
Abstract
Objective:
We surveyed patients who visited multiple outpatient specialty practices to understand what summary content was most helpful with the goal of optimizing meaningful outpatient clinical visit summary content.
Materials and Methods:
We constructed a survey instrument to measure delivery, use, and contents of clinical visit summaries. We surveyed patients who visited with at least 2 different outpatient medical specialties to understand preferences.
Results:
Most patients in our sample valued the summary information they received, and retained it as healthcare documentation (84%) and/or quick reference in supporting self-care (70%). Patients most commonly reported that information on results of completed tests (91%) and treatment plan instructions (89%) were very helpful. Additionally, patients expressed the importance of online access to clinical visit summary information.
Discussion:
Most patients used the clinical visit summary as healthcare documentation, and valued online availability of their summary information. Patients most often reported that information on results of recently completed tests and specific instructions on treatment plan were very helpful. Patients who sought further information after their visit most often looked to a provider and/or online.
Conclusions:
Patients valued clinical visit summary accessibility and as a reference tool to summarize care and provide next steps. Optimal clinical visit summaries might collate and integrate assessments and recommendations from multiple specialties into coherent care plans for patients.
Background and Significance
Patients are becoming clinically more complex and accumulating medical comorbidities. Sixty percent of US adults have multi-morbidity (2 or more medical conditions) which increases to 92% among individuals aged >65 years. 1,2 For patients interacting with the healthcare system, provider-patient communication is an important measure of healthcare quality 3 and, when done effectively, can improve health outcomes. 4
The provision of healthcare across multiple providers presents unique challenges to the achievement of coordinated and integrated care. Clinical visit summaries present an opportunity to supplement oral communication to enhance patient knowledge and engagement during and after clinic visits. 5 Additionally, clinical visit summaries have been endorsed through legislation as a means to empower patients to understand and manage their health and to promote secure exchange of health information to facilitate better clinical outcomes through increased transparency and efficiency. 6 Clinical visit summaries are provided to more than 50% of patients completing outpatient visits in the US. 5
The Centers for Medicare and Medicaid Promoting Interoperability Programs (formerly “Meaningful Use”) increased focus on interoperability and improving patient access to health information. 7 Clinical visit summaries, constructed under the premise of Meaningful Use, are offered after office visits to engage patients in their health and improve care coordination in the outpatient setting; this has generally been viewed as having a high degree of utility. 8 -15 However, they vary widely in format and included content and may be hard to use for some patients and caregivers. Patients have reported that information on medications and follow-up appointments are the most important knowledge enhancers of a clinical visit, however, these findings are reported from primary care or single specialty settings. 8 -10,12,15,16 A standard for providing summary information across specialties does not exist, and the perceived benefit and essential components of clinical visit summaries for patients receiving care from multiple specialties has not been defined.
Objective
We surveyed patients who visited a tertiary integrated medical center and had outpatient consults with multiple outpatient specialty practices to understand patient beliefs on what was most helpful with the goal of optimizing meaningful outpatient clinical visit summary content. We assessed delivery of the summary information, what information patients considered to be most helpful, and what additional information they sought after their visits.
Methods
Overview
We conducted an electronic survey of patients who received care from at least two different clinical outpatient specialties within a two-week period during their visit to Mayo Clinic in Rochester, MN. The goal of this study was to improve the quality of clinical care delivery, and therefore did not require IRB review.
Setting
The Mayo Clinic Department of Medicine (DOM) in Rochester, Minnesota is a large, integrated multi-specialty practice of 474 physicians serving more than 200,000 unique patients annually. Ten clinical specialty divisions of DOM include: allergic diseases and immunology; endocrinology; gastroenterology and hepatology; general internal medicine; hematology; infectious disease; preventive, occupational, and aerospace medicine; pulmonary; sleep medicine; and rheumatology. Providers across DOM work in similar staffing models, and share a reporting infrastructure through departmental leadership. The DOM is a tertiary medical practice providing consultations for patients from across the United States as well as 137 countries who are seeking care for complex, multi-morbid, or rare diseases.
Subjects
Patients who had seen at least two different clinical specialties during their visit to Mayo Clinic were selected to receive a survey via email. Patient demographics and visit information were collected using institutional data sources. Patients were sampled with the following criteria: 1) an initial visit in one of the DOM specialties two months prior to survey launch; 2) at least one additional outpatient, non-procedural outpatient clinic visit within two weeks of the index visit; 3) had no visits to any specialties in the two weeks immediately following their last visit; 4) valid email address on file. To assess for non-response bias, we compared the demographic information of respondents to those who did not respond to our survey.
Survey Development
We developed a survey instrument that was used to perform a cross-sectional assessment for patients who had seen multiple different clinical specialties. We electronically deployed our survey using Qualtrics (Provo, Utah).
Survey Instrument
We constructed a new survey instrument with 42-items including three domains: patient receipt of clinical visit summary materials, patient satisfaction with these materials, and gaps in the information provided on received clinical visit summary materials (Supplemental File 1).
Information Delivery and Use
Our previous work highlighted moments during visits where patients received information from their providers as drivers of positive patient experience. 17 In order to capture patient views on this, we asked a series of questions on whether the patient received information on test(s) related to their condition, the medication(s) received during their encounter with Mayo Clinic, and explanations provided for the patient’s diagnosis or medical condition. If patients indicated that they received written information on any of these three topics, we then asked whether it met their needs, and what they did with the information they received. We also asked about use of summary information, including review with a provider and availability of their summary information through access to their electronic health record [EHR] through the online patient “portal.”
Informational Content
In order to understand which summary information patients valued, we asked survey responders to rate individual content items from “Very Helpful” to “Not Helpful” on a four-point Likert scale. Individual items represented content already present on the Epic® After Visit Summary form (Epic Systems, Madison, WI), and content found within a review of published, academic literature on clinical visit summaries. 8 -12,14 -16, 18, 19 We did not require a response indicating that the patient had received summary materials in order to respond to these questions in order to understand not only which received summary items were most helpful, but also what patients would have liked to receive as summary information. Differences in ratings of helpfulness were assessed for patients who saw two specialties compared with those who saw three or more specialties. Bivariate analyses with Chi-square test were used with significant association determined when p-values less than 0.05. All data management and statistical analyses were performed using Statistical Analysis Software (SAS) Version 9.4 (Cary, NC).
Additional Information Sought
In order to understand information gaps, we asked patients who reported receiving summary information whether they sought additional information regarding their condition and medication(s). If respondents indicated that they had looked for additional information, we then asked what type(s) of information the patient sought and where they sought this information with two open-ended questions. Qualitative review and coding of this information, as well as any additional patient comments was completed by three of the authors (PR, DR, LP) for thematic synthesis.
Results
A total of 2,093 patients met criteria for inclusion. Of those, 886 had a valid email address on file and were emailed a survey. We received 252 responses (response rate: 28%) (Table 1).
Survey Respondent Characteristics (N = 252).
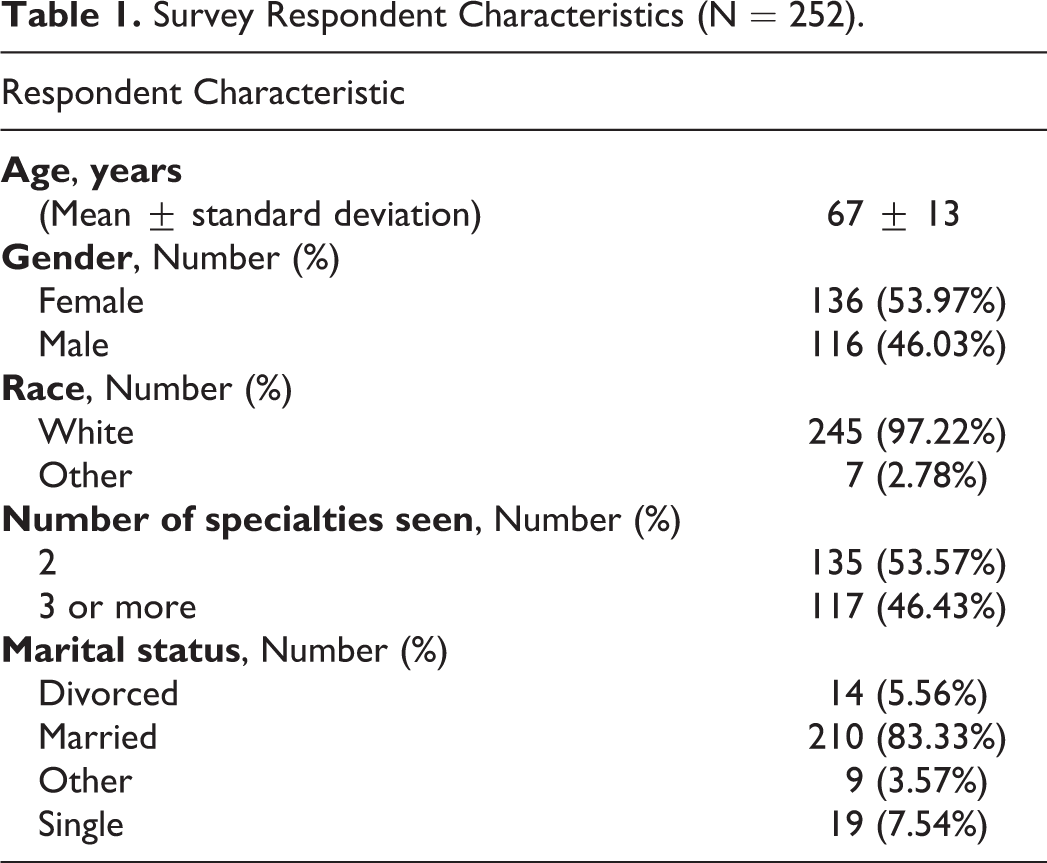
More than one-half of respondents were 66-84 years of age. Respondents were predominantly white (97%), female (54%), and married (83%). The majority of respondents indicated “Very Good” (34%) or “Good” (25%) health. Patients more commonly saw providers in the following specialties: General Internal Medicine (15%), Cardiovascular Medicine (14%), and Pulmonary Medicine (11%).
Respondents were significantly older than non-respondents (67 ± 13 years vs. 60 ± 15 years; p < 0.001) (Supplemental File 2). No statistically significant difference was observed in the distribution of gender, marital status, race, or ethnicity between respondents and non-respondents.
Information Delivery and Use
Most respondents reported receiving written summary information on tests completed (73%), new medications (60%), or medical condition (71%). More than 90% of these patients reported that their needs were met with the summary information they received. The majority of patients who received clinical visit summaries kept them as documentation of their care (84%), and/or used them as a quick reference for medications or next steps (70%) (Figure 1).
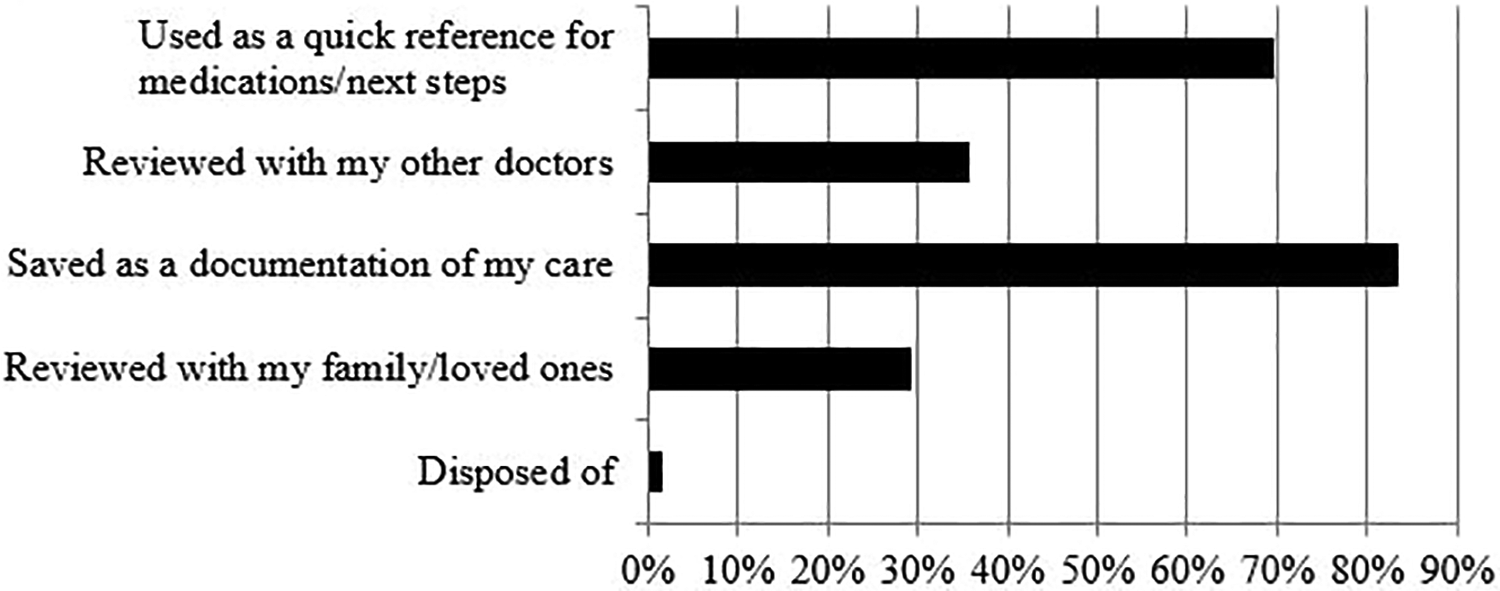
Use of clinical visit summary (n = 252).
Overall, patients believed that online accessibility of summary information was very helpful (Table 2).
Patient Beliefs Regarding Helpfulness of Clinical Visit Summary Delivery, Use, and Informational Content (N = 252).

One patient noted:
All of my responses are based on the information I access on my patient portal, which I prefer over printed information which is easily lost and misplaced.
Always provide a paper copy of the visit summary to the patient before they leave. It is unbelievable how many times I knew I had been listening but went back to review the summary and missed a few important pieces.
Indeed this is a very important challenging area especially for patients who are keen in taking care of their health and conducting the necessary follow-up at home, with their Primary Care provider(s) and specialists…
Especially when you are seen by multiple departments it would be helpful to have a final visit with a physician to review all the results and discuss any needed follow ups. Posting the results of all visits/phone calls on the online portal would help me and my local physicians better understand the results and any recommended follow up.
…each summary from each doctor contains the lengthy synopsis of information of my condition. For maintaining records, I would have preferred that this synopsis appear on the primary physician’s report, rather than on each report. Particularly when sharing info back home with various physicians…
Informational Content
Patients most commonly reported that results of completed tests (91%) and treatment plan instructions (89%) were very helpful (Table 2). Individual items more commonly deemed “not helpful at all” were Information on how to log into the portal (14%) and list of allergies (11%). We did not find any significant association between ratings of helpfulness for summary items, and patients who saw two specialties as opposed to three or more specialties.
Additional Information Sought
More than a third (38%) of patients who reported that they received summary information indicated that they had searched for further information on their condition or treatment after their visit, and commonly looked to a medical professional (51%) or online for this information (29%). Patients commonly looked for information on dosing or side effects of medications (38%), clarification on a question (34%), or information on treatment recommendations (13%). Patients noted:
For a newly prescribed medicine the name, dosage and frequency of usage….
I always want to know as much as possible about my meds.
Discussion
We observed that most patients used the clinical visit summary as healthcare documentation and that they valued online availability of their summary information through access to their electronic health record. Patients most often reported that information on results of recently completed tests and specific instructions on treatment plan were very helpful. Additionally, patients reported that summary items such as list of allergies and immunization history were the least helpful. Patients who sought further information after their visit most often looked to a provider and/or online.
We observed that most patients used the clinical visit summary as a documentation of care which can facilitate improved communication with other care providers. Patients review their doctors’ notes to be better prepared for clinic visits, remember their care plan better, and feel more in control of their health. 20 -23 Review of the clinical visit summary with a care team member was suggested by patients in our study. This engagement may be a way to prompt clarifying questions and discussion, and help to resolve the need for patients to seek information after the visit. Furthermore, aligning patient and provider views to reach common ground in establishing and adhering to a care plan can improve patient experience. 24
Federman et al 12 found that both patients and providers viewed the utility of the clinical visit summary in communicating health care information, guiding self-management, and relaying information about specific health care–related tasks to complete. While patients in this study were not satisfied with the EHR-generated visit summary, they valued them as a mode for communicating medical information if they saw subsequent clinicians.
Our observation that the vast majority of patients valued having access to the clinical visit summary through their EHR is consistent with previous literature. Patients who accessed their clinical information online through their EHR strongly believed that they would be able to access their clinical information quickly and efficiently, track visits and tests, and reinforce their understanding of physicians’ instructions. 8,9,11,12,14 -16,19,25 Similarly, a randomized study by Pavlik et al 15 found that satisfaction with the clinical visit summary was significantly associated with online access through the electronic medical record.
Clinical visit summaries may be especially important for patients with multiple medical comorbidities. Black et al 18 conducted a purposive sample of patients with a chronic health condition to participate in focus groups on clinical visit summary preferences, with the understanding that these patients may have more complicated communications with multiple providers involved in their care. Patients who kept the clinical visit summary described its value as an information source, and desired health data elements included medication side effects, device use, and information from multiple specialties participating in their care. One of our patients highlighted the importance of a final visit review after being evaluating by multiple subspecialties. Our observations and extant literature suggest that optimal clinical visit summaries collate and integrate assessments and recommendations from multiple specialties into coherent care plan for patients.
Our study has several strengths. First, we were able to leverage institutional appointment data and send surveys to patients who had seen multiple outpatient specialty providers 14 days after their visits took place, thereby limiting recall bias. Second, we did not direct responding patients to a particular form or format of clinical visit summary information and instead kept questions open to any summary information they may have received during their visits, or would have liked to receive. This allowed us to focus data capture on what content was most valuable for these patients.
Our study has several limitations. First, the smaller sample size and single institution study setting which may limit broad generalizability of our findings. However, we observed that the health information type preferences identified in our sample are consistent with other studies. Additionally, thematic synthesis allowed for further insight into patient preferences. Second, as the focus of this study was on preferred content areas, we were not able to account for material type and lexical considerations with format or readability of any summary materials received by patients, which may impact the perceived helpfulness of clinical visit summary materials. We were also not able to account for highest achieved education level of patients in our analyses, as this information was missing for most. Finally, uniform use of the helpful scale to rate summary information types may have resulted in decreased power to discriminate the utility of information.
Conclusion
Our study assessed clinical visit summary information needs of patients who visited multiple specialties and is highly relevant to a growing population of patients managing multiple morbidities. Clinical visit summary materials may be more impactful for patients facing greater burden of disease to facilitate comprehensive care plans across specialties and support self-management of disease. Future work should advance methods for tailoring of clinical visit summary to patient desired informational elements.
Supplemental Material
Supplemental Material, Dismissal_Survey - Helpfulness of Clinical Visit Summary Content From Multi-Specialty Care: A Mixed-Methods Assessment
Supplemental Material, Dismissal_Survey for Helpfulness of Clinical Visit Summary Content From Multi-Specialty Care: A Mixed-Methods Assessment by Priya Ramar, Daniel L. Roellinger, Roma F. Merrick, Jon O. Ebbert and Lindsey M. Philpot in Health Services Research and Managerial Epidemiology
Supplemental Material
Supplemental_2 - Helpfulness of Clinical Visit Summary Content From Multi-Specialty Care: A Mixed-Methods Assessment
Supplemental_2 for Helpfulness of Clinical Visit Summary Content From Multi-Specialty Care: A Mixed-Methods Assessment by Priya Ramar, Daniel L. Roellinger, Roma F. Merrick, Jon O. Ebbert and Lindsey M. Philpot in Health Services Research and Managerial Epidemiology
Footnotes
Authors’ Note
All manuscript authors qualify for authorship of this study, and have participated in the conceptualization or design of the work (P.R., R.F.M., J.O.E., L.M.P.), data collection (R.F.M., D.L.R.), data analysis and interpretation (P.R., D.L.R.), drafting the article (P.R., D.L.R., J.O.E., L.M.P.), critical revision of the article (P.R., D.L.R., R.F.M., J.O.E., L.M.P.), and final approval of the version to be published (P.R., D.L.R., R.F.M., J.O.E., L.M.P.).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Robert D. and Patricia E. Kern Center for the Science of Healthcare Delivery and the Mayo Clinic College of Medicine and Science.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.