
Abstract
Background:
Despite health care access challenges among underserved populations, patients, providers, and staff at community health clinics (CHCs) have developed practices to overcome limited access. These “positive deviant” practices translate into organizational policies to improve health care access and patient experience.
Objective:
To identify effective practices to improve access to health care for low-income, uninsured or underinsured, and minority adults and their families.
Participants:
Seven CHC systems, involving over 40 clinics, distributed across one midwestern state in the United States.
Methods:
Ninety-two key informants, comprised of CHC patients (42%) and clinic staff (53%), participated in semi-structured interviews. Interview transcripts were subjected to thematic analysis to identify patient-centered solutions for managing access challenges to primary care for underserved populations. Transcripts were coded using qualitative analytic software.
Results:
Practices to improve access to care included addressing illiteracy and low health literacy, identifying cost-effective resources, expanding care offerings, enhancing the patient–provider relationship, and cultivating a culture of teamwork and customer service. Helping patients find the least expensive options for transportation, insurance, and medication was the most compelling patient-centered strategy. Appointment reminders and confirmation of patient plans for transportation to appointments reduced no-show rates.
Conclusion:
We identified nearly 35 practices for improving health care access. These were all patient-centric, uncovered by both clinic staff and patients who had successfully navigated the health care system to improve access.
Keywords
Introduction
Health care in the United States continues to be at a crossroad, with its quality and economic security at risk due to system problems in health care delivery. 1 Limited access to health care is an important equity and social issue in the United States and persists as a significant burden on its population. 2 Low-income people, as well as racial and ethnic minorities, are more likely to receive lower quality of care and encounter more obstacles to health care access compared to other groups. 3 A recent study found that among adults aged 18 to 64 years who had no insurance in the prior year, 1 (22%) in 5 had an unmet medical need related to cost. 4
Access to health care means having “the timely use of personal health services to achieve the best health outcomes.” 2 Good access to care is comprised of 3 distinct steps: (1) achieving entry into the health care system, (2) obtaining access to essential health care services, and (3) locating providers that can meet patients’ individual needs and with whom they can communicate and build a respectful and trusting relationship. 3 Access to health care is critical for optimal health and wellness; thus, addressing obstacles that occur at each of these steps is important for improving the patient experience and health outcomes.
Enhanced access and continuity of care are also core components of patient-centered care. 5,6 Several interventions have been used to enhance access to primary care. The existing strategies have been classified into 5 categories: (1) practice reorganization, (2) patient support, (3) new services, (4) financial incentives, and (5) workforce development. 7 The aim of the current study was to investigate barriers and effective practices in community health centers (CHCs) to improve access to primary health care, in outpatient ambulatory care settings, for underserved populations: low-income, uninsured or underinsured, and minority adults and their families. Although we sought strategies within all 5 categories, our focus was on practice reorganization, patient support, and new services.
At the onset of this project, approximately 1.5 million low-income individuals had inadequate access to health care services in Indiana, 21 most of whom would turn to CHCs for their care. CHCs are nonprofit organizations that “provide affordable, high quality, comprehensive primary care to medically underserved populations, regardless of their insurance status or ability to pay for services.” 15(p3) In 2014, there were 23 CHC systems in Indiana serving over 393 000 patients, the majority of which were low income and uninsured or underinsured. 15 CHCs vary in the types of services available, with some having laboratory testing and pharmacies on-site. In order to understand and address barriers to accessing care, we formed a collaborative with 7 Indiana CHC systems (see Table 1), spanning 40 clinic sites.
Information on the CHC Systems, Patient Served in a Year, the Number of Physical Service Delivery Sites, the EHR Used, and Appointment Scheduling Method Currently in Place.

Abbreviations: CHC, community health center; EHR, electronic health record.
This study was the first of a 3-phase redesign project aimed at improving access to primary care in CHCs. In this study, we report the patient-centered solutions identified for managing challenges particular to providing access to care for underserved populations that emerged from a thematic analysis of stakeholder interviews.
Methods
Semi-structured interviews were conducted over a period of 18 months with key informants (patients and staff) at each participating CHC system (Table 1) as a means to understand primary care access challenges and corresponding practices that individuals have found helpful in overcoming limited access.
We took a unique approach in our study recruitment, applying a contextual framework involving “positive deviance” (PD) from complexity science, in order to identify innovative, successful practices of key informants, whose practices enable them to find solutions to overcome health care access problems. 8,9 Positive deviance is a bottom-up improvement approach that considers people doing the work as experts and focuses specifically on utilizing them as a typically untapped resource. Individuals or groups whose behaviors or practices enable them to find better solutions to prevalent, seemingly intractable problems are considered “positive deviants.” 10 Thus, the PD approach was used here in an attempt to discover these positive deviants within a population of CHC patients and frontline staff and engage them in identifying solutions to existing access barriers. Positive deviance has demonstrated its efficacy in solving health-related problems 8,9,11,12 and supporting improvement and redesign efforts in health care organizations. 13,14 The PD framework was applied both for recruiting targeted participants and as a lens for data analysis.
Interview Methods
Interviews were conducted face-to-face with a sample of CHC managers, providers, and other staff, as well as patients seeking care at those clinics. We asked our clinic liaison (typically the clinic manager or upper-level management) to select patients who demonstrated successful strategies or practices to gain access to health care and staff who had developed successful practices in delivering care. While not all the individuals that we interviewed could be categorized as positive deviants, successful practices for improving health care access were identified across all interviews.
Site Selection
CHCs were invited to participate via a mailing to administrators describing the project, expected responsibilities, and benefits. Participating clinics were selected based on expressed commitment, a diverse patient population, and willingness to share data and participate in implementing an intervention. Participating clinics were diverse according to both patient- and clinic-level factors (Table 1).
Data Collection
Prior to clinic visits, clinic liaisons (typically the clinic manager or upper-level management) identified patients and staff who demonstrated successful strategies or practices to improve patient health care access. Of those identified, we recruited staff across a range of key roles to understand clinic processes from various vantage points and how processes relate to patient’s health care access. Research staff completed the informed consent process with all participants individually prior to their interview. Semi-structured interviews focused on successful patient-centered practices to overcome availability, accommodation, and affordability challenges (see Table 2 for example questions). Patient participants were compensated with a US$20 gift card; clinic staff and providers were not directly compensated, but the clinic received a stipend to account for employee time. All interviews were conducted in a private room, recorded, and transcribed. No individual or clinic identifiers were retained in the transcripts. The institutional review board at our university approved all procedures.
Sample of Interview Questions Used With Patients.
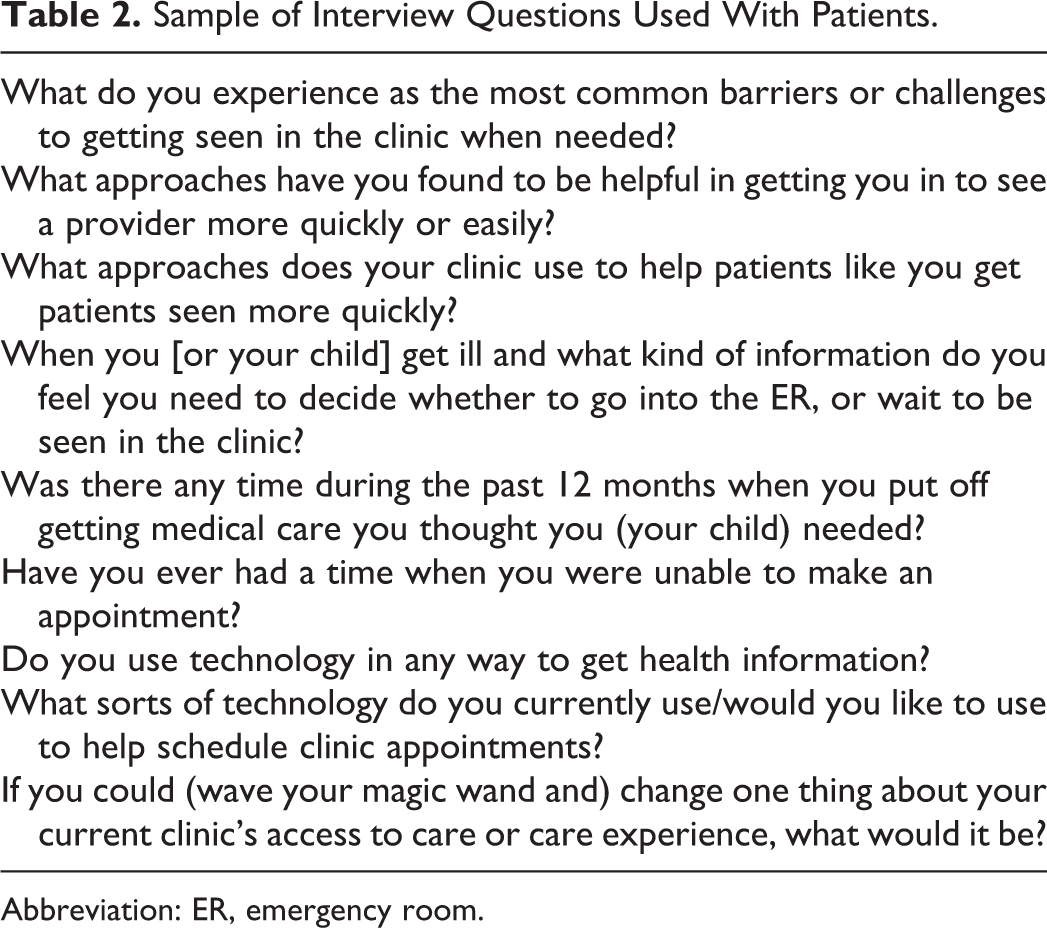
Abbreviation: ER, emergency room.
Data Analysis
We conducted a qualitative thematic analysis 16 of the transcribed interviews. The research team developed a code book after reviewing 3 complete transcripts. Using an iterative consensus-based process, members coded data independently and then met to discuss discrepancies and reach consensus. The final consensus for each pair of reviewers was entered into NVivo. 17 After coding 10% of the data in this manner, team members independently coded transcripts. After coding, the data were compiled and each category was reviewed for upward abstraction. Specifically, the data were represented at a higher level of abstraction so that interview responses could be integrated across cases to show patterns of strategies.
Results
We conducted a total of 92 key informant interviews, split between clinic patients (42%) and clinic staff (53%; Table 3). Participating staff included providers, managers, nurses (registered nurses [RN] and licensed practical nurses [LPN]), medical assistants, schedulers, front desk staff, social workers, care navigators, and billing coordinators. Roughly half (47%) had worked in the clinic for more than 5 years. The majority of participating patients were uninsured or underinsured (84%) and had been patients at the clinic for a median length of 6 years. Patients reported their health status to be “poor” (12%), “fair” (42%), “good” (39%), or “very good” (7%).
Summary Characteristics of Interviewees.

Interview themes related to improving access are shown in Table 4. One of the central contributions from this work was a list of 35 practices for improving health care access (Table 5). These strategies were all patient-centric, uncovered by both clinic staff and patients who had surmounted barriers to health care access. This list of practices was refined and prioritized in a later part of our study, then used to identify the clinic interventions for improving access in our third and final phase of our study. Based on the study goals, we focus on fully describing the creative strategies and PD approaches uncovered 7 during the interviews that resonated across all of the thematic categories (Table 4).
Summary of Thematic Analysis.

Abbreviations: IT, information technology; EHR, electronic health record; pt, patient
Thirty-Five Practices for Improving Health Care Access Emerging From Interviews.

Positive Deviance Practices to Improve Patient-Specific Challenges
Patient-centered practices to improve health care access in response to patient challenges included addressing illiteracy and low health literacy, identifying low cost or free resources, expanding care offerings at the clinic, and socializing patients to health care delivery. Illiteracy and poor understanding of chronic disease management was identified as a major barrier to access. One provider discussed how the clinic had applied a candid approach to evaluate patients’ ability to read by directly asking them, “Can you read?” Being direct in identifying challenges was considered important in determining patient education needs. You just have to go there and be honest…I found 4 patients [1] morning—none of them could read and all of them were on at least 7 or 8 medicines. (Physician)
Providing specialty care and other health services in the clinic was seen as an effective mechanism to improve access to care. In particular, dental care, language interpretation, pharmacy, laboratory tests, urgent care, and mental health services were present in clinics. For instance, 1 clinic staff member explained the value of having an integrated mental health treatment option to prevent long wait times for appointments with a specialist. In another example, 1 PD practice that came from a nurse manager was rooted in the need to get more women into the clinic for the prevention of chronic diseases that are associated with obesity. Her idea was to create a primary care practice that was strictly focused on weight management, leveraging the fact that most people experience societal pressures to be thin. “…[if] we have someone who focuses specifically on weight loss, you can get many preventative things done, too. This is a good way to bring patients in for their preventive care.” Further, this nurse also suggested wrapping mental health services around other high-interest programs such as weight loss to address underlying issues which impair adherence to self-care recommendations. Also, providing multiple services at 1 location circumvented transportation problems to another location.
In general, staff and providers exuded passion for the community they served. For some, this translated into PD practices. For example, 1 medical director considered nearly every social interaction in his professional community as an opportunity to find specialists who may be willing to provide care to his patient population. There are not that many specialists out there that will accept our patients on a sliding scale. So as a clinical and medical director, my job is to go and find those people who have a heart for the community. So I’m in a constant search. I take every opportunity to find those people. If I’m in a social gathering or in a meeting, if I’m on the road, in the hospital, wherever I am, I try to make the contacts. (Physician) …when I talk to patients I validate their issues because to everybody their issues are real…the other thing is I educate patients on “how it really needs to work” and “this is how it needs to happen.” I validate where they are, and I help them try and get to where I need them to be…I’d say I have a very good success rate of people leaving here happy with a better understanding of what the expectations are. And I think sometimes people just need to be told, you know, what part of it is your responsibility.” (Administrator) The preventive services that you get wasn’t really advertised…No matter what your deductible is or your premium, it’s covered for free. So I made 1 [brochure] for adults, 1 for women, and 1 for children. So now when people sign up for coverage, I can give them one of those.” (Patient Navigator)
Positive Deviance Practices to Improve Patient Experience
Multiple factors can contribute to a negative care experience. The most commonly mentioned contributors to a negative experience included prolonged waiting time until available appointment, poor customer service (either on the phone or in the clinic), disorganized care, lack of empathy, short amount of time with the provider, long wait time on the phone, and high turnover in clinical staff.
Multiple comments suggested the remedy for improving patient experience was grounded in positive interpersonal relationships and building a culture of customer service and patient-centeredness. We most often heard about positive practices which built rapport with patients by actively listening and communicating in a respectful and collegial manner. One patient explained the value of “that personal touch, you know, it was a friendship there, you know, not just as a doctor. I always felt that he cared about my sons…” Numerous patients noted the rapport and engagement generated when clinic staff knows their name; others talked about the security of seeing providers and staff who have been in the clinic for years. One mother discussed a time when she brought her son in for help with mental health challenges. One of the nurses has known him since he was born, and she is still there. And that was the first face he saw when he walked down the hallway…He felt at ease, you know. So, I have those long-term relationships…” (Mother of Adolescent Patient) We are somewhat aggressive in talking directly to teenagers and kicking parents out of the room because they don’t need to be involved in parts of the conversation…I had some of them tell me “we like talking to you ‘cause you’re real and you talk to me.” (Physician)
The architectural design, physical appearance of the clinic, and its amenities and services also contributed to positive patient experiences. Patients expressed a desire for a clean, open-design and comfortable environment with a play area for children. One patient told us that she scouted out the clinic before scheduling an appointment, “I just acted like I had to use the bathroom and I could like check it out and see if everything was up to par. I came in here and it was like, oh, yeah, they’re clean and everything.”
Other contributors included specific actions, services, or policies that had been established. For example, creating tailored education to facilitate diabetes self-care or group visits and incentive programs aimed at improving adherence to recommended prenatal visits. Other factors such as easy appointment scheduling, limited paperwork, clinic proximity to home, and short waiting time were also valued. Patients also appreciated surveys and/or follow-up phone calls to identify, address, and resolve patient concerns. For convenience, patients preferred to have laboratory tests, radiologic scans, and other procedures, all offered on-site at the clinic.
Notably, some clinics had hired dedicated staff focused on serving the homeless population in the community. There were several PD approaches to improve access for homeless patients, including working to accommodate homeless patient schedules that revolve around temporary part-time work, meal availability at shelters, and case management meetings.
At 1 site, homeless outreach personnel brought care directly to patients in their living environment, “If I take the flu shots over to the [homeless shelter] I have a much better turnout rate than if I just say, “‘Hey I’m doing a walk-in. Why don’t you guys come over [to the clinic].” This individual also kept a ready supply of needed items that she could give patients when they came for an office visit, I always find that they need things…So I have things here like toothbrushes, toothpaste, floss, personal hygiene items, pads, ChapStick, eye drops, first aid kits with triple antibiotic ointment, and Band-Aids that they’re able to take.” (Homeless Outreach Coordinator)
There were numerous no-cost/low-cost practices that shared 2 characteristics: process and communication. For example, in every clinic, there existed frustration around the phone system. Breakdowns in appointment scheduling, patient–clinic relationships, and clinic efficiencies could all be tied back to the phone system. Although in some cases the phone systems themselves simply needed to be replaced, more often the issue had been resolved with improved process and communication. One clinic manager we encountered had trained her front office and scheduling staff to handle phone interactions as if patients were hotel guests, mandating a commitment to customer service. More important than the idea of customer service itself was the process put in place and communication of this goal to all staff. Similarly, establishing no-show policies, enforcing them, and communicating expectations to patients was an effective means established by the clinic chief medical officer (CMO) to foster accountability in patients. Equally important to the innovative policy was the creation of a mutually respectful platform for discourse between patients and staff.
Discussion
Although numerous studies have examined the needs of underserved patients and improved access to health care, 7,18 –25 our approach to understanding this problem is unique. First, we applied a PD approach 9 to identify individuals who were known to have uncommon approaches to either obtaining health care (patient perspective) or delivering care effectively (clinic staff perspective). This approach gave us an opportunity to focus our findings on unique strategies that complement existing challenges to accessing health care. Across strategies to improve health care access in CHCs (practice reorganization, patient support, and new services 7 ), patient centeredness and customer service consistently motivated trialing new practices and seeking process and care delivery improvements. Moreover, similar to other findings, these emergent strategies for improving health care access reinforce that nonfinancial barriers (e.g., acceptability, accessibility, accommodation, and availability 25 ) are critical for improving health care access. 18 –20 For example, our participants agreed that successfully gaining access to care was dependent on people understanding on how to navigate the health care delivery system (accessibility) as well as being aware of the expectations of them as patients (acceptability). While financial barriers (affordability 24 ) were discussed by many participants as an important obstacle to overcome, we found this to be reported along with nonfinancial barriers to accessing health care. 19,20 For example, limited transportation options to pick up medications or attend an office visit present an accessibility barrier that is inextricably linked to affordability of obtaining care and adhering to medical recommendations. 26
Although the present study included a general underserved population seeking care at CHCs, other research has targeted health care delivery issues for specific populations (e.g., elderly people, immigrants). Taken together, findings suggest that consideration for social determinants of health are vital for improving health care access. Batista and colleagues 22 suggest that, for immigrants, social programs that facilitate social networks and integration into a community can encompass health care access and understanding health care delivery options. Likewise, clinics’ ability to provide interpreter services and cultural sensitivity is responsive to cultural barriers affecting health care access. 24 For elderly, rural populations, Ford and colleagues’ 23 literature review suggests that ease of scheduling an appointment, navigating health care systems, and comfort in a clinic can impact the decision to seek care for persistent physical symptoms. In response to these contextual factors, clinics need efficient scheduling practices, referral programs when specialty care is required, and sufficient allotted time with providers. These recommendations are consistent with strategies employed by participants in this study to improve the patient experience. Creating a culture of customer service and patient centeredness was a prominent PD approach, including meeting patients where they are for care delivery (e.g., homeless patients), explicitly making patients feel welcome, and personalized reminders.
In addition to addressing health care access, clinics must ensure that health care delivery includes a range of health services, from prevention to managing chronic conditions. As Comino and colleagues report, 7 effective strategies for prevention and chronic disease management diverge somewhat. For diabetes, a chronic condition, consistent monitoring improved diabetes management; effective interventions targeting this outcome included practice reorganization, workforce development, and financial incentives. Similarly, as a practice reorganization strategy in the present study, clinics offered patients with diabetes bundled appointments with a provider (glucose monitoring), dietician, and health educator during 1 clinic visit. Also in Comino and colleagues’ review, the number of patients receiving a preventive service was improved by ensuring patients showed up to appointments; effective interventions to improve patient attendance included patient support/education and appointment reminders (practice reorganization effort). Likewise, in the present study, at 1 clinic, providers (physician, medical technician, nurse, and behavioral health specialist) worked as a team with a patient consistently, which over time facilitated relationship building and patient support. Additionally, automated reminder systems and reminder calls were used at several clinics to increase patient attendance.
Limitations of the Study
Our study findings are limited by the purposeful sampling method used to recruit participants and the challenges experienced in finding PD interview participants. Although we asked clinic managers to recruit patients who routinely came to their office appointments and had overcome some major obstacles in life, and to invite clinic staff who were passionate about their work and took unique approaches, not all of the participants we interviewed could be considered as positive deviants. Ideally, we would have used objective data to select those who had been more successful in regularly improving access. Unfortunately, most clinics found this level of analytics capability infrequently available. However, by simply using a PD lens to understand and look for promising novel approaches to problems inspired discourse during our interviews. For example, 1 question that we used in every interview was “…if you had a magic wand and could change anything about the clinic, what would it be?” The interviewer would further probe participants to consider possible changes without constraints of practicality and logistics. In this question, the true PD thinking often emerged. Also, a semi-structured interview approach was appropriate to understand details of strategies that exist in a complex work environment such as a clinic. However, future research could employ other methods to further understand strategies to improve health care access. Focus groups could recruit patients from specific subpopulations or with particular medical conditions to uncover targeted strategies to improve access or health care delivery for these individuals; alternatively, a large-scale survey on access strategies and customer service could be used to gather opinions and beliefs across a wider range of individuals.
Implications for Policy or Practice
Based on these findings, several practice implications for CHCs emerge. First, there are opportunities to improve patient experience in clinics by setting expectations for accountability in their own care and providing an enhanced feeling of customer service. For example, staff can help patients understand the trickle-down effect on access to care when they miss or cancel an appointment. Likewise, to encourage a customer service orientation when interacting with patients, staff can be trained to manage care delivery delays or difficulties and support patients emotionally. Creating a more effective patient no-show/cancellation policy is one strategy to ensure that available appointment slots are not wasted. Finally, this study is a demonstration of applying a PD approach and offering a novel look into this process. 12
Conclusion
We uncovered many practical approaches to improving access to care for underserved populations by listening to patients, clinical staff, and providers who have found creative pathways through the health care system. Specifically, we found that a patient-centered approach to specific challenges—including poor health literacy, providing tailored support to overcome the social determinants of health and integrated care services (e.g. mental health, dental care)—to be the pathway of the positive deviants in our study. Additionally, delivering a good patient experience (e.g., positive interpersonal relationships, feeling known, being encouraged, and a clean clinic environment) was a prominent strategy among patients who were successful at gaining access to care and clinics that were able to reach difficult populations. Compassion is fundamental: among both clinic staff/providers with a heart for the clinic mission and patients taking a cooperative stance in their own care.
Footnotes
Acknowledgments
The authors thank Ayten Turkcan, Amy Olson Miller, Iman Mohammadi, and patients/staff of participating community health centers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through a Patient-Centered Outcomes Research Institute (PCORI) Award (IH-12-11-5488).