
Abstract
Objectives:
To evaluate the effect of a team-based primary care redesign on primary care, emergency department (ED) and urgent care (UC) utilization, and new patient access to primary care.
Study Design:
A retrospective pre–post difference-in-differences analysis of utilization outcomes for patients on a redesigned primary care team compared to a standard primary care group.
Methods:
Within a patient-centered medical home, a pilot team was developed comprising 2 colocated “teamlets” of 1 physician, 1 nurse practitioner (NP), 1 registered nurse (RN), and 2 licensed practical nurses (LPNs). The redesigned team utilized physician–NP comanagement, expanded roles for RNs and LPNs, and dedicated provider time for telephone and e-mail medicine. We compared changes in number of office, ED, and UC visits during the implementation year for patients on the redesigned team compared to patients receiving the standard of care in the same clinic. Proportion of new patient visits was also compared between the pilot and the control groups.
Results:
There were no differences between the redesign group and control group in per-patient mean change in office visits (Δ = −0.04 visits vs Δ = −0.07; P = .98), ED visits (Δ = 0.00 vs Δ = 0.01; P = .25), or UC visits (Δ = 0.00 vs Δ = 0.05; P = .08). Proportion of new patient visits was higher in the pilot group during the intervention year compared to the control group (6.6% vs 3.9%; P < .0001).
Conclusions:
The redesign did not significantly impact ED, UC, or primary care utilization within 1 year of follow-up. It did improve access for new patients.
Background
Over the past decade, health-care delivery organizations, insurers, and specialty organizations have supported the transition of primary care practices toward the Patient-Centered Medical Home (PCMH) model to address the triple aim of health-care reform: improving quality of care and patient experience while controlling health-care costs. 1,2,3 -7 However, effects of PCMH models have been mixed. 7 -11 Shortages of primary care physicians, patient complexity, and competing demands on primary care present growing challenges to the goals of the medical home model. 2,5 Team-based care is a central feature of the PCMH with potential to address some of these challenges, yet team composition and implementation are variable among medical homes. 2,10,12 -14 Current proposals for primary care redesign call for further work in team-based care and emphasize expanded use of non-face-to-face visits. 2,15,16 Although lack of reimbursement for such encounters has been a barrier to innovation in these domains, as health policy and reimbursement shift toward value-based payment, care models that utilize teams and non-face-to-face visits may be well positioned to address ongoing gaps in access and care. 17 -20
Concentrating care in a smaller care unit, or “teamlet,” within a larger practice can enhance continuity and improve experience for both providers and patients. 14 Collaboration between a physician and an advanced practice provider (APP) in shared care of a panel of patients is an example of a teamlet that has demonstrated improved quality measures and provider and patient satisfaction. 21,22 Expanding non-face-to-face access within such teams with established provider–patient relationships may further enhance care delivery. 15 Specifically, use of telephone and online encounters to meet patients’ needs can improve access, efficiency, continuity, and timeliness of visits. 23 -25
We piloted a teamlet-based primary care model incorporating enhanced non-face-to-face access. The goal of this study was to determine the effect of this pilot on primary care, emergency department (ED), and urgent care (UC) utilization. Because enhanced access and care continuity are associated with decreased ED utilization, we hypothesized that in comparison to a control group within the same clinic, patients attributed to the pilot providers would have decreased ED and UC utilization. 3,26 A secondary goal of the study was to determine the effect of the pilot on access for new patients.
Methods
Study Setting
The study was conducted at a National Committee for Quality Assurance level III academic PCMH 27 that cares for approximately 12 000 adult patients. The practice was closed to new patients, and patients’ ability to see their personal primary care physician for acute or timely follow-up care was often limited; patients were often scheduled with any available provider for acute visits. Providers had no dedicated clinic time for non-face-to-face visits. The majority of the APPs’ clinic time was spent seeing patients for acute care, preoperative, or preventive care rather than chronic disease management. There were 7 registered nurses (RNs) dedicated to telephone triage. Seven licensed practical nurses (LPNs) and 4 medical assistants (MAs) were paired with providers to perform visit preparation, rooming duties, and panel management. The LPNs and MAs were termed clinical care associates (CCAs). The RNs performed face-to-face patient visits rarely, and LPN visits were limited to vaccine and medication administration.
Intervention
A team-based care pilot was developed within the PCMH with a mission to improve new patient access, care value, and patient access to their personal care team. The pilot was implemented in May 2015 and comprised of 2 teamlets of 5 providers (an MD, an APP, an RN and 2 CCAs, including at least 1 LPN; Figure 1). The team was colocated in 1 hallway, with each MD-APP pair sharing office space. Team meetings occurred 1 to 3 times weekly to coordinate care and iterate process work. 28,29
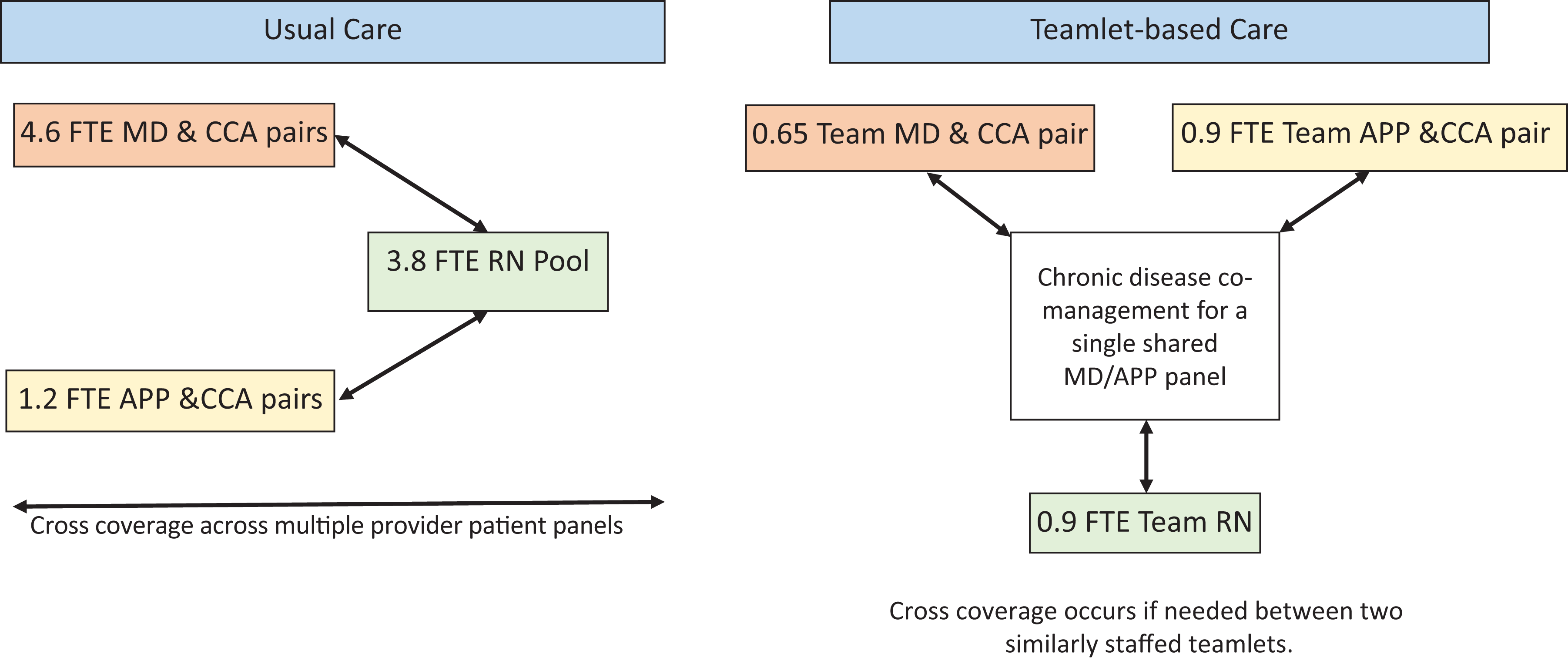
Usual care model compared with pilot teamlet-based care model.
Physicians were given 30 minutes and APPs 90 minutes daily for non-face-to-face patient care. Phone staff were instructed to direct all pilot patient calls for acute concerns to the pilot RN rather than schedule directly with providers and were instructed not to schedule nonpilot patients with pilot providers and vice versa. Efforts were made to accommodate pilot patients for acute visits within the patient’s teamlet rather than the alternate teamlet. Over the first 6 months, a chronic disease comanagement model within the MD-NP pairings was developed iteratively; patients with chronic medical conditions who were seen every 1 to 6 months were scheduled alternately with the APP and the MD every other visit.
Nonprovider staff on the pilot team had expanded roles in managing chronic illness and coordinating care. The CCAs reviewed after visit instructions and checked patients out in the examination room rather than patients checking out at the front desk. Beginning in June 2015, outreach calls to patients who had recently been to the university hospital ED or UC were made by either the teamlet APP or the LPN. The LPN and RN blood pressure, diabetes, and medication reconciliation face-to-face visits began in July 2015, with protocols refined iteratively.
During pilot implementation, the nonpilot providers and staff were aware of the abovementioned interventions but did not participate, thus serving as a control for this study. The APPs on the pilot team and one physician in the control provider group were listed as accepting new patients during the pilot implementation period.
Data Collection and Statistical Analysis
We conducted a retrospective review of electronic health record (EHR) data for all patients attributed to the clinic who had at least 1 visit to the clinic during both a baseline year (May 2014 to April 2015) and the intervention year (May 2015 to April 2016). Patients were attributed to either pilot providers or control providers based on their EHR primary care provider assignment on May 1, 2014. Billing data from visits to the clinic and to the university ED and UC center were collected, all of which used the same EHR. International Classification of Diseases, Tenth Revision (ICD-10) codes for common chronic medical conditions were obtained from patient problem lists for baseline characteristics.
We compared demographic characteristics of patients within the pilot group to the control group using simple χ2 and t tests (Table 1). Difference-in-differences regression analyses were used to compare changes over the 2 time periods for 3 outcomes: number of patient visits to the ED, UC, and clinic, between the pilot team and the control group (Table 2). 30 The following model (Equation 1) was fit for each outcome (Yi ,t ):
Patient Demographics for Pilot Group Versus Control Group.

Unadjusted Mean Annual Per-Patient Visit Counts Pre- and Postintervention for Pilot Group Versus Control Group.

a P value for the difference-in-differences effect between the pilot and control groups from pre to post intervention from Poisson regression models controlling for age, sex, hypertension, diabetes, current smoker, anxiety/depression, and insurance type as potential confounders.

The patient-level regression models (Equation 1) for each outcome (Yi , t ) used a difference-in-differences specification to examine the impact of care redesign, where i was an indicator for pilot redesign, and t was an indicator for time period. Each regression also included demographics (age, sex, current smoker, and insurance type in 2014) and active problem list diagnoses (hypertension, diabetes, and anxiety/depression) from the EHR as potential confounders. Due to excess zeros in number of visits (count) data, we used the zero-inflated Poisson (ZIP) regression models. 31 The ZIP regression model included 2 parts: a Poisson count model and the logit model for predicting excess zeros. All ZIP models were run with the robust option in Stata statistical software version 15. 31 The ZIP models were compared to standard Poisson models; if there was not a better model fit using ZIP, standard Poisson was used. We used χ2 analysis to evaluate differences in proportion of new patient visits between the pilot and control groups. This study was approved by the institutional review board.
Results
There were no differences in baseline characteristics between the pilot group (n = 1807 patients) and control group (n = 4715 patients) with respect to age, insurance type, smoking status, or prevalence of hypertension or diabetes. The pilot group had a significantly smaller proportion of females and a higher proportion of patients with anxiety or depression (Table 1). We found no differences between the pilot group and thecontrol group in per-patient mean change in office visits (Δ = −0.04 visits vs Δ = −0.07; P = .98), ED visits (Δ = 0.00 vs Δ = 0.01; P = .25), or UC visits (Δ = 0.00 vs Δ = 0.05; P = .08; Table 2). There was no difference in baseline proportion of new patient visit between the pilot (191/6578 = 2.9%) and control groups (507/16 962 = 3.0%; P = .729). The pilot group had a higher proportion of new patient visits (437/6628 = 6.6%) during the intervention period compared to the control group (661/17 063 = 3.9%; P < .001).
Discussion
Our study adds to the growing body of literature evaluating the impact of primary care redesign efforts. We found that the primary care team pilot did not significantly impact ED, UC, or primary care utilization within 1 year of follow-up when compared to a control group. The pilot team did increase access for new patients, which demonstrates the ability of care teams with expanded nonphysician roles to accommodate increases in panel size. Although we cannot fully separate the effects of the intervention from confounding secular or unmeasured effects, we are confident that this practice redesign was the dominant practice innovation throughout the study.
There are several limitations to this study. Given the nonrandomized application of the intervention, there may be unmeasured ways in which the study and control groups differed. Since the intervention took place within the same clinic as the control group, it is also possible that some of the pilot methods were adopted less formally by members of the control group. 3 We were not able to assess the integrity of some aspects of the intervention; for example, we could not quantify non-face-to-face visits in our EHR data. Further, as a pilot study in a single practice, the results may not generalize to other sites.
Given the iterative nature of the pilot team’s work, a 1-year duration may not have been enough to observe significant differences in care value. 32,33 The trend toward fewer UC visits among patients attributed to the pilot team compared with control patients during the implementation year suggests that with longer follow-up, a significant difference may have been found. The small sample size may have further limited our ability to detect differences in utilization between the groups. Two larger studies of pilot medical home redesigns with follow-up over 2 to 4 years did demonstrate improvement in ED and UC utilization. 34 Further, the baseline characteristics of our study showed higher rates of anxiety and depression in patients attributed to the pilot group, which could have affected utilization. 35,36 Additionally, baseline ED and UC rates were low, limiting ability to demonstrate improvement. 37 -39 We were only able to collect ED and UC utilization data from the university hospital; although this methodology was the same during both the baseline and the intervention year and the next closest hospital is 27 miles away, the true ED and UC utilization data are underrepresented in our study.
Other quality measures such as glucose and blood pressure control were not evaluated in our study and could have added meaningful outcome data, although team care innovations showing improvement in these areas usually focus on a specific chronic disease. 20,22 Our pilot study is more reflective of the mixed outcomes often seen in multifaceted care delivery innovations. 9,32 We did not design a method for evaluating patient satisfaction with the pilot team model compared to the nonpilot team model, which may have been informative. A qualitative evaluation of a measure of the fourth aim of health-care reform, provider and staff experience with the redesign, was completed and analysis is underway. 40 Finally, a cost analysis of the redesign was beyond the scope of this study; however, the component of the model with the greatest cost impact is the increased provider time for non-face-to-face visits. This component may only be feasible with alternative payment structures.
Despite these limitations, ED/UC utilization in primary care redesign efforts is an important outcome, and our study adds insight into the difficulties in showing improvements within complex and dynamic practice environments. Future studies of primary care redesign efforts could explore longer follow-up, additional care value measures, patient satisfaction, and focused evaluation of single process improvement cycles.
Conclusion
The pilot primary care practice redesign did not significantly impact ED, UC, or primary care utilization within 1 year of follow-up. The redesign team did accommodate more new patient visits during the implementation year. Our study adds insight into the challenges of demonstrating broad utilization benefits of complex system redesign.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was a pilot study supported by the University of Vermont Medical Center (UVMMC) in that, in contrast to the standard business model at UVMMC, pilot care providers were not held accountable to any RVU targets during the pilot implementation year.