
Abstract
Purpose:
The purpose of this study was to determine the difference in the rate of statin prescribing based on the Adult Treatment Panel (ATP) III and 2013 American College of Cardiology (ACC)/American Heart Association cholesterol guidelines across sex in Federally Qualified Health Centers (FQHCs), and to determine the proportion of patients on recommended statin dosage based on the 2013 cholesterol guideline.
Methods:
The Office Guidelines Applied to Practice (Office-GAP) study is a quasi-experimental, 2 FQHCs center study that enrolled patients with coronary heart disease and diabetes mellitus (DM). We computed 10-year atherosclerotic cardiovascular disease (ASCVD) risks scores based on ACC guidelines and determined the rate of statin prescribing across sex in FQHCs using both guidelines. Main outcomes measures were (1) rate of statin prescribing based on ATPIII and 2013 cholesterol guidelines across sex and (2) proportion of patients on recommended statin dosage based on the 2013 cholesterol guideline.
Results:
The 2013 cholesterol guideline did not increase the rate of eligibility of statin for men and women compared to ATPIII guideline. No significant difference between men and women in statin prescribing under ATPIII (67% vs 57%, P = .13) and 2013 cholesterol guidelines (66% vs 63%, P = .69) and in the recommended dosage of statin per the 2013 cholesterol guidelines between men and women in FQHCs (12% vs 22%, P = .22).
Conclusions:
We found statin underprescribing for both men and women with ASCVD and DM in FQHCs. Utilizing both the ATPIII and the 2013 cholesterol guidelines, men with ASCVD and DM were prescribed statin more than women. However, fewer men were found to be on the recommended dosage of statin based on the 2013 cholesterol guideline. Our findings suggest that Office-GAP may have improved the prescription/use of statin in both men and women.
Introduction
In the United States, 1 in every 4 women, ≥20 years of age, die from heart disease. 1,2
Evidence from meta-analyses showed that statins are equally effective for both men and women in reducing risk of cardiovascular events after adjusting for baseline risk. 3 -5 Coronary intravascular ultrasound used to measure serial changes of plaque burden showed that in women with coronary artery disease (CAD), the use of high-intensity statins may be more beneficial than for men. 5
Few studies evaluating the sex disparity among acute myocardial infarction survivors demonstrated that women are significantly less likely to be prescribed optimal therapy, 6 particularly statin, 7 and have disproportionately poorer prognoses. 8 The recently published modeling study assessing the benefit–harm balance for statins showed that the net benefit from statin occurs at a higher 10-year risks for cardiovascular disease (CVD) and varies by age, sex, and statin type. 9
The release of the 2013 cholesterol guideline 10 raised a major concern that it would significantly increase the number of adults on statin. Contrary to the 2002 Adult Treatment Panel III (ATPIII) guideline, 11 the 2013 cholesterol guideline did not rely on low-density lipoprotein (LDL) level to determine the eligibility for statin and, instead, recommends statin therapy in all individuals who have an LDL level of ≥70 mg/dL and who also have either diabetes or a 10-year risk of CVD of 7.5% or more, as estimated based on the pooled-cohort equations. 12,13
Over 28 million Americans receive health care from Federally Qualified Health Centers (FQHCs), 14 which provide primary health-care services to patients who live in medically underserved areas, are low-income, and who would otherwise have difficulty in securing access to health care. 15 -20 Based on the 2006 to 2008 National Ambulatory Medical Care Survey, in FQHCs, the adherence to old ATPIII guidelines was <50% in CAD, which is comparable to private primary care practices. 21 With the introduction of newer thresholds to initiate high-/moderate-intensity statins in CAD and diabetes, 22 the adherence to statin use in FQHCs is not known. The aim of this secondary analysis was to (1) determine the difference in the rate of statin prescribing based on ATPIII and 2013 American College of Cardiology/American Heart Association (ACC/AHA) cholesterol guidelines across sex in FQHCs and (2) determine the proportion of patients on recommended statin dosage based on the 2013 ACC/AHA guideline.
Methods
The Office Guidelines Applied to Practice (Office-GAP) study was a quasi-experimental design, conducted in 2 FQHCs (intervention/control) in Mid-Michigan, enrolled 243 patients from October 2010 to March 2014. The study was approved by the Michigan State University institutional review board. Eligible patients were aged 18 years or older, who could provide informed consent, and had either a diagnosis of coronary heart disease (CHD) and/or diabetes mellitus (DM) based on International Classification of Disease-9 codes. Patients with cognitive impairment, dementia, and psychosis were excluded from the study. The primary results have been published previously. 23,24 We present here the analysis of 206 patients who completed the study with the information on statin use.
Intervention
As previously reported, 23,24 the Office-GAP intervention included 3 key elements: (1) physician training, (2) patient activation/engagement intervention, and (3) Office-GAP checklist. 24 The checklist was based on the guidelines of the AHA/ACC on secondary prevention of heart disease and the American Diabetes Association 25 and provided a systematic list of evidence-based medications/interventions for patient and provider to review together at 2 regularly scheduled visits at 3 and 6 months. Rates of statin use along with other cardiovascular medications were obtained at baseline, 3, 6, and 12 months. Medication use was assessed by self-report at each visit, validated by the presence of the prescription in the medical record, and confirmed by patients bringing in all active medications.
Statistical Analysis
Based on the ATPIII guideline, we calculated the proportions of statin prescription among those with atherosclerotic CVD (ASCVD) and those with DM but no ASCVD and compared the proportions between men and women using χ2 tests. Based on the 2013 cholesterol guideline, we first calculated the 10-year risk score of ASCVD using the published coefficients in the ACC/AHA guideline 26 and then followed the guideline to find the number of patients eligible for statin prescription (those currently having ASCVD and those with 10-year risk score ≥7.5%). The proportions of statin prescription were calculated among those eligible for statin using the 2013 cholesterol guideline. We compared baseline characteristics between men and women using χ2 test or t test. We used the Wilcoxon rank-sum test to compare the 10-year risk scores of ASCVD between men and women and black and nonblack races. To compare statin prescription between men and women, we used the random-effect logistic regression to account for clustering of observations within individuals and control for baseline characteristics that were significantly different between sex. We used cluster robust standard errors to account of clustering of individuals within FQHCs. Both unadjusted and adjusted odds ratios (ORs) were presented.
Results
Table 1 describes the demographic and health status of the patients by sex. Compared with men, women had higher average body mass index (35 vs 31, P = .004), higher proportion of obesity (67% vs 54%, P = .05), and lower prevalence of CAD (10% vs 26%, P = .002).
Demographic Characteristic by Sex.

Abbreviation: SD, standard deviation.
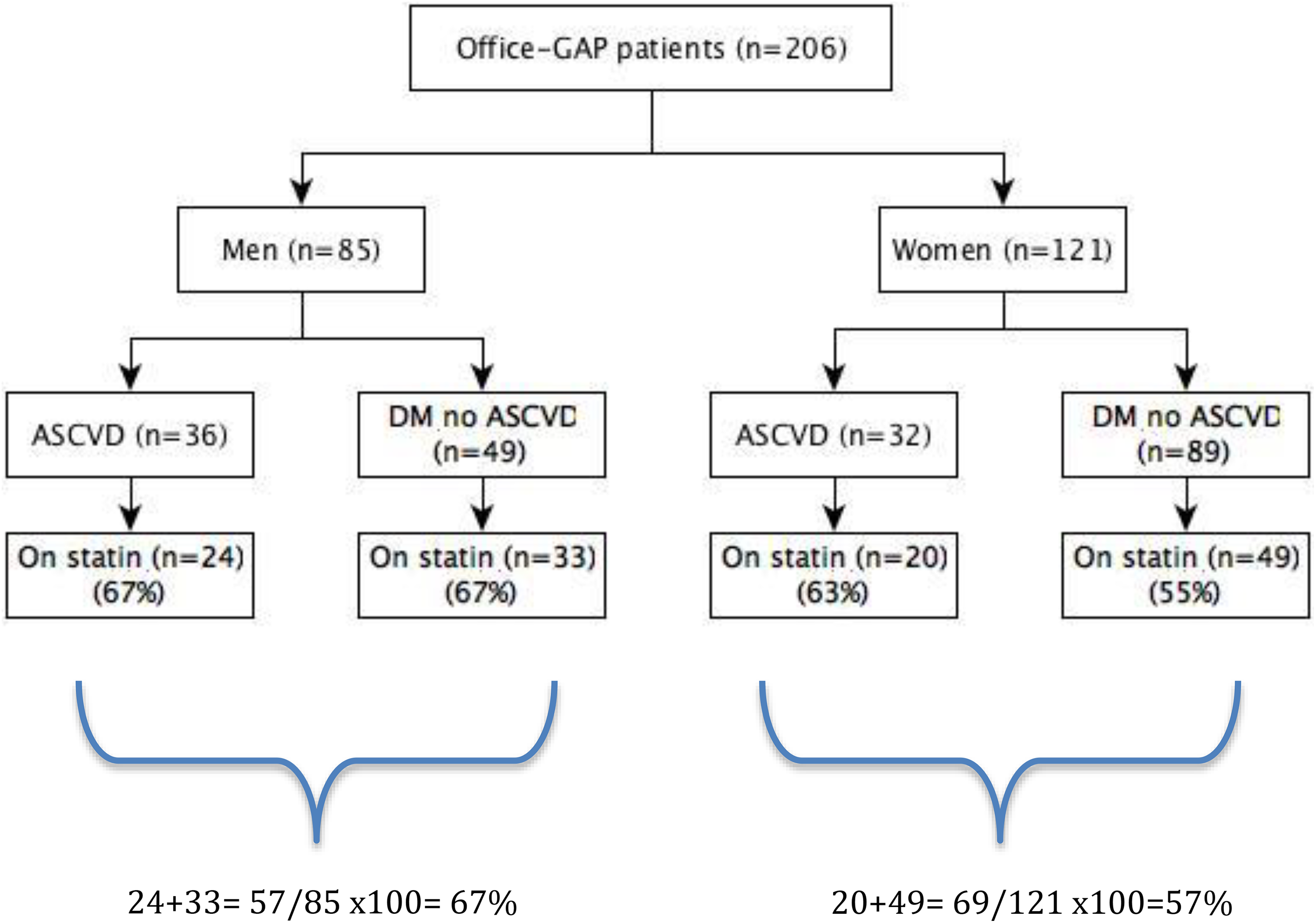
Figure 1 shows the statin use by the ATPIII guideline by sex. Based on ATPIII guidelines, 36 (42%) men and 32 (26%) women with ASCVD and 49 (58%) men and 89 (74%) women with DM and no ASCVD were eligible for statin. For rate of statin’s prescription based on ATPIII guideline, of the 68 patients with ASCVD eligible for statin, 24 (67%) of 36 men versus 20 (63%) of 32 women were on statin (P = .85). Of the 138 patients with DM but no ASCVD, 33 (67%) of 49 men versus 49 (55%) of 89 women were prescribed statin (P = .12). The overall difference in statin use by the ATPIII guideline between men (67%) and women (57%) at baseline was not statistically significant (P = .13).
ATP III guideline: statin use by sex. ATP III indicates Adult Treatment Panel III.
Figures 2 and 3 show the statin use by the 2013 guideline for men and women, respectively. Based on the 2013 cholesterol guidelines, 36 (42%) men and 32 (26%) women with ASCVD and 44 (52%) men and 61 (50%) women with DM and high-risk scores without ASCVD were eligible for statin. Among the 105 who had high-risk scores but without ASCVD, 29 (66%) of 44 men and 39 (64%) of 61 women were prescribed statin (P = .71). Among the 68 patients with ASCVD eligible for statin, the rates were as described above (24/36 [67%] men vs 20/32 [63%] women). Based on the eligibility for statin per the 2013 cholesterol guideline, there was no difference in statin prescription at baseline between men (53/80 [66%]) and women (59/93 [63%]; P = .69).

2013 cholesterol guideline: statin use by men.

2013 cholesterol guideline: statin use by women.
Only (7/53) 13% of these men were on the recommended dosage, whereas 22% (13/59) of these women were on the recommended dosage. This difference in the recommended dosage of statin between men and women was not statistically significant (P = .22).
We found that the implementation of Office-GAP improved the prescription/use of statin in both men and women. In men, statin use increased from 67% pre-GAP to 74% at 12-month follow-up (P = .17). In women, statin use increased from 57% pre-GAP to 71% at 12-month follow-up (P = .02; Table 2). Our findings demonstrate that the use of medicines for triglycerides was low in both men and women and did not improve over the 6-month study period (Table 3).
Statin Use by Sex.

Abbreviations: CI, confidence interval; GAP, Guidelines Applied to Practice; OR, odds ratio.
a Adjusted by BMI, smoking, and coronary artery disease prevalence.
b P value based on cluster robust standard errors.
c Persistent use is defined as having statin prescription in medical record, among patients who had all 3 follow-ups.
Triglycerides Lowering Medications Use by Sex.
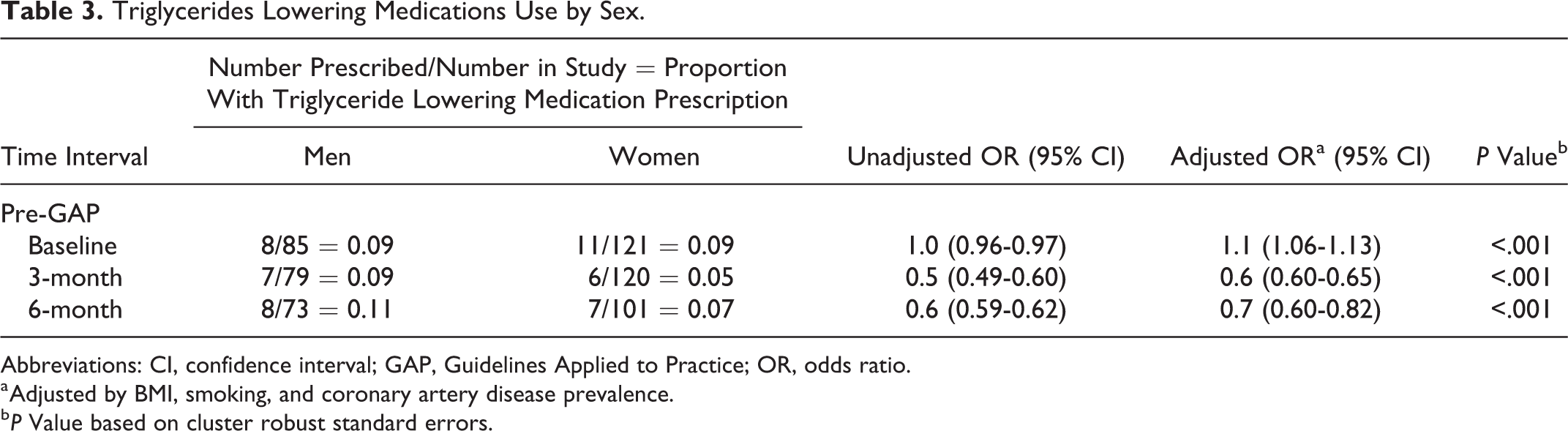
Abbreviations: CI, confidence interval; GAP, Guidelines Applied to Practice; OR, odds ratio.
a Adjusted by BMI, smoking, and coronary artery disease prevalence.
b P Value based on cluster robust standard errors.
Furthermore, we found the ASCVD scores were significantly higher in black men than black women (P = .004) and white men (P = .043). The risk scores were significantly different between white women and black women (P = .018). However, there was no significant difference in distribution between white men and white women (P = .10; Figure 4).

ASCVD 10-year risk score by race and sex. ASCVD indicates atherosclerotic cardiovascular disease.
Discussion
Our findings from FQHCs demonstrate that men were more likely to be prescribed statin but less likely to be on the recommended dosage based on the 2013 ACC/AHA guideline compared to women. Our findings of sex disparity in the rate of statin prescribing in FQHCs are contrary to the well-known national findings of difference that exist in statin prescribing for both men and women. 27,28 Interestingly, we found that more women are on the recommended dosage of statin than men. The reason for finding this difference may be due to the underlying differences in psychosocial factors, whether men are more reluctant to adjust medication is unknown. It may be that the cohort of women in FQHCs better tolerate statins; however, Karalis et al 29 found that women were more likely to stop statin than men due to muscle cramps. It is widely known that side effects from statin therapy often lead to discontinuation of treatment or result in limitation of the dose that is recommended by the guidelines.
Furthermore, we found that in FQHCs, the new 2013 ACC/AHA cholesterol guideline did not increase the rate of eligibility of statin in both men and women. This is contrary to the initial prediction that the 2013 ACC/AHA cholesterol guideline would increase the number of patients eligible for statin 30 but is consistent with the recently published findings by Okerson et al 31 that showed unchanged statin use before and after the guidelines (32% and 31%, respectively). After applying the 2013 guidelines, we found that the percentage of men on the recommended dosage is about half of those for women.
Our findings of improved statin use with the Office-GAP implementation and its sustainability (at 12 months) underscore the significance and possible need for patient activation interventions in patients with chronic conditions. The use of medicine for triglycerides remains low and did not improve over the study period is not a surprise as it is well-known that these medications are not the first-line agent and when they are used in combination with statin, increase risk of adverse events.
Our analysis further demonstrates that black men had higher ASCVD 1-year risk scores compared to white men. The “Jackson Heart Study” 32 showed that African American individuals who had low-to-intermediate ASCVD risk, were not eligible for statins based on the US Preventive Services Task Force guideline, 33 had a higher ASCVD event rate in the presence of coronary artery calcium (CAC) relative to without CAC. These findings further emphasize that the 2013 Cholesterol guidelines appear to be inadequate to accurately estimate ASCVD risk in an African American population and larger studies and special interventions are needed to address the increased CV risk in this population.
Strengths and Limitations
Though our study is based on a small sample size, it reports findings from a population that is not widely studied. Our findings confirm that among our FQHC cohort, black men remain at higher risk of CVD as demonstrated by their higher ASCVD score and emphasize the need for additional intervention and better communication for this patient population. Our Office-GAP intervention is a good fit with these needs, showing sustainability at 12 months although the study ended at 6 months.
Our study has several limitations. First, the data regarding statin use are based on patient self-report and adherence to statin was not objectively determined. However, we confirmed these reports with chart abstraction and by asking patients to bring their medications to office visits or to call the research assistant with their medication list. Second, we enrolled patients with CHD and DM from October 2010 to March 2014, and the findings may not reflect full implementation of the 2013 cholesterol guideline. While the 2013 guideline provides a simplified and effective strategy to reduce the risk of ASCVD, it does not provide recommendations on LDL goals. 13 It is noteworthy and reassuring that the new 2018 guideline now added LDL values and suggests statin use for LDL ≥70. Whether there has already been an improvement in prescribing of statin since the implementation of the 2018 Cholesterol guideline remains unknown, further studies are needed to answer this question. 34
Conclusions
In this quasi-experimental, 2 FQHC study, we found underprescribing of statin for both men and women with ASCVD and DM. For both the ATPIII and the 2013 ACC/AHA guidelines, we found no difference in statin prescribing between men and women. However, fewer men compared to women were found to be on the recommended dosage of statin based on the 2013 ACC/AHA guideline, but this was not statistically significant.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Agency for Healthcare Research and Quality (AHRQ) grant #1 KO8 HS018104.