
Abstract
Objectives
Severe Acute Malnutrition is a significant cause of mortality in children under the age of 5 years in low-resource settings, including Northern Nigeria. The study aimed to determine the associations between selected risk factors and mortality outcomes in children admitted with SAM in a facility in Katsina State, Northern Nigeria.
Methods
A prospective observational cohort of 201 children aged 6 to 59 months who were admitted with severe acute malnutrition (SAM) in stabilization centers in Katsina State, Northern Nigeria between May 18, 2021, and July 20, 2021, (63 days) were assessed followed up. Outcomes were analyzed using Kaplan-Meir analysis to estimate time to death, and Cox proportional-hazard regression model was used to determine predictors of mortality.
Results
The log-rank test showed significant differences in the probability of death between categories of diarrheal status (log-rank statistic = 9.760, P = .021) and presence of existing disease (comorbidity) (log-rank statistic = 5.338, P = .021). The study identified that severely malnourished children admitted with comorbidities showed significant association with time to event (death) (AHR: 4.109, 95% CI: 1.51, 32.60). The estimated mean time until death was 57.9 days (±3.0) for children without comorbidities and 20.1 (±3.0) days for children with comorbidities. The median survival time was 18 days for children with comorbidities.
Conclusion
The presence of comorbidities was significantly associated with mortality. Severely malnourished children with comorbidities had 4 times higher mortality risk than severely malnourished children admitted without comorbidities. Clinicians and health workers should give due emphasis to the early detection and effective management of comorbidities in children with severe acute malnutrition.
Keywords
Introduction
Adequate nutrition is a critical determinant of health and development and vital for the survival of children under 5 years of age. Severe Acute Malnutrition (SAM) is defined as a weight-for-height z-score of <−3 or a Mid-Upper Arm Circumference (MUAC) of <115 mm or the presence of bilateral pitting edema, or both in children 6 to 59 months of age. 1 SAM prevalence of ≥2% in a given population is considered critical. 2 UNICEF estimated that 2.5% and 2.3% of children globally and West Africa are severely malnourished. 3 A review of SAM inpatient mortality rates in some health facilities in sub-Saharan Africa indicates that mortality rates were up to 40%. 4 High mortality rates of 5.8%, 10.8%, and 12.5% were reported among severely malnourished children receiving inpatient care in Ethiopia respectively,5–7 and 9.8% in Uganda. 8 Although very high mortality rates of 40.5% and 46% were reported in Zambia, respectively.9,10 A myriad of factors are associated with the outcome of SAM children treated in hospitals. In Ethiopia, predictors of mortality in hospitalized severely malnourished children were found to be HIV infection, bronchopneumonia, diarrhea, rickets, and malaria.11,12 Although another study found altered metabolism, anemia, and hypoglycemia as predictors of mortality among hospitalized malnourished children. 13 Northwestern Nigeria generally has poor health indices with the prevalence of SAM as high as 8.3%. 14 Children with complicated SAM are those who have clinical features of infection, metabolic disturbance, severe edema, hypothermia, vomiting, severe dehydration, severe anemia, or a lack of appetite, requiring in-patient treatment initially with low-protein milk-based feeds. These children are later considered for discharge to continue nutritional management as outpatients if complications resolve. Although the World Health Organization (WHO) and United Nations Children's Fund (UNICEF) have developed guidelines for treating children hospitalized with SAM, high mortality is still reported in some developing countries.
Figure 1 illustrates the relationship between certain underlying and immediate factors of patients with SAM and their outcomes during hospitalization. Socioeconomic factors such as maternal educational status and family income can affect water quality and access to health care. These, together with the breastfeeding status, immunizations, and comorbid conditions in the patient, can determine the ability to feed well and have sufficient glucose stores, fluids, electrolytes, or adequate immunity for recovery. Similarly, poor quality of care or support at the hospital can immediately affect patient outcomes. 15 Diarrheal diseases further derange fluids and electrolytes, affecting the severity of illness and the outcome of inpatients. Understanding the socioeconomic and environmental factors that accelerate mortality in patients with SAM will be vital in addressing the community and health facility levels.
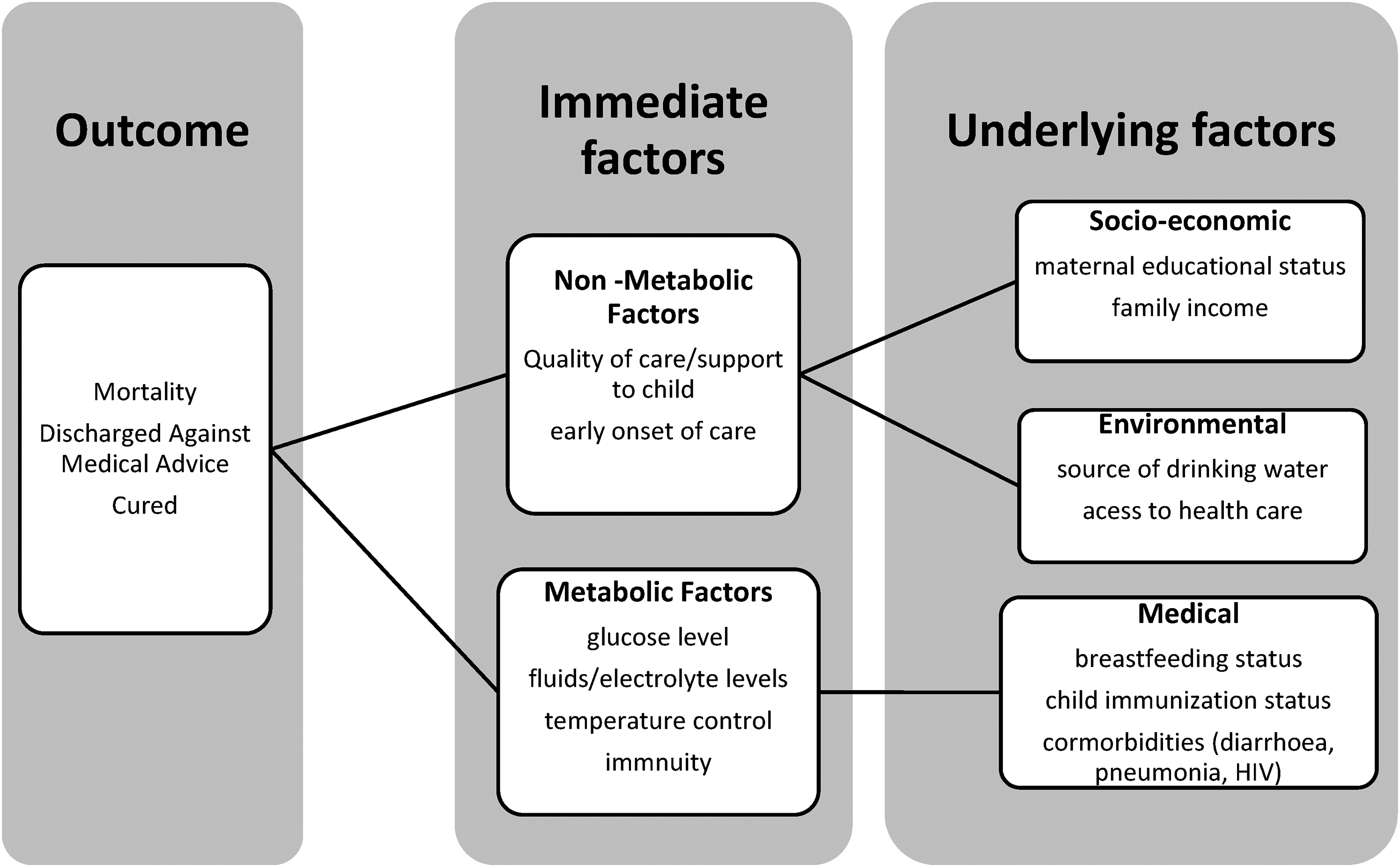
Conceptual framework on the relationship between determinants of inpatients with SAM and outcome.
SAM is prevalent in low- and middle-income countries where poverty is common and resources limited. Etiologically, SAM results from the complex interplay between nutritional, pathological, and socioeconomic factors. Children born in conflict, famine, and population displacement tend to be more prone to SAM. 16 Africa and Asia bear almost 98% of the burden of malnutrition. 17 Within Africa, Western Africa has the highest number of severely wasted children, with Nigeria contributing significantly. In 2018, Nigeria was expected to have 2.4 million new cases of SAM, accounting for nearly two-thirds of the annual estimated burden of SAM among the 9 countries of the Sahel Africa. 18 Within the country, the Northern region is the epicenter of all forms of malnutrition. 2 There have been concerted efforts to reduce child mortality caused by malnutrition, as highlighted in Goal 2 of the United Nations Sustainable Development Goal, which aims to achieve food security and improved nutrition. 19 Although such efforts markedly improved nutrition, malnutrition still threatens the lives of millions of children globally. 20 In 2018, over 49 million children under the age of 5 (under-5 children) were wasted, and among them, 17 million were severely wasted. 17
In 2009, Nigeria, in collaboration with UNICEF, flagged off its Community Management of Acute Malnutrition (CMAM) program. 21 Currently, the Northern states of Adamawa, Bauchi, Borno, Gombe Jigawa, Kano, Katsina, Kebbi, Sokoto, Yobe, and Zamfara benefit from the program. 22 CMAM has 4 primary components: outpatient therapeutic program (OTP) for SAM cases without complications; inpatient therapeutic program (ITP) for SAM cases with complications; community mobilization; and, where appropriate, supplementary feeding program for a moderate form of acute malnutrition. Since its inception, CMAM centers in Nigeria treat an average of 80% of its targeted caseload of SAM annually, which in 2018 was 648 040 children. However, based on the estimated burden of SAM, the SAM target population coverage was 26.8%. 18 It is a continuous effort to increase CMAM centers in countries with a high prevalence of SAM, such as Nigeria. Increasing the number of CMAM centers improves management outcomes and reduces the number of children who develop SAM and death complications. 19
In practice, children who present with uncomplicated SAM and are assessed to be having an appetite and clinically well are treated as outpatients. Only a few studies on the performances of CMAM centers within the study area are available. Treatment outcomes of hospitalized children with SAM have been studied in some developing countries with varying survival rates. However, deaths among hospitalized malnourished children were associated with certain factors and comorbidities such as hypothermia, anemia, pneumonia, and HIV. 2 For instance, 2 studies in India and Ethiopia found a significant association between diarrheal disease and mortality in children with SAM.,23,24 A retrospective study covering OTP records obtained within 2010 to 2013 at CMAM centers in Katsina and Jigawa states reported an 87.1% cure rate, 9.2% defaulter rate, 2.9% non-recovery rate, and 0.2 death rate. 22 The result conforms to the recommended outcomes at the CMAM centers of a minimum standard of more than 75% of the hospitalized children cured. And less than 15% and 5% of the children should default from treatment or die during hospitalization, respectively. 25 But the authors were also unable to deal with the effect of missing data and selection bias during data collection, which is a general limitation of retrospective studies. Analyzed OTP records also showed CMAN program acceptable outcomes in Katsina state.26,27
Contemporary literature shows several surveys of SAM in Nigeria involved children within the 6 to 59 months age group; however, very few researchers identified the predictors of mortality among the hospitalized critically ill children with the severe form of malnutrition. This is the case in Katsina, located in North-Western Nigeria, where the prevalence of SAM is highest and resources are limited. This study's objectives are to determine the case mortality rate of in-patients with severe acute malnutrition admitted in the CMAM stabilization centers in Katsina State and to determine risk factors associated with mortality among children 6 to 59months admitted with severe acute malnutrition in CMAM stabilization centers. The results could inform contextualized policy and decisions and used as a prognostic guide and improve the triage of children with SAM at CMAM centers in the study area. The study will be guided by the conceptual framework of the relationship between malnutrition, infections, and poverty. 15
Methodology
Ethical Consideration
Ethical approval for the use of data in this study was obtained from the Ministry of Health, Katsina State. Informed consent was obtained from every caregiver and documented before the interview by explaining the research objective. No incentives were given to the caregivers as compensation for partaking in the study. Records are appropriately archived kept confidential in a computer database protected by a password. The names of participants and research assistants were coded to ensure the anonymity of information coded to ensure the privacy of participants and anonymity of information.
Study Population
The study population was children aged from 6 months to 59 months diagnosed with severe acute malnutrition (SAM) receiving hospital-based care at the Community Management of Acute Malnutrition (CMAM) centers in Katsina State, Northwestern Nigeria. The children were admitted based on standard criteria from the Operational Guidelines on Community Management of Acute Malnutrition (CMAM) in Nigeria. 21 The inclusion criteria include children diagnosed clinically with severe acute malnutrition based on the following signs and anthropometric measurements; bilateral pitting edema or with mid-upper arm circumference (MUAC) of <11.5 cm and weight for height (z-scores) of <−3 standard deviation (SD).
Study Design
The study design was a prospective observational cohort. Hospital records of 201 children with SAM receiving in-patient management and therapeutic feeding were reviewed on admission and followed till discharge or death between May 18, 2021, and July 20, 2021 (63 days).
Sample Size Determination
The sample size was determined through power analysis with sample size calculator. 28 The power analysis considered the level of precision or alpha level (α) at 0.05, beta-level (β) set at 0.20, q1 = proportion of subjects that were in the exposed group (estimated from death rate among HIV positive malnourished children = 25%), q0 = proportion of subjects that were in the unexposed group from a previous study in Uganda.. 29 The analysis resulted in 255 study subjects.
Sampling and Sampling Procedure
The purposive sampling technique selected the 9 stabilization centers in the districts with functional CMAM centers in the state. The selected CMAM stabilization centers were Comprehensive Health Center Bakori, General Hospital Danmusa, General Hospital Kankara, General Hospital Jibia, Comprehensive Health Center Safana, Comprehensive Health Center Dandume, General Hospital Dutsinma, Comprehensive Health Center Faskari, Comprehensive Health Center Sabuwa. General Hospitals usually have a higher caseload than comprehensive health centers. Thus, 75% (192) of the sample size was allotted to the General Hospitals and the remaining 25% (63) to the Comprehensive Health Centers using proportionate sample allocation. The 4 General Hospitals were assigned 48 subjects each, and 4 comprehensive health centers were allotted 13 subjects each. One Comprehensive health center was left with 11 subjects. A consecutive sample of subjects was obtained from each of the CMAM stabilization centers.
Data Collection Procedure
A structured questionnaire was used to extract information on baseline characteristics on admission. A pilot survey was held at General Hospital Katsina to test the questionnaire on 30 randomly selected children. Two independent randomly selected research assistants were trained for 3 days on data collection using the questionnaire. Each of the assistants administered the survey tool on the randomly selected children to measure uniformity and consistency. The outcome of the inter-rater reliability indicated substantial agreements between the 2 assistants, К = .830, (P < .0005), 95 CI (0.430, 1.03). The inter-rater reliability measured by calculating Cohen's Kappa index yielded 83% consistency. Cohen's Kappa index values ranging from 60% to 79% were considered substantial.
On admission, a physical examination of the child was conducted to assess the body temperature. Then anthropometric measurements were taken to determine eligibility for inclusion in the study. Caretakers were interviewed on admission about the details on the predictors of mortality among malnourished children. Although details of outcome measures (dependent variables) cured, defaulted, died will be monitored and documented daily by a clinician.
Data Analysis
Data was entered and analyzed in SPSS software version 24. The sociodemographic and clinical characteristics on admission were compared between the groups for significant differences. Pearson's χ2 test was used to assess the differences in proportions between groups among the predictors namely sex, temperature, immunization status, diarrheal status, diarrheal Frequency, ANC Status, comorbidity, and child's access to CMAM center from residence. The assumptions for Kaplan-Meir estimation and proportional Cox-regression model were checked. The Kaplan-Meir (KM) curve was used to compare time to the event among the different groups of children receiving hospital-based care at the CMAM centers. Significance tests for these differences were assessed using the log-rank test. The proportional hazards Cox model was used to determine the predictors of mortality. A P value of less than or equal to 5% was considered significant.
Results
Sociodemographic and Admission Characteristics
Two hundred and fifty-five children were recruited for the study with a response rate of 79%. Thirty-three parents and caregivers of eligible children refused consent, and 21 of the children were not accompanied by a caregiver who could act as a proxy for consent. As such, 201 were followed up from admission to discharge, event, or default during the 63-day study period. Out of 201 subjects, 98 (48.8%) were female. The mean age (±SD) of the children was 23.34 (±5.0) months, with median birth order of 4.08 (±7.0). About half, 99 (49.3%) of all children were from monogamous settings, and nearly a third, 63 (31.3%), had extended families. As shown in Table 1, 11 subjects (5.5%) of the children had lost a parent with an approximately equal ratio (1:1) between paternal (5) and maternal loss (5). The majority of the caregivers, 178 (88.6%), were the mothers to the children.
Sociodemographic Characteristics of Children With SAM at Stabilization Centers in Katsina State, Nigeria.

Management Outcome of Children With SAM at the Stabilization Centers
Table 2 depicts the frequency of outcome measures among children with SAM at stabilization centers. Seventeen children (8.5%) died during their stay at the stabilization centers, whereas 180 children (89.6%) were cured, with 4 children (2%) who defaulted. Nine out of the 17 deaths and 3 of the 4 defaulted children were females. Of the 17 deaths, 6 had fever on admission, 6 were not immunized, and 6 were partially immunized. Children with diarrhea constituted 113 (56.2%) of the severe acute malnutrition cases. Sixty-seven (33.3%), 33 (16.4), and 13 (6.5) had acute, recurrent, and chronic diarrhea, respectively. Thirteen out of the 113 children with diarrhea died during hospitalization, out of which 7 were admitted with recurrent diarrhea. On admission, children with diarrheal frequency less than 6 times a day accounted for 71% of the deaths. Over half of the children, 113 (56.2%), were admitted with comorbidities, and 13 (6.5%) of the children died. Thus, children with comorbidities accounted for 13/17 (76.5%) of the mortalities. Table 3 depicts the various forms of comorbidities associated with the children admitted with SAM, with some of the children having multiple symptoms and conditions. Other than diarrhea, 21 (10.5) %, 33 (16.4%), 41 (20.4%), and 14 (7.0%) of the children on admission had respiratory disease, malaria, measles, and anemia cases, respectively.
Frequency of Outcome Measures Among Children With SAM at Stabilization Centers in Katsina State, Nigeria.
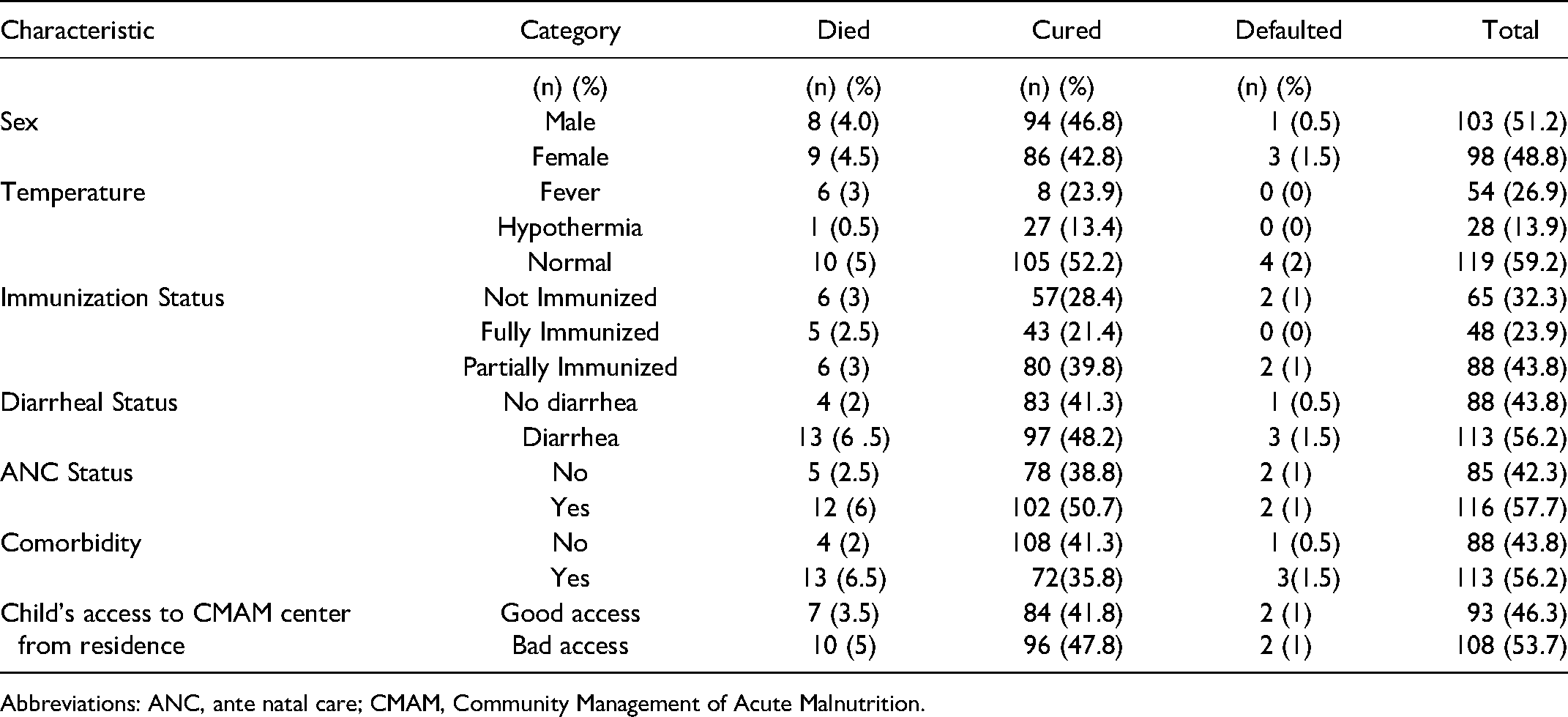
Abbreviations: ANC, ante natal care; CMAM, Community Management of Acute Malnutrition.
Comorbidities Among Children With SAM at Stabilization Centers in Katsina State, Nigeria.

Collinearity Diagnostics
Tests to see if the data met the assumption of collinearity were carried out and the results indicated that multi-collinearity was not a concern (Sex, Tolerance = 0.965, VIF = 1.037; Temperature, Tolerance = 0.826, VIF = 1.211; Immunization Status, Tolerance = 0.956, VIF = 1.046; Diarrheal Status, Tolerance = 0.366, VIF = 2.729; Diarrheal Frequency, Tolerance = 0.404, VIF = 2.474; ANC Status, Tolerance = 0.925, VIF = 1.081; Existing Disease [Comorbidity], Tolerance = 0.488, VIF = 2.047; Child's Access to CMAM center from Residence, Tolerance0 = .942, VIF = 1.061).
Life Table and Kaplan-Meier Analysis
Assumptions for the Kaplan-Meier estimation were not violated in the study. Both censored and event (death) states were mutually exclusive, the time to censorship or event (death) were well defined and measured, that is, the survival probabilities were the same for all the children admitted early and late in the study, and there was the independence of both censoring and event (death) occurring. Cured and defaulted outcomes were considered censored in the Kaplan-Meier analysis.
The Kaplan-Meir (KM) survival curve for children with SAM admitted with and without comorbidity showed that the treatment outcome of children without comorbidities was better than that of children with comorbidities (Figure 2). The estimated mean time until death is 57.9 (±3.0) days for children without comorbidities and 20.1 (±3.0) days for children with comorbidities. The median survival time (when 50% of them have died) is 18 (±3.0) days for children with comorbidities. Also, the Kaplan-Meir (KM) survival curve for children with SAM admitted with diarrhea showed that the treatment outcome of children without diarrhea was better than that of children with diarrhea (Figure 3). Until death, the estimated mean time is 58.3 days for children without diarrhea, 22.2 days for children with acute diarrhea, 16.8 days for children with recurrent diarrhea, and 13.4 days for children with chronic diarrhea. The median survival time for children with recurrent and acute diarrhea was 23 days and 18 days, respectively. The cumulative probability of staying in the stabilization centers was 97% on the third day, 94% on the sixth day, 87% on the ninth day, 81% on the 12th day, 76% on the 15th day, 70% at the 18th day and remains at 64% % from 21st day to 63rd day at the end of the study admission.

Kaplan-Meier plot of survival time of children with SAM admitted with and without comorbidity (N = 201). No—(n = 60) and Yes—(n = 142).
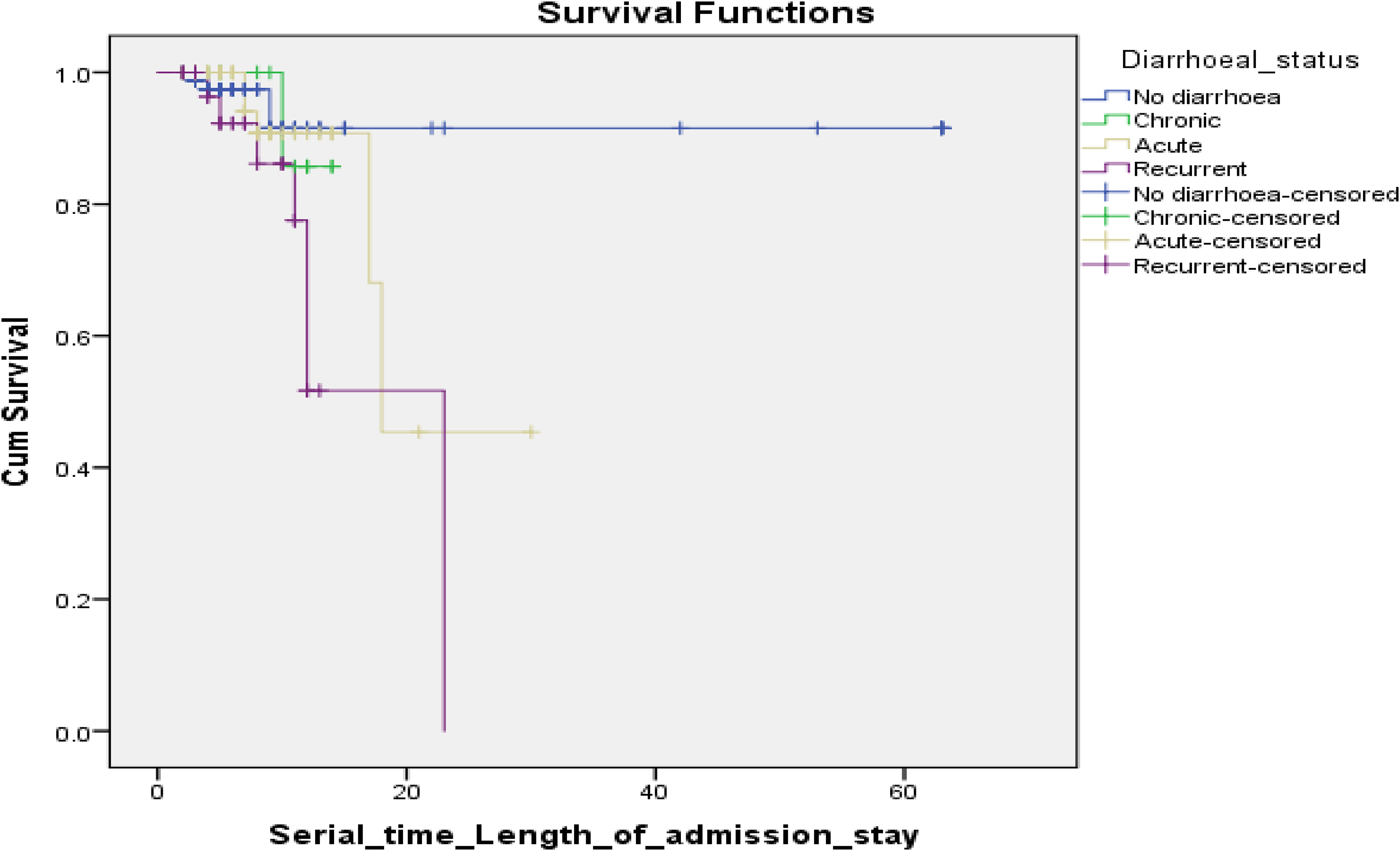
Kaplan-Meier plot of survival time of children with SAM admitted with diarrhea (N = 201). No diarrhea—(n = 88), Chronic—(n = 13), Acute—(n = 67), and Recurrent—(n = 33).
The log-rank test was used to test the null hypothesis that there was no difference between the categories in the probability of an event (death) during management at the stabilization centers. The log-rank test was carried out based on the same assumptions as the Kaplan-Meier estimation. The log-rank test showed that there was no significant difference in the probability of an event (death) between categories of sex, temperature, immunization Status, diarrheal frequency, ANC status, and child's access to CMAM center from residence (P < .05) (Table 4). However, the log-rank test showed significant differences in the probability of an event (death) between categories of diarrheal status (log-rank statistic = 9.760, P = .0021) and presence of existing disease (comorbidity) (log-rank statistic = 5.338, P = .021). Therefore, diarrheal status and existing disease (comorbidity) were further considered covariates in the multivariable Cox regression model.
Log-Rank Test of Significance for the Determinants of Outcome Measures Among Children With SAM at Stabilization Centers in Katsina State, Nigeria.

Abbreviations: ANC, ante natal care; CMAM, Community Management of Acute Malnutrition.
Are variables with the significant association on Log-rank and the assumption for Kaplan-Meier was met.
Comparison of Survival Curves
Determinants of Event (Mortality)
As depicted in Table 5, the study identified that severely malnourished children admitted with comorbidities showed significant association with time to event (death) P < .05, (AHR: 4.109, 95% CI: 1.51, 32.60). Thus, at admission, severely malnourished children with comorbidities had 4 times the mortality risk than severely malnourished children admitted without comorbidities.
Proportional Hazards Cox Regression Model Multiple Variable Analysis for the Determinants of Outcome Measures Among Children With SAM at Stabilization Centers in Katsina State, Nigeria.

Abbreviation: AHR, adjusted hazard ratio.
Study Limitations
Effect of Censoring—this study ended up with many censored values, especially from children that were cured 184 (91.5%) and 4 children (2%) were lost to follow-up. Thus, the large numbers of censored values decreased the equivalent number of subjects exposed (at risk), making the Kaplan-Meier estimates less reliable than they would be for the same number of subjects with less censoring.
Selection bias—There was a chance of selection bias occurring in the study because the 4 children lost to follow-up (default)
Confounding bias—It is possible for diarrhea to positively confound the association between comorbidity and the event (death)
Discussion and Recommendations
The finding of this study revealed a survival (recovery) rate of 89.6%, defaulter rate of 2%, and death rate of 8.5%. The mortality rate of 8.5% is below the 30% to 50% World Health Organization expected under-5 case-fatality rate for severe acute malnutrition. 30 The findings were similar to studies conducted in Northern Nigeria.,9,10 and Ethiopia. 31 Children with comorbidities at admission were 4 times more likely to die than children without comorbidities in the study, which is in line with the study done in Southern Ethiopia. 32 Conversely, a similar study in the same Ethiopian region did not show any significant association between comorbid conditions and mortality in SAM patients. The disparity was probably because of the small sample size used in the study. 33 Diarrhea, respiratory disease, malaria, measles, and anemia were the commonest forms of comorbidities recorded in the survey. A higher risk of inpatient mortality often results from a relatively defective immune status caused by severe acute malnutrition. Similar outcomes of complicated SAM were reported in Egypt, 34 in South Africa, 35 and Uganda. 36
Diarrhea was the most common comorbidity in patients at the CMAM centers. Treatment outcomes of patients without diarrhea are better than those with diarrhea. Over half (56.2%) of children hospitalized with SAM in the study had diarrhea, and over three-fourths (76.5%) of children that died had diarrhea during hospitalization. The treatment outcome of children without diarrhea was also better than those who had diarrhea. Children with diarrhea may be more vulnerable due to severe fluid loss, nutrient depletion, and serum electrolytes imbalance. Moreover, identifying dehydration in children with SAM may be challenging, leading to delay in initiating appropriate treatment, especially in resource-limited settings. This observed mortality pattern is comparable to a similar study in Kenya. 37 Promoting primary preventive measures are potent solutions to mitigate deaths from diarrhea among children with SAM. These interventions include routine immunization, provision of safe drinking water, adequate sanitation, and improved hygiene especially good infant feeding practices. Also, Exclusive breastfeeding and supplementation with vitamin A and zinc should be enhanced during hospitalization at the stabilization centers to reduce the severity of SAM, the onset of complications, and improve outcomes. More than 20% of patients of SAM among the study population had malaria, which is a significant cause of under-5 mortality in Nigeria and a common cause of anemia. These findings are in keeping with the studies done in Ethiopia, where malaria was a significant predictor of mortality.5,6 Integrated malaria control interventions along with appropriate nutritional and deworming interventions are essential in reducing mortality in SAM patients in the study area.
Routine immunization is one of the most cost-effective means of preventing infectious childhood diseases such as measles. The proportion of SAM patients in this study showed that more than 16% of patients had measles. Measles induces immunosuppression with associated vitamin A deficiency, leading to further susceptibility to other bacterial infections and mortality. High-quality, large-scale measles vaccination campaigns and strong routine immunization systems are critical to sustaining high population immunity to measles in the study area. About 10.5% of patients of SAM among the study population had respiratory diseases. Acute lower respiratory tract infections are significantly associated with morbidity and mortality among children below 5 years of age in Nigeria. 38 Almost half of the children with bronchopneumonia, the most typical form of acute lower respiratory tract infection, will require hospitalization. The disease kills approximately more than 140 000 children annually in Nigeria. 39 Studies have shown that SAM is associated with increased frequency and severity of bronchopneumonia, leading to mortality. Interventions such as promoting breastfeeding, routine immunization coverage, and personal hygiene can reduce the risk of children dying from pneumonia in the study area. Tuberculosis (TB) is another vital form of respiratory disease associated with malnutrition. TB predominantly affects children in resource-poor settings where it predisposes them to malnutrition. Conversely, the immunosuppressive impact of malnutrition increases the children's risk of developing TB. The stabilization centers in the study area will improve treatment outcomes through the screening, identification, and treatment of TB among children with SAM. Even though most caregivers were mothers, women's empowerment levels in Katsina State are shallow, especially in rural areas where malnutrition rates are high, which invariably contributes to low demand for health care services during illness. 40 The findings support an increased focus on early detection and treatment of children with medical comorbidities at the inpatient stabilization centers. This approach can be achieved through health workers' strict compliance with the WHO-recommended complicated SAM treatment protocol. 41 Likewise, through capacity building of health workers, the stabilization centers can enhance effective integrated management of medical conditions and nutrition interventions. The significant relationship between mortality and medical conditions among children with SAM supports the Nigeria Integrated Community Case Management of Childhood Illnesses (ICCM) strategy. The ICCM approach enables the assessment, classification, treatment, and referral of cases of the leading causes of mortality among children under 5 years in Nigeria. 42 Based on these findings, methodological implications for future research explore the relationships between the nutritional status of the children (anthropometric measurements), that is, edema, mid-upper arm circumference (MUAC), and weight for height (z-scores) and mortality. Furthermore, future research should consider conducting a facility-based survey to identify the associations between compliance with CMAM and ICCM protocols among health workers and the outcome of SAM at stabilization centers.
Conclusion
Death, recovery, and defaulter rates were all consistent with the acceptable SPHERE reference values, which state that recovery rate should be greater than or equal to 75%, defaulter rate should be less than or equal to 15%, and death rate should be less than or equal to 10%. 25 There were significant associations between the presence of comorbidities and mortality among children with SAM. Interventions to reduce deaths should focus on the early detection and effective management of comorbidities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors wish to declare that there is no conflict of interest or royalty associated with this study. The authors acknowledge, with gratitude, approval on the use of data from the Ministry of Health Katsina State, Nigeria for the sole purpose of this study.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.