
Abstract
Background:
Sepsis is a life-threatening syndrome and a leading cause of morbidity and mortality representing significant financial burden on the health-care system. Early identification and intervention is crucial to maximizing positive outcomes. We studied a quality improvement initiative with the aim of reviewing the initial management of patients with sepsis in Canadian community emergency departments, to identify areas for improving the delivery of sepsis care. We present a retrospective, multicenter, observational study during 2011 to 2015 in the community setting.
Methods:
We collected data on baseline characteristics, clinical management metrics (triage-to-physician-assessment time, triage-to-lactate-drawn time, triage-to-antibiotic time, and volume of fluids administered within the first 6 hours of triage), and outcomes (intensive care unit [ICU] admission, in-hospital mortality) from a regional database.
Results:
A total of 2056 patients were analyzed. The median triage-to-physician-assessment time was 50 minutes (interquartile range [IQR]: 25-104), triage-to-lactate-drawn time was 50 minutes (IQR: 63-94), and triage-to-antibiotics time was 129 minutes (IQR: 70-221). The median total amount of fluid administered within 6 hours of triage was 2.0 L (IQR: 1.5-3.0). The ICU admission rate was 36% and in-hospital mortality was 25%. We also observed a higher ICU admission rate (51% vs 24%) and in-hospital mortality (44% vs 14%) in those with higher lactate concentration (≥4 vs ≤2 mmol/L), independent of other sepsis-related parameters.
Conclusion:
Time-to-physician-assessment, time-to-lactate-drawn, time-to-antibiotics, and fluid resuscitation in community emergency departments could be improved. Future quality improvement interventions are required to optimize management of patients with sepsis. Elevated lactate concentration was also independently associated with ICU admission rate and in-hospital mortality rate.
Background
Sepsis is a life-threatening syndrome and a leading cause of morbidity and mortality worldwide. 1 It also represents a significant financial burden on the health-care system, incurred through high care needs and lengthy admissions, oftentimes in the intensive care unit (ICU). As with other medical emergencies such as myocardial infarction, stroke, and trauma, early identification and intervention are crucial to maximizing positive outcomes. Rapid administration of antibiotics was found to be associated with lower in-hospital mortality, 2 and hemodynamic resuscitation has shown benefit if delivered within the first 6 hours of presentation. 3 Thus, current guidelines recommend administering empiric broad-spectrum antibiotics within the first hour of recognition of septic shock and achieving fluid resuscitation goals within the first few hours. 4 However, early identification of patients with sepsis can be challenging as clinical signs and symptoms of sepsis can be varied, subtle, and nonspecific, such as fever, chills, tachycardia, and tachypnea.
In this study, we sought to review the metrics of sepsis care delivery in community emergency departments as part of a quality improvement initiative and to determine areas that could be addressed to better improve the initial management of sepsis and subsequent outcomes. Specifically, we focused on the triage-to-physician assessment time, triage-to-lactate-drawn time, triage-to-antibiotics time, and the volume of fluid administered within the first 6 hours of triage, as well as the clinical outcomes of ICU admission and in-hospital mortality.
Methods
Study Design and Setting
We conducted a retrospective, multicenter, observational cohort study of patients presenting to 3 community emergency departments in the Niagara Region, Ontario, Canada, from July 2011 to July 2015.
Patient Population
Inclusion criteria included: inclusion in the regional sepsis database (which includes all patients who present to the emergency departments and are diagnosed with sepsis by the treating physician). Exclusion criteria included: (1) missing data fields as outlined in the “Data Collection” section and (2) pediatric patients (age <18 years).
The diagnosis of sepsis was based on emergency department physician assessment. However, each case was subsequently reviewed automatically by an electronic health information management system, as well as manually by a dedicated study nurse or an infectious disease specialist. The criteria by which these quality checks were done were based on the systemic inflammatory response syndrome (SIRS) criteria for sepsis. 5 Cases that did not receive a diagnosis code of sepsis by the emergency department physician but met SIRS criteria, or vice versa, were queried to the treating physician to verify whether or not the case should truly be diagnosed as sepsis for inclusion into the database.
Data Collection
The data used in this study were part of a quality improvement initiative to assess the management of patients with sepsis and identify opportunities for improvement. A dedicated regional sepsis coordinator (registered nurse) retrospectively collected data on demographics (eg, age, sex) and clinical (eg, systolic blood pressure, heart rate, respiratory rate, altered mental status, urine output), laboratory (eg, lactate, leukocyte count, platelets, international normalized ratio, total bilirubin, creatinine), management, and outcome parameters (eg, time of triage, time of physician assessment, time of blood collection, time of antibiotics, antibiotic choice, total fluids administered within the first 6 hours of triage, vasopressor use, hospital length of stay, ICU admission, and in-hospital mortality). Patient records that had missing data with respect to key management parameters (eg, time of triage, time of antibiotics, total fluids administered, ICU admission, and in-hospital mortality) were excluded from analysis. De-identified data are available upon reasonable request from the corresponding author.
Data Analysis
Descriptive data are presented as medians with interquartile ranges (IQRs) for continuous data and frequencies (percentages) for categorical data. Patients were stratified into 3 groups based on their initial lactate concentration: low lactate group (≤2.0 mmol/L), moderate lactate group (>2.0 to <4.0 mmol/L), and high lactate group (≥4.0 mmol/L). This stratification was based on the finding that a serum lactate ≥4.0 mmol/L is unusual in normal and noncritically ill hospitalized patients, regardless of underlying comorbidities, 6 and a recent study demonstrating that a lactate threshold of ≥2.0 mmol/L should be used as an indication for the initiation of specific intervention and monitoring for sepsis. 7
We compared outcome data, ICU admission rate, and in-hospital mortality among the 3 lactate groups using χ2 test. Multivariable logistic (for categorical outcomes) regression was used to adjust for potential confounders in assessing the association between initial lactate concentration and ICU admission rate, and in-hospital mortality. The following variables were considered as potential confounders as they are related to severity of illness and were adjusted for in all multivariable models: systolic blood pressure, vasopressor use, heart rate, respiratory rate, temperature, altered mental status, urine output, 4,8 and leukocyte count. All P values were 2 sided and statistical significance was defined as P < .05. Statistical analyses were performed using R statistical software (version 3.2.2).We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) cohort checklist when writing our report. 9
Results
A total of 2056 patients were analyzed (Figure 1; Table 1). The median triage-to-physician-assessment time was 50 minutes (IQR: 25-104), triage-to-lactate-drawn time was 50 minutes (IQR: 63-94), and the triage-to-antibiotics time was 129 minutes (IQR: 70-221; Table 2). The median total volume of resuscitative fluids administered in the first 6 hours of triage was 2.0 L (IQR: 1.5-3.0). The ICU admission rate for all patients was 35.9%, and the in-hospital all-cause mortality rate for all patients was 24.7%. The median hospital length of stay for patients discharged from hospital was 9 days (IQR: 4-15). Aggregate data on the antibiotics used are also provided (Supplemental Table).

Study patients meeting inclusion and exclusion criteria.
Baseline Characteristics of Study Patients.

Abbreviations: HR, heart rate; INR, international normalized ratio; IQR, interquartile range; PTT, partial thromboplastin time; RR, respiratory rate; SBP, systolic blood pressure; SIRS, systemic inflammatory response syndrome; WBC, white blood cell leukocyte count.
Clinical Management Metrics and Outcomes of Study Patients.
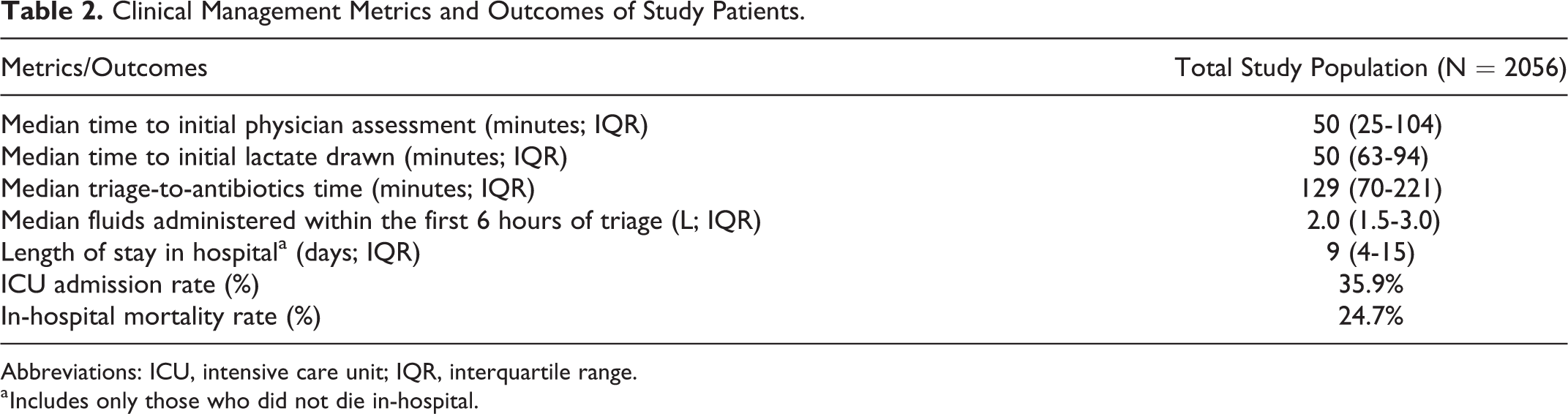
Abbreviations: ICU, intensive care unit; IQR, interquartile range.
a Includes only those who did not die in-hospital.
We also stratified patients to a low lactate group (n = 761), moderate lactate group (n = 691), or high lactate group (n = 604; Table 1). χ2 Testing demonstrated statistically significant differences in the ICU admission rate and in-hospital mortality rate between the 3 lactate groups (P < .001). Specifically, patients in the high lactate group had an ICU admission rate of 51.0% (n = 308), compared to 23.9% (n = 182) in those in the low lactate group (Table 3). Patients in the moderate lactate group also had an increased rate of ICU admission of 35.9% (n = 248), although not as high as those in the high lactate group. After adjusting for potential confounders, the odds ratio for ICU admission for patients in the moderate and high lactate group were 1.54 (95% confidence interval [CI]: 1.20-1.97) and 2.03 (95% CI: 1.55-2.65) respectively, when compared with those in the low lactate group.
Results of Univariate and Multivariate Logistic Regression Models for Intensive Care Unit Admission and In-Hospital Mortality.a
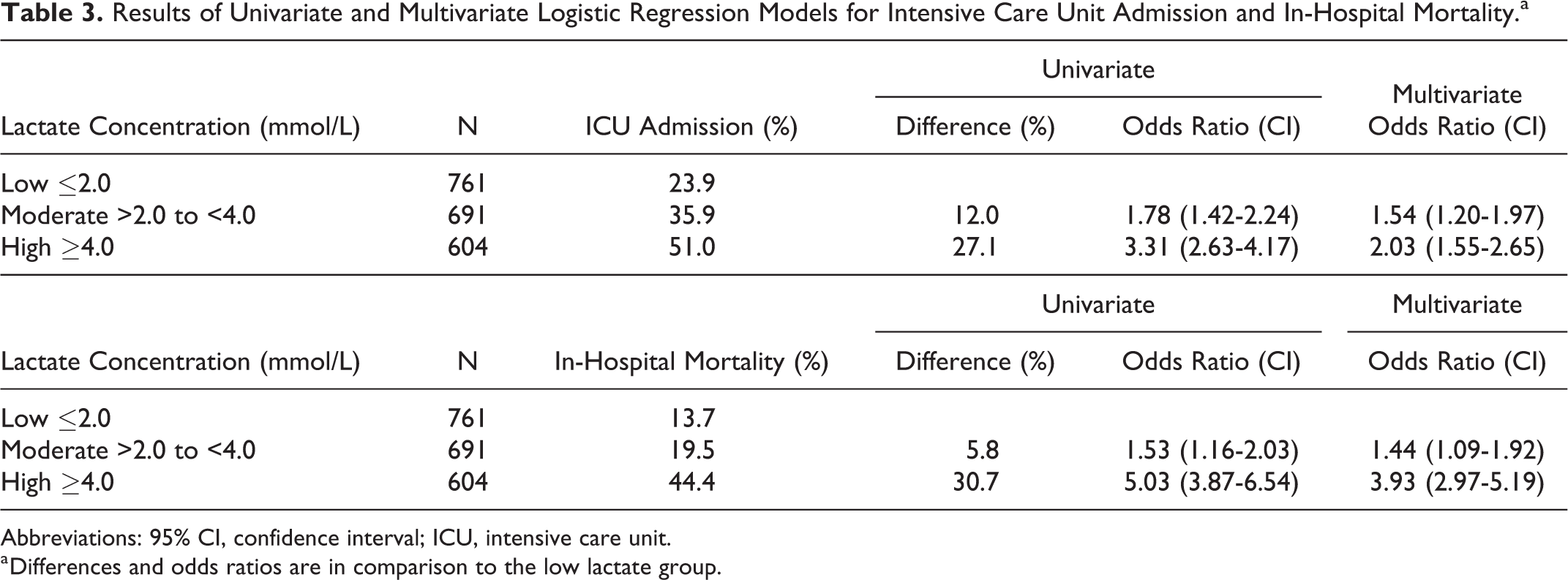
Abbreviations: 95% CI, confidence interval; ICU, intensive care unit.
a Differences and odds ratios are in comparison to the low lactate group.
Similarly, patients in the moderate and high lactate groups had an in-hospital mortality rate of 19.5% and 44.4%, respectively (n = 135 and 268), compared to 13.7% (n = 104) in those in the low lactate group (Table 3). After adjusting for potential confounders, the odds ratio for in-hospital death in patients in the moderate and high lactate groups were 1.44 (95% CI: 1.09-1.92) and 3.93 (95% CI: 2.97-5.19) respectively, compared to those in the low lactate group.
Discussion
Our study summarizes the metrics of sepsis care delivery at 3 community hospitals in Canada from 2011 to 2015 and found that there is room for improvement in key management parameters. Specifically, the average time-to-antibiotics was 129 minutes, which exceeds the Surviving Sepsis Campaign recommendations of administering empiric antibiotics within an hour of sepsis recognition. Additionally, given the importance of early recognition of sepsis such that appropriate management can be initiated, the average time-to-physician assessment and time-to-lactate-drawn of 50 minutes represents aspects of sepsis care that should be improved.
Current sepsis guidelines recommend fluid resuscitation of 30 mL/kg in the first 3 hours based on the Protocolized Care for Early Septic Shock (ProCESS) and Australasian Resuscitation in Sepsis Evaluation trials (ARISE), which averaged to 2 L in the PROMISE trial. 10 -12 This is a strong recommendation but based on low quality evidence. Our study also demonstrated a median of 2 L but over 6 hours, which was a design of the database at the time of development. Therefore, while direct comparisons cannot be made to the guidelines, it can be at least inferred that the average patient in this study received the recommended fluid volume at best, but realistically likely received less.
Our study also found an ICU admission rate of approximately 36% and an average hospital length of stay of 9 days. While we do not delineate how much time is spent in the ICU or a noncritical care unit, these results nonetheless confirm that sepsis care requires significant hospital resources. The in-hospital mortality rate was found to be approximately 25%, further demonstrating the clinical severity of sepsis and the importance of proper recognition and treatment to avoid negative outcomes.
We recognize that there is a spectrum of illness severity in sepsis and thus further analyzed our clinical outcome data with stratification of patients into low, moderate, and high lactate groups. Consistent with existing literature, 13 we demonstrated that the clinical outcomes of ICU admission and in-hospital mortality were significantly worse in patients with higher lactate concentration than those with low lactate concentration. Our multivariate analysis demonstrates that these associations were independent of other clinical indicators of sepsis including systolic blood pressure, heart rate, respiratory rate, temperature derangements, mental status changes, oliguria, abnormal leukocyte count, and vasopressor use.
While in-hospital processes such as triage, physician assessment, bloodwork, sample processing, and antibiotic dispensing represent potential delays to timely treatment, a potential strategy to shorten delay to treatment is to have therapy initiated prior to patient arrival to the hospital. A study by Seymour et al found that more than 40% of severe sepsis hospitalizations (from a total of 13 249 cases) in a community-based cohort were patients who presented via emergency medical services (EMS) transport, with 80% of cases diagnosed upon admission. 14 Given the importance of early intervention and treatment, the prehospital interval (while the patient is in the care of EMS personnel) represents a potential opportunity for the recognition and initiation of sepsis care. Indeed, there is an ongoing study of prehospital initiation of antibiotics by EMS personnel on sepsis outcomes (ClinicalTrials.gov Identifier: NCT03068741).
Another barrier to more timely intervention includes the aforementioned fact that identification of patients with sepsis can be challenging given its nonspecific signs and symptoms. Serum lactate is a widely adopted biomarker in helping clinicians identify the severity of illness in patients with sepsis. However, as demonstrated in this study, there are barriers to obtaining lactate in a timely manner to help support sepsis recognition and clinical decision-making. One potential solution to overcoming this obstacle is through the use of point-of-care (POC) lactate testing. The POC fingertip testing for lactate measurement has been shown to correlate well with standard laboratory lactate analyzers. 15 Its turnaround time is also very rapid (<10 minutes) 15 and can be made available for use in the emergency department or in the prehospital setting by EMS personnel.
Limitations
Sepsis cases in this study were identified at the discretion of the treating emergency physicians, which can lead to significant variability given the challenge of diagnosing sepsis upfront. In an effort to promote standardization, we used the SIRS criteria retrospectively to capture potential cases of sepsis, which we acknowledge is poorly specific but has better sensitivity than quick Sequential Organ Failure Assessment (qSOFA).
16
Furthermore, SIRS criteria were selected because parameters defined in the Sepsis-3 definition
17
such as Pa
While our multivariate logistic regression takes into account common clinical signs and laboratory measures of severity of illness, our in-hospital mortality data were not specifically adjusted for the severity of illness and include all causes of in-hospital mortality and not just sepsis-related mortality. It should also be acknowledged that baseline renal and liver dysfunction influences the kinetics of serum lactate, and this was not accounted for in the analysis.
Conclusions
Time-to-clinician assessment and time-to-antibiotics metrics in community emergency departments need to be further improved to improve patient outcomes in sepsis care. As such, future quality improvement interventions are required to optimize the management of patients with sepsis. This study also reaffirms that initial serum lactate concentration is an independent factor associated with higher ICU admission rates and all-cause in-hospital mortality in patients with higher lactate concentration.
Supplemental Material
Supplemental Material, Health_Services_Research_Lactate_Supplemental_File - Management of Patients With Sepsis in Canadian Community Emergency Departments: A Retrospective Multicenter Observational Study
Supplemental Material, Health_Services_Research_Lactate_Supplemental_File for Management of Patients With Sepsis in Canadian Community Emergency Departments: A Retrospective Multicenter Observational Study by Victor C. K. Lo, Haitong Su, Yuet Ming Lam, Kathleen Willis, Virginia Pullar, Matthew Kowgier, Ryan P. Hubner and Jennifer L. Y. Tsang in Health Services Research and Managerial Epidemiology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.