
Abstract
Background:
Since the 1980s, Stenotrophomonas maltophilia has emerged as an important pathogen associated with significant mortality in pneumonia and bacteremia of severely immunocompromised, hospitalized patients. The drug of choice in S maltophilia infections is sulfamethoxazole-trimethoprim (SMX/TMP); SMX/TMP resistance is a serious concern in clinical practice. The aim of this study was to assess the prevalence of S maltophilia in lower respiratory tract (LRTI) samples at a tertiary-care university hospital.
Methods:
This retrospective cohort study was carried out using microbiological data collected between January 2008 and December 2017. Routine antimicrobial susceptibility testing was performed for SMX/TMP and levofloxacin; in case of resistance, susceptibility testing for additional antibiotics (tigecycline, amikacin, and colistin) was also performed.
Results:
A total of 579 individual S maltophilia isolates were identified (2008-2012: n = 160, 2013-2017: n = 419; P = .0008). In all, 78.46% of patients were younger than 5 or older than 50 years of age and had recent trauma, surgery, or underlying conditions (malignancies, respiratory distress syndrome, congenital disorders, and cystic fibrosis). In 28.16% of samples, more than 1 pathogen was identified, and 5.35% of coisolated pathogens were multidrug resistant (MDR). In all, 12.1% of isolates were SMX/TMP-resistant (2008-2012: 6.12%, 2013-2017: 18.06%; P = .034), while 8.99% were resistant to levofloxacin (2008-2012: 7.86%, 2013-2017: 10.12%; P > .05). SMX/TMP resistance was detected more frequently in samples originating from inpatients (n = 2.50 ± 2.39 vs n = 11.50 ± 3.76; P = .0002).
Conclusions:
In all, 5.87% of isolates were extensively drug resistant (XDR), that is, in addition to SMX/TMP, they were resistant to levofloxacin, amikacin, colistin, and tigecycline. The results of our study correspond to the findings in the literature.
Keywords
Introduction
Stenotrophomonas maltophilia is a nonfermenting Gram-negative rod that is ubiquitous in nature (predominantly occurring in aquatic environments and on plants) 1 . Biochemically, it is catalase positive and oxidase negative, and it produces acid from maltose (hence the name “maltophilia”). 2,3 Due to its charged cell wall surface and biofilm production, it may attach to and survive on abiotic surfaces in clinical settings (eg, central venous catheters, disinfectant and hand-washing solutions, solutions for hemodialysis, endoscopes, inspiration/expiration circuits of ventilators, nebulizers, tap water, and showerheads). 1,4 –7 This pathogen is frequently responsible for nosocomial outbreaks, especially in intensive care units (ICUs). 6,8,9 Before the 1980s, there have been seldom reports of the isolation of this microorganism in the context of human infections 10 ; however, after the 1980s, the prevalence of nosocomial infections associated with S maltophilia has increased rapidly. 11 On the one hand, S maltophilia is a pathogen of low virulence and limited invasiveness; therefore, bypassing the natural defenses of the body is crucial for the development of any pathologies. 1,4,10 –12 Advancements in medical interventions (complex surgeries, chemotherapy of advanced malignancies, immunosuppressive therapy for organ transplantation, or autoimmune disorders) have also resulted in the increase in the number of patients at risk. 1,4,10 –12 Nonetheless, advancements in the identification methods in clinical microbiology laboratories (eg, polymerase chain reaction, mass spectrometry, and sequencing) have allowed for the more precise identification of this pathogen. 13 –15 To complicate things even further, the prevalence of community-acquired S maltophilia infections (presumably due to the increase in the number of immunocompromised/debilitated patients in outpatient care settings) has also increased since the 2000s. 16
The main clinical manifestations of S maltophilia infections include nosocomial lower respiratory tract infections (LRTIs; namely, tracheobronchitis/pneumonia, usually associated with mechanical ventilation) and bacteremia. Nevertheless, other manifestations, for example, wound/soft tissue infections (ie, ecthyma gangrenosum), cellulitis, mastoiditis, meningitis, peritonitis, bone and joint infections, urinary tract infections, conjunctivitis, and otitis media have also been described. 4,9 –11 These infections usually occur in severely debilitated, immunosuppressed individuals, in addition to patients with a chronic illness or a developmental abnormality affecting a specific organ system. 4,9 –11,17 –19 Stenotrophomonas maltophilia represents the fourth most common pathogen among nonfermenting gram-negative bacteria (following Pseudomonas aeruginosa, Acinetobacter spp, and Burkholderia cepacia complex), with a reported incidence of 7.1 to 37.7 cases/10 000 discharges (regarding nosocomial infections) 20 . Stenotrophomonas maltophilia infections are associated with a high crude mortality of 25% to 75% in case of pneumonia and 20% to 60% in case of bacteremia. 3 The mortality rate increases sharply if the patients receive inappropriate antimicrobial therapy (which mainly occurs empirically) 3,4,9 –11 .
Stenotrophomonas maltophilia may colonize the respiratory tract and persist in the sputum of these patients for a long period of time; therefore, it may be difficult to ascertain the clinical significance of a positive culture result from the microbiology laboratory. 21,22 However, previously verified colonization is one of the main risk factors for manifestation of S maltophilia LRTI; thus, culture positivity for this microorganism does pertain clinically useful information. 6,21,22 While some reports suggest that S maltophilia LRTIs are characterized by the lack of acute inflammatory response, Di Bonaventura et al found an pronounced inflammatory response (increased expression of IL-8 and TNF-α) in murine airway epithelial cells and macrophages, which may contribute to airway inflammation in vivo. 23,24 Histologically, S maltophilia LRTIs are frequently characterized by focal lung necrosis and lung hemorrhage, while pleural effusions and cavitations are rarely observed. 20 As many S maltophilia infections are polymicrobial, clinicians should be extremely cautious when interpreting radiological findings (especially in patients with cancer), as several copathogens (eg, Pseudomonas spp, Acinetobacter spp, Nocardia spp, Staphylococcus aureus, and opportunistic fungi) may be present simultaneously. 1,4,10 –12 In severely immunosuppressed patients, fatal hemorrhagic pneumonia may occur, which is the fulminant course of the infection. 10 –12 In addition, S maltophilia is a well-known colonizer and pathogen in patients with cystic fibrosis (CF); it has been described that the colonization/infection rate (especially in 105-106 CFU) correlates well with disease progression and loss of lung function. 25,26 Air-borne transmission of this microorganism from the cough (aerosol) of patients with CF have also been described. 25,26
The therapeutic options regarding S maltophilia infections are very limited, owing to the intrinsic resistance of this pathogen to several classes of antibiotics: β-lactam antibiotics (most notably carbapenems) are hydrolyzed by zinc-dependent, chromosomally mediated β-lactamases (namely, L1 and L2), aminoglycosides (acetyl-transferases and temperature-dependent changes in the lipopolysaccharide), while a plethora of other drugs may be affected by the overexpression of energy-dependent efflux pumps. 4,7,9 –11,20 Currently, the therapy of choice in these infections is a high-dose sulfamethoxazole/trimethoprim (SMX/TMP; cotrimoxazole) 1,9 –11 . Although a recent publication by Ko et al has reported that fluoroquinolones (a popular alternative to cotrimoxazole) are equally effective in the therapy of these infections 27 , SMX/TMP resistance (among other things, as drug allergies may also be present) is a serious therapeutic challenge for clinicians. Due to the proclivity of this microorganism to become multidrug resistant (MDR) and extensively drug resistant (XDR), it has been listed by the World Health Organization as one of the most concerning multidrug resistant organisms worldwide. 28 Apart from SMX/TMP and fluoroquinolones, other drugs that may be considered for therapy (and several case reports are available in successfully curing patients) are the tetracyclines (doxycycline, minocycline, and tigecycline), ticarcillin/clavulanate, ceftazidime, colistin, and chloramphenicol 4,7,9 –11,20 .
Despite the abundance of global surveillance studies published, there are only few reports assessing the microbiological and clinical significance of S maltophilia in LRTIs, as the majority of studies have focused on the isolation of MDR Pseudomonas spp and Acinetobacter spp. The aim of this study was to assess the prevalence of S maltophilia in respiratory tract specimens at a tertiary-care hospital in Hungary retrospectively, during a 10-year study period (2008-2017).
Materials and Methods
Characteristics of the Study and the Clinical Center
This study was performed on the basis of retrospectively collected microbiological data regarding a 10-year time period on January 1, 2008, to December 31, 2017. Our institute is the dedicated microbiological diagnostic laboratory of a 1820-bed tertiary-care teaching hospital in Szeged (Hungary), which is responsible for the medical care of >400 000 patients in the southern region of Hungary. Data were collected by an electronic search of the Institutional laboratory information system records for the designated time period, which was conducted by the authors. Isolates were considered separate if their isolation happened >14 days apart, or S maltophilia isolates with different antibiotic susceptibility results were detected from the same patient. Polymicrobial infection was defined by the isolation of more than 1 organism in a single sample. 29 As a part of this study, data on the affected patients were also collected, which was limited to demographic characteristics (age, sex, and inpatient/outpatient status) and the indication for sample submission. The relevant data were collected if S maltophilia was isolated in significant colony count from the samples of the abovementioned patients. The study was deemed exempt from ethics review by the institutional review board, and informed consent was not required as data anonymity was maintained.
Processing of Microbiological Samples, Identification, and Susceptibility Testing
Respiratory sampling from patients was performed in line with current recommendations with international guidelines, respective to each individual sample type. The processing of respiratory tract samples was based on current international guidelines of routine clinical bacteriology; culture plates were incubated at 37°C for 24 to 48 hours, aerobically. For bacterial identification, classical phenotypic methods and VITEK 2 Compact ID/AST (bioMérieux, Marcy-l’Étoile, France) were used between 2008 and 2012; however, starting with 2013, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS; Bruker Daltonik GmbH, Germany) was introduced to the diagnostic workflow of our laboratory. Sample preparation methods and technical specifications for MALDI-TOF MS measurements are described elsewhere. 30 Susceptibility testing for S maltophilia isolates was performed for SMX/TMP and levofloxacin routinely; if SMX/TMP resistance was detected, supplementary antibiotics (tigecycline, amikacin, and colistin) were also tested. The susceptibility testing methods utilized and the interpretative criteria were described elsewhere in detail. 29
Statistical Analyses
Data for analysis were collected from the MedBakter laboratory information system, while the management of data and the preparation of data for statistical analyses were performed using Microsoft Excel 2013 (Microsoft Corp, Redmond, Washington). Statistical analyses were performed with SPSS software version 24 (IBM SPSS Statistics for Windows 24.0; IBM Corp Armonk, New York). The normality of variables was tested using Shapiro-Wilk tests. P values <.05 were considered statistically significant.
Results
A total of 579 S maltophilia isolates were identified (57.9 ± 31.0/year, highest in 2015, lowest in 2008) from various respiratory samples between 2008 and 2017. The number of isolates between 2008 and 2012 was n = 160 (32.0 ± 5.33/year, range: 24-38), while for 2013 to 2017 this number was n = 419 (83.8 ± 21.53/year, range: 55-111). A sizable (P = .0008) increase was observed in the detection of S maltophilia in the second part of the study period (2013-2017). The affected patients presented with a pronounced male dominance (female-to-male ratio: 0.69; 63.84% male); the median age of the affected patients was 55 years (range: 0-96 years), both in the inpatient and outpatient groups. The age distribution of patients was as follows: 16.03% 0 to 5 years, 3.84% 6 to 17 years, 6.51% 18 to 35 years, 11.20% 36 to 50 years, 26.24% 51 to 65 years, and 36.19% of patients were older than 65 years.
Tracheal aspirates were the most common samples type (65.28%), followed by sputum samples (17.20%), bronchoalveolar lavage (BAL; 16.82%, including and bronchoscopic BAL and MiniBAL), in addition to samples attained through pleural and pericardial puncture (0.35% each). Indications for the submission of the abovementioned positive samples included septicemia (19.17%), hematological malignancies (predominantly acute myeloid leukemia) and solid tumors (lung, stomach, and colon cancer; 16.23%), recent trauma, burns or invasive surgery (13.47%), congetinal disorders or preterm delivery (12.78%), pneumonia, pleuritis or acute respiratory distress syndrome (11.07%), cardiovascular illnesses (10.89%), cystic fibrosis (6.91%), meningitis (5.54%), or other reasons (3.94%). The largest amount of isolates originated from the intensive care units (which has 3 subsections, namely, cardiology–hematology, surgery, and traumatology; 47.49%), department of internal medicine (27.29%), department of pediatrics and neonatology (9.86%), department of otorhinolaryngology, head and neck surgery (8.11%), department of oncology (5.78%), and other affiliated institutions (1.47%). At the time of isolation, 24.89% of affected patients were treated as outpatients; the number of isolates from outpatient samples was significantly higher in the second half of the study period (n = 40 vs n = 103; P < .04).
In 71.84% of relevant respiratory samples, S maltophilia was the only isolated pathogen, whereas in 28.16%, more than 1 (2 in 18.13%, 3 in 6.05%, 4 in 2.76%, and 5 or more in 1.21%) different species could be isolated (Table 1). Other nonfermenting Gram-negative and Candida species were the most frequent species coisolated. Pseudomonas aeruginosa (in 57 cases) and C albicans (in 54 cases) were the most frequent coisolates; 5.35% of coisolated pathogens were MDR (including MDR P aeruginosa, methicillin-resistant S aureus [MRSA], and extended-spectrum β-lactamase-producing [ESBL] Enterobacteriaceae).
Pathogens Coisolated With Stenotrophomonas Maltophilia in Respiratory Samples, 2008-2017.

Abbreviations: ESBL, extended-spectrum β-lactamase MRSA, methicillin-resistant Staphylococcus aureus.
During the 10-year period, almost 88% (87.90%) of respiratory S maltophilia were susceptible to SMX/TMP, while levofloxacin susceptibility (Minimum Inhibitory Concentration [MIC] range: 0.5-64 mg/L) was shown to be somewhat higher (91.01%). This left 12.1% of isolates (2008-2012: 6.12%; 2013-2017: 18.06%; P = .034) resistant to SMX/TMP and 8.99% of isolates (2008-2012: 7.86%; 2013-2017: 10.12%; P > .05) resistant to levofloxacin, respectively. Of the SMX/TMP-resistant S maltophilia strains, 71.42% was also resistant to amikacin (MIC range: 1-32 mg/L), 10.20% for tigecycline (MIC range: 1-32 mg/L), and 8.57% for colistin (MIC range: 0.25-256 mg/L). It is worth noting that in 5.87% of isolates, resistance to SMX/TMP, levofloxacin, amikacin, tigecycline, and colistin was present simultaneously; therefore, these isolates should be considered XDR strains. The SMX/TMP resistance was detected more frequently in samples originating from inpatients (n = 2.50 ± 2.39 vs n = 11.50 ± 3.76; P = .0002), while a numerical but not statistical tendency was observed for levofloxacin resistance (n = 4.49 ± 0.23 vs n = 5.86 ± 0.91; P = .078).
Discussion
The amount of specific studies regarding the prevalence and resistance trends of S maltophilia isolates in LRTI samples is very limited, the available literature concerning this topic is summarized by the authors in Table 2. Stenotrophomonas maltophilia LRTIs are thought to be infrequent, but their clinical relevance is increasing in the era of surgical interventions and heavily immunosuppressed patients. 1 –4,9 –11,16 –22 The presence of obstruction in the lungs creates advantageous conditions for several opportunistic pathogens to cause infections, including S maltophilia, in addition obstruction has been shown to be an independent risk factor for a poor outcome. 3 In line with the findings of other studies, we have demonstrated that most of the affected patients were very young or older than 50 years of age (78.46% of patients in the present study), with an observed male dominance in the patient population. A possible explanation for this phenomenon is that males are more prone to contract S maltophilia, due to their activities in the outdoors/aquatic environments. 3 Based on our results, we have noted an increase in the isolation rate of S maltophilia from LRTI samples, in addition to an increase in its prevalence in outpatient settings. The introduction of MALDI-TOF MS in our institute may explain the increase in the detection of these species; additionally, carbapenem prescription levels (both in the region and in Hungary overall) have increased dramatically (mainly due to the emergence of ESBL-positive strains) which may also have resulted in a more pronounced selection pressure for S maltophilia isolates. 49
Summary of the Literature Regarding Susceptibility Trends of Stenotrophomonas Maltophilia From Respiratory Tract Isolates
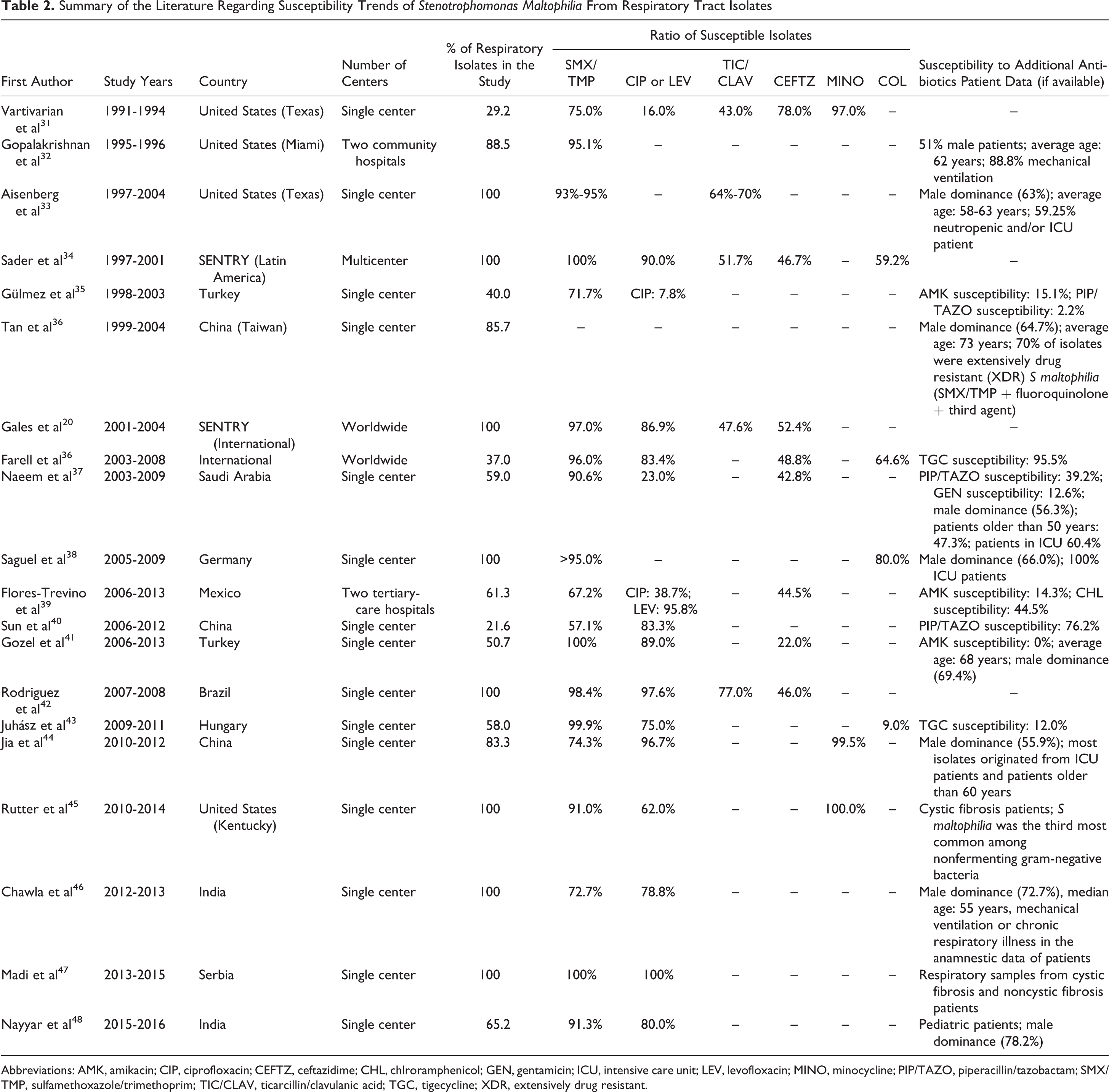
Abbreviations: AMK, amikacin; CIP, ciprofloxacin; CEFTZ, ceftazidime; CHL, chlroramphenicol; GEN, gentamicin; ICU, intensive care unit; LEV, levofloxacin; MINO, minocycline; PIP/TAZO, piperacillin/tazobactam; SMX/TMP, sulfamethoxazole/trimethoprim; TIC/CLAV, ticarcillin/clavulanic acid; TGC, tigecycline; XDR, extensively drug resistant.
The local levels of SMX/TMP resistance were similar to those found in the global literature (Western Hemisphere: 2%-10%; however, some outliers with higher resistance levels [eg, Spain: 27%; Turkey 10%-15%] in Europe and Asia [Taiwan: > 25%; China: 30%-48%]) but somewhat higher than the European average. 7 In a similar study recently published by Gajdács et al in the same geographical region, 16.0% of isolates from bacteremia were resistant to SMX/TMP, and of these resistant strains, 32.7% were also resistant to levofloxacin, tigecycline, and colistin (thus, 5.2% overall were XDR isolates). 29 In contrast, during our current study regarding respiratory isolates, it was found that the levels of SMX/TMP and LEV resistance were lower (12.1% and 8.99%, respectively), while the ratio of XDR isolates was higher, recorded at 5.87%. It must be noted that in patients with malignant neoplasms, ICU patients, and patients with CF, resistance levels may be even higher (20%-80%). 4 The matter of SMX/TMP resistance is complex, as there is no definite consensus or guideline on the susceptibility testing and interpretation (breakpoints) for S maltophilia for several antibiotics, which may lead to confusion when interpreting published clinical data. Institutions must establish therapeutic protocols for these cases based on local resistance trends and international guidelines. In addition, more studies are needed to assess the relevance of various combination therapies in a controlled clinical setting. 50
Several limitations of this study should be acknowledged. First, due to the inability to access the medical records of the individual affected patients, the presence and nature of symptoms of the patients were unknown. Additionally, the correlation between the presence/absence of all relevant risk factors and S maltophilia isolation from the respiratory tract could not be assessed. There is also a risk of selection/referral bias, as studies describing the prevalence of infectious diseases and resistance trends are mainly tertiary-care centers, which generally correspond to patients with more severe conditions or underlying illnesses, compared to community-based settings 29 .
In this present study, we observed the increasing prevalence of S maltophilia from respiratory tract specimens; the increase in prevalence may be due to the developments in diagnostic technologies in microbiology laboratories; however, there have been reports that isolation of S maltophilia increases proportionally with the utilization rate of carbapenem antibiotics (which provides selection pressure). Due to the increasing prevalence of extended-spectrum β-lactamase-producing gut bacteria in severe infections in Hungary, this observation correlates with the increased administration of carbapenems. The key points of the present study are the reporting of resistance trends of S maltophilia in the Central Eastern part of Europe, from where only few reports were published thus far; while the ratio of resistant strains to SMX/TMP and LEV (10.12% and 8.99%, respectively) is not outliers from the data found in the international literature, more than 1 of 20 of these respiratory isolates were representative of the XDR phenotype. For severely debilitated, immunocompromised patients, this corresponds to a very severe therapeutic conundrum, with little or no antimicrobial options left to treat them. 1,29 Both in the literature and based on our own results, S maltophilia was isolated with another significant pathogen. Therapeutically, this may bring forth additional challenges, especially if the mentioned copathogen is also resistant to several antibiotics (eg, ESBL Enterobacteriaceae, carbapenem-resistant Pseudomonas and Acinetobacter, and MRSA). 51 –53 The use of inhalational/aerosolized antibiotics may have an important role in the therapy of these LRTI infections; their use is gaining increasing attention, in addition to combinational antibiotic therapy.
Footnotes
Authors’ Note
M.G. conceived and designed the study. E.U. was the senior microbiologist and performed the identification of the bacterial isolates during the study period. M.G. and E.U. performed data collection and analysis, wrote, and revised the full article.
Acknowledgments
The authors would like to thank Tünde Deák and Erika Karasz for the excellent laboratory assistance during the routine diagnostic work.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.G. was supported by the National Youth Excellence Scholarship [Grant Number NTP-NTFÖ-18-C-0225] and the ESCMID Mentorship and Observership Programme.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.