
Abstract
Background:
The article describes variations in the organization of clinical services for diabetes patients in 10 public primary health clinics in Malaysia with the view to learn from current innovations and improve diabetes service provision.
Methods:
This study combined the use of secondary data and a qualitative multicase study approach applying observations in 10 randomly selected Ministry of Health (MOH) health clinics in Kuala Lumpur and Selangor and semistructured interviews of the family medicine specialists from the same clinics.
Results:
Although there are specific MOH guidelines for diabetes care, some clinics had introduced innovations for diabetes care such as the novel ‘personalized care’, ‘one-stop-centre’ and utilization of patients’ waiting time for health education. Analysis showed that there was room for improvement in terms of task shifting to free precious time of staff with specialized functions, streamlining appointments for various examinations, increasing continuity of consultations with same doctors, and monitoring of performance.
Conclusion:
We contend that there is a potential for increased effectiveness and efficiency of primary diabetes care in Malaysia without increasing the resources – a potential that may be tapped into by systematic learning from ongoing innovation.
Background
Burden of Noncommunicable Diseases in Malaysia
Malaysia has made great strides in providing quality health care for its citizens since the 1960s. Life expectancy has increased for women from 65.6 to 77.3 years and men from 61.6 to 72.2 years between 1970 and 2016. 1,2 The trends seen in life expectancy in Malaysia exceeded that of upper middle-income countries but fared marginally lower than high-income nations. 3
Despite these achievements, there are numerous public health challenges that continue to persist. Malaysia is undergoing an epidemiological transition with causes of mortality shifting from communicable to noncommunicable diseases (NCDs). Malaysia has successfully reduced undernutrition among children but has gradually seen an increase in obesity, not only among children but also among the public in general with a prevalence of 47.7%. 4,5 In 2014, communicable, maternal, perinatal, and nutritional conditions contributed 16% to total deaths, whereas NCDs contributed 73%. 6 In particular, the prevalence of diabetes has seen a drastic increase over the past 10 years with an increase of prevalence rates from 11.6% in 2006 to 15.7% in 2015 for population 18 years and above. 4 These figures translate to about 3.6 million adult Malaysians living with diabetes.
The Malaysian Primary Health-Care System
Malaysia has a health-care system comprising of a comprehensive public sector complemented by an active private sector. Equitable health care is ensured by the implementation of universal health coverage ranging from primary care to tertiary treatments, and basic health care is delivered even to the most remote areas. 1 Primary health care has been declared as the thrust of health services since the inception of the 7th Malaysia Plan in 1996. 1
A large proportion of the primary health-care services in the nation is publicly funded. Currently, 1061 health clinics fall under the direct jurisdiction and oversight of the Ministry of Health (MOH), with smaller clinics in the more remote areas. 7 The bigger health clinics are headed by family medicine specialists (FMSs; who undergo an additional minimum of 4 years postgraduate structured training) and have resident doctors (called medical officers or MOs) and complete in-house facilities that range from medical laboratory tests, plain X-rays, and pharmacies. Thus, the MOH primary care service takes a multidisciplinary team approach to patient care encouraging collaboration between nurses, assistant MOs, nutritionists, dieticians, pharmacists, physiotherapists, and occupational therapists. 8 A large proportion of nurses and assistant MOs have undergone specialized training in DM education, obstetric ultrasonography, eye care, and emergency care. An established referral protocol is in place to ensure continuity of care between MOH primary care clinics and hospitals is maintained at all times. 1
The second major provider of primary health-care services is the private sector including private general practitioners and private primary care clinics that have been established throughout the country, especially in urban areas, to a total of 7146 in 2015. 7 These clinics largely operate single-handed or a by group of 2 to 3 general practitioners, often without the complement of allied health-care personnel. Payments for the services provided are largely borned by the patients, their employers, or health insurance schemes. 1
Diabetes Care in Malaysia
In Malaysia, most people diagnosed with chronic diseases are already receiving their care at the primary care level and for patients diagnosed with diabetes, almost 80% of these seek treatment at MOH health-care facilities, with the majority of patients seen at MOH health clinics. 4 These clinics can be divided into 3 categories of “service delivery package”: universal, intermediate, and advanced, defined by the availability of human resources and services available at the health clinics 9 (Table 1).
Definition of the 3 Categories of “Service Delivery Package” for MOH Primary Health Clinics.
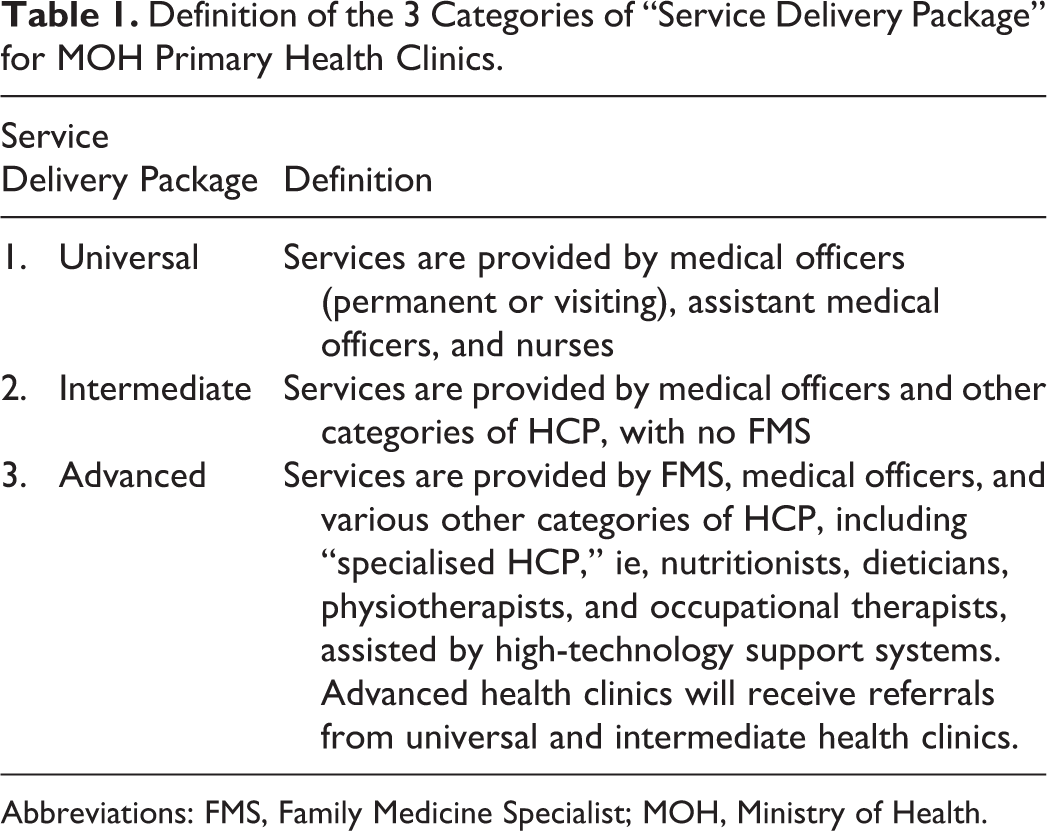
Abbreviations: FMS, Family Medicine Specialist; MOH, Ministry of Health.
Diabetes has been used by the MOH as the entry point for improving the delivery of care of chronic diseases in the Malaysian primary health-care system. Various initiatives have been introduced since the late 1990s and early 2000s to improve the delivery of care for patients with diabetes. These included the establishment of a multidisciplinary approach in managing diabetes patients; setting up of “diabetes resource centers” (DRCs) in MOH hospitals and MOH health clinics to function as “one-stop-centers” for diabetes patients; establishing a post-diploma 6-month structured training for nurses and assistant MOs in diabetes management leading to the title “diabetes educators” after a passed examination; and setting up the use of clinic-held and patient-held diabetes records (called “green cards” since the covers are green in color) to enable clinical audit and for continuity of care of patients across different service provider, for example, between different clinics and hospitals, and across public and private facilities. 10
More recent diabetes-related quality initiatives included the implementation of a nation-wide Diabetes Clinical Audit for type 2 diabetes (T2D) patients in MOH health clinics in 2009, as well as the Quality Assurance (QA) Program called the “Quality of care of diabetes care in MOH health clinics: Glycaemic control,” both starting in 2009. 11,12 To support the implementation of both the Diabetes Clinical Audit and the QA Program, the National Diabetes Registry (NDR), a web-based application, went live on January 1, 2011. 8
The MOH has published several clinical practice guidelines (CPGs) relating to the management of diabetes (both type 2 and type 1) and the major complications relating to diabetes. 13 -15 These CPGs apply to both primary and secondary care. In addition, a standard operating procedure (SOP) document on the management of diabetes patients in MOH health clinics was also published in 2005. 16 This SOP document describes the patient flow in the various types of health clinics (clinics without MOs, clinics with MOs, and clinics with FMSs; delivery of the various components of diabetes care; and the roles and responsibilities of each of the health-care providers involved with the diabetes care).
The objective of this article is to describe the variations in the organization of clinical services for diabetes patients in 10 public primary health clinics in Malaysia, with the view to learn from current innovations, and make service provision more effective. Organization of clinical services for diabetes management is defined as the flow of services or algorithm that a patient has to go through in order to receive the necessary services provided at the clinic with regard to diabetes care.
Methods
Study Design
The study combined the use of secondary data and a qualitative multicase study approach comprising 10 randomly selected MOH health clinics in Kuala Lumpur and Selangor. The study took place within the framework of a larger educational evaluation study. 17,18
Clinic Selection
Ten MOH primary health clinics located in the states of Selangor and Kuala Lumpur were randomly sampled from a sampling frame of 43 health clinics, with a minimum of 1000 active diabetes patients registered, stratified at 2 levels. 18 Both these states are located in the central region of peninsular Malaysia. The capital city of Malaysia as well as several big cities and towns are located in these 2 states, and therefore, the health clinics on average would have a higher patient load overall as well as diabetes patients as compared to the other states in peninsular Malaysia. Data were collected for a period of 3 months from June 2016 to August 2016. There were no cases of dropouts at the clinic or individual staff level during the study.
Data Collection
The study combined primary and secondary data. Primary data were collected in the form of observations of the health clinics based on an observation guide and in-depth interviews of the 10 FMSs of these clinics using a question guide. 18 Both the observation format and the semistructured interview guide for the FMSs contained items and questions relating to key steps in the organization of clinical services for diabetes management in the health clinic, in particular understanding the patient flow in each clinic and the points where various services relating to diabetes care were received by individual diabetes patients. A single senior researcher conducted the observations and all of the in-depth interviews with FMSs. During the observations, the researcher was able to move around to all the various contact points that the patients passed during the visit to the clinic, thereby getting a firsthand impression of the interaction.
Secondary data were obtained from the Family Health Development Division database, MOH Headquarters in Malaysia including data on the type of clinic, size of clinic, average patient load per day for general outpatient attendances, number of new patients and repeat attendees, number of health-care providers by category, and the “service delivery package” available at each health clinic.
The results of the Diabetes Clinical Audit for year 2015 were obtained from the NDR, facilitated by the Disease Control Division, MOH Headquarters. Data were available at the individual clinic level, that included number of diabetes patients registered and on regular follow-up, proportion of patients achieving the hemoglobin (HbA1c) target of <6.5% and mean HbA1c levels.
Data Analysis
Interview transcripts with the FMSs were analyzed using thematic content analysis relating to the organization of clinical services for diabetes management in each health clinic. As the main purpose of this analysis was to identify the key components of the local diabetes-related health systems, these formed a priori domains for coding into which subcategories were generated. In addition, the analysis allowed for the inclusion of themes not predefined in the template. ATLAS.ti was used for analysis.
The observation notes were analyzed to identify common themes and to paint a picture of the organization of the clinical services within which diabetes care was offered based on the items in the observations guide. As the observational data and the data from the in-depth interviews were derived from guides addressing the same points, it was possible to combine the 2 sets of data in order to achieve triage of perspectives.
Results
General Characteristics of the Selected Clinics
Of the 10 MOH health clinics, 7 were located in Selangor and 3 in Kuala Lumpur. It was a diverse group of clinics, in terms of location, size of clinic, type of building, average daily outpatient attendances, and the number of diabetes patients registered. Table 2 provides a summary of some of the main characteristics of these 10 clinics, including the average HbA1c results from their Diabetes Clinical Audit for year 2015. Eight of the 10 health clinics were located in urban areas, and of these all except one were located in purpose-built buildings. Only 2 clinics were located in relatively new buildings. The clinics located in old buildings have had extensive renovations, particularly those in urban areas, to accommodate the increasing number of patients and the increasing scope of services provided at the primary care level. All clinics apart from 2 provided the advanced diabetes service delivery package. These clinics cover an estimated local population that ranges from about 27 000 to 290 000. In terms of average daily outpatient attendances, they range from about 150 patients per day up to about 750 patients per day. The number of registered diabetes patients on regular follow-up at these health clinics ranged from about 1100 up to 4000 patients.
Selected Characteristics of the Study’s 10 MOH Health Clinics in Selangor and Kuala Lumpur, Malaysia.

Abbreviations: CI, confidence interval; HbA1c, hemoglobin A1c; MOH, Ministry of Health.
The mean HbA1c results from the annual Diabetes Clinical Audit showed some variations, ranging from 7.8% to 8.5%. However, the 95% confidence interval (CI) value showed considerable overlap between most of the health clinics (Table 2).
Based on MOH guidelines, the FMSs were the administrative as well as the clinical heads of each health clinic, and in principle they are supposed to be based full time in a particular health clinic. However, in some cases, FMSs have to cover other health clinics if cases where the FMS post are vacant, or there isn’t any post in that particular health clinic. In clinics where the FMS is a visiting FMS, there is usually a senior MO who will undertake the day-to-day administrative duties, but he/she is still answerable to the visiting FMS.
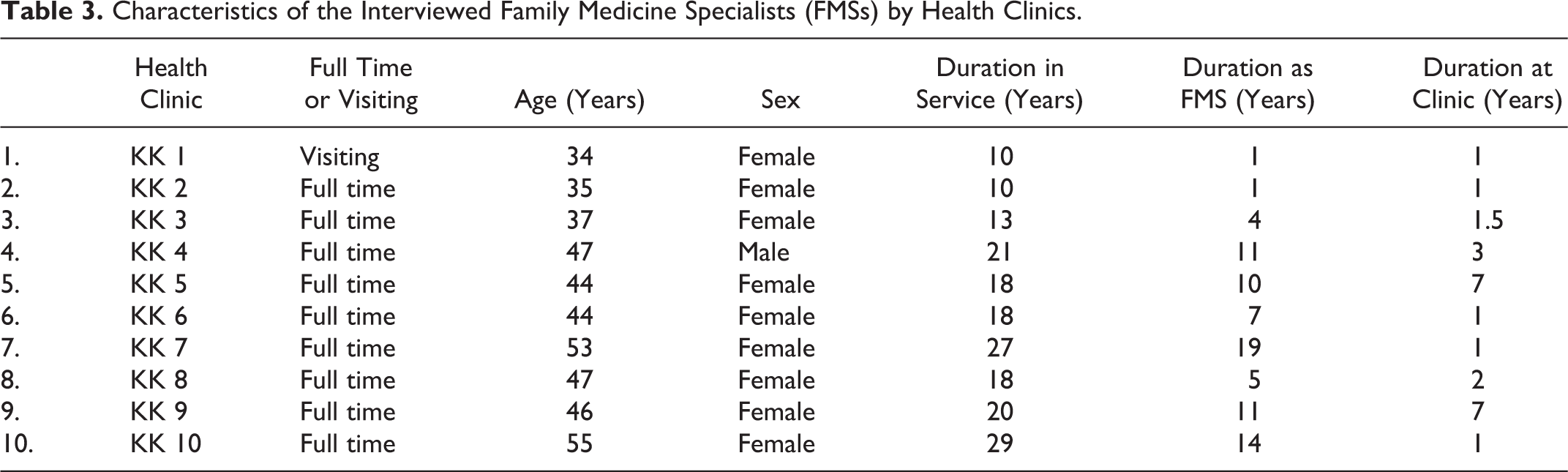
Table 3 shows the characteristics of the FMSs responsible for the 10 health clinics. It is a diverse group of professionals, from very junior FMSs who have just been gazetted as a clinical specialist, to the very senior FMSs with 19 years’ experience as a clinical specialist. All except one FMS were based full time in the health clinics.
Characteristics of the Interviewed Family Medicine Specialists (FMSs) by Health Clinics.
Organization of Delivery of Primary Diabetes Care
The patient flow from the point of registration to discharge from the clinic, and the points of organization of service delivery with roles and responsibilities of the various health-care providers (HCP) in the clinic, is mapped out in Figure 1 to which reference is made in the various sections of the results section.

Typical type 2 diabetes patient flow in a Ministry of Health (MOH) health clinic patient flow is described from the point of registration until discharge from the clinic. The boxes and arrows indicate the standard flow or main consultation received by patient in every appointment. Patients may require to attend separate appointments for the investigations, examinations, or consultation with various health-care providers such as family medicine specialist (FMS), dietician, nutritionist, or pharmacist. The need of consultation with various health-care providers will be indicated and referred by the medical officer (MO). The investigations or examinations may be provided in the same or other clinics.
This study showed that there were variations in the way diabetes patients were managed within the 10 study clinics, partly because of availability of specialized clinical functions and personnel, and partly because of the way work was organized.
Registration
In general, all outpatients were registered at a common registration counter at the health clinic. All 10 health clinics practiced a staggered or block appointment system for diabetes patients who were on regular follow-up or who were newly diagnosed. Diabetes patients might come at any working day outside of the appointment time; however, these patients would be assigned to the general outpatient services, and any diabetes medication would only be prescribed up to the date of the new follow-up appointment.
All 10 MOH health clinics used a standard clinic-held diabetes record called the “green book,” and each patient kept a summary record in a corresponding patient-held “green book” as well. The use of the green books was established in year 2000. Upon registration, the clinic-held green books were retrieved from the records room and be made available to the nurses and MOs.
The variations noted were: Although the usual opening hours for MOH health clinics are from 8 The number of days in the week that appointments were given to diabetes patients for newly diagnosed and on regular follow-up varied. Seven of the 10 clinics have diabetes appointments 4 days a week, from Monday to Thursday, one clinic 5 days a week, one clinic 3 days a week (Tuesday to Thursday), and one clinic only 2 days a week (Wednesday and Thursday).
Screening counter
After registration, diabetes patients would then move on to the “screening counter” (in Malaysia more commonly called “triage counter”) or “screening room.” In all 10 health clinics, the counters were staffed by nurses, usually 2 per counter. The nurses stationed at these screening counters might include certified “diabetes educators.” Only 6 of the 10 health clinics had the services of a diabetes educator (Table 4).
Availability of Selected Diabetes-Related Services in the 10 MOH Primary Health Clinics.
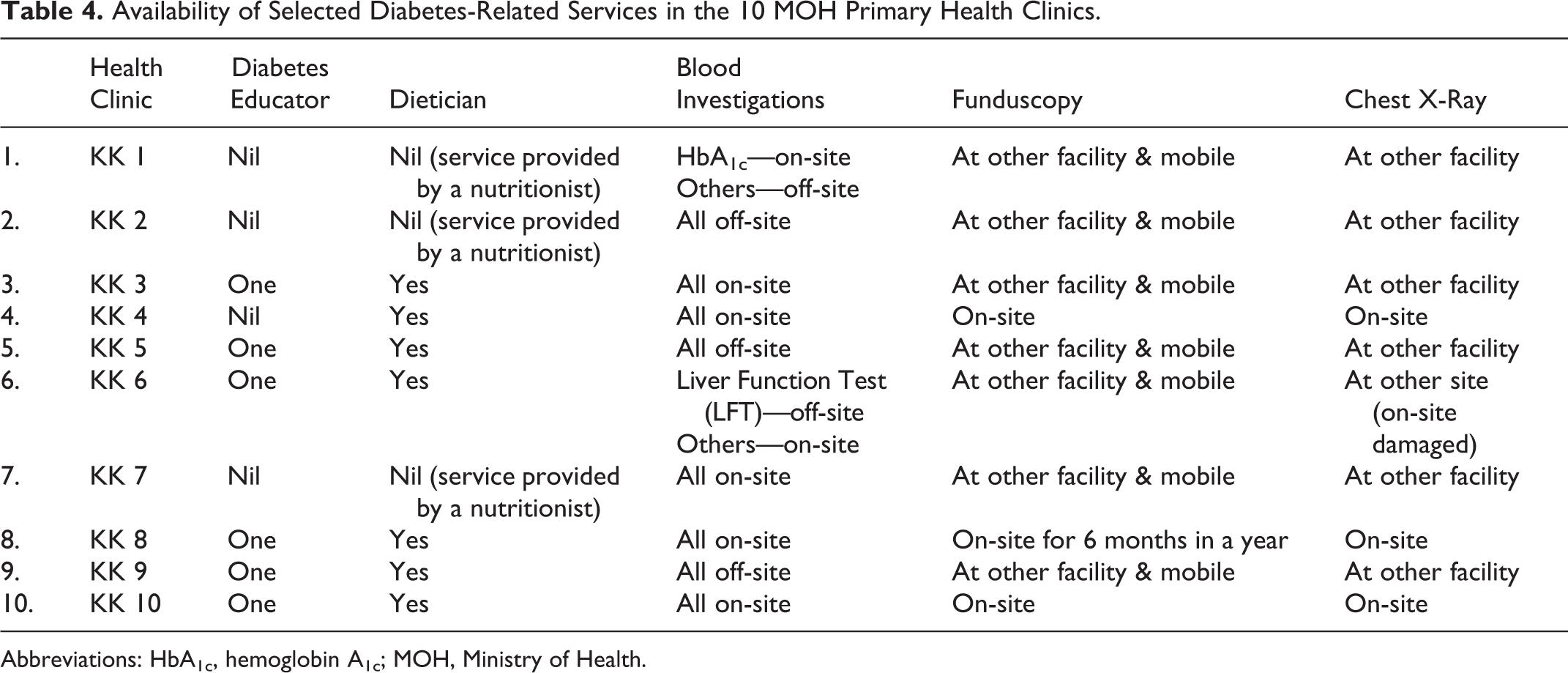
Abbreviations: HbA1c, hemoglobin A1c; MOH, Ministry of Health.
At all counters, patients would have their blood pressure, weight (and height when required), and blood sugar checked. These counters were all located in common areas, and all procedures were done in full view of other patients in the clinic. This may explain why waist circumference measurements were not conducted although this is part of the screening protocol, as this meant some degree of exposure of the patients.
The nurses at these counters were also responsible for reviewing the completeness of the blood investigation results as well as the diabetes-related complication screenings and documenting them in the green cards, both clinic held and patient held, prior to the consultation with the MOs. At 7 clinics, the nurses also completed the routine blood investigation forms for the next visit, which essentially reduced the administrative tasks for the MOs, enabling them to spend more of their contact time with patients doing actual medical consultation.
Since the nurses are helping review availability of results (of screening of complications) and fill up the necessary forms, the MOs can spend more time engaging the patients. Before this, the MOs had to search for results and fill up all investigation forms…it was very distracting. (FMS, KK 1)
In contrast, in 3 health clinics, the nurses were not responsible for reviewing the completeness of results and investigations. In these clinics, the MOs were fully responsible for ensuring all results were available, documenting them in the green cards, and even completing all of the investigations forms for the subsequent visit.
The MOH has published a guideline on the roles and responsibilities of diabetes educators. 16 However, due to the current high work burden in the respective health clinics, these diabetes educators were also responsible for other outpatient clinical duties such as work at the screening counters. Only in 3 health clinics, we observed that the diabetes educators were able to conduct one-to-one consultation with diabetes patients.
However, in one clinic, it was observed that the diabetes educator was singly responsible for all diabetes patients, with minimal assistance of other nursing staff. She had to conduct patient counseling, foot examination, tracing blood investigation results (if missing), and also providing patients with their subsequent follow-up appointment dates. In this clinic, patients would also engage the diabetes educator from multiple points of contact at the clinic, for example, referred by the nurses at the screening counter, referred by the MO for further management, and following the MO consultation for patients to get their next appointment.
In another clinic, because this clinic did not have a diabetes educator, a nurse was assigned this responsibility. In a small, enclosed space that provided some degree of privacy, this nurse was responsible for ensuring that all of the complications screening including foot examination were conducted, blood investigations results made available, and all of the information in the records was updated before the MO saw the patient. The nurse also conducted foot examinations in the same space.
This is an old clinic with very limited space, but I felt it was important that the diabetes nurse had her own “space” to do her work. Despite the limited space, she is able to do her job well and get most of the screening examinations done…(FMS, KK 2)
In summary, the variations noted were: Either there was a common screening counter for all outpatients or a dedicated space for diabetes and/or hypertension patients only. Whether these nurses were only tasked in performing specific clinical examinations or include assisting the MOs on administrative tasks relating to patient care. The availability of diabetes educators in the health clinics, and in their absence, whether a specific nurse was assigned that responsibility. Roles and responsibilities of the diabetes educators and nurses functioning as diabetes educators also differed between health clinics.
Consultation with MO
The mainstay of diabetes management of the health clinic is the responsibility of the MO from the history taking, examination, diagnosis, and treatment. In 3 health clinics, the MOs have full responsibility for ensuring that all of the results of investigations were available for the current consultation, ordering the necessary investigations for the next follow-up and were fully responsible for the patient education on adherence to therapy, dietary advice, and physical activity advice. In clinics where some of these tasks were shifted to the nurses including the diabetes nurses, the MOs were able to spend a larger proportion of their consultation time to focus fully on clinical duties.
In 8 health clinics, 2 MOs shared a single consultation room due to space limitations. This was not very conducive for effective consultation due to lack of privacy and high level of background noises.
Our patients have no privacy…the consultation room is noisy…but what can we do? Our patient load is high and we don’t have enough consultation rooms…and I wonder how much our patients are sharing with the doctors…(FMS, KK 7)
In 8 of the 10 health clinics, consultations for diabetes patients were either conducted in dedicated consultation room(s) with dedicated MOs or a variation in the “Family Doctor Concept” (FDC) described further under the “Innovations” section of the discussion below. The dedicated MOs were either permanently assigned to see diabetes patients or rotated on a weekly, monthly, or 3-monthly basis; or a combination of one permanent MO and one or more rotating MO(s). In the remaining 2 health clinics, it was observed that diabetes patients were seen in between other common outpatient cases, by all of the MOs in the health clinic.
Implementation of the FDC would require a larger clinic space, that is not possible (in my clinic). So when I moved to this clinic over a year ago, I started this new system (of assigning specific rooms for diabetes consultation on specific days) since I felt it is important for diabetes patients to have continuity of care (seeing the same MO). (FMS, KK 3) I have started the system (of assigning patients to specific MOs) since 2 years ago when I had enough MOs…because I can now monitor the quality of care for each MO, I find that they are more accountable for their work…(FMS, KK 5)
Variability was observed for the following activities: Dedicated MOs for diabetes patients versus diabetes patients being seen by all MOs in between other outpatients. In addition to clinical management of diabetes patients, the MOs in some clinics were fully responsible for ensuring completeness of screening investigations and completeness of documentation, while in some clinics these tasks were shifted to nurses. Single or sharing consultation rooms due to space limitations.
Consultation with FMSs, dieticians, nutritionists, and pharmacists
Based on the current status and needs of the patient, he/she might then be referred to the FMS (or other clinical specialists at the hospital level) for further management and to the dietician or nutritionist (where available) for specific dietary advice; the diabetes educator (where available) for more general diabetes care advice; or the Diabetes Mellitus Therapy Adherence Clinic (DM-TAC) services run by the pharmacists.
Referral to the FMS and dietician or nutritionist would usually mean separate appointments, whereas the DM-TAC referral would be made to the pharmacist before the patient collects his/her medications at the pharmacy. All MOH health clinics have their own in-house pharmacies to dispense medications.
Several big clinics in urban areas lack the services of a dietician (Table 4). Although the dietician may be based in a particular clinic, they are essentially “visiting” since they have to cover multiple clinics within the same district. Therefore, they have a monthly visiting timetable for each health clinic that they cover with their own separate appointment system. In clinics where dietetics services were not available, the function was taken over by nutritionists. Some of these nutritionists have additional training in dietetics, but this is not a prerequisite.
We are lucky now to have dieticians posted in health clinics…although we only have one for the whole district, at least some of my patients now can see a dietician. Previously I had to refer my patients to see the nutritionist, and luckily, my nutritionist had formal training in dietetics, but she already has a heavy work burden in managing childhood malnutrition issues. (FMS, KK 1)
Variability was observed regarding: The availability of the FMS at the health clinic; they are either full time or visiting. The availability of either dieticians or nutritionists, and the frequency of their visits to any particular health clinics.
Examinations and investigations
The Malaysian T2D CPG clearly states the examinations and investigations required for diabetes patients together with the time intervals for each examination and investigation. As per common practice for MOH health clinics, for blood investigations that required venous blood taking, patients were given an appointment specifically for blood taking usually conducted by a nurse about 2 weeks prior to their doctor’s appointment. This means that diabetes patients would have to attend the clinics at least once prior to the consultation appointment date.
Depending on the health clinic, some investigations were done at the laboratory at the clinic itself and some would need to be sent to another clinic equipped with the necessary laboratory services. Regardless of whether the tests were done on- or off-site, the results would be made available during the upcoming follow-up appointment. Except for 2 health clinics that used an electronic medical record system called “Tele-Primary Care,” the results were recorded and made available manually.
As part of the screening for diabetes complications protocol, ECGs and foot examinations were also mostly conducted at the same clinic on a separate appointment also prior to the consultation appointment date. These appointments were usually during the afternoon clinic session when the clinics were less busy and conducted by the nurses in the treatment room.
The use of fundus camera is the method of choice for screening for diabetes retinopathy. The fundus camera may be permanently located and available in a health clinic, or patients are referred to the nearest health clinic with a fundus camera (Table 4). In Selangor and Kuala Lumpur, the ophthalmology services have developed a mobile fundus camera service, whereby a single fundus camera is placed in different clinics based on a fixed timetable, manned by the staff at that particular clinic. During the period when the fundus camera is available, the health clinic would then schedule fundus examination for as many patients as possible.
When we had to refer patients to the nearest clinic with a fundus camera to have their fundus checked, our coverage for screening (for diabetes retinopathy) was low. Patients were not going because it was inconvenient for them. Since we started rotating the fundus camera in each KK every 3 months and scheduled fundus examinations around these rotations, our annual screening rates showed drastic improvement…(FMS, KK 5)
The variations that were observed: Laboratory services were available on-site versus off-site, depending on the type of blood investigations. The availability of funduscopy, either it is available on-site permanently or during specified time periods (as part of a mobile fundus camera service), or available off-site at another clinic or nearby MOH hospital. The availability of chest X-ray services, either on-site versus off-site.
Discussion
Innovations Introduced
KK 3 has a unique FDC and personalized care that was introduced by the FMS, when she started working in this clinic one and half years ago. This is unique in the sense that it is not part of current MOH SOP. A diabetes patient is assigned a specific day of the week for all of his/her regular follow-up appointments, and a specific consultation room is also assigned a specific day to receive diabetes patients. Although 2 MOs share each consultation room, with this system, a patient either sees the same MO or at least the same MO is present in the same consultation room.
KK 5 employed a similar FDC that was introduced by the FMS over the past 2 years. A diabetes patient was assigned a specific day of the week for all of his/her regular follow-up appointments, and a specific MO is assigned a specific day to receive diabetes patients. The FMS was only able to implement this new system about 2 years ago when the number of MOs increased to 4. The other innovation introduced in KK 5 was the HbA1c charting of patients being seen by the MOs. Since each MO has their own set of patients, the FMS is able to assess individual performances of each MO based on the HbA1c achievements.
Another innovation done in KK 5 was that while the patient was waiting to be seen by the MO, the DM-TAC pharmacist would select patients with poorly control diabetes for counseling. The counseling not only covered issues on adherence but also touched on dietary and physical activity aspects. This innovation was done on the own initiative of the DM-TAC pharmacist.
The last innovation observed was in KK 7 that had a unique “diabetes one-stop-center” where nurses and MOs shared the same space that also functioned as the DRC. With chairs arranged along a wall in the room, patients waited for their turns to be firstly reviewed by one of the 2 nurses. The nurses ensured that all of the necessary screening investigations were ordered and reviewed for completeness before the MO sees the patient. The nurses also checked the blood pressure, weight (and height when required), and blood sugar together with the foot examination. The nurses working in this room were rotated within the clinic on a daily basis. Patients would then wait to see 1 of the 2 MOs. One of the MOs was dedicated to diabetes management, while the other MO was rotated on a daily basis.
General Issues
This is to our knowledge the first paper that describes in detail the delivery of primary diabetes care in MOH health clinics in Malaysia. Based on the Malaysian T2D CPG, almost all of the required examinations and investigations were made available to the diabetes patients. However, in spite of a well-defined set of guidelines, the study has shown that there was much variability in the delivery of primary diabetes care within key areas.
One common feature was that diabetes patients were required to have multiple visits to the clinic outside of their “main” consultation appointment with the MO to obtain related “services,” such as blood taking, foot examination, fundus examination, ECG, or consultation with the FMS or dietician (Figure 1). Although it is possible that some of these investigations or additional consultation may happen on the same day as the main consultation, by and large this was the exception rather than the rule. As Malaysia moves toward “patient-centered care,” MOH must reengineer the work processes at the health clinics to reduce the number of visits outside of the main consultation appointment. Ideally, all relevant examinations such as chest X-ray and fundoscopy should be conducted at the same appointment. This would not only reduce the time and financial burden for patients and caregivers but is also likely to increase the coverage of screening for diabetes-related complications due to less defaulters of these additional clinic visits. 19 -21
One ethical and clinical issue that was observed was the lack of privacy for patients at the screening counter and consultation with the MO. All of the screening counters or rooms were located in public areas or sharing the same room, and this may explain why waist circumference measurements were not observed. In addition, the high level of noise made any conversations between the nurses and patients difficult. Patients also lacked privacy during the consultation with the MO because of the shared consultation rooms. Although physical examinations can be conducted in suitably private curtained areas, conversations between the MO and patient were not private. This limited the ability of the MO to build rapport and trust with the patient. This also made it very difficult for patients to share more intimate or sensitive health issues, such as incontinence or sexual dysfunctions.
In line with the “patient-centered care” theme, continuity of care by the same health-care provider has been shown in studies to improve patients’ adherence to follow-up, treatment regimes, quality of care, and quality of life for the patients. 22 -25 In the current delivery of primary diabetes care in MOH health clinics, patients do not get to see the same MO during their follow-up visits. This was observed in 8 of the 10 health clinics. However, in 2 clinics, the FMSs have introduced a unique FDC. This innovation has the advantages, that it ensured continuity of care by the same MO, and furthermore the system worked within existing resource constraints of consultation rooms or space and existing number of MOs.
It should be highlighted that the innovative patient-centered initiatives instituted by the FMS and the pharmacist in KK 5, working around their existing local health systems and resources. Due to their personalized care system, KK 5 was able to institute monitoring the performance of individual MOs based on the HbA1c achievement of their patients. This was not possible for the other health clinics since diabetes patients do not see the same MO for repeated visits. Studies have shown the improvement in quality of care for diabetes patients when the appropriate indicators are monitored on a regular basis. 25,26
Other studies have shown the importance of specialized diabetes teams and clinics or services in managing diabetes patients in increasing quality of care and reducing the risks of diabetes-related complications. 22,23,26 We found that 8 the 10 health clinics adopted different strategies to ensure the delivery of dedicated diabetes services by the MOs for patients on scheduled appointments. Therefore, it was possible within current resource constraints and in compliance with existing CPGs to reengineer the delivery of primary diabetes care. In the remaining 2 health clinics that still managed diabetes patients in between general outpatient attendees.
Task shifting from the MOs to the nurses for primary diabetes care has the potential to contribute to addressing the issues of insufficient number of MOs. 27 -29 This in turn can improve health delivery systems where the procedures are well defined and HPC work in a coordinated and organized manner. 30,31 We observed that task shifting was already happening for the pharmacists through the DM-TAC services, providing counseling not only for adherence to oral medications but counseling on the use of insulin including injection techniques. Reengineering the delivery of primary diabetes care should also involve reexamining the roles and responsibilities of nurses in the clinic. Traditionally, the MO is the primary caregiver with the other HCPs playing a supporting role, particularly the nurses. It was observed that in most clinics the nurses undertook very routine tasks, for example, taking blood pressure, blood taking, or routine dressings. They were not observed to conduct any patient counseling. In clinics where the nurses were diabetes educators, they were mostly unable to conduct patient counseling because they were overburdened with routine tasks due to inefficient task division between the nurses. The provision of adequate training and supervision of the nurses would be important in order to improve their knowledge and skills before additional tasks are assigned to them so that the quality of care would not be compromised. 32,33
Another innovation at KK 5 involving the DM-TAC pharmacist circumvented the need for the patient to spend additional waiting time at the pharmacy. Not only did this save time for the patients, it also utilized the time of the patient already spent waiting in the clinic before seeing the MO, which is usually substantial. These innovations hardly cost additional resources to institute.
Although the selected KKs provided a variation in location, size of clinic, type of building, average daily outpatient attendances, and the number of diabetes patients registered, we could not identify any influence on organization of services based on these parameters. Neither did we find any differences according to whether the KKs are situated in urban or rural areas. There was some difference in the availability of human resources and services provided, though this does not seem to determine the extent to which innovations were implemented. The conspicuous factor seemed to be the managerial decisions of the FMSs. Being both the administrative and clinical head of a health clinic, the FMS is in a key position to make changes in the delivery of primary diabetes care in the health clinic. Although it would be expected that such changes would revolve within existing CPGs and SOPs, it was observed that several FMSs made changes outside of these recommended procedures, as described in the innovation section of this article. Unfortunately, the FMSs didn’t conduct any evaluation of the outcome for the patients as a result of the changes and innovations. Neither does the MOH systematically collect the various innovations thereby reaping the potential for improvement in primary health-care services.
The findings of this study lead to other research questions: What do the patients think about the varieties of delivery of primary diabetes services?; Do the different delivery of primary diabetes services actually affect patients’ adherence to their overall follow-up appointments?; Does improved monitoring of the diabetes care in relation to FDC lead to better services?; and not least, does reengineering and streamlining of primary diabetes care lead to improved glycemic control and reduced incidence of complications?
Although it is very important for MOH to invest more in the primary health-care system, 34 based on the findings of this study, quality of care can still be improved within current constraints.
Conclusion
In spite of a centralized MOH health-care system supported by a common national framework that includes an organizational structure, CPGs and SOPs, there is scope for further streamlining the diabetes services in MOH primary health clinics. The study illustrates that existing innovations at individual clinics may potentially improve services at no extra cost. Although standardized national-level guidelines are important, they should be treated as guidelines and provide the overall framework for implementation. The FMSs must be empowered to make changes and introduce innovations to improve quality of care for diabetes patients.
The MOH is advised to more systematically collect and disseminate experiences about current constraints as well positive innovations made at various health clinics with the view to further increase effectiveness. Such a stance of the MOH as being a “learning organization” is likely to have concrete impact not only on diabetes care but even health care in Malaysia more generally.
Footnotes
Authors’ Note
F.I.M., J.A-.H., and U.B-.C. conceived and contributed to the design of the study. F.I.M. and S.C.L. contributed to the acquisition, analysis, and interpretation of data. F.I.M., J.A-.H., and S.C.L. involved in drafting the manuscript. N.H.N., T.A., and U.B-.C. critically revised the manuscript for intellectual content. All authors have read and approved the final manuscript. The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Consent for publication was obtained from the Ministry of Health, Malaysia. Approval to conduct the research in MOH health clinics was provided by the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia, reference NMRR-16-449-29909 (IIR), dated 7 April 2016. Ethics exemption was provided since the research did not involve collecting data from patients and only based on observations and interviews of FMSs. All interviewees were provided with an informed written consent form prior to participation in the in-depth interview.
Acknowledgments
The authors would like to thank the Director General of Health, Malaysia, for his permission to publish this article. The authors would also like to thank the State Health Director of Selangor and Kuala Lumpur for the continuous support during the study period and also the interviewees and other health-care providers for sharing their time and experiences with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is fully funded by Novo Nordisk Foundation.