.16%; and illegible, 0.01%. RFV1 codes and their descriptions are downloadable from the NHAMCS website. 20
Also included in the national data are two fields for age. Age by each year is coded (AGE) and includes 94 years from 0 through 93 and a 95th age group representing 94 and above. In addition, there is also an ordinal age variable (coded AGER) for six mutually exclusive age ranges. The six age ranges in the NHAMCS field AGER are: 0–14, 15–24, 25–44, 45–64, 65–74, and ages 75 and up.
Outcomes Measures
Our primary outcome was hospital admissions. Hospital admission was considered an outcome proxy for an unavoidable ED visit. Visits with a very low probability of hospitalization could potentially be handled safely in less intensive settings such as urgent care clinics, retail clinics, or outpatient offices. We determined the proportion of hospital admissions by each primary reason for visit (RFV1) and by age range (AGER).
Statistical Analysis
We used Stata® 18.0 (College Station, Texas). The binary field of hospital admission was used for proportions (percent hospitalizations) and logistic regression. For our analysis, we used the Stata complex survey design module to calculate the proportion of hospitalizations with each reason for visit and with six mutually exclusive age categories within each reason for visit. The six age categories we used were those already in the dataset design of the NHAMCS. Logistic regression analysis was used to evaluate the change in admission odds ratios by age for selected reasons for visits. The age subgroup of 25–44 was used as the base to make logistic regression comparisons with older age subgroups.
The NCHS has recommendations concerning best practice for use of the NHAMCS dataset. We followed the recommendations by avoiding use of any subgroup with fewer than 30 ED observations.22,23
This study was a secondary data analysis of publicly available, deidentified data from the CDC. Thus, this study did not qualify as human subjects research and was exempt from IRB review.
Results
The combined 10-year survey sample was 221,027 ED visits. Complex survey analysis of these 221,027 sampled visits resulted in an estimated total of 1.37 billion (1.37B) visits across the US population. There were 23,228 hospitalizations from the surveyed visits for an estimated hospitalization rate for all ED visits of 10.6%, (CI 95%; 9.8% to 11.4%). The risk of hospitalization from an ED visit for females was 10.0% (CI 95%; 9.2% to 10.8%), males were 11.3% (CI 95%; 10.5% to 12.2%).
ED visits for those under age 15 were estimated to be 257 million (M) (18.8%), ages 15–24 at 198 M visits (14.5%), ages 25–44 with 381 M visits (27.8%), ages 45–64 with 308 M visits (22.5%), ages 65–74 with 104 M visits (7.6%), and ages 75 and older with 124 M visits (9.1%).
Hospitalization by Primary Reason for ED Visits (RFV1, all Ages)
The national data had a total of 736 different primary reasons for visits for the 10-year ED visit sample. Of the 736, there were 396 RFV1s that met the criteria of having at least 30 ED visits each. These 396 RFV1s accounted for 1.35B estimated ED visits or 98.5% (1.35B/1.37B) of the total estimated ED visits.
Figure 1 is a histogram of the 396 RFV1s by the estimated percent hospitalized for each RFV1. There were 97 RFV1s that each had a probability of hospitalization from the ED visit of less than 2%. These ED visits with less than 2% probability of hospitalization accounted for 16.4% of total estimated ED visits. There were 52 RFV1s associated with ED visits with 2% to 4% probability of hospitalization each (10.7% estimated visits), and 72 RFV1s associated with hospitalization outcomes in 4% to 8% of the ED visits (24% of total estimated visits). There were 175 RFV1s associated with a higher probability of hospitalization: 100 RFV1s, each with 8% to 20% hospitalized (34.6% estimated visits) and 75 RFV1s, each resulting in greater than 20% hospitalized from the ED visits (12.9% of total estimated visits). The entire 396 list of reasons for visits along with the associated hospitalization risk (estimate) is available in supplemental files as “hospital admit percent by primary reason for visit—all ages combined,” sorted by ED visit frequency.
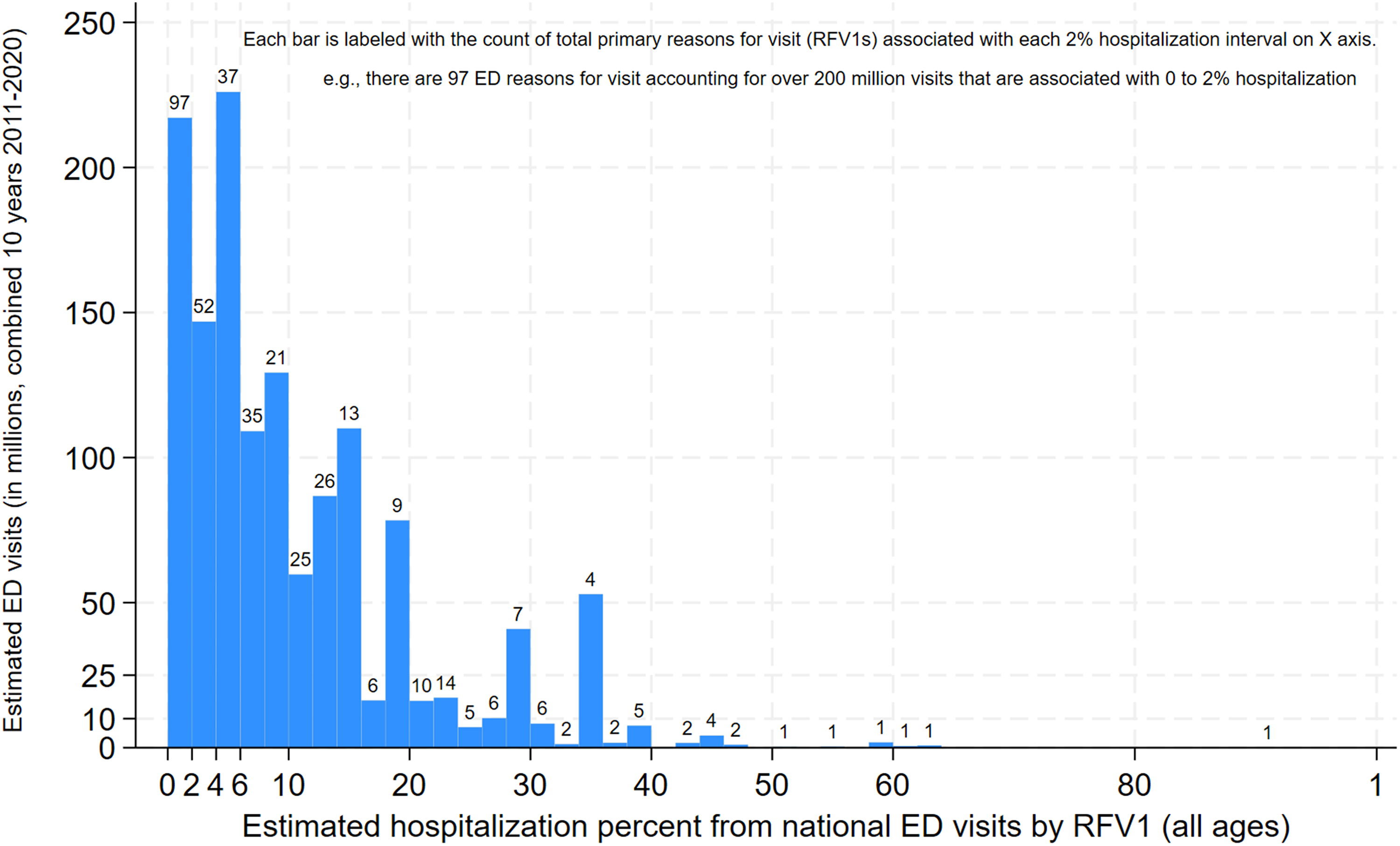
Histogram of 396 reasons for NHAMCS ED visits by the estimated hospitalization percent for each RFV1. Reasons for visits included all that met criteria of at least 30 survey occurrences over all ages for the 10-year combined sample.
Hospitalization from ED as a Function of Age
Probability of hospitalization associated with ED visits was strongly associated with age. Figure 2 shows the hospitalization percentages by patient age. With a best-fit logit transformation of hospitalization probability (logit = ln [probability hospitalized/probability not hospitalized]), the transformed linear fit was excellent (adjusted r2= .97, P < 0.0001). The best-fit logit model (shown in Figure 2) was −3.91 (CI 95% −4.08 to −3.74) + age (in years) × 0.038 (CI 95% 0.036 to 0.040).

Hospitalization percent by each year in age. A best-fit logit model (ln(odds hospitalized) = constant (−3.91) + 0.038 × age (in years)) is superimposed. 0 is birth to 1 year, 1 is from age 1 to 2. The final year on the x-axis is age 94 and up.
The relationship between age and hospitalization is also shown in the histograms of reasons for visits by age group (Figure 3). Advancing age groups are generally associated with increasingly higher hospitalization rates for each particular reason for visit. Thus, in Figure 3, we observe a flattening of the histogram with advancing age, with low probability reasons for visit getting fewer in number and more reasons for visit having higher probabilities of hospitalization. This clearly demonstrates that there are fewer and fewer opportunities to identify low-risk reasons for visit with advancing age.

Counts of reasons for visits by ED hospitalization risk for that RFV1. Separated by age groups (AGER field in NHAMCS data). Each RFV1 within the age group has a minimum of 30 ED survey visits.
Hospitalizations Associated with Reasons for Visit and Age
Because there were six age categories, not all of the 396 RFV1s with at least 30 surveyed ED visits when counted over all ages had at least 30 visits in each RFV1-age subgroup. However, there were 271 RFV1s of the 396 that had 30 or more surveyed ED visits in at least one of the 6 age subgroups. These 271 RFV1s were represented in a total of 953 unique RFV1-age subgroups that each contained over 30 surveyed ED visits. These 953 unique RFV1-age subgroups accounted for 94% (1.27B/1.35B) of the 10-year estimated ED visits. Both Table 1 and Figure 3 use the 953 unique RFV1-age subgroups. Columns of Table 1 separate the ED visits by risk of hospitalization and show the number of RFV1-age subgroups and estimated ED visits associated with hospitalization probabilities. The supplemental file “hospital admit percent by primary reason for visit and age” contains all 953 unique RFV1-age subgroups with associated admit percent and age group category referred to in Figure 3 and Table 1.
Hospitalization Percent Categories (Columns) by Age Group (Rows) Showing Estimated ED Visit Volume (in Millions) and Number of Different RFV1-Age Subgroups That are Involved.

Changes in RFV1 Frequency Rank with Age
The frequency rank of the primary reasons for visit changes with age as shown in Figure 4. For example, sore throat is a very common reason for visit in younger ages and ranks 11th overall in national ED visit frequency, but in the 75 and older group drops to 109th. Figure 4 shows that skin rash as a reason for visit also drops in relative frequency with age while vertigo and back pain as reasons for visit increase with age.

Twelve most frequent reasons for ED visits (over all ages) showing within age group relative frequency rank as age increases. In parentheses are the NHAMCS RFV codes for each of the twelve most frequent reasons for visit.
Other less frequent overall reasons for visit (not shown in Figure 4) such as neurologic symptoms of arm weakness or speech problems have higher frequencies with age. Alcohol intoxication is more common as a reason for visit among younger adults but not in children or older adults. Our supplemental files contain estimated ED visit counts, thus allowing readers to consider frequency of ED visits along with hospitalization risk in determining what interventions may be most effective.
Changes in Hospitalization Risk by Age for Most Frequent Individual Reasons for Visit
Figure 5 shows the same 12 top ED visits have differing amounts of change in hospitalization percent with age. Figure 5 shows that within each RFV1 there is generally an increase of percent hospitalization with increasing age, which we have examined in more detail in the next section.

Twelve most frequent reasons for ED visits (over all ages) showing the ED visit percent hospitalized as age increases. In parentheses are the NHAMCS RFV codes for each of the twelve most frequent reasons for visit.
Odds Ratios of Hospital Admission for Adults Following Emergency Department Visit
The association of hospitalizations with age in Figure 2 shows that adults in the age range 25–44 have lower overall hospitalization risk compared to older age groups. In comparison to a baseline group of ages 25–44, those aged 45–64 had a hospitalization odds ratio (OR) of 2.52 (CI 95%; 2.34 to 2.71). Compared to the 25–44-year-old base, those aged 65–74 had a hospitalization OR of 5.12 (CI 95%; 4.62 to 5.67), and those 75 years and up had hospitalization OR of 7.10 (CI 95%; 6.49 to 7.76).
We were also able to examine the change in hospitalization odds ratio with individual RFV1s using logistic regression in the complex survey design. There were 90 reasons for visits that met criteria for 30 ED visits in each of four adult age groups.
Of the 90 RFV1s fulfilling criteria for analysis, there were 5 RFV1s in the base age of 25–44 that had no hospital admissions among the surveyed visits. The RFV1s with no admissions in ages 25–44 were: suture insertion/removals (0 admissions/250 survey ED visits, 1.4 M estimated ED visits); shoulder injury (0 admissions/126 survey visits, 721 K est. ED visits); urinary frequency and urgency (0/75, 437 K); other urinary dysfunction (0/53, 333 K); and nosebleeds (0/54, 394 K). Lacking a single hospital admission for those 5 RFV1 in the age base range, we eliminated them from further OR analysis, leaving 85 RFV1s, all of which had at least the 30 requisite ED survey counts in all 4 upper age groups and at least one hospital admission in the comparison base of ages 25–44. For those 85 RFV1s we calculated the odds ratio of hospital admission of each of the three older age groups (ages 45–64, 65–74, and 75 and up) compared to the base of those aged 25–44. The complete list of 85 RFV1s with odds ratios and confidence intervals are in supplemental files as “hospital admit odds ratios of reasons for visit by age group compared to the 25–44 age group.”
Of the 85 RFV1s meeting the above criteria, none had a statistically significant lower hospitalization OR (CI 95% upper limit less than 1) for any of the 3 older comparison age groups. For the 45- to 64-year-olds, 41% (35/85) of the reasons for visit had significantly higher odds of hospitalization than the base group of 25- to 44-year-olds (CI 95% lower limit OR greater than 1). The same analysis for 65- to 74-year-olds showed that 68% of examined reasons for visit (58/85) had significantly higher hospitalization odds compared to the 25- to 44-year-olds. For those 75 and older, 78% (66/85) of RFV1s had significantly greater hospitalization odds compared to the 25- to 44-year-olds. No hospital admissions were reported in the surveys for three additional RFV1-age subgroups (above the 25- to 44-year base age): insect bites in 2 age subgroups (65–74, and 75 and up) and lacerations (head and neck) in the 65–74 age group. Odds ratios could not be calculated for these subgroups and are left blank in the supplemental file.
Reasons for Visit with Low Probabilities of Hospitalization from ED
Table 1 shows that there were 191 M emergency department visits from 211 RFV1-age subgroups that had extremely low hospitalization rates (less than 1%). An additional 141 M visits from 84 RFV1-age subgroups had hospitalization rates between 1% and 2%.) These low-risk subgroups (<2% hospitalizations) accounted for 332 M ED visits (26.2% of the 1.27B estimated visits). Using the supplemental file labeled “hospital admit less than 1% by primary reason for visit and age,” readers can examine reasons for ED visit sorted by <1% hospitalization risk and age group. Although the level of detail in the supplemental files is intended to help those wanting to look for specific healthcare opportunities to decrease avoidable ED visits, a few generalizations can be stated. In the age group 0 through 14, the extremely low-risk RFV1s (<1% hospitalizations) include injuries, lacerations, extremity/joint pain, ear and eye concerns, skin rashes, sore throat, and bites. There were 57 of these low hospitalization risk reasons for visit in this age group that accounted for 75 M national ED visits (Table 1). For the 15–24 age group, there were 58 individual RFV1s that were associated with hospitalization in less than 1% of the 51 M ED visits (Table 1). This older age group also had extremity injuries, ear and eye concerns, skin rashes, sore throat, and extremity/joint pain accounting for the ED visits with low hospitalization risk. In addition, the 15–24 age group also had low-risk ED visits concerning exposure to sexually transmitted disease, unconfirmed pregnancy, vaginal symptoms, wheezing, cough, sore throat, and urinary tract infection.
The supplemental file labeled “hospital admit percent by primary reason for visit and age” contains the complete information on hospitalization risk (and 95% confidence intervals) for each of the 953 RFV1-age subgroups that met the criteria for inclusion (at least 30 ED visits in each subgroup of RFV1 and age range).
Discussion
Principal Findings
The hospitalization risk of an ED visit varies widely with primary reason for visit and age. National data is available to help determine reasons for ED visits that are unlikely to result in a hospitalization. These lower-risk reasons for visits may be opportunities to intervene with alternatives to the ED. Use of this national data may help guide those who are developing interventions to decrease potentially avoidable ED visits.
Practice Implications
Our analysis shows that there are millions of ED visits with very low probability of hospital admission. It has been suggested that many of these ED visits are avoidable and may be safely handled in other practice settings, both in the US and internationally.24–26 A number of interventions to decrease avoidable ED visits have been tried with varying degrees of success. 27 Interventions have used strategies such as improving primary care access, 6 and ED diversion either before or at the time of ED visit.28,29 In addition, there has been evidence of increasing utilization of non-ED options for receiving acute care such as urgent care centers for treatment of low-acuity conditions. 2 Identification of potentially avoidable ED visits is an important issue to consider when addressing healthcare costs and quality. 13
Hollander and Sharma in a commentary in the NEJM Catalyst categorize some potential approaches to decrease ED visits by distinguishing acute health concerns that are (1) unlikely to need ED, (2) reasonable to evaluate before deciding if they need to go to the ED, and (3) highly likely to need in-person evaluation in ED. 30 The datasets we supply in this manuscript can help do this, identify those unlikely to need the ED as well as those who very likely need to be evaluated in the ED. Institutions can use the hospitalization risk tables herein to tailor interventions to specific reasons for visit that pertain to their unique healthcare system. For example, we found that younger patients with extremity injuries were low risk for hospitalization. Our institution's online self-triage self-scheduling intervention took advantage of this finding as well as the Ottawa x-ray rules 31 to direct patients reporting ankle injuries to self-schedule an outpatient visit with a pre-scheduled x-ray. Likewise, Mayo Clinic developed an online self-triage and self-scheduling tool for ear and hearing symptoms. 32 Mayo Clinic outcomes data from online ear and hearing self-triage supports that these symptoms are low risk, similar to the findings of national ED visits found in this study. 32 In addition to a lack of concerning outcomes such as increased hospitalizations, the makeup of diagnoses following the ear and hearing self-triage use were similar to those from ED visits, suggesting that using self-triage might be an intervention that could decrease avoidable ED visits. 33 It should be noted that outcomes research for self-triage is difficult and evaluation of self-triage quality has often been done using “patient vignettes” or “simulated patients.” 34 One of the more recent actual outcomes studies of self-triage was limited to ear and hearing concerns as noted above 32 and more research needs to be done. 34
Patient Implications
National ED data shows that elderly patients presenting to the ED often end up admitted to the hospital. Our supplemental tables may be helpful to consult when deciding about interventions for potentially avoidable ED visits and whether there should be some age limits for those interventions.
Perceived seriousness of medical problem was the reason for an ED visit for 77% of adults ages 18–64 based on the National Health Interview Survey. 35 It is possible that online resources such as self-triage could help direct patients to healthcare that was more consistent with the actual need for acute medical attention rather than the patient-perceived seriousness. Additional research is needed to determine how best to do this. Although online self-triaging (available 24/7) would seem to be an excellent modality to triage and advise low-risk patients for alternative care options to the ED, Mayo Clinic self-triage experience tells us that many patients with ear and hearing concerns still went to the ED with diagnoses that could have been treated in the office despite no online triage recommendation to go to the ED. 32
Clearly there are a number of factors in addition to perceived seriousness of medical problem that impact the patient decision to go to the ED. Patients now have the opportunity to have telemedicine visits 24/7 with providers via services such as Teladoc, Virtuwell, and others.36,37 Patients also have the opportunity to self-schedule face-to-face or other visits with providers through Zocdoc, Lybrate, or with their own providers.38–42 Many patients also now have the ability to message their provider for advice about acute care. Social determinants of health also appear to play a significant role in ED visits, 43 and Medicaid expansion may also. 44 Low health literacy, lack of access to online resources, and illness anxiety can limit the potential impact of telemedicine visits, patient messaging, and self-triage for those in need. Many patients who visit the ED do not have the financial means for online care or do not have a digital connection. Thus, potential interventions involving patient messages and other forms of connected care are not currently feasible for many ED patients. Identification of avoidable ED visits can help guide selection of patients for interventions, but the interventions themselves will need to take into account the myriad reasons why patients elect to go to the ED and the resources available to these patients.
Comparison with Other Studies
Our findings are consistent with the findings of Yang et al who found that non-avoidable ED visits were associated with increasing age. 45 Ginsburg et al also suggested that age be used in the adult triage process in the ED. 46 Reasons for visit stated as injury and psychiatric symptoms also influence predictability of an avoidable visit. 45
Limitations
The NHAMCS datasets have several limitations. It is a challenging task to obtain a representative sample of ED visits across diverse populations and locations in the United States. Advances in data collection from interoperability and accessibility of electronic health records have resulted in the CDC discontinuing the NHAMCS survey methodology that was used for the data we are using here. The last public user files using the methodology in the current datasets will be for 2022 data to be released in 2024. 47
The RFV1 categories are subject to possible patient and ED staff interpretation. It is unknown how well the patient articulates the reason for ED visit and how well it gets translated into the survey dataset.
Hospital admission has been a de facto standard as a measure for illness severity. However, a number of factors identified by survey such as ED busyness, time of day, waiting times, patient social support, and ED culture all have been found to influence the decision to admit. 48 In addition, reasons for visit with a low probability of admission might quite reasonably require monitoring in an ED setting; for instance, anaphylaxis, which might be coded as “shortness of breath” or “rash” requires ED-level care, but may not necessitate hospital admission.
Observation admissions are also used in EDs instead of hospital admission for a variety of reasons. The NHAMCS datasets have a field labeled OBSDIS which are observations then dismissals. However, observation admissions both for adults and children are highly variable depending on the ED and hospital.49,50 We did not include observation admissions as a primary measure. However, for readers who are interested, we did include the proportion of ED visits where there was either a hospital or observation unit admission (either ADMITHOS =1 or OBSDIS =1). These risks are found in our tables in supplemental files.
We also did not examine other potential ways of looking at “avoidable” ED visits. For example, Hsia et al and Yang et al considered avoidable ED visits from a “conservative definition” as those who not only were dismissed from the ED but also did not have any diagnostic tests, screening, procedures or medications before dismissal.15,45 We also acknowledge that algorithms identifying low-acuity emergency department visits are “imperfect predictors of visit acuity” as noted by Chen et al. 16
Rosano et al published a systematic review of the impact of access on ED visits which gives context to studies such as this one. 51 The NHAMCS dataset does not have data that pertains directly to available healthcare access in the locations surrounding the sampled national EDs. Thus, our study lacks the ability to assess the role access has in national ED visits. In addition, there are medical conditions whose hospital admission rates through the ED are affected by local healthcare factors. The terminology “ambulatory care-sensitive conditions” (ACSCs) has been used to describe this.52,53 An example of an ACSC is asthma. A patient with asthma who is unable to readily get treatment for exacerbations, lacks appropriate immunizations, or whose asthma is not well controlled due to factors in the healthcare system, may have a higher likelihood of hospital admission. The NHAMCS does not contain specific data to assess how different healthcare systems might alter the hospital admission rates for ambulatory care-sensitive conditions.
The NHAMCS dataset was not designed to contain data on all the possible reasons for the ED visit other than the “reason for visit” data field. Lack of primary care access, lack of after hours care, lack of transportation, and lack of financial resources are all possible reasons for patients to go the ED, regardless of the presenting symptom contained in the “reason for visit” data field. As such, the NHAMCS dataset was not designed to help us answer exactly why the patient presented to the ED for care rather than seek care somewhere else. What the national data does show is that there are large numbers of younger patients being seen across a national ED sample who have very low risk for hospitalization.
Our included supplemental files examine in detail the risk of hospitalization associated with the ED reason for visit and patient age. Those planning interventions to decrease ED utilization, whether through triage, 24 h walk-in clinics to improve access, or other interventions, can use our supplemental files to help assess the potential risk of ED diversion. For example, use of our hospitalization risk tables can help those planning interventions to reduce ED overcrowding. A concern for ED diversion interventions is the potential risk when patients do not go to the ED for a specific symptom. Those planning interventions to address ED overcrowding can cite the national data we supply in the supplemental files. Using the supplemental tables, those planning the interventions can identify patients with lower risk.
Conclusion
Further interventions aimed at decreasing avoidable ED visits are necessary to reduce ED overcrowding and optimize the use of limited healthcare resources. Our research found that although hospitalization risk by ED visit varies with primary reason for visit and age, there remain millions of ED visits at low risk for hospitalization and thus may represent a possibility for intervention. The data we have collected regarding the primary reason for visit frequency and subsequent hospitalization risk may assist those in developing interventions specific to their patient populations and healthcare systems.
Supplemental Material
sj-xlsx-1-hme-10.1177_23333928231214169 - Supplemental material for Hospitalization Risk Associated With Emergency Department Reasons for Visit and Patient Age: A Retrospective Evaluation of National Emergency Department Survey Data to Help Identify Potentially Avoidable Emergency Department Visits
Supplemental material, sj-xlsx-1-hme-10.1177_23333928231214169 for Hospitalization Risk Associated With Emergency Department Reasons for Visit and Patient Age: A Retrospective Evaluation of National Emergency Department Survey Data to Help Identify Potentially Avoidable Emergency Department Visits by Frederick North, Gregory M Garrison, Teresa B Jensen, Jennifer Pecina and Robert Stroebel in Health Services Research and Managerial Epidemiology
Supplemental Material
sj-xlsx-2-hme-10.1177_23333928231214169 - Supplemental material for Hospitalization Risk Associated With Emergency Department Reasons for Visit and Patient Age: A Retrospective Evaluation of National Emergency Department Survey Data to Help Identify Potentially Avoidable Emergency Department Visits
Supplemental material, sj-xlsx-2-hme-10.1177_23333928231214169 for Hospitalization Risk Associated With Emergency Department Reasons for Visit and Patient Age: A Retrospective Evaluation of National Emergency Department Survey Data to Help Identify Potentially Avoidable Emergency Department Visits by Frederick North, Gregory M Garrison, Teresa B Jensen, Jennifer Pecina and Robert Stroebel in Health Services Research and Managerial Epidemiology
Supplemental Material
sj-xlsx-3-hme-10.1177_23333928231214169 - Supplemental material for Hospitalization Risk Associated With Emergency Department Reasons for Visit and Patient Age: A Retrospective Evaluation of National Emergency Department Survey Data to Help Identify Potentially Avoidable Emergency Department Visits
Supplemental material, sj-xlsx-3-hme-10.1177_23333928231214169 for Hospitalization Risk Associated With Emergency Department Reasons for Visit and Patient Age: A Retrospective Evaluation of National Emergency Department Survey Data to Help Identify Potentially Avoidable Emergency Department Visits by Frederick North, Gregory M Garrison, Teresa B Jensen, Jennifer Pecina and Robert Stroebel in Health Services Research and Managerial Epidemiology
Supplemental Material
sj-xlsx-4-hme-10.1177_23333928231214169 - Supplemental material for Hospitalization Risk Associated With Emergency Department Reasons for Visit and Patient Age: A Retrospective Evaluation of National Emergency Department Survey Data to Help Identify Potentially Avoidable Emergency Department Visits
Supplemental material, sj-xlsx-4-hme-10.1177_23333928231214169 for Hospitalization Risk Associated With Emergency Department Reasons for Visit and Patient Age: A Retrospective Evaluation of National Emergency Department Survey Data to Help Identify Potentially Avoidable Emergency Department Visits by Frederick North, Gregory M Garrison, Teresa B Jensen, Jennifer Pecina and Robert Stroebel in Health Services Research and Managerial Epidemiology
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One of the authors serves as the Editor in Chief of this journal.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as public datasets were used and analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.